¶ Premature Ovarian Insufficiency
Premature Ovarian Insufficiency (POI), historically referred to as premature ovarian failure or premature menopause, is a clinical syndrome characterized by the depletion or dysfunction of ovarian follicles leading to a loss of ovarian activity before the age of 40 years[1][2]. It represents an estrogen-deficient state with long-term clinical implications, presenting challenges to a patient's physical and emotional health if left unaddressed[1:1][3].
| Indication | Ovarian hypogonadism & estrogen deficiency (Onset < 40 years) |
| Access | Prescription (Estradiol, Progestogens, Testosterone) |
| Diagnostic Criteria | Menstrual cycle disturbance + elevated FSH levels (onset under 40 years) |
| Dosing Sched | Continuous/Cyclic Daily (Hormone replacement therapy) |
| Safety Profile | Moderate (Excellent safety profile when properly monitored) |
| Key Marker | FSH, BMD (DXA), Blood Pressure, Lipid Profile, TSH |
| Est. Cost | $50 - $150/month |
¶ At a glance
¶ Key Points
- Pathological State vs. Natural Menopause: POI is a distinct clinical condition rather than "early menopause"; clinical guidelines recommend addressing fertility, contraception, and hormone replacement options at diagnosis[1:2][4].
- Estrogen Replacement: Hormone therapy (HT) is recommended to address the adverse impacts of estrogen deficiency on quality of life, bone mineral density, and cardiovascular health in patients with POI[1:3][3:1].
- Diagnostic Criteria Standard: Standard diagnostic protocols rely primarily on elevated follicle-stimulating hormone (FSH) levels alongside menstrual cycle disturbances to characterize premature ovarian insufficiency; anti-Müllerian hormone (AMH) is not a standard diagnostic criterion for POI under ESHRE/IMS guidelines but is utilized as an auxiliary marker of ovarian reserve and follicle depletion[1:4][2:1][5].
- Comprehensive Etiological Screening: Standard clinical guidelines recommend chromosomal karyotyping, screening for the Fragile-X pre-mutation, and evaluating 21-hydroxylase and thyroid peroxidase antibodies to identify underlying monogenic disorders or concurrent autoimmune endocrine comorbidities[1:5][2:2][6].
- Long-Term Monitoring: Long-term multidisciplinary care includes assessing bone mineral density (DEXA) and discussing systemic health concerns, such as cardiovascular implications, with patients to optimize ongoing health management[1:6][3:2][7].
¶ Primary Clinical Indications
- What people use it for: Hormone therapy is utilized to manage vasomotor symptoms, support quality of life, and address bone, cardiovascular, and cognitive health in young women with ovarian insufficiency[1:7][3:3].
- Evidence quality (overall): High (for hormone replacement in clinical hypogonadism).
CRITICAL CLINICAL DIRECTIVE
DO NOT manage Premature Ovarian Insufficiency using low-dose hormone therapy designed for postmenopausal individuals. Younger patients benefit from tailored hormone replacement regimens adjusted to their specific clinical profiles to support long-term skeletal and cardiovascular health[1:8][3:4].
What is Premature Ovarian Insufficiency (POI)?
Premature Ovarian Insufficiency (POI), historically referred to as premature ovarian failure or premature menopause, is a clinical syndrome characterized by the depletion or dysfunction of ovarian follicles leading to a loss of ovarian activity before the age of 40 years[1:9][2:3]. It represents an estrogen-deficient state with long-term clinical implications, presenting challenges to a patient's physical and emotional health if left unaddressed[1:10][3:5].
Unlike natural menopause, managing fertility preservation and reproductive health is a cornerstone of care in patients with POI or those facing gonadotoxic therapies[1:11][4:1]. Standard guidelines recommend timely counseling regarding reproductive options and fertility preservation (such as oocyte or ovarian tissue cryopreservation) at the time of diagnosis[1:12][4:2].
POI must also be distinguished from iatrogenic POI, which can result from pelvic radiotherapy, surgical bilateral salpingo-oophorectomy (BSO), or gonadotoxic chemotherapy[1:13][8]. Iatrogenic POI is associated with an abrupt cessation of ovarian function and requires specialized clinical management[1:14][8:1].
