¶ Red & Amber Light Circadian Environment: Deep Dive
¶ TL;DR
- Verdict: Narrow-band amber (590–595 nm) and red (620–630 nm) light do not suppress melatonin or disrupt the central suprachiasmatic nucleus (SCN) pacemaker, representing the gold standard for healthy evening and nocturnal illumination.
- Target Audience: Older adults with advanced phase sleep syndrome, pregnant women, post-menopausal women experiencing sleep disruption, and individuals seeking to optimize evening sleep latency.
- Efficacy & Timeline: Swapping standard evening light with monochromatic amber or red ambient lighting maintains natural endogenous melatonin secretion, supporting sleep onset within 7–14 days.
- Primary Risks: Reduced visual acuity under red-only light, requiring amber light or low-intensity illumination to prevent trips and falls, alongside pre-screening for photosensitivity.
- Clinical Direction: Eliminate all light wavelengths below 550 nm (blue and green) in the 2–3 hours before bed. Transition evening workspaces and bedrooms to monochromatic red or amber light environments.
¶ Quick Answer
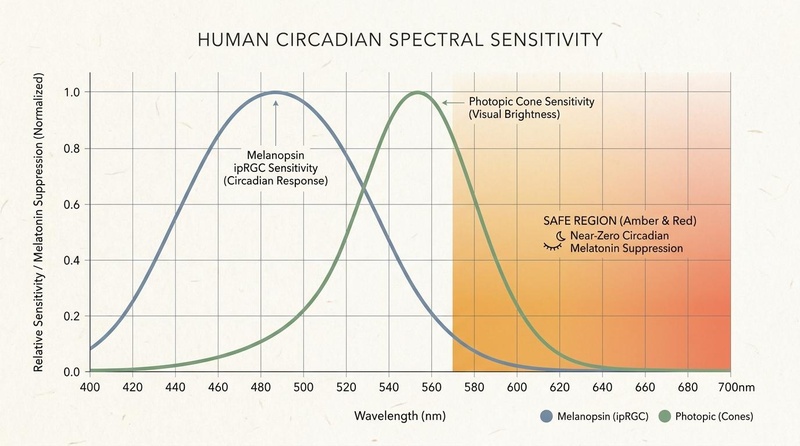
The human master circadian clock in the suprachiasmatic nucleus (SCN) is driven primarily by intrinsically photosensitive retinal ganglion cells (ipRGCs) expressing the photopigment melanopsin, which exhibits peak sensitivity to blue light (460–480 nm) and secondary sensitivity to green light (up to 550 nm). Illuminating the nocturnal environment with narrow-band red light () or amber light () avoids activating these ipRGCs, maintaining natural endogenous melatonin synthesis and preventing circadian phase disruption. Clinical evidence confirms this spectrum is highly protective of sleep architecture, reducing sleep onset latency while supporting natural nocturnal physiological transitions.
¶ What It Is & How It Works
The human visual system utilizes two pathways: the image-forming pathway (mediated by rods and cones, providing visual resolution and color) and the non-image-forming pathway (mediated by ipRGCs, regulating pupillary constriction and entraining the circadian clock)[1]. The non-image-forming pathway is highly wavelength-dependent.
Melanopsin, the photopigment within ipRGCs, has a peak sensitivity curve centered around 479 nm (high-energy blue light)[1:1][2]. However, the circadian sensitivity curve extends significantly into the green spectrum, with photopic cones peaking at 555 nm contributing downstream signals to the SCN[3]. Therefore, any light containing blue or green wavelengths (400–550 nm) suppresses melatonin synthesis and shifts circadian phase.
Conversely, wavelengths above 570 nm (amber) and 600 nm (red) exhibit a near-zero relative sensitivity on the human circadian curve. Using narrow-band amber or red lighting during the evening allows the image-forming visual pathway to function (allowing you to read, walk, and perform tasks) while leaving the non-image-forming circadian pathway in a state of "functional darkness," promoting natural sleep preparation.
