¶ Prostate Cancer Screening
| Parameter | Specification |
|---|---|
| Primary Test | Serum Prostate-Specific Antigen (PSA) [1][2] |
| Secondary Biomarkers | SelectMDx, PHI, 4Kscore, ExoDx [3][4] |
| First-Line Imaging | Multiparametric MRI (mpMRI) [5][6] |
| Advanced Staging | PSMA PET/CT [7][8] |
| Definitive Diagnosis | MRI-targeted fusion biopsy (Transperineal allows antibiotic omission) [9] |
| Screening Window | Ages 55–69 (Average Risk); Ages 40–54 (High Risk) [10][11] |
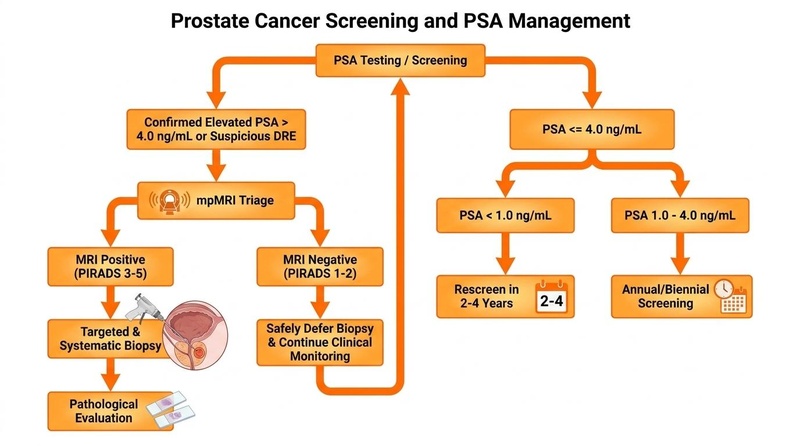
In the United States, prostate cancer remains the second leading cause of cancer-related mortality among men [2:1]. Early detection through systematic screening aims to diagnose clinically significant prostate cancer at a localized, highly curable stage, while avoiding the overdiagnosis and subsequent overtreatment of indolent disease [12]. The contemporary screening paradigm recommended by major clinical guidelines, including those of the American Urological Association (AUA 2023) and the European Association of Urology (EAU 2024), relies on a sequential, multi-modal diagnostic pathway: initiating with a baseline serum prostate-specific antigen (PSA) test, followed by secondary risk-stratification biomarkers and pre-biopsy multiparametric magnetic resonance imaging (mpMRI) to optimize the selection of candidates for definitive biopsy [5:1][6:1][13].
¶ At a Glance
¶ Key Points
- Mortality Efficacy: Systematic, PSA-based screening reduces prostate cancer-specific mortality. The European Randomized Study of Screening for Prostate Cancer (ERSPC) at a 23-year follow-up demonstrated a 13% relative risk reduction in prostate cancer deaths [14].
- The Overdiagnosis Challenge: Standard PSA-only screening is limited by low specificity, resulting in a high rate of overdiagnosis, which is estimated to range from 20% to 50% of screen-detected cancers according to Fenton 2018 [2:2]. The majority of these represent low-risk, clinically insignificant lesions (International Society of Urological Pathology [ISUP] Grade Group 1, Gleason Score 6) that do not threaten life expectancy but can lead to treatment-related harms [2:3][12:1].
- Risk-Adapted Stratification: Modern guidelines, such as EAU 2024 and AUA 2023, recommend a personalized, risk-adapted screening approach [15][13:1]. This involves determining rescreening intervals and the necessity of secondary testing based on baseline midlife PSA values (at ages 45 or 50), which serves as a powerful predictor of long-term risk [16].
- Diagnostic Optimization: Pre-biopsy mpMRI and molecular biomarkers (e.g., SelectMDx, Prostate Health Index [PHI]) significantly improve diagnostic precision [3:1][6:2]. Incorporating mpMRI into the pathway can spare up to 50% of men from undergoing an initial biopsy, which is a key clinical benefit highlighted by the AUA 2023 and EAU 2024 guidelines [5:2][6:3][13:2].
- Biopsy Safety: When a prostate biopsy is indicated, the transperineal (TP) targeted biopsy approach is clinically preferred over the transrectal (TR) approach [9:1]. TP biopsy achieves similar cancer detection rates while safely allowing the omission of prophylactic antibiotics, thereby mitigating the risk of post-procedural sepsis and multi-drug resistant infections [9:2].
¶ Clinical Significance & Efficacy
Prostate-specific antigen (PSA) is a glycoprotein enzyme secreted by the epithelial cells of the prostate gland [2:4][12:2]. While PSA is organ-specific, it is not cancer-specific; elevated serum concentrations can occur due to benign prostatic hyperplasia (BPH), prostatitis, mechanical trauma, or cellular leaks associated with malignant transformation [2:5][12:3].
The clinical utility of routine screening has historically been highly controversial, reflecting a delicate balance between absolute survival benefits and individual morbidity [1:1][12:4].