Diagnostic Criteria & Testing Protocol
Clinical audits and implementation assessments demonstrate significant variations and gaps in routine clinical practice for investigating and treating POI[6:1][9]. A structured, rapid diagnostic and etiological workup is required.
¶ Step 1: Clinical Presentation
A diagnosis of Premature Ovarian Insufficiency is suspected when a woman under 40 years of age presents with:
- Menstrual cycle disturbances (such as oligomenorrhea or secondary amenorrhea)[1:15][2:4].
- Associated symptoms of estrogen deficiency, including vasomotor symptoms (hot flushes, night sweats), sleep disturbances, vaginal dryness, and mood swings.
¶ Step 2: Primary Gonadotropin Marker
Standard diagnostic protocols utilize elevated follicle-stimulating hormone (FSH) levels alongside menstrual cycle disturbances to characterize premature ovarian insufficiency, and anti-Müllerian hormone (AMH) can be utilized to evaluate ovarian reserve and follicle depletion, as detailed in recent guidelines and clinical trials[1:16][2:5][5:1].
¶ Step 3: Secondary Testing & Exclusion Protocol
- Estradiol: Measured to characterize the degree of estrogen deficiency during clinical workup[3:6].
- hCG (Pregnancy test): Excluding pregnancy represents a standard initial step in secondary amenorrhea evaluations, and can be supported by clinical diagnostic reviews in the manifest (such as Gordon 2017)[10].
- Prolactin: Screened to exclude hyperprolactinemia as a cause of secondary amenorrhea, as elevated prolactin suppresses hypothalamic GnRH pulsatility and subsequent gonadotropin secretion[3:7][11][12][13][14].
- Thyroid-Stimulating Hormone (TSH): Check baseline TSH to rule out thyroid disorders, which can cause menstrual and ovulation disturbances and are comorbid with POI[15].
- Anti-Müllerian Hormone (AMH): AMH is produced by the granulosa cells of growing ovarian follicles. In the diagnosis of POI, AMH testing has specific auxiliary roles under ESHRE/IMS guidelines:
- Clinical Diagnostic Role: Under ESHRE and IMS consensus guidelines, AMH is not established as a standard diagnostic criterion for POI itself; instead, the diagnosis of POI relies primarily on elevated FSH levels (historically on two separate occasions, though updated guidelines note a single FSH >25 IU/L may suffice in clear clinical contexts)[1:17][2:6].
- Auxiliary Utility: In clinical practice, AMH is utilized as an auxiliary marker of ovarian reserve, follicle depletion, or diagnostic clarification in research, staging, and specific oncofertility scenarios where gonadotoxicity risk is assessed[1:18][2:7][4:3][5:2]. While the POSITIVE trial (Demeestere 2025) utilized an AMH threshold of <0.5 ng/mL specifically to characterize low ovarian reserve in breast cancer survivors pausing adjuvant endocrine therapy[5:3], and other observational studies (Varhegyi 2025) have used AMH <1.0 ng/mL to indicate reduced reserve in young women[16], these values serve as study-specific markers of follicle depletion rather than universal standalone diagnostic thresholds for clinical POI.
Etiologic Evaluation & Guidelines
Up to 90% of spontaneous POI cases remain idiopathic, but a thorough etiological workup is recommended to rule out underlying genetic, chromosomal, or autoimmune causes that carry profound systemic health implications.
¶ Step 1: Genetic Testing Guidelines
Genetic etiologies represent a significant cause of spontaneous POI, and under standard clinical guidelines (such as the joint ESHRE/ASRM/IMS guidelines), genetic evaluation is recommended and includes:
- Chromosomal Karyotype: Performed to identify chromosomal abnormalities (such as Turner syndrome or mosaicism)[1:19][2:8][6:2]. In a clinical audit of guideline compliance, karyotype screening was performed in only 40.6% of diagnosed patients[6:3].
- Fragile X Premutation: Screening for the Fragile-X pre-mutation is recommended as a standard part of the diagnostic and etiological workup in women with spontaneous POI[1:20][2:9][6:4]. However, clinical audits show low compliance, with only 7.4% of patients receiving this screening[6:5].