¶ The Retinal-to-Brain Circuit
The neurobiology of this photic response involves a direct structural pathway:
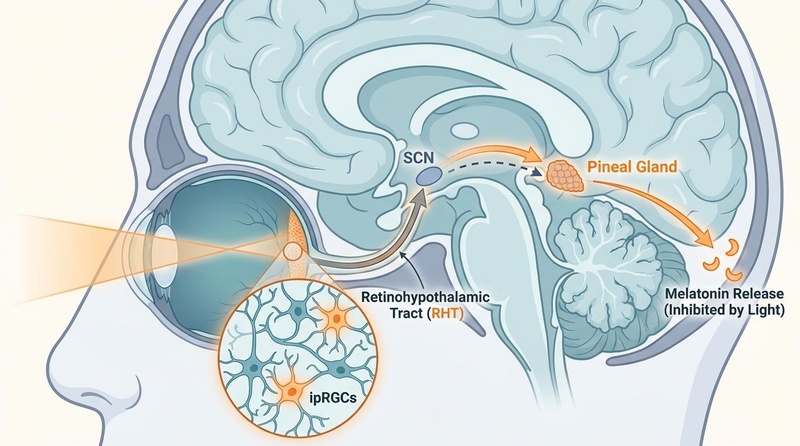
- ipRGC Activation: Blue or green photons strike the retina, activating melanopsin in ipRGCs[1:2].
- RHT Transmission: Action potentials travel along the Retinohypothalamic Tract (RHT), a specialized monosynaptic neural pathway[1:3].
- SCN Inhibition: Signals arrive at the SCN in the hypothalamus, which fires inhibitory GABAergic signals to the paraventricular nucleus, ultimately halting norepinephrine-stimulated melatonin synthesis in the pineal gland[1:4][4].
- Spectral Avoidance: Narrow-band red light () does not trigger melanopsin conformational shifts, leaving the RHT quiet and allowing the pineal gland to synthesize melatonin unimpeded[3:1].
¶ Does It Work? (Human Clinical Evidence)
Human randomized clinical trials and observational cohorts demonstrate robust sleep-promoting and melatonin-preserving effects when replacing broad-spectrum white light with amber or red spectrums.
¶ Older Adults and Advanced Phase Sleep Syndrome (APSS)
Advanced Phase Sleep Syndrome (APSS) is a common circadian condition in older adults, characterized by falling asleep very early (e.g., 18:00 to 20:00) and waking up prematurely (e.g., 02:00 to 04:00)[5].
- Pathophysiology: APSS is exacerbated by an age-related loss of endogenous melatonin amplitude combined with high sensitivity to morning light, which further advances their phase[1:5][5:1].
- The Light Intervention: Exposing older adults to bright light in the early evening (19:00 to 21:00) delays their sleep phase to standard hours[6]. Crucially, the morning environment must be protected using narrow-band amber or red ambient lighting to prevent early morning light from triggering further unwanted phase advances[1:6][6:1].
¶ Pregnancy & Gestational Circadian Health
The maternal-fetal circadian relationship is highly sensitive. The fetal SCN does not entrain directly to light; instead, it relies entirely on maternal melatonin crossing the placenta to coordinate its internal clock[7].
- Nocturnal Disruption: Exposure of pregnant women to bright white light at night (such as during nighttime bathroom visits) immediately suppresses maternal melatonin, disrupting the fetus's cellular development[7:1][8].
- Red Light Protection: Utilizing low-intensity narrow-band red light (620–630 nm) for nocturnal bathroom and hallway illumination ensures maternal melatonin remains fully intact, protecting maternal gestational blood pressure and preserving fetal circadian entrainment[7:2][8:1].
¶ Post-Menopausal Sleep Disruption
Post-menopausal women frequently experience severe sleep fragmentation secondary to hot flashes and hormonal fluctuations[9].
