¶ Probiotics, Prebiotics, and Postbiotics
| Type | Microbiome Therapeutic Classes |
| Subclasses | Prebiotics, Probiotics, Synbiotics, Postbiotics |
| Main Actives | Fibers, Live Microbes, SCFAs, Bacteriocins |
| Key Targets | Gut Epithelium, GALT, ENS, Vagus Nerve |
| Clinical Uses | IBS, Antibiotic Recovery, Immune Modulation |
The clinical manipulation of the human gastrointestinal microbiome has evolved far beyond the simple consumption of generic live bacteria [1]. Today, microbiome medicine is built on a precise, multi-tiered framework established by the International Scientific Association for Probiotics and Prebiotics (ISAPP): probiotics (live beneficial microbes), prebiotics (selective microbial substrates), synbiotics (synergistic combinations), and postbiotics (inanimate microbial preparations and metabolites) [2][3][4]. Understanding the pharmacological behavior, cellular targets, and clinical limitations of each "biotic" class is critical for optimizing human healthspan, addressing metabolic dysfunction, and managing mucosal immune disorders [5].
¶ At a glance
Key points (high-level summary)
- Defining the Classes: Probiotics introduce live beneficial species; prebiotics selectively nourish resident taxa; synbiotics pair both synergistically; postbiotics deliver standardized, non-viable cell parts and active metabolites directly [1:1].
- Strain Specificity is Absolute: The clinical effects of probiotics are entirely strain-specific (e.g., L. rhamnosus GG has different immunological targets than L. rhamnosus HN001). Species-level labeling is insufficient for clinical outcomes [6].
- The Rise of Postbiotics: Postbiotics offer high chemical stability, long shelf-life, and represent a major safety breakthrough, as they can be administered to immunocompromised individuals without the risk of bacterial translocation or sepsis [4:1].
- Precision Prebiotics: Modern prebiotics have shifted from simple bulk fibers to engineered polysaccharides designed to selectively increase specific target taxa (such as Akkermansia muciniphila or Faecalibacterium prausnitzii) to resolve systemic metabolic and inflammatory states [7].
What people use it for
- Main goals: Ameliorating irritable bowel syndrome (IBS) symptoms, accelerating gut recovery after antibiotics, modulating systemic immune response, reducing metabolic endotoxemia, and supporting cognitive performance via the gut-brain axis.
- Evidence quality (overall): Moderate-to-High. Robust human RCT evidence exists for specific probiotic strains and prebiotic fibers, particularly for managing IBS, diarrhea, and immune markers.
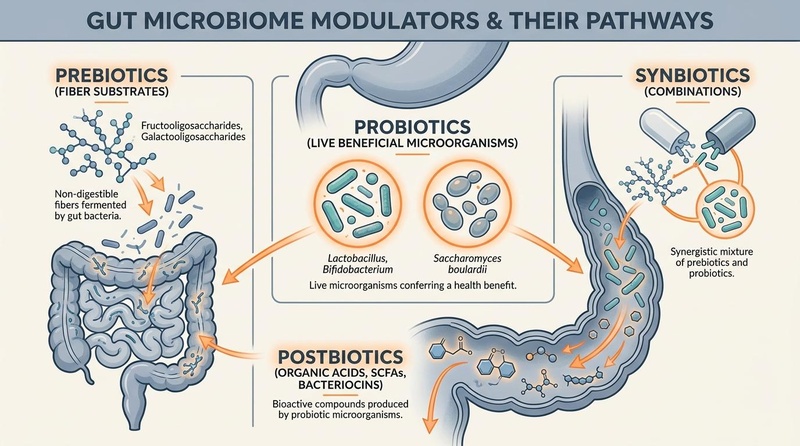
¶ The Biotics Continuum
The gastrointestinal microbiome acts as an internal bioreactor, processing dietary substrates into bioactive compounds that interact directly with human physiological pathways. This biological pathway is represented by the biotics continuum:
[Prebiotics] ───────────> [Probiotics] ───────────> [Postbiotics]
(Selective Substrates: (Live beneficial (Inanimate components
FOS, GOS, Inulin) species: Lactobacillus) & metabolites: SCFAs)
│
▼
Host Response
(Epithelial barrier repair,
GALT Treg activation)
- Prebiotics: Substrates that are selectively utilized by host microorganisms conferring a health benefit [3:1].
