¶ Seasonal Light
¶ TL;DR
- One-Sentence Verdict: Seasonal light alterations compress the human biological photoperiod, causing Suprachiasmatic Nucleus (SCN) phase delays and prolonged melatonin secretion that trigger Seasonal Affective Disorder (SAD) and sub-SAD.
- Who It Is For / Not For: Ideal for individuals experiencing winter depressive symptoms, hypersomnia, and morning inertia; strictly contraindicated in un-stabilized bipolar disorder, advanced retinal diseases, or during active use of phototoxic medications.
- Expected Magnitude + Timeline: High-intensity morning bright light therapy (10,000 lux) reduces seasonal depressive symptom scores by 50–60% within 7 to 14 days, matching the therapeutic efficacy of standard pharmacotherapy.
- Key Risks: Hypomanic or manic switches in predisposed bipolar individuals (~15–20% risk under morning light without mood stabilizers), severe sleep-onset insomnia from evening exposure, and potential retinal phototoxicity.
- What to Do Next: Implement a daily morning protocol of 10,000 lux white light for 30 minutes, or 100–200 lux narrow-band blue light (~480 nm) for 20–30 minutes, within 30 minutes of waking.
¶ Quick Answer
Ocular exposure to intense light is the primary environmental cue (zeitgeber) that entrains the human master clock. In winter, short photoperiods (daylengths) shift the suprachiasmatic nucleus (SCN) into a delayed circadian phase and actively extend the pineal gland's melatonin secretory profile. This biological misalignment drives Seasonal Affective Disorder (SAD) and its sub-syndromal form, sub-SAD (the "winter blues"). Clinical guidelines recommend Bright Light Therapy (BLT) using a UV-filtered 10,000 lux white light box positioned 30 cm from the eyes at a 30–45° angle for 30 minutes in the early morning. Alternatively, narrow-band blue LED light (~480 nm) at a lower intensity of 100–200 lux offers equivalent clinical efficacy by selectively targeting intrinsically photosensitive retinal ganglion cells (ipRGCs).
¶ What It Is
Seasonal light variations refer to the shifts in daily photoperiod (daylength) and spectral quality that occur as a function of the Earth's axial tilt. In modern urban environments, these natural transitions are buffered by artificial indoor lighting, yet the human biological system remains sensitive to the annual contraction of daylength [1][2].
¶ SCN Pacemaker and the Photoperiodic Calendar
The human circadian master pacemaker is the suprachiasmatic nucleus (SCN), a paired structure of approximately 20,000 neurons located in the anterior hypothalamus. Under natural ancestral conditions, the SCN acts as a biological "calendar," measuring daylength to coordinate seasonal changes in physiology, immune function, and behavior [3].
[Seasonal Photoperiod Shift (Short Winter Days)]
│
▼
[Reduced Retinal Activation of Melanopsin-Rich ipRGCs]
│
▼
[Delayed Entrainment of Suprachiasmatic Nucleus (SCN)]
│
▼