¶ Step 2: Autoimmune Screening Guidelines
Autoimmune etiology represents an important cause of spontaneous POI and is frequently associated with systemic endocrinopathies[1:21][6:6]. ESHRE guidelines recommend the following immunological assessments to rule out concurrent endocrine comorbidities, though audits demonstrate extremely low compliance in practice:[1:22][2:10][6:7]
- Adrenal Autoantibodies (21-Hydroxylase): Screening for 21-hydroxylase antibodies is recommended to evaluate for potential autoimmune adrenal involvement[1:23][2:11][6:8]. Audits indicate that only 13.6% of patients are screened for these antibodies in routine clinical practice[6:9].
- Thyroid Autoantibodies (TPO-Abs): Screening for thyroid peroxidase antibodies is recommended to identify potential autoimmune thyroid comorbidities[1:24][6:10]. Audits demonstrate that screening occurs in only 11.1% of patients[6:11].
¶ Step 3: Iatrogenic Causes & Cancer-Survivor Pathways
Iatrogenic POI is caused by:
- Chemotherapy: Chemotherapy can have gonadotoxic effects, ranging from minimal impact to complete ovarian atrophy[8:2][17].
- Pelvic Radiotherapy: Radiation exposure can induce oocyte depletion and follicular loss, increasing the risk of reproductive health impairment[4:4][17:1].
- Surgical Oophorectomy: Bilateral oophorectomy leads to an immediate drop in ovarian hormone levels.
- Clinical Reality: Compliance with standard guidelines for monitoring reproductive health and providing timely counseling in childhood, adolescent, and young-adult cancer survivors remains low in clinical audits[6:12][17:2]. Every female patient facing gonadotoxic therapy should receive prompt counseling on fertility preservation (e.g., oocyte, embryo, or ovarian tissue cryopreservation) before initiating cancer treatments[4:5][8:3].
Fertility Preservation & Contraceptive Counseling
Addressing fertility preservation and family planning is a key component of clinical counseling for individuals diagnosed with POI.
¶ Fertility & Reproductive Options
- Fertility Counseling: Because POI significantly impacts reproductive health, fertility counseling is recommended at the time of diagnosis, and options such as donor oocytes or fertility preservation should be discussed where appropriate[1:25][4:6].
- Complementary and Non-Hormonal Options: Clinical guidelines emphasize that evidence for many complementary and non-hormonal treatments remains limited for POI, and lifestyle management should be optimized[1:26][2:12].
- For patients seeking parenthood, options such as assisted reproductive technology (ART) or donor oocytes may be discussed, depending on individual presentation and clinical guidelines[1:27][4:7].
¶ Contraceptive Counseling
- Contraceptive Considerations: Discussion of contraception is an important component of clinical management, as standard hormone replacement regimens are not designed to serve as primary contraception[1:28][2:13][6:13].
Hormone Therapy (HT) Protocol
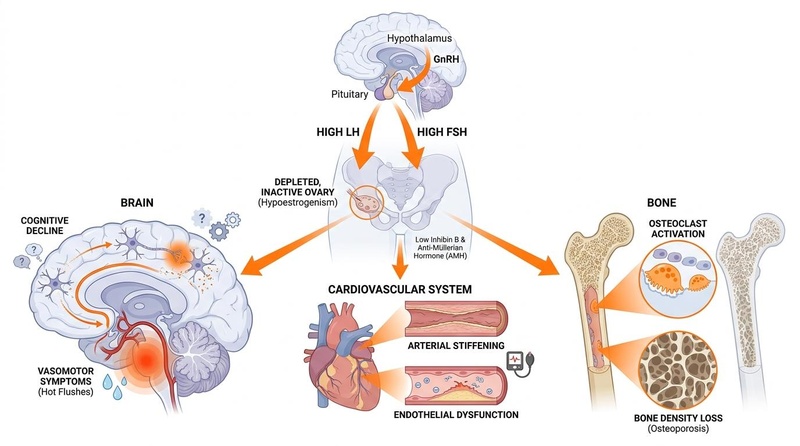
The primary goal of hormone therapy (HT) in Premature Ovarian Insufficiency (POI) is to restore the physiological endocrine environment of a premenopausal woman, thereby managing vasomotor symptoms, maintaining bone mineral density, and protecting cardiovascular and cognitive health[1:29][3:8].