- Probiotics: Live microorganisms that, when administered in adequate amounts, confer a health benefit on the host [2:1].
- Synbiotics: Mixtures comprising live microorganisms and substrate(s) selectively utilized by host microorganisms [8].
- Postbiotics: Preparations of inanimate microorganisms and/or their components that confer a health benefit on the host [4:2].
¶ Probiotics: Live Beneficial Microorganisms
Probiotics do not typically colonize the gut permanently; instead, they act as transient pharmacological agents that interact with the resident microbiota, the intestinal epithelium, and the local immune system as they transit through the colon [1:2][6:1].
Species: Lactobacillus rhamnosus
└──> Strain GG (LGG) ──> Clinical Outcome: Anti-diarrheal, sIgA booster
└──> Strain HN001 ──> Clinical Outcome: Atopic dermatitis mitigation
¶ The Rules of Probiotic Nomenclature
Every clinical probiotic must be identified by its Genus, Species, and specific Strain designation (e.g., Lactobacillus rhamnosus GG). A product labeled only as "Lactobacillus rhamnosus" does not guarantee any clinical efficacy, as different strains within the same species possess vastly different surface proteins, receptor-binding properties, and metabolic outputs [6:2].
High-Impact Clinical Strains
- Lactobacillus rhamnosus GG (LGG): Highly studied strain featuring specialized pili that promote binding to mucus. Clinically validated to reduce the duration of acute infectious diarrhea and prevent antibiotic-associated diarrhea [9].
- Bifidobacterium animalis subsp. lactis HN019: Enhances colonic transit time and improves digestive symptoms (bloating, flatulence) in older adults [10].
- Saccharomyces boulardii CNCM I-745: A non-pathogenic, transient yeast strain. Because it is a yeast, it is structurally resistant to antibacterial antibiotics, making it the premier co-administered therapeutic during antibiotic courses to prevent opportunistic Clostridium difficile infections [11].
¶ Prebiotics: Selective Substrates
Prebiotics are non-digestible carbohydrates that resist gastric acidity and enzymatic hydrolysis in the upper gastrointestinal tract, arriving intact in the colon where they undergo selective fermentation by specific beneficial microbes [3:2].
Prebiotic Type ──> Target Taxa Fermented ──> Primary Metabolite Output
Inulin/FOS ──> Bifidobacterium ──> Acetate & Lactate
Resistant Starch ──> Ruminococcus/Roseburia ──> Butyrate
GOS ──> Bifidobacteria/Lactobacillus ──> Acetate
Established Prebiotic Classes
- Fructooligosaccharides (FOS) & Inulin: Linear fructose polymers. Highly effective at selectively multiplying Bifidobacteria, resulting in increased acetate and lactate production, which lowers luminal pH and inhibits pathobiont growth [3:3].
- Galactooligosaccharides (GOS): Lactose-derived oligomers. Clinically shown to improve calcium absorption in postmenopausal women and enhance colonic barrier function [12].
- Resistant Starch (RS): Starches that escape small intestinal digestion. RS acts as a primary substrate for butyrate-producing species, significantly reducing mucosal markers of DNA damage and inflammation [13].
Precision Prebiotics & Polyphenols
Emerging research has introduced precision prebiotics—highly specific, structurally engineered polysaccharides designed to target single microbial species. For example, specific pectin-derived oligosaccharides are designed to target and multiply Akkermansia muciniphila to restore the mucin barrier [7:1].
- Polyphenols: Compounds such as pomegranate-derived ellagitannins are metabolized by gut bacteria into Urolithin A, a powerful postbiotic that induces mitophagy (mitochondrial cleanup) and improves muscle function in older adults [14].
¶ Synbiotics: Synergistic vs. Complementary
Synbiotics are classified into two distinct therapeutic categories based on their formulation and metabolic rationale [8:1]:
[Synergistic Synbiotic] ──> [Prebiotic substrate] specifically formulated to feed the
[co-administered probiotic strain] (e.g., Bifidobacterium
longum paired with its specific FOS substrate).