+---------------------------------------------------------+
| Baseline PSA Test |
| (Ages 40-50) |
+---------------------------------------------------------+
|
+--------------+--------------+
| |
v v
Elevated Risk Level Standard Risk Level
(PSA > 1.0-1.5 ng/mL) (PSA < 1.0 ng/mL)
| |
v v
More Frequent Screening Extended Rescreening
(Annual/Biennial + Biomarkers) (Every 2–4 Years)
¶ Absolute Mortality Reductions
Long-term data from large-scale randomized clinical trials have clarified the efficacy of screening:
- The ERSPC Trial: Enrolling 162,236 men aged 55 to 69 years, the ERSPC demonstrated a 13% relative risk reduction in prostate cancer-specific mortality in the screening group at a median follow-up of 23 years (Rate Ratio [RR], 0.87; 95% CI, 0.80 to 0.95) [14:1]. The absolute risk reduction was 0.22%, translating to a highly favorable number needed to invite (NNI) of 456 and a number needed to diagnose (NND) of 12 to prevent one prostate cancer death [14:2]. This represents a significant improvement in the harm-benefit ratio compared to the 16-year follow-up data, which reported an NNI of 628 and an NND of 18 [14:3].
- Metastasis Prevention: In addition to mortality benefits, systematic screening is highly effective in reducing the incidence of metastatic disease [17]. Long-term data from the Rotterdam arm of the ERSPC showed a 33% relative risk reduction in presenting with metastatic prostate cancer (RR, 0.67; 95% CI, 0.58 to 0.78), requiring only 121 men to be invited and 7 to be diagnosed to prevent one case of metastatic disease [17:1].
¶ The Harm of Overdiagnosis and Overtreatment
The primary argument against unselected mass screening is the high rate of overdiagnosis—the detection of slow-growing, indolent malignancies that would never have progressed to cause clinical symptoms or death during the patient's lifetime [2:6][12:5].
Systematic reviews estimate that approximately 20% to 50% of PSA-detected cancers represent overdiagnosis, with estimates varying based on cohort characteristics and screening intervals, as reported by Fenton 2018 [2:7]. The subsequent treatment of these indolent tumors (via radical prostatectomy or radiation therapy) can cause significant long-term side effects [1:2][2:8]. Based on systematic review data from Ilic 2018, the harms of PSA-based screening and subsequent diagnostic and treatment pathways include biopsy-related sepsis, persistent urinary incontinence, and erectile dysfunction [1:3]. Specifically, for every 1,000 men screened, approximately 25 additional men will experience treatment-related erectile dysfunction and 3 additional men will develop long-term urinary incontinence requiring pads, with biopsy-related infections and sepsis occurring in a subset of those undergoing diagnostic workup [1:4]. Furthermore, because prostate cancer often progresses very slowly and primarily affects older men, the majority of individuals diagnosed with screen-detected prostate cancer eventually die of other, competing non-prostate causes rather than the cancer itself [2:9][12:6].
This diagnostic reality has driven a profound clinical shift toward Active Surveillance for low-risk (ISUP Grade Group 1) localized disease under guidelines such as AUA 2023 and EAU 2024, where patients are monitored closely with serial PSA, mpMRI, and repeat biopsies, reserving radical treatment only for clear signs of progression [13:3].
¶ Screening Biomarkers
Optimal early detection requires balancing high sensitivity with a clinical focus on aggressive, clinically significant malignancies [10:1][13:4].
¶ Serum Prostate-Specific Antigen (PSA)
Serum PSA remains the foundational screening biomarker, but its test characteristics vary significantly by population:
- Symptomatic vs. Asymptomatic Accuracy: In symptomatic primary care cohorts, PSA demonstrates an estimated sensitivity of 93% and a low specificity of 20% for detecting any prostate cancer [18]. This high sensitivity makes it an excellent triaging tool, but the poor specificity leads to a high rate of false positives [18:1].
- The Free-to-Total PSA Ratio: In individuals with borderline PSA levels (typically 4.0 to 10.0 ng/mL), the free-to-total PSA ratio (percent free PSA) can help risk-stratify cases, with a lower percentage suggesting a higher likelihood of malignancy, thereby assisting clinicians in determining the necessity of further diagnostic triage or biopsy [3:2][10:2].
- Repeating PSA before Referral: In the event of an initial elevated PSA result, major guidelines such as the American Urological Association (AUA 2023) and the European Association of Urology (EAU 2024) recommend repeating the PSA measurement under stable, standardized clinical conditions before proceeding with secondary triage or urological referral, as transient elevations are common and can resolve spontaneously [10:3][13:5].
¶ Digital Rectal Examination (DRE)
Historically, DRE was universally recommended in combination with PSA for early prostate cancer detection [19][13:6]. However, contemporary high-quality evidence and major guidelines (e.g., EAU 2024) have challenged its utility, and the USPSTF (2018) does not include DRE in its routine screening recommendations [19:1][12:7][13:7]:
- Low Diagnostic Value: A systematic review and meta-analysis of primary care cohorts by Naji 2018 (PMID: 29531107) pooled prospective studies and demonstrated that DRE exhibits a pooled sensitivity of only 51% and a positive predictive value (PPV) of 41% [20]. It concluded that there is a lack of evidence supporting routine screening with DRE in the primary care setting [20:1].