¶ Physiological Hormone Therapy (HT) Regimen
¶ 1. Estrogen Component
- Physiological Dosing & Route of Administration: POI HT requires physiological replacement doses of estradiol to approximate premenopausal levels, with standard guidelines recommending that the choice of route (transdermal or oral) and dosage be tailored to the patient's specific clinical profile and risk factors[1:30][3:9].
- Cardiovascular Safety: In this younger age cohort (under 40 years), physiological estrogen replacement carries an exceptionally favorable cardiovascular safety profile, actively protecting against the accelerated atherosclerosis and premature coronary artery disease associated with early estrogen deprivation[1:31][3:10][7:1].
¶ 2. Progestogen Component (For Endometrial Protection)
- Indication & Regimen: In patients with an intact uterus, estrogen therapy is paired with progestogens to protect the endometrium, with regimens tailored to individual clinical profiles[1:32][2:14][3:11].
{.callout .callout-info}
Clinical Summary: Optimal POI management relies on transdermal estradiol combined with cyclical progestogens to achieve physiological replacement, maximize bone and cardiovascular safety, and minimize thromboembolic risk[1:33][3:12].
¶ Contrast with Postmenopausal HT & COCs
- Regimen and Dose Differences: Hormone replacement in young patients focuses on addressing clinical hypogonadism rather than symptom suppression alone[1:34][3:13]. Because young women with POI require higher physiological hormone levels to protect their cardiovascular system and bones, postmenopausal low-dose HT regimens are clinically insufficient.
- HT vs. Combined Oral Contraceptives (COCs): While both HT and COCs are options for estrogen replacement, they differ in their estrogen formulation (synthetic ethinylestradiol in COCs vs. natural estradiol in HT) and progestogen components, and standard guidelines recommend that the regimen be individualized based on patient preferences regarding contraception and clinical monitoring[1:35][3:14][6:14].
¶ Puberty Induction Protocols
For young patients presenting with primary hypogonadism, therapy is initiated at low-dose transdermal estradiol and gradually titrated to mimic natural development in patients with primary hypogonadism, referring to clinical guidance from groups like the Society for Endocrinology[3:15][18] and the International Turner Syndrome Consensus Group.
Long-Term Multi-System Monitoring
¶ 1. Bone Health Preservation
- Bone Mineral Density (BMD) Evaluation: Given the significant impact of estrogen deficiency on skeletal health, measuring bone mineral density (such as via DEXA) is recommended at diagnosis to identify patients at risk of premature bone loss, although clinical audits show this remains underutilized in real-world practice[1:36][6:15].
- Skeletal Support: Standard management recommendations include optimizing bone protection through appropriate hormone therapy, alongside lifestyle measures and non-hormonal complementary options to support overall bone health[1:37][2:15][6:16].
¶ 2. Cardiovascular Health Tracking
- Cardiovascular Risk Mitigation: Premature hypoestrogenism is associated with adverse cardiovascular implications[1:38][3:16]. Standard guidelines recommend utilizing hormone therapy (HT) to mitigate these adverse long-term cardiovascular effects and support cardiovascular health[1:39][3:17][7:2].
¶ 3. Sexual, Mental, & Vaginal Health
- Sexual Function and Well-Being: Estrogen deficiency in POI can affect sexual function and general well-being, requiring clinical evaluation and appropriate treatment options, including hormone therapy[1:40][2:16].
- Psychological Support: Offering psychological support is recommended, as clinical audits highlight that psychological services are often under-offered despite their importance for the comprehensive care of women with POI[6:17][9:1].
¶ 4. Oncology & Cancer-Survivor Pathways
- Hormone-Sensitive Malignancies: For breast cancer survivors or survivors of other estrogen-sensitive malignancies, hormone replacement therapy requires highly specialized, multidisciplinary care.