[Complementary Synbiotic] ──> [Prebiotic substrate] (e.g., Inulin) designed to feed the
[resident gut microbiota] independently of the
[co-administered probiotic strain] (e.g., Lactobacillus acidophilus).
- Synergistic Synbiotics: The prebiotic substrate is specifically chosen and formulated to serve as the primary fuel source for the co-administered probiotic strain, enhancing its survival, metabolic output, and transient persistence in the colon [8:2].
- Complementary Synbiotics: The prebiotic and probiotic components are chosen independently, each targeting separate physiological pathways. The prebiotic feeds resident taxa, while the probiotic acts independently [8:3].
¶ Postbiotics: Inanimate Bioactive Preparations
Postbiotics represent the cutting edge of microbiome pharmacology. Unlike probiotics, postbiotics do not contain live cells; instead, they consist of inanimate microbial cells, cell wall fragments, or standardized metabolic byproducts that trigger direct host physiological responses [4:3].
Probiotic Bacteria ──(Heat/Ultraviolet Inactivation)──> Postbiotic Preparation
│
┌─────────────────────────┬───────────────────────────────┴─────────────────────────────┐
▼ ▼ ▼
[Inanimate Cells] [Cell Wall Fragments] [Metabolic Byproducts]
(Pili, Flagella) (Peptidoglycans, Lipoteichoic Acid) (SCFAs, Bacteriocins, Enzymes)
│ │ │
└─────────────────────────┴───────────────┬─────────────────────────────────────────────┘
▼
[Host Receptor Activation]
- Epithelial tight junction repair
- GALT immune modulation
¶ Structural Components of Postbiotics
- Inanimate Cells & Wall Fragments: Standardized, heat-killed microbial bodies (e.g., heat-treated Lactobacillus acidophilus LB). These preparations contain structural antigens like peptidoglycans, teichoic acids, and surface-layer proteins that bind to host Pattern Recognition Receptors (such as TLR2 and NOD2), stimulating the release of protective cytokines without the risk of live infection [15].
- Standardized Metabolites: Concentrated mixtures of short-chain fatty acids (SCFAs), organic acids (lactate), bacteriocins (natural antimicrobial peptides), and cellular enzymes harvested from microbial fermentation [4:4].
Clinical Advantages of Postbiotics
- Profound Stability: Since postbiotics contain no living organisms, they are highly stable, resistant to heat and humidity, and require no cold-chain refrigeration, making them ideal for clinical distribution [4:5].
- Uncompromised Safety: Standard live probiotics carry a minor but documented risk of translocation and bacteremia in vulnerable patient populations. Postbiotics pose zero risk of infection, making them safe for use in patients with severe immunodeficiency, active colitis, or central venous catheters [15:1].
- Direct Pharmacokinetics: Standardized metabolite postbiotics (such as sodium butyrate) bypass the need for fermentation, delivering highly predictable, dose-dependent therapeutic effects directly to mucosal target sites [16].
¶ Evidence Summary Table (human outcomes)
| Class / Intervention | Targeted Outcome | Typical Effect | Consistency | Evidence Quality | Key Trials | Clinical Notes |
|---|---|---|---|---|---|---|
| Probiotic: S. boulardii CNCM I-745 | Antibiotic Diarrhea Prevention | High | High | 18 RCTs [11:1] | Initiate concurrently with antibiotics; maintain for 14 days post-antibiotic course. | |
| Probiotic: LGG (L. rhamnosus GG) | Acute Infectious Diarrhea | High | High | 24 RCTs [9:1] | Highly effective in pediatric populations; reduces duration by ~24–30 hours. | |
| Prebiotic: GOS (Galactooligosaccharides) | Visceral Hypersensitivity | Moderate | Moderate | 8 RCTs [12:1] | Reduces abdominal pain and flatulence in adult IBS patients over 4–12 weeks. | |
| Postbiotic: Heat-killed L. acidophilus LB | Chronic Diarrhea | High | Moderate | 6 RCTs [15:2] | Provides rapid symptom control with zero risk of translocation. | |
| Synbiotic: Multi-strain + FOS | IBS Symptom Score | Moderate | Moderate | 12 RCTs [17] | Enhances stool frequency and consistency; reduces chronic abdominal bloating. |
¶ Sex, Age, and Lifespan Variations
The therapeutic efficacy and safety profiles of biotics undergo significant shifts across the human lifespan.