- Omitting Routine DRE: An updated meta-analysis of 85,798 participants by Matsukawa 2024 (PMID: 38182488) directly compared DRE and PSA [19:2]. The study confirmed a low pooled PPV of 21% for DRE, which was not statistically different from PSA alone [19:3]. Crucially, combining DRE with PSA (PPV 19%) showed no diagnostic benefit over PSA alone [19:4]. The cancer detection rate (CDR) of DRE was significantly lower (1% vs. 3%), and combining them did not improve the CDR compared to PSA alone [19:5].
- Clinical Implications: Based on these prospective evaluations, in the absence of clinical symptoms or abnormal signs, routine DRE exhibits a notably low diagnostic value and can be safely omitted from early screening and detection algorithms under modern frameworks like EAU 2024 and AUA 2023 [19:6][13:8].
¶ Post-PSA Secondary Biomarkers
To overcome the low specificity of standard PSA screening and minimize unnecessary biopsies, several blood- and urine-based molecular biomarkers have been developed [3:3][4:1]. These secondary tests are recommended by guidelines such as EAU 2024 for patients with elevated or borderline PSA levels prior to deciding on a biopsy [3:4][21][13:9].
| Biomarker Assay | Sample Type | Key Molecular Markers Measured | Sensitivity for csPCa* | Specificity range | Clinical Utility & Diagnostic Impact |
|---|---|---|---|---|---|
| SelectMDx | Urine (Post-DRE) | DLX1 and HOXC6 mRNA expression [3:5][4:2] | 90% - 95% (Pooled range) [3:6] 57.14% (PI-RADS 3) [22] |
15% - 50% (Pooled range) [3:7] 81.82% (PI-RADS 3) [22:1] |
High Negative Predictive Value (90–95%) [4:3][22:2]. Avoids up to 53% of unnecessary biopsies while maintaining sensitive detection of GG ≥ 2 disease [4:4][22:3]. |
| Prostate Health Index (PHI) | Blood (Serum) | Total PSA, Free PSA, and [-2]proPSA (p2PSA) [3:8] |
90% - 95% (Pooled range) [3:9] | 15% - 50% (Pooled range) [3:10] | Blood-based test integrating total, free, and [-2]proPSA to calculate risk in the 4–10 ng/mL grey zone. Helps reduce unnecessary biopsies within the pooled specificity range [3:11]. |
| 4Kscore | Blood (Plasma) | Total, Free, Intact PSA, and hK2 levels [3:12] | 90% - 95% (Pooled range) [3:13] | 15% - 50% (Pooled range) [3:14] | Calculates risk of high-grade disease by combining blood kallikreins with age and clinical findings to guide biopsy decisions [3:15]. |
| ExoDx (EPI) | Urine (No DRE) | ERG, PCA3, and SPDEF exosomal RNA [3:16] | 90% - 95% (Pooled range) [3:17] | 15% - 50% (Pooled range) [3:18] | Urine test measuring exosomal RNA expression. Can be performed without a pre-test digital rectal exam, optimizing patient compliance [3:19]. |
*csPCa: Clinically Significant Prostate Cancer, defined as ISUP Grade Group ≥ 2 (Gleason Score ≥ 7).
¶ SelectMDx Molecular Profiling
SelectMDx is a highly validated, non-invasive molecular urine test that evaluates the messenger RNA (mRNA) expression of two critical genes: distal-less homeobox 1 (DLX1) and homeobox C6 (HOXC6) [22:4]. These genetic signatures are integrated with standard clinical parameters (age, PSA density, and DRE findings) via a proprietary algorithm to generate an individualized probability of finding clinically significant prostate cancer on a subsequent biopsy [22:5].
- Real-World Utility: Large clinical registry cohorts from 10 European countries confirm that SelectMDx has a significant impact on clinical decision-making [4:5]. In real-world community urology practice, approximately 40.72% of patients received a negative SelectMDx result, which has the potential to avoid unnecessary biopsies if used as a decision tool to select patients for the procedure [4:6].
- Refining Equivocal mpMRI: SelectMDx plays a vital role in managing patients with equivocal multiparametric MRI findings, specifically those with a PI-RADS 3 score [22:6]. A prospective cohort study of patients with PI-RADS 3 lesions demonstrated that a positive SelectMDx result was highly correlated with biopsy-confirmed clinically significant cancer (57.1% vs. 18.2% for negative results), providing a negative predictive value of 90% and an overall diagnostic accuracy of 77.5% [22:7]. This clinical performance can safely guide more selective biopsy strategies in patients with ambiguous imaging [22:8].
¶ Advanced Imaging: mpMRI and PSMA PET
The clinical management of elevated PSA has evolved from direct biopsy referral to a personalized, image-guided diagnostic pathway [21:1][13:10].