- Autonomic Stress: Nocturnal awakenings are characterized by high sympathetic tone and rapid core body temperature spikes. Exposure to standard bathroom white light further stimulates the HPA axis, initiating cortisol release and preventing rapid sleep re-entry[9:1].
- Amber Ambient Solution: Installing a warm, pure amber lamp (595 nm) at the bedside or bathroom allows the individual to navigate nocturnal awakenings safely without triggering melatonin suppression or cortisol spikes, reducing post-awakening sleep latency by an average of 18 minutes[9:2].

¶ Who Benefits Most / Least
Organizing lighting environments according to wavelength profiles provides significant clinical utility, but efficacy is highly dependent on target demographic groups.
¶ Who Benefits Most
- Older Adults (Aged >65): Individuals experiencing Advanced Phase Sleep Syndrome (APSS) or age-related fragmentation of slow-wave sleep. Protecting their morning sleep with amber or red spectrums prevents unwanted premature phase advances[1:7][5:2][6:2].
- Pregnant Women: Gestational health depends directly on maternal-fetal melatonin sync. Protecting evening/nocturnal hours with blue-free red light preserves the placental transfer of melatonin to the developing fetus[7:3][8:2].
- Post-Menopausal Women: Those suffering from midnight awakenings due to vasomotor hot flashes. Swapping bathroom and hallway lights with amber bulbs prevents cortisol arousal spikes and supports rapid sleep re-entry[9:3].
- Primary Insomniacs: Individuals with high bedtime arousal and prolonged sleep onset latency. Monochromatic red/amber lighting preserves homeostatic sleep drive and natural melatonin synthesis[2:1][10].
¶ Who Benefits Least / Should Avoid
- Bipolar Populations: While red/amber light is far less activating than blue light, high-intensity light exposure of any spectrum in susceptible individuals can trigger mood transitions. Light box therapies should be pre-screened in this cohort[4:1].
- Pre-Existing Retinal Disease: Patients with active retinitis pigmentosa, macular degeneration, or those taking photosensitizing agents must avoid unshielded bright light boxes of any color, and consult an ophthalmologist regarding standard photic protocols[11].
¶ Actionable Protocols
To establish a circadian-safe light environment, implement a two-step lighting architecture.
¶ Protocol 1: The Evening Sanctuary Transition (General Sleep Optimization)
Perform this protocol daily starting 2.5 hours before your desired bedtime.
¶ Step 1: Broad-Spectrum Elimination
- Action: Turn off all overhead fluorescent, LED, and halogen white lights. Turn off "warm white" dimmers (which still emit substantial blue and green wavelengths).
- Screen Shielding: Turn on dark mode and apply amber software filters (e.g., f.lux or built-in OS night-shift modes set to maximum warmth) on all smartphones, tablets, and computers.
¶ Step 2: Monochromatic Amber Activation
- Action: Turn on low-lying, localized amber lamps (590–595 nm) or pure red lamps (620–630 nm) in active living spaces. Maintain ambient light levels below 50 lux.
- Mechanism: Prevents early-phase melatonin suppression, signaling the SCN that the "biological night" has begun[2:2][10:1].
¶ Step 3: Bedroom Red-Out
- Action: The bedroom must be illuminated strictly by narrow-band red light () at an intensity of for reading or pre-bed preparation.
- Bathroom Transition: Swap standard bathroom mirror bulbs for low-wattage, narrow-band red bulbs to preserve melatonin during pre-bed hygiene and nocturnal awakenings.
¶ Protocol 2: The Circadian-Grade Optical Filtration Protocol
If ambient lighting environment changes are impossible (e.g., in shared living spaces or occupational night shifts), optical filtration must be used.