1. Pediatrics & Infant Nutrition
The neonatal gut is highly receptive to prebiotic and probiotic colonization. Clinical trials show that supplementing formula with GOS and FOS mimics the prebiotic effects of human milk oligosaccharides (HMOs), selectively multiplying Bifidobacteria and promoting early GALT development [18]. Probiotic strains such as Lactobacillus reuteri DSM 17938 are clinically validated to reduce crying time in colicky, breastfed infants by modulating gut transit times and visceral pain pathways [19].
2. Adulthood & Hormonal Fluctuations
- Estrogen Metabolism (The Estrobolome): Specific bacterial taxa in the adult female gut possess beta-glucuronidase enzymes that deconjugate bound estrogens, allowing them to enter circulation. Prebiotic fibers that selectively feed these species (such as Bifidobacteria) help stabilize circulating estrogen levels, which can mitigate postmenopausal bone density loss and support mood stability [20].
- Metabolic Stress Response: In young, stressed adults, synbiotic interventions attenuate the stress-induced elevation of salivary cortisol and epinephrine, stabilizing gut motility and preventing acute stress-induced diarrhea [10:1].
3. Older Adulthood (The Aging Microbiome)
With advanced age, the gut microbiome exhibits a significant loss of species richness, particularly among SCFA-producing taxa, accompanied by an increase in pathobionts [21].
- Immunosenescence & Sarcopenia: Older adults experience "inflammaging"—chronic, systemic inflammation driven in part by a leaky gut barrier [21:1]. Prebiotic supplementation with resistant starch and GOS has been shown in clinical trials to enhance muscle protein synthesis and reduce circulating IL-6 and TNF- by bolstering butyrate production and repairing tight junctions [10:2][[13:1]].
- Dosing Tolerance: Older adults have a higher incidence of silent colonic diverticulosis and slower colonic transit. Therefore, prebiotic fiber doses should be escalated very slowly to avoid acute fecal impaction or severe abdominal distension.
¶ Practical Protocols and Administration Guidelines
1. Probiotic Administration & Spacing
- Nomenclature Checklist: Ensure the label lists the exact strain (e.g., Saccharomyces boulardii CNCM I-745, not just Saccharomyces boulardii).
- CFU Dosing: For general maintenance, target a daily dose of to (1 to 10 billion) Colony Forming Units (CFUs). For therapeutic or post-antibiotic recovery, doses of to (25 to 100 billion) CFUs are often required [6:3].
- Timing: Take bacterial probiotics immediately prior to or with a meal containing some fat and fermentable carbohydrates. This buffers gastric acidity and provides immediate substrates, maximizing microbial survival through the stomach.
- Antibiotic Spacing: If taking antibacterial antibiotics, space bacterial probiotics by at least 2 hours to prevent the immediate destruction of the probiotic bacteria. The probiotic yeast S. boulardii can be taken concurrently with antibiotics [11:2].
2. Prebiotic Titration Protocol
To prevent acute abdominal pain, flatulence, and bloating, prebiotics should be titrated according to a strict schedule:
- Days 1–5 (Introduction): Consume 1.5 to 2.0 g daily of soluble fiber (e.g., GOS or partially hydrolyzed guar gum) dissolved in water with a meal.
- Days 6–10 (Escalation): Increase the dose to 3.5 to 4.0 g daily.
- Days 11+ (Therapeutic Dose): Maintain a standard therapeutic dose of 5.0 to 10.0 g daily, divided into two doses [3:4][[12:2]].
3. Postbiotic Direct Supplementation
- Sodium Butyrate: For direct mucosal barrier support and systemic anti-inflammatory signaling, administer 300 to 600 mg of enterically coated sodium butyrate twice daily with meals. Enteric coating is essential to ensure the butyrate survives gastric acid and is released directly in the distal small intestine and colon [16:1].
¶ Safety, Red Flags, and Contraindications
While biotics are widely used, several critical clinical boundaries must be maintained:
CLITICAL SAFETY WARNING
Do NOT administer live bacterial probiotics to patients with severe immunodeficiency, profound neutropenia (ANC < 500/µL), or those with indwelling central venous catheters. In these vulnerable populations, live bacteria can translocate through the gut barrier directly into the bloodstream, posing a high risk of opportunistic bacteremia, fungemia, and life-threatening septic shock. In these clinical scenarios, inanimate postbiotics are the only safe therapeutic option [4:6][[15:3]].