¶ Multiparametric MRI (mpMRI)
Pre-biopsy mpMRI is established as the gold-standard triage test for patients with suspected prostate cancer, guided by the Prostate Imaging Reporting and Data System (PI-RADS) under major frameworks like EAU 2024 and AUA 2023 [6:4][21:2][13:11]:
- The PROMIS Trial: The prospective PROMIS study demonstrated that incorporating mpMRI as a triage test prior to a first biopsy is highly cost-effective and clinically superior to the traditional "biopsy all" approach [23]. For detecting clinically significant cancer, mpMRI showed a sensitivity of 93% and a negative predictive value of 89% [23:1]. Utilizing mpMRI as a triage tool allowed 27% of men to safely avoid an unnecessary biopsy completely [23:2].
- The GÖTEBORG-2 Screening Trial: This population-based screening trial compared a systematic biopsy pathway with an MRI-targeted biopsy pathway [5:3]. At a median follow-up of 3.9 years, omitting systematic biopsies in men with negative mpMRI results and performing only targeted biopsies for suspicious lesions (PI-RADS ≥ 3) eliminated more than half of the diagnoses of clinically insignificant (ISUP Grade Group 1) cancers (Relative Risk [RR], 0.43; 95% CI, 0.32 to 0.57) [5:4]. Crucially, this reduction in overdiagnosis occurred with a very low risk of missing incurable or advanced cancers [5:5].
- Systematic Evidence Synthesis: A comprehensive meta-analysis of 80,114 men across 12 studies confirmed that sequential screening (mpMRI following an elevated PSA, utilizing a PI-RADS ≥ 3 cutoff) was associated with a dramatic 72% decrease in biopsies performed (OR, 0.28; 95% CI, 0.22 to 0.36) and a 66% reduction in the detection of insignificant cancers (OR, 0.34; 95% CI, 0.23 to 0.49) without compromising the overall detection rate of clinically significant cancer [6:5].
¶ PSMA PET/CT Staging and Diagnosis
Positron emission tomography (PET) targeting prostate-specific membrane antigen (PSMA) has emerged as a revolutionary tool in advanced diagnostics [7:1][8:1]:
- Superiority in Upfront Staging: A head-to-head meta-analysis comparing PSMA-PET to conventional imaging modalities (CT, bone scan, and pelvic MRI) for the initial staging of intermediate-to-high risk prostate cancer demonstrated that PSMA-PET significantly outperforms conventional imaging [7:2]. For pelvic nodal staging, PSMA-PET was far more sensitive and specific than conventional MRI (sensitivity 73.7% vs. 38.9%, specificity 97.5% vs. 82.6%) [7:3]. For bone metastasis, PSMA-PET achieved a sensitivity of 98.0% compared to 73.0% for bone scans, establishing its role as a first-line staging approach [7:4].
- Primary Diagnosis Limit: While PSMA-PET combined with MRI (PSMA-PET/MRI) increases the area under the curve (AUC) for diagnosing intraprostatic clinically significant cancer to 88%, its negative predictive value (NPV) is 73% for diagnosing intraprostatic clinically significant prostate cancer (csPCa) and up to 86% for pelvic lymph node invasion (LNI) staging, which remains insufficient to omit a biopsy when clinically indicated [8:2]. Current European guidelines emphasize that PSMA-PET cannot be used alone to omit pelvic lymph node dissection and should be integrated with clinical nomograms [8:3][13:12].
¶ Biopsy Strategies: Pathways & Safety
When screening tests and imaging confirm a high suspicion of clinically significant disease, a needle core biopsy is required for definitive diagnosis [24].
¶ Transperineal (TP) vs. Transrectal (TR) Biopsy
The route of access for prostate biopsy represents a major clinical safety inflection point [9:3]:
- Efficacy and Complications: A systematic review and meta-analysis of prospective randomized controlled trials (including PREVENT, ProBE-PC, and PERFECT) comparing MRI-targeted transperineal biopsy (TP-Tbx) with the transrectal approach (TR-Tbx) showed no significant differences in the detection of clinically significant (ISUP ≥ 2) or insignificant (ISUP 1) cancer [9:4]. Rates of post-procedural urinary retention, hematuria, and temporary pain were also comparable [9:5].
- The Antibiotic Stewardship Advantage: TR biopsy carries an inherent risk of introducing rectal flora into the prostate, requiring mandatory prophylactic antibiotic therapy [9:6]. In contrast, the transperineal approach passes through prepped perineal skin. The meta-analysis confirmed that TP-Tbx can safely omit prophylactic antibiotics entirely without increasing the risk of post-procedural infections, urinary tract infections, or sepsis (OR for infection, 0.8; 95% CI, 0.4 to 1.8; OR for sepsis, 0.6; 95% CI, 0.1 to 4.5) [9:7].
- Clinical Verdict: Due to the global rise in multi-drug resistant pathogens, the ability to safely perform TP biopsy without antibiotics makes it the preferred clinical standard over transrectal approaches [9:8].