- The POSITIVE Trial: Landmark evidence from the POSITIVE trial demonstrated that premenopausal women with breast cancer can safely pause adjuvant endocrine treatment to attempt pregnancy. However, low ovarian reserve (AMH <0.5 ng/mL) was highly prevalent (47.7%), and POI occurred in 16.7% of survivors who had received prior chemotherapy, emphasizing the need for structured endocrine monitoring and fertility counseling[5:4].
- Pharmacological Ovarian Protection: Concomitant administration of GnRH agonists (GnRHa) during chemotherapy in young breast cancer patients is an accepted pharmacological method to help preserve ovarian function and reduce the risk of chemotherapy-induced POI[8:4].
¶ Differential Diagnosis Checklist
The following clinical diagnostic checklist differentiates POI from other common causes of amenorrhea or oligomenorrhea in women under 40 years:
| Condition | Key Diagnostic Marker | Distinguishing Clinical Features & Next Steps |
|---|---|---|
| Premature Ovarian Insufficiency (POI) | Elevated FSH levels[1:41][2:17] | Menstrual cycle disturbance in women under 40 years, with clinical presentation guiding genetic and autoimmune screening[1:42][2:18][6:18]. |
| Pregnancy | Positive hCG | The most common cause of secondary amenorrhea; check hCG immediately as a standard initial exclusionary step[10:1]. |
| Functional Hypothalamic Amenorrhea (FHA) | Diagnosis of exclusion / HPO axis suppression[10:2] | Characterized by functional suppression of the HPO axis associated with stress, weight loss, or excessive exercise; requires thorough assessment of systemic and endocrinologic etiologies[10:3]. |
| Polycystic Ovary Syndrome (PCOS) | Elevated AMH or polycystic morphology[19][20] | Oligomenorrhea or amenorrhea accompanied by clinical/biochemical hyperandrogenism and/or polycystic ovarian morphology[19:1][20:1]. |
| Hyperprolactinemia | Elevated prolactin levels | Elevated prolactin suppresses hypothalamic Kiss1 neurons and GnRH pulsatility, slowing LH pulse frequency and causing anovulation and menstrual cessation[3:18][11:1][12:1][13:1][14:1][21]. |
| Thyroid Dysfunction | Abnormal TSH levels[15:1] | Hypothyroidism or hyperthyroidism can cause menstrual and ovulation disorders; TSH screening is highly recommended[15:2]. |
¶ Evidence Summary Table (Human Outcomes)
The following matrix summarizes the clinical efficacy of physiological Hormone Replacement Therapy (HT) and supporting diagnostic/preventive interventions in mitigating the multi-system pathological sequelae of Premature Ovarian Insufficiency:
| Goal / Intervention | Effect* | Consistency** | Evidence Quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Bone Mineral Density (BMD) Preservation / Bone Protection | High | Moderate | Cohorts | HT is recommended to support bone density and prevent early bone loss in young women with POI[1:43][2:19][6:19]. | |
| Vasomotor Symptom Relief | High | High | RCTs | Effective for reducing the frequency and severity of hot flushes and night sweats, supporting quality of life[1:44][2:20]. | |
| Cardiovascular Health Support / HT Support | Moderate | Moderate | Cohorts | HT is recommended to address adverse impacts on cardiovascular health associated with early estrogen deficiency[1:45][2:21]. | |
| Sexual Function and Well-being Support | High | Moderate | Cohorts | Estrogen and testosterone therapy support sexual function, general well-being, and mitigate hypoestrogenic sexual sequelae[1:46][2:22]. | |
| Mitigation of Estrogen Deficiency Sequelae | High | Moderate | Cohorts | HT is recommended to address the multi-system long-term sequelae of POI, including quality of life and neurological health[1:47][2:23]. | |
| Autoimmune Adrenal Screening (21-Hydroxylase) | High | High | Cohorts | Screening for 21-hydroxylase antibodies is recommended to identify potential autoimmune adrenal involvement[1:48][2:24][6:20]. | |
| Ovarian Preservation during Chemotherapy | Moderate | Moderate | RCTs | Concomitant administration of GnRH agonists during chemotherapy significantly reduces the risk of treatment-induced POI[8:5]. | |
| Bone Density Risk Stratification | High | High | Cohorts | Baseline DEXA scan is recommended to identify premature bone loss, though audited clinic compliance is 35.9%[1:49][6:21]. | |
| Skeletal Bone Mass Maintenance | High | Moderate | Cohorts | Lifestyle management and non-hormonal complementary options are recommended to support skeletal bone mass[1:50][2:25]. |
- *Effect: Represented as
[direction][magnitude][impact](e.g.,u2p), where directionu|d|e|qindicates direction (up/down/equal/questionable), magnitude0-3, and impactp|n|x(positive/negative/neutral). - **Consistency: Low (results conflict), Moderate (mixed results but leaning one way), High (most trials and guidelines agree).