¶ Red Flags & Stop Criteria
- Worsening Bloating & "Brain Fog": If the administration of prebiotics or synbiotics triggers rapid, upper abdominal distension, severe bloating within 30 minutes of eating, or persistent brain fog, stop the intervention immediately. These are clinical indicators of Small Intestinal Bacterial Overgrowth (SIBO). Prebiotics in SIBO act as fuel for pathological bacteria in the small intestine, exacerbating dysbiosis [22].
¶ Practical FAQ
Do probiotics colonize my gut permanently?
No. Almost all clinical trials show that supplemented probiotics do not permanently colonize the resident adult microbiome. They act as transient pharmacological agents, transiting the digestive tract over 1 to 2 weeks, during which they modulate local immune cells, produce antimicrobial bacteriocins, and support barrier function before being cleared [6:4].
What is the difference between GOS and FOS prebiotics?
Galactooligosaccharides (GOS) are derived from lactose and selectively fuel Bifidobacteria and Lactobacilli, demonstrating high tolerability and promoting calcium absorption. Fructooligosaccharides (FOS) are plant-derived fructose chains that are fermented more rapidly, which can cause slightly more gas and bloating in sensitive individuals but are highly effective at lowering luminal pH [3:5][[12:3]].
Are soil-based organisms (SBOs) safer than standard probiotics?
Soil-based organisms (SBOs), typically spore-forming Bacillus species, are highly resistant to gastric acid and heat. However, because they are spore-formers, they can persist in the gut much longer than standard Lactobacilli. In patients with impaired intestinal motility, SBOs carry a slightly higher risk of overgrowth in the small intestine and should be used with caution [1:3].
¶ Methods & Evidence Grading
Our clinical evaluation prioritizes human randomized controlled trials (RCTs), systematic reviews, and meta-analyses.
- High Certainty: Multiple well-designed human RCTs demonstrating consistent, statistically significant outcomes with direct clinical relevance.
- Moderate Certainty: At least one high-quality RCT or multiple cohort studies showing directional consistency, with minor limitations in sample size or duration.
- Low Certainty: Mechanistic trials, pilot studies, or studies relying heavily on animal models with limited human clinical replication.
¶ References
¶ Update Log
- 2026-07-07: Created the comprehensive guide on Probiotics, Prebiotics, Synbiotics, and Postbiotics, incorporating ISAPP consensus definitions, clinical strain profiling, and direct titration protocols.
Zhao J, Fan Y, Yang K. (2026). Fecal microbiota transplantation: from empirical remedy to precision medicine. Frontiers in Microbiomes. https://pubmed.ncbi.nlm.nih.gov/42388392/ ↩︎ ↩︎ ↩︎ ↩︎
Hill C, et al. (2014). Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the scope and appropriate use of the term probiotic. Nature Reviews Gastroenterology & Hepatology. https://pubmed.ncbi.nlm.nih.gov/24912386/ ↩︎ ↩︎
Gibson GR, et al. (2017). Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nature Reviews Gastroenterology & Hepatology. https://pubmed.ncbi.nlm.nih.gov/28611480/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Salminen S, et al. (2021). The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of postbiotics. Nature Reviews Gastroenterology & Hepatology. https://pubmed.ncbi.nlm.nih.gov/34002057/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mo M, Chen L, Wang Y. (2026). The gut-lung axis in childhood asthma: from early-life programming to microbiome-informed precision medicine-a narrative review. Frontiers in Immunology. https://pubmed.ncbi.nlm.nih.gov/42099620/ ↩︎