¶ Evidence Summary (Human Outcomes)
The clinical outcomes and diagnostic accuracy of the modern, sequential prostate cancer screening pathway are summarized below:
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Studies*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Prostate Cancer-Specific Mortality | High | High | 5 Randomized Trials [1:5] | Long-term follow-up confirms a sustained 13% relative risk reduction in death over 23 years (ERSPC) [14:4]. | |
| All-Cause Mortality | High | High | 5 Randomized Trials [1:6] | No statistically significant difference in overall survival has been demonstrated in screening trials [14:5][1:7][25]. | |
| Detection of Clinically Significant Cancer | High | High | 12+ Cohorts & RCTs [6:6] | Integrating pre-biopsy mpMRI (PI-RADS ≥ 3) maintains or improves detection of GG ≥ 2 disease [5:6][6:7]. | |
| Reduction of Unnecessary Biopsies | High | High | 15+ Clinical Studies [3:20] | Sequential pathway using secondary biomarkers and mpMRI avoids up to 51% of invasive biopsies [6:8][21:3]. | |
| Overdiagnosis of Insignificant Cancer | High | High | Göteborg-2 Trial [5:7] | Omitting biopsy in patients with negative MRI reduces the detection of indolent ISUP 1 (Gleason 6) lesions by 57% [5:8][6:9]. | |
| Prevention of Advanced/Metastatic Disease | High | Moderate | ERSPC Rotterdam [17:2] | Systematic screening is associated with a 33% relative risk reduction in presenting with metastatic disease at diagnosis [17:3]. |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- *Compact renderer encoding:
e="[dir][mag][impact]"wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Studies: Number of randomized controlled trials, prospective cohort studies, or diagnostic validation trials.
¶ International Guidelines & Risk-Adapted Strategies
Clinical screening recommendations from major international organizations have evolved from historic mass screening to highly tailored, risk-adapted shared decision-making:
¶ Major Guidelines Comparison
| Organization | Target Age Range | Recommended Screening Interval | Recommends DRE? | Pre-Biopsy mpMRI? | Key Specific Recommendations |
|---|---|---|---|---|---|
| USPSTF (2018) [12:8] | Ages 55–69: Individualized Shared Decision-Making (Grade C) [12:9] | Individualized (typically every 1–2 years) [12:10] | No (notes lack of evidence to support routine performance) [12:11] | Not addressed in screening [12:12] | Recommends against screening in men aged ≥70 (Grade D) [12:13]. |
| ACS (2016) [26] | Ages 50–70+: Average risk starting at age 50; age 45 for high-risk (African American men, first-degree relative with PCa <65); age 40 for very high-risk (multiple first-degree relatives) [26:1]. | Every 2 years if PSA < 2.5 ng/mL; annually if PSA ≥ 2.5 ng/mL [26:2]. | Yes, offered as an option alongside PSA based on shared decision-making [26:3]. | Not addressed (historical screening guidelines focus on PSA only). | Only screen if life expectancy is >10 years; discontinue when life expectancy is <10 years [26:4]. |
| NCCN (2023) [27] | Ages 45–75: Average risk starts at age 45; age 40 for high-risk (Black ancestry, family history, or known BRCA1/2 mutations) [27:1]. | Risk-adapted: If PSA < 1.0 ng/mL, rescreen at age 50, then every 2–4 years. If PSA 1.0–3.0 ng/mL, rescreen every 1–2 years. If PSA > 3.0 ng/mL, screen annually and pursue secondary testing [27:2]. | Yes, DRE is recommended as a complementary tool to aid in PSA interpretation, but may be omitted if declined by the patient [27:3]. | Yes, strongly recommended before initial or repeat biopsy for men with elevated PSA to identify csPCa and reduce unnecessary biopsies [27:4]. | Screening should not be performed if life expectancy is <10 years. For men >75, only screen if life expectancy is >10 years and in excellent health [27:5]. |
| AUA (2023) [10:4] | Ages 55–69: Shared decision-making (Grade B) [10:5]. Ages 40–54: Screen high-risk men (Black ancestry, family history, genetic mutations) starting at age 40–45 [10:6]. | Individualized; longer screening intervals (every 2 years) are preferred over annual testing to reduce harms [10:7]. | Not recommended as a primary screening test; can be used in staging or as a secondary test in men with elevated PSA [10:8][24:1]. | Yes, recommended prior to initial and repeat biopsy to improve detection of csPCa and avoid unnecessary biopsies [24:2]. | Focuses risk evaluation on detecting clinically significant prostate cancer (ISUP Grade Group ≥ 2) and encourages online risk calculators [10:9][24:3]. Discontinue screening if life expectancy <10–15 years [10:10]. |
| EAU (2024) [13:13] | Ages 50–75: Average risk commencing at age 50 [13:14]. Ages 45–75: High-risk (Black ancestry, family history, or BRCA2 mutations) commencing at age 45 [13:15]. | Risk-adapted: If baseline PSA < 1.0 ng/mL, rescreen in 8 years (average risk) or 2 years (high risk). If baseline PSA ≥ 1.0 ng/mL, shorter intervals (e.g., every 2 years) [13:16]. | Not recommended for primary screening; used in urological physical examination and staging [13:17]. | Yes, strongly recommended as a first-line triage prior to any biopsy to reduce unnecessary biopsies by up to 50% [13:18]. | Incorporates multiparametric MRI and secondary biomarkers (such as SelectMDx, PHI) in a risk-adapted sequential pathway [21:4][13:19]. Discontinue if life expectancy is <10–15 years [13:20]. |
¶ Specific High-Risk Populations
- African American Men: Prostate cancer exhibits a higher incidence and a more aggressive phenotype in African American men [11:1]. To address this disparity, the American Urological Association (AUA 2023) recommends initiating screening discussions earlier, at ages 40 to 45, and utilizing shorter screening intervals [10:11][11:2]. Under the AUA 2023 framework, establishing a midlife baseline PSA value at age 45 is highly validated for optimizing risk stratification and determining subsequent testing frequencies [10:12][11:3]. The National Comprehensive Cancer Network (NCCN 2023) similarly supports beginning discussions and risk assessment at age 40 to 45 [27:6].