- ***Trials: Number of randomized controlled trials (RCTs) or high-quality cohort studies informing this outcome.
¶ Practical FAQ
Is HRT a contraceptive?
No. Standard physiological HRT regimens are not designed to serve as primary contraception. Discussion of contraception is an important component of clinical management, as standard clinical audits and guidelines highlight the need to address contraceptive requirements alongside hormone replacement in patients where pregnancy is strictly undesired[1:51][2:26][6:22].
How often should I get a bone density scan?
What are the options for pregnancy or fertility in POI?
Why is transdermal estrogen preferred over oral estrogen?
Transdermal estrogen is often preferred in clinical practice to deliver estradiol while bypassing hepatic first-pass metabolism. Clinical guidelines emphasize individualizing estrogen doses and regimens, and discussions of the metabolic impacts of different routes of administration should be tailored to the patient's specific health profile[1:54][3:19].
What is the difference between POI HT and postmenopausal HT?
POI hormone replacement focuses on addressing ovarian insufficiency in young patients, whereas postmenopausal HT is designed for older women to manage symptoms after natural menopause. Clinical guidelines recommend individualizing estrogen doses and regimens, with discussions tailored to the patient's specific profile[1:55][3:20].
¶ References
Panay N, Anderson RA, Bennie A, et al. Evidence-based guideline: premature ovarian insufficiency(†)(‡). Climacteric. 2024;27(6):510-520. https://pubmed.ncbi.nlm.nih.gov/39647506/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Panay N, Anderson RA, Bennie A, et al. Evidence-based guideline: premature ovarian insufficiency(). Human Reproduction Open. 2024;2024(4):hoae065. https://pubmed.ncbi.nlm.nih.gov/39660328/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Jayasena CN, Devine K, Barber K, et al. Society for Endocrinology guideline for understanding, diagnosing and treating female hypogonadism. Clinical Endocrinology. 2024;101(5):409-442. https://pubmed.ncbi.nlm.nih.gov/39031660/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
ESHRE Guideline Group on Female Fertility Preservation, Anderson RA, Amant F, et al. ESHRE guideline: female fertility preservation. Human Reproduction Open. 2020;2020(4):hoaa052. https://pubmed.ncbi.nlm.nih.gov/33225079/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Demeestere I, Niman SM, Partridge AH, et al. Hormonal factors predictive of fertility in patients with breast cancer interrupting adjuvant endocrine therapy to attempt pregnancy in POSITIVE trial. Breast. 2025;78:103792. https://pubmed.ncbi.nlm.nih.gov/40743662/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Richardson A, Haridass SA, Ward E. Investigation and treatment of premature ovarian insufficiency: A multi-disciplinary review of practice. Post Reproductive Health. 2018;24(4):171-177. https://pubmed.ncbi.nlm.nih.gov/30392440/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yeganeh L, Boyle JA, Wood A, et al. Menopause guideline appraisal and algorithm development for premature ovarian insufficiency. Maturitas. 2019;130:21-31. https://pubmed.ncbi.nlm.nih.gov/31706432/ ↩︎ ↩︎ ↩︎