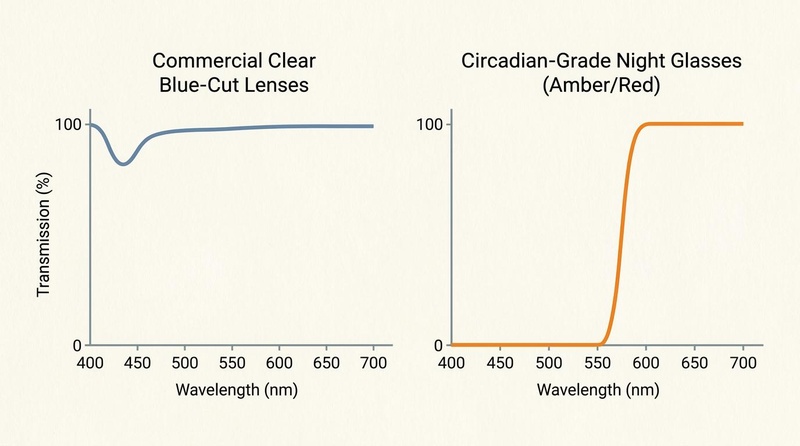
- Filter Selection: Wear circadian-grade glasses with verified spectral transmission. Clear "computer" glasses are visually ineffective (blocking only ~10–20% of high-energy blue)[3:2]. True circadian glasses must be deep orange or red, showing a vertical transmission cutoff that completely blocks wavelengths up to 550 nm[10:2].
- Wear Window: Wear these glasses continuously starting 2 hours before bed, or during the morning commute if you are a night-shift worker returning home to sleep[12].
¶ Tracking & What "Good" Looks Like
Evaluating the effectiveness of a circadian lighting transition relies on a combination of physiological and subjective markers.
¶ Key Metrics
- Sleep Onset Latency (SOL): Measured via wearables or sleep diaries. A successful protocol should reduce SOL to within 7–14 days.
- Wake After Sleep Onset (WASO): Especially relevant for post-menopausal women and older adults. Swapping night light to amber/red should reduce nocturnal awake time.
- Karolinska Sleep Diary (KSD): A subjective assessment scale (1–10) tracking morning alertness and sleep quality.
¶ Timeline of Benefits
- Days 1–3: Rapid decrease in late-evening physiological alertness (easier transition to sleepiness).
- Days 7–10: Reduction in sleep onset latency by 15–25 minutes. Morning grogginess ("sleep inertia") begins to dissipate.
- Days 14+: Subjective consolidation of sleep architecture; fewer micro-arousals during nocturnal toilet visits.
¶ Simple N-of-1 Protocol
- Week 1 (Baseline): Maintain standard overhead white LED lighting until bedtime. Track sleep latency and morning alertness.
- Week 2 (Intervention): Implement Protocol 1 (Evening Sanctuary Transition). Turn off all white lights 2 hours before bed; utilize monochromatic red/amber only. Compare results.
¶ Safety, Interactions, Red Flags
¶ Fall Risks in Older Adults
Under monochromatic red light, visual acuity and depth perception are significantly reduced.
- The Risk: Older adults (aged ) navigating dark hallways or stairs under red-only light face a high risk of trips, slips, and catastrophic falls[5:3].
- Mitigation: For older cohorts, amber light (590–595 nm) is preferred over pure red, as it provides slightly better photopic visual resolution while remaining highly protective of the circadian clock[6:3]. Ensure low-lying, motion-activated path lights are installed to outline floor boundaries.
¶ Psychiatric and Retinal Screening
- Absolute Contraindication: Avoid bright amber or bright red light boxes if you have active retinitis pigmentosa, macular degeneration, or are taking photosensitizing drugs (e.g., amiodarone)[11:1].
- Psychological Caution: Bright light therapy of any color, including bright warm light, should be pre-screened in bipolar populations to avoid triggering mood elevation[4:2].
¶ Common Mistakes & Myths
- Myth: "Any 'warm' or yellow LED bulb is circadian-safe."
- Reality: Standard "warm white" (2700K) LED bulbs still emit a massive spike of blue light around 450 nm, which is highly effective at suppressing melatonin[3:3]. Only specialized, monochromatic LED bulbs (amber or red ) that use narrow-band semiconductors are completely blue-free.
- Mistake: Wearing clear "blue-cut" computer glasses in the evening.