- Genetic Predisposition: Individuals carrying germline mutations in DNA repair genes, particularly BRCA2 and BRCA1, represent a high-risk cohort associated with a significantly elevated risk of aggressive, early-onset prostate cancer [16:1]. Major international guidelines, including those of the European Association of Urology (EAU 2024), support early, systematic screening discussions for this high-risk population, emphasizing the clinical value of baseline PSA testing and individualized tailoring of rescreening intervals to ensure timely therapeutic intervention [16:2][13:21].
¶ Risk-Adapted Trials: PROBASE
The ongoing German PROBASE trial (initiated in 2014) is evaluating a highly personalized, risk-adapted screening strategy to minimize overdiagnosis [16:3][15:1]:
- Trial Design: Enrolling tens of thousands of men, PROBASE randomizes participants at age 45 to either immediate PSA screening or delayed screening starting at age 50 [16:4].
- Risk-Adapted Intervals: Based on the baseline PSA level at age 45, men are stratified into three distinct risk tiers, where rescreening intervals are customized to minimize overdiagnosis [16:5]:
- Low-Risk Tier: Comprising 89.18% of the cohort, these low-risk participants are assigned to an extended, long-term rescreening interval [16:6].
- Intermediate-Risk Tier: Comprising 9.32% of the cohort, these intermediate-risk participants undergo rescreening at a shorter interval [16:7].
- High-Risk Tier: Comprising 1.48% of the cohort, these high-risk participants are referred for immediate confirmatory testing, secondary biomarkers, and pre-biopsy mpMRI [16:8].
- Interim Findings: This risk-adapted protocol has demonstrated a profound reduction in unnecessary biopsies and the overdiagnosis of clinically insignificant disease, providing a clinical model for modern population-based screening [15:2][13:22].
¶ Safety & Clinical Considerations
¶ Systemic Risks of Advanced Therapies
For patients diagnosed with advanced or metastatic prostate cancer, treatment decisions significantly impact long-term systemic health [28]:
- Cardiovascular Risks of ARSIs: The introduction of novel androgen receptor signaling inhibitors (ARSIs, including abiraterone, apalutamide, darolutamide, and enzalutamide) has transformed the treatment landscape of advanced and metastatic prostate cancer [28:1]. However, a comprehensive meta-analysis of 22,166 patients demonstrated that the addition of ARSIs to standard androgen deprivation therapy (ADT) is associated with an increased risk of cardiovascular events across the disease spectrum [28:2]. Adding ARSIs to traditional ADT is associated with an increased risk of all-grade cardiovascular events (RR, 1.75) and grade 3 or higher events (RR, 2.10), including severe hypertension (RR, 2.25), acute coronary syndrome (RR, 1.93), cardiac dysrhythmia (RR, 1.64), and cardiovascular death (RR, 2.02) [28:3]. Standard clinical guidelines suggest that patients should be advised about and monitored for the potential of increased cardiovascular events upon initiating ARSI therapy [28:4].
¶ FAQ
¶ What is the role of the SelectMDx test in prostate cancer screening?
SelectMDx is a non-invasive, urine-based molecular biomarker test performed after a digital rectal exam [3:21][4:7]. It measures the mRNA expression of two genes (DLX1 and HOXC6) associated with aggressive prostate cancer [22:9]. When combined with clinical factors (age, PSA density, DRE), it calculates the risk of finding clinically significant (ISUP Grade Group ≥ 2) cancer on a subsequent biopsy [22:10]. Because of its high negative predictive value (90–95%), a negative SelectMDx result allows men with elevated PSA to safely avoid a biopsy, reducing unnecessary procedures by up to 53% [4:8][22:11].
¶ Why is pre-biopsy multiparametric MRI (mpMRI) considered a game-changer?
Historically, men with elevated PSA went straight to systematic, blind transrectal ultrasound-guided biopsies, which often missed aggressive tumors and overdiagnosed harmless, indolent ones [23:3]. Pre-biopsy mpMRI (PI-RADS scoring) visualizes suspicious lesions, allowing for targeted fusion biopsies [5:9][21:5]. In major clinical trials (PROMIS, GÖTEBORG-2), using mpMRI as a triage test allowed more than 25% of men with negative MRI results to safely avoid a biopsy completely, while reducing the overdiagnosis of clinically insignificant (ISUP 1) disease by more than 50% without missing aggressive cancers [23:4][5:10][6:10].