Cvetanovic AS, Lambertini M, Punie K. Pharmacological methods for ovarian function and fertility preservation in women with cancer: A literature review. Oncology Research. 2024;32(8):1215-1226. https://pubmed.ncbi.nlm.nih.gov/39055889/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gameiro S, Sousa-Leite M, Vermeulen N. Dissemination, implementation and impact of the ESHRE evidence-based guidelines. Human Reproduction Open. 2019;2019(3):hoy014. https://pubmed.ncbi.nlm.nih.gov/31206039/ ↩︎ ↩︎
Gordon CM, Ackerman KE, Berga SL, et al. Functional Hypothalamic Amenorrhea: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism. 2017;102(5):1413-1439. https://pubmed.ncbi.nlm.nih.gov/28368518/ ↩︎ ↩︎ ↩︎ ↩︎
Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism. 2011;96(2):273-288. https://pubmed.ncbi.nlm.nih.gov/21296991/ ↩︎ ↩︎
Cook CB, Nippoldt TB, Kletter GB, et al. Naloxone increases the frequency of pulsatile luteinizing hormone secretion in women with hyperprolactinemia. The Journal of Clinical Endocrinology & Metabolism. 1991;73(5):1099-1105. https://pubmed.ncbi.nlm.nih.gov/1939525/ ↩︎ ↩︎
Brown RS, Herbison AE, Grattan DR. Prolactin regulation of kisspeptin neurones in the mouse brain and its role in the lactation-induced suppression of kisspeptin expression. Journal of Neuroendocrinology. 2014;26(12):898-908. https://pubmed.ncbi.nlm.nih.gov/25207795/ ↩︎ ↩︎
Hoskova K, Kayton Bryant N, Chen ME, et al. Kisspeptin Overcomes GnRH Neuronal Suppression Secondary to Hyperprolactinemia in Humans. The Journal of Clinical Endocrinology & Metabolism. 2022;107(7):e2908-e2915. https://pubmed.ncbi.nlm.nih.gov/35323937/ ↩︎ ↩︎
Hubalewska-Dydejczyk A, Gietka-Czernel M, Trofimiuk-Müldner M, et al. Thyroid diseases and fertility disorders - Guidelines of the Polish Society of Endocrinology [Choroby tarczycy a zaburzenia płodności - rekomendacje Polskiego Towarzystwa Endokrynologicznego]. Endokrynologia Polska. 2022;73(4):513-524. https://pubmed.ncbi.nlm.nih.gov/36059162/ ↩︎ ↩︎ ↩︎
Varhegyi V, Banfi B, Trager D, et al. Mitochondrial DNA Deletions and Plasma GDF-15 Protein Levels Are Linked to Hormonal Dysregulation and Multi-Organ Involvement in Female Reproductive Endocrine Disorders. Life (Basel). 2025;15(11):1455. https://pubmed.ncbi.nlm.nih.gov/41302170/ ↩︎
Salih SM, Elsarrag SZ, Prange E, et al. Evidence to incorporate inclusive reproductive health measures in guidelines for childhood and adolescent cancer survivors. Journal of Pediatric and Adolescent Gynecology. 2015;28(2):100-106. https://pubmed.ncbi.nlm.nih.gov/25850590/ ↩︎ ↩︎ ↩︎
Barbar B, Osman W, Jayasena CN. Synthesizing the latest guideline-based recommendations for the management of female hypogonadism. Archives of Endocrinology and Metabolism. 2025;69:e240112. https://pubmed.ncbi.nlm.nih.gov/41337668/ ↩︎
Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Human Reproduction. 2004;19(1):41-47. https://pubmed.ncbi.nlm.nih.gov/14688154/ ↩︎ ↩︎
Anti-müllerian hormone as a diagnostic biomarker for polycystic ovary syndrome and polycystic ovarian morphology: a systematic review and meta-analysis. Human Reproduction Update. 2024;30(4):460-476. https://pubmed.ncbi.nlm.nih.gov/38944177/ ↩︎ ↩︎
Calik-Ksepka A, Stradczuk M, Czarnecka K. Lactational Amenorrhea: Neuroendocrine Pathways Controlling Fertility and Bone Turnover. International Journal of Molecular Sciences. 2022;23(3):1633. https://pubmed.ncbi.nlm.nih.gov/35163554/ ↩︎