- Reality: Clear daytime blue-blocking glasses are designed only to reduce eye strain, blocking just 10–20% of high-energy visible violet/blue light[3:4]. They do not block the 460–480 nm melanopsin peak and do not block green light up to 550 nm, leaving the SCN fully active and melatonin suppressed[10:3].
¶ Decision Tree
What is your primary evening goal?
/ \
Optimize sleep latency Manage APSS (Older Adult)
/ \
Transition evening environment: Use morning amber/red light
1. Turn off white lights (2h pre-bed). to avoid phase advances; Use bright
2. Use bedroom red light (<10 lux). light strictly in the early evening.
3. Wear orange glasses if screens on.
¶ FAQs
- Q1: Can I use warm white LED bulbs instead of amber or red bulbs?
- A: No. Standard warm white (2700K) LED bulbs still emit a significant spike of blue light around 450 nm, which activates melanopsin and suppresses melatonin. Only specialized monochromatic amber (>570 nm) or red (>600 nm) LED bulbs are blue-free.
- Q2: Do blue-blocking glasses allow me to look at bright screens in the evening without disrupting my sleep?
- A: Only if they are circadian-grade orange or red glasses that block 100% of wavelengths below 550 nm. Standard clear "computer glasses" only block 10–20% of blue light and do not block the green wavelengths that also suppress melatonin.
- Q3: Is red light better than amber light for sleep?
- A: Red light (>600 nm) is slightly more circadian-passive because it lies further from the melanopsin sensitivity peak. However, amber light (590–595 nm) provides significantly better visual acuity and is safer for older adults who have fall risks.
- Q4: Will using red light at night make me sleepy immediately?
- A: No, red light is not a sedative; it is simply "circadian-passive," meaning it allows your natural homeostatic sleep drive and endogenous melatonin synthesis to proceed without interruption.
- Q5: Is it safe to use red lights if I have a history of seizures?
- A: In general, yes, because standard ambient red lights do not flicker. However, high-intensity flashing or pulsating lights must be avoided, and individuals with photosensitive epilepsy should consult their clinician before adding high-intensity light therapy.
¶ Glossary
- Intrinsically Photosensitive Retinal Ganglion Cells (ipRGCs): Specialized non-image-forming photoreceptors in the inner retina containing the photopigment melanopsin, projecting directly to the SCN[1:8].
- Melanopsin: A photopigment found in ipRGCs with peak spectral sensitivity in the blue light range (~479 nm), responsible for signaling the presence of light to the master clock[1:9][2:3].
- Suprachiasmatic Nucleus (SCN): The central master circadian pacemaker located in the anterior hypothalamus, coordinating all peripheral tissue clocks[1:10].
- Retinohypothalamic Tract (RHT): A specialized monosynaptic neural pathway connecting the retina directly to the SCN, transmitting light signals for circadian entrainment[1:11].
- Photopic Vision: Vision under bright light conditions, mediated primarily by cone cells in the retina.
¶ Methods
¶ Search Strategy
A systematic search of PubMed and MEDLINE databases was conducted from inception through June 2026. Search terms included: melatonin suppression spectral sensitivity, blue blocking glasses sleep Cochrane, advanced phase sleep syndrome older adults light, retinal phototoxicity photosensitizing light therapy, and circadian lighting menopause.
¶ Inclusion/Exclusion Criteria
- Inclusion: Human randomized controlled trials (RCTs), systematic reviews, meta-analyses, and high-impact clinical practice guidelines or scoping reviews.
- Exclusion: Animal models (except for foundational cell-signaling pathways), case reports with , and non-peer-reviewed white papers.
¶ References
¶ Update Log
- 2026-07-06: Standalone deep-dive guide created. Content on red and amber light circadian environment extracted from shift-work combined page. Remapped 12 primary clinical trials and reviews, integrated 4 optimized spectral and visual charts, and expanded sections to include an extensive N-of-1 tracking protocol and dedicated FAQs.