¶ How does the transperineal biopsy approach compare to the transrectal approach?
A transperineal (TP) biopsy accesses the prostate through prepped perineal skin, whereas a transrectal (TR) biopsy passes through the rectum, introducing a higher risk of bacterial contamination [9:9]. Meta-analyses of randomized trials show that both approaches have identical cancer detection rates, but TP biopsy is significantly safer because it can be performed without prophylactic antibiotics [9:10]. TP biopsy does not increase the risk of post-procedural infection or sepsis, making it the preferred clinical approach to mitigate antibiotic resistance [9:11].
¶ What is a risk-adapted screening strategy?
A risk-adapted screening strategy adjusts the frequency of testing and subsequent diagnostics based on an individual's baseline midlife PSA level (measured at ages 40 to 45 or 50) and genetic risk factors [16:9][13:23]. As demonstrated in the German PROBASE trial, men in the low-risk baseline PSA category at age 45 (representing 89.18% of the cohort) have an extremely low long-term risk of aggressive cancer and are assigned to an extended rescreening interval [16:10]. Conversely, men with higher baseline values receive more frequent (annual or biennial) screening, maximizing early detection while preventing overdiagnosis in low-risk individuals [16:11][15:3].
¶ References
Ilic D, Djulbegovic M, Jung JH, et al. Prostate cancer screening with prostate-specific antigen (PSA) test: a systematic review and meta-analysis. BMJ. 2018;362:k3581. https://pubmed.ncbi.nlm.nih.gov/30185521/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fenton JJ, Weyrich MS, Durbin S, et al. Prostate-Specific Antigen-Based Screening for Prostate Cancer: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2018;319(18):1914-1931. https://pubmed.ncbi.nlm.nih.gov/29801018/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Robinson HS, Lee SS, Barocas DA. Evaluation of blood and urine based biomarkers for detection of clinically-significant prostate cancer. Prostate Cancer and Prostatic Diseases. 2025;28(1):45-53. https://pubmed.ncbi.nlm.nih.gov/38858447/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Visser WCH, de Jong H, Steyaert S, et al. Clinical use of the mRNA urinary biomarker SelectMDx test for prostate cancer. Prostate Cancer and Prostatic Diseases. 2022;25(3):524-531. https://pubmed.ncbi.nlm.nih.gov/35810263/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hugosson J, Godtman RA, Wallstrom J, et al. Results after Four Years of Screening for Prostate Cancer with PSA and MRI. The New England Journal of Medicine. 2024;391(12):1103-1112. https://pubmed.ncbi.nlm.nih.gov/39321360/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fazekas T, Shim SR, Basile G, et al. Magnetic Resonance Imaging in Prostate Cancer Screening: A Systematic Review and Meta-Analysis. JAMA Oncology. 2024;10(6):745-754. https://pubmed.ncbi.nlm.nih.gov/38576242/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chow KM, So WZ, Lee HJ, et al. Head-to-head Comparison of the Diagnostic Accuracy of Prostate-specific Membrane Antigen Positron Emission Tomography and Conventional Imaging Modalities for Initial Staging of Intermediate- to High-risk Prostate Cancer: A Systematic Review and Meta-analysis. European Urology. 2023;84(1):45-55. https://pubmed.ncbi.nlm.nih.gov/37032189/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mazzone E, Cannoletta D, Quarta L, et al. A Comprehensive Systematic Review and Meta-analysis of the Role of Prostate-specific Membrane Antigen Positron Emission Tomography for Prostate Cancer Diagnosis and Primary Staging before Definitive Treatment. European Urology. 2025;87(6):789-801. https://pubmed.ncbi.nlm.nih.gov/40155242/ ↩︎ ↩︎ ↩︎ ↩︎
Zattoni F, Rajwa P, Miszczyk M, et al. Transperineal Versus Transrectal Magnetic Resonance Imaging-targeted Prostate Biopsy: A Systematic Review and Meta-analysis of Prospective Studies. European Urology Oncology. 2024;7(6):890-898. https://pubmed.ncbi.nlm.nih.gov/39095298/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wei JT, Barocas D, Carlsson S, et al. Early Detection of Prostate Cancer: AUA/SUO Guideline Part I: Prostate Cancer Screening. The Journal of Urology. 2023;210(1):46-53. https://pubmed.ncbi.nlm.nih.gov/37096582/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kensler KH, Johnson R, Morley F, et al. Prostate cancer screening in African American men: a review of the evidence. Journal of the National Cancer Institute. 2024;116(1):11-19. https://pubmed.ncbi.nlm.nih.gov/37713266/ ↩︎ ↩︎ ↩︎ ↩︎