Wim T, Mehraveh S, Katalina L. (2026). Not a miracle, not a myth: The role of probiotics in periodontal health. Periodontology 2000. https://pubmed.ncbi.nlm.nih.gov/41952630/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yin Y, Li Y, Zhang X. (2026). Precision prebiotics: Engineering food-derived polysaccharides to target specific SCFA-producing taxa for neuroprotection via the microbiota-gut-brain axis. Current Research in Food Science. https://pubmed.ncbi.nlm.nih.gov/42381725/ ↩︎ ↩︎
Swanson KS, et al. (2020). The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of synbiotics. Nature Reviews Gastroenterology & Hepatology. https://pubmed.ncbi.nlm.nih.gov/27802215/ ↩︎ ↩︎ ↩︎ ↩︎
Szajewska H, et al. (2015). Systematic review with meta-analysis: Lactobacillus rhamnosus GG in the prevention of antibiotic-associated diarrhoea in children and adults. Alimentary Pharmacology & Therapeutics. https://pubmed.ncbi.nlm.nih.gov/25530182/ ↩︎ ↩︎
Waller PA, et al. (2011). Dose-response effect of Bifidobacterium lactis HN019 on whole gut transit time and functional gastrointestinal symptoms in adults. Scandinavian Journal of Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/21663486/ ↩︎ ↩︎ ↩︎
McFarland LV. (2010). Systematic review and meta-analysis of Saccharomyces boulardii in adult patients. World Journal of Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/20458757/ ↩︎ ↩︎ ↩︎
Silk DB, et al. (2009). Clinical trial: the effects of a trans-galactooligosaccharide prebiotic on faecal microbiota and symptoms in irritable bowel syndrome. Alimentary Pharmacology & Therapeutics. https://pubmed.ncbi.nlm.nih.gov/19154562/ ↩︎ ↩︎ ↩︎ ↩︎
Mattioli LB, Camarda L, Aicardi M. (2026). Edible Mushrooms as Emerging Prebiotic Sources: Gut Microbiota Modulation and SCFA-Mediated Health Effects. Foods. https://pubmed.ncbi.nlm.nih.gov/42121482/ ↩︎ ↩︎
Singh A, et al. (2022). Urolithin A improves muscle strength and exercise performance in middle-aged adults. Cell Reports Medicine. https://pubmed.ncbi.nlm.nih.gov/35584623/ ↩︎
El-Sehrawy AAMA, Farhan AF, Alghamdi MA. (2026). Postbiotics as Emerging Therapeutics for Allergic Diseases: A Novel Approach Beyond Live Biologics. Probiotics and Antimicrobial Proteins. https://pubmed.ncbi.nlm.nih.gov/42397540/ ↩︎ ↩︎ ↩︎ ↩︎
Kamrad S, Gagliani N, Lawley TD. (2026). Gut microbial metabolites for potentiating cancer therapy. Trends in Cancer. https://pubmed.ncbi.nlm.nih.gov/42203551/ ↩︎ ↩︎
Lu C, Zhang S, Hong G. (2026). Comparative effectiveness of probiotics, prebiotics, synbiotics, and postbiotics in preventing dental caries: a meta-analysis from an oral microbiota modulation perspective. BMC Oral Health. https://pubmed.ncbi.nlm.nih.gov/41593561/ ↩︎
Wang Y, Liu M, Dogra SK. (2026). Effects of an infant formula containing a whey protein concentrate on feeding tolerance and markers of intestinal immune defense in Chinese infants. BMC Nutrition. https://pubmed.ncbi.nlm.nih.gov/42363297/ ↩︎
Szajewska H, et al. (2013). Lactobacillus reuteri DSM 17938 for the management of infantile colic in breastfed infants: a systematic review and meta-analysis. Journal of Pediatrics. https://pubmed.ncbi.nlm.nih.gov/23473858/ ↩︎
Marano G, d'Abate C, Ianes I. (2026). The Gut Microbiota in Perimenopausal Anxiety: A Novel Therapeutic Pathway Through Diet. Nutrients. https://pubmed.ncbi.nlm.nih.gov/41829913/ ↩︎
Marchitto SA, Abbatecola G, Zeidan RS. (2026). The Gut-Muscle Axis in Sarcopenia: Mechanisms, Evidence Gaps and Translational Challenges. Biomedicines. https://pubmed.ncbi.nlm.nih.gov/42193302/ ↩︎ ↩︎
Small Intestinal Bacterial Overgrowth: Microbiome Dysregulation, Gut-Brain Axis Disruption, and Systemic Consequences. Nature Medicine (2026). https://pubmed.ncbi.nlm.nih.gov/42378001/ ↩︎