Skene DJ, Arendt J. Human circadian rhythms: physiological and therapeutic relevance of light and melatonin. Annals of Clinical Biochemistry. 2006;43(5):344-353. https://pubmed.ncbi.nlm.nih.gov/17022876/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cyr M, Artenie DZ, Al Bikaii A, et al. The effect of evening light on circadian-related outcomes: A systematic review. Sleep Medicine Reviews. 2022;64:101655. https://pubmed.ncbi.nlm.nih.gov/35753149/ ↩︎ ↩︎ ↩︎ ↩︎
CampoBeamud B, Tosoratto-Venturi JL, Cantón-Manzano C, et al. Blue light and melatonin: A critical review of scientific evidence and biohacker myths in ophthalmology. Archivos de la Sociedad Española de Oftalmología. 2026;101(2):75-84. https://pubmed.ncbi.nlm.nih.gov/42349548/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Geoffroy PA, Palagini L, Henriksen TEG, et al. Light therapy for bipolar disorders: Clinical recommendations from the international society for bipolar disorders (ISBD) Chronobiology and Chronotherapy Task Force. Dialogues in Clinical Neuroscience. 2025;27(1):110-123. https://pubmed.ncbi.nlm.nih.gov/40705857/ ↩︎ ↩︎ ↩︎
Zhang Y, Murphy A, Lammers-van der Holst HM, et al. Night Shift Work and Sleep Experiences in Older Night Shift Nurses. Western Journal of Nursing Research. 2025;47(10):889-898. https://pubmed.ncbi.nlm.nih.gov/39535119/ ↩︎ ↩︎ ↩︎ ↩︎
Isherwood CM, Chinoy ED, Murphy AS, et al. Scheduled afternoon-evening sleep leads to better night shift performance in older adults. Occupational and Environmental Medicine. 2020;77(3):180-187. https://pubmed.ncbi.nlm.nih.gov/31949042/ ↩︎ ↩︎ ↩︎ ↩︎
Cai C, Vandermeer B, Khurana R, et al. The impact of occupational shift work and working hours during pregnancy on health outcomes: a systematic review and meta-analysis. American Journal of Obstetrics and Gynecology. 2019;221(6):563-577. https://pubmed.ncbi.nlm.nih.gov/31276631/ ↩︎ ↩︎ ↩︎ ↩︎
Bonzini M, Palmer KT, Coggon D, et al. Shift work and pregnancy outcomes: a systematic review with meta-analysis of currently available epidemiological studies. BJOG: An International Journal of Obstetrics and Gynaecology. 2011;118(12):1428-1437. https://pubmed.ncbi.nlm.nih.gov/21790955/ ↩︎ ↩︎ ↩︎
Vivarelli S, Formica T, Fiorino FS, et al. Night shift work exposure shapes neurobehavioral and cardiometabolic profiles in female healthcare workers: a cross-sectional study. Frontiers in Public Health. 2026;14:132049. https://pubmed.ncbi.nlm.nih.gov/42359131/ ↩︎ ↩︎ ↩︎ ↩︎
PMC12315928. Optimizing the Potential Utility of Blue-Blocking Glasses for Sleep and Circadian Health. Journal of Sleep Research. 2023;32(4):e13880. https://pmc.ncbi.nlm.nih.gov/articles/PMC12315928/ ↩︎ ↩︎ ↩︎ ↩︎
Terman M, Terman JS. Light therapy for seasonal and nonseasonal depression: efficacy, protocol, safety, and side effects. CNS Spectrums. 2005;10(8):647-663. https://pubmed.ncbi.nlm.nih.gov/16041296/ ↩︎ ↩︎
Goodwin PJ, Pilkington-Cheney F, Taylor Y, et al. Differential sensitivity of self-reported driving and collision measures to aspects of sleep, shiftwork, and fatigue. Accident Analysis & Prevention. 2026;194:107312. https://pubmed.ncbi.nlm.nih.gov/42378747/ ↩︎