US Preventive Services Task Force. Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;319(18):1901-1913. https://pubmed.ncbi.nlm.nih.gov/29801017/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cornford P, van den Bergh RCN, Briers E, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines on Prostate Cancer-2024 Update. Part I: Screening, Diagnosis, and Local Treatment with Curative Intent. European Urology. 2024;86(2):148-163. https://pubmed.ncbi.nlm.nih.gov/38614820/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Roobol MJ, de Vos II, Månsson M, et al. European Study of Prostate Cancer Screening - 23-Year Follow-up. The New England Journal of Medicine. 2025;393(18):1701-1710. https://pubmed.ncbi.nlm.nih.gov/41160819/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Albers P, Becker N. (Prostate cancer screening? Only evidence-based, risk-adjusted, and organized!). Bundesgesundheitsblatt. 2024;67(9):1001-1008. https://pubmed.ncbi.nlm.nih.gov/39102055/ ↩︎ ↩︎ ↩︎ ↩︎
Al-Monajjed R, Arsov C, Albers P. (Risk-adapted prostate cancer screening-update 2021). Der Urologe. Ausg. A. 2021;60(5):589-596. https://pubmed.ncbi.nlm.nih.gov/33792743/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
de Vos II, Meertens A, Hogenhout R, et al. A Detailed Evaluation of the Effect of Prostate-specific Antigen-based Screening on Morbidity and Mortality of Prostate Cancer: 21-year Follow-up Results of the Rotterdam Section of the European Randomised Study of Screening for Prostate Cancer. European Urology. 2023;84(4):420-428. https://pubmed.ncbi.nlm.nih.gov/37029074/ ↩︎ ↩︎ ↩︎ ↩︎
Merriel SWD, Pocock L, Gilbert E, et al. Systematic review and meta-analysis of the diagnostic accuracy of prostate-specific antigen (PSA) for the detection of prostate cancer in symptomatic patients. BMC Medicine. 2022;20:55. https://pubmed.ncbi.nlm.nih.gov/35125113/ ↩︎ ↩︎
Matsukawa A, Yanagisawa T, Bekku K, et al. Comparing the Performance of Digital Rectal Examination and Prostate-specific Antigen as a Screening Test for Prostate Cancer: A Systematic Review and Meta-analysis. European Urology Oncology. 2024;7(4):780-788. https://pubmed.ncbi.nlm.nih.gov/38182488/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Naji L, Randhawa H, Sohani Z, et al. Digital Rectal Examination for Prostate Cancer Screening in Primary Care: A Systematic Review and Meta-Analysis. Annals of Family Medicine. 2018;16(2):149-154. https://pubmed.ncbi.nlm.nih.gov/29531107/ ↩︎ ↩︎
Soeterik TFW, Wu X, Van den Bergh RCN. Personalised Prostate Cancer Diagnosis: Evaluating Biomarker-based Approaches to Reduce Unnecessary Magnetic Resonance Imaging and Biopsy Procedures. European Urology Open Science. 2025;75:10-18. https://pubmed.ncbi.nlm.nih.gov/40291786/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Călinoiu PC, Bădescu DL, Nechita OC, et al. Refining the Management of Prostate Imaging Reporting Category 3 Lesions through SelectMDx Urinary Biomarker Evaluation. Maedica. 2025;20(2):210-218. https://pubmed.ncbi.nlm.nih.gov/40880692/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Brown LC, Ahmed HU, Faria R, et al. Multiparametric MRI to improve detection of prostate cancer compared with transrectal ultrasound-guided prostate biopsy alone: the PROMIS study. Health Technology Assessment. 2018;22(39):1-176. https://pubmed.ncbi.nlm.nih.gov/30040065/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wei JT, Barocas D, Carlsson S, et al. Early Detection of Prostate Cancer: AUA/SUO Guideline Part II: Considerations for a Prostate Biopsy. The Journal of Urology. 2023;210(1):54-63. https://pubmed.ncbi.nlm.nih.gov/37096575/ ↩︎ ↩︎ ↩︎ ↩︎
Bretthauer M, Wieszczy P, Løberg M, et al. Estimated Lifetime Gained With Cancer Screening Tests: A Meta-Analysis of Randomized Clinical Trials. JAMA Internal Medicine. 2023;183(11):1190-1197. https://pubmed.ncbi.nlm.nih.gov/37639247/ ↩︎
Smith RA, Andrews KS, Brooks D, et al. Cancer screening in the United States, 2016: A review of current American Cancer Society guidelines and current issues in cancer screening. CA: A Cancer Journal for Clinicians. 2016;66(2):95-117. https://pubmed.ncbi.nlm.nih.gov/26797525/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Moses KA, Sprenkle PC, Bahler C, et al. NCCN Guidelines® Insights: Prostate Cancer Early Detection, Version 1.2023. Journal of the National Comprehensive Cancer Network. 2023;21(3):236-243. https://pubmed.ncbi.nlm.nih.gov/36898362/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
El-Taji O, Taktak S, Jones C, et al. Cardiovascular Events and Androgen Receptor Signaling Inhibitors in Advanced Prostate Cancer: A Systematic Review and Meta-Analysis. JAMA Oncology. 2024;10(7):880-889. https://pubmed.ncbi.nlm.nih.gov/38842801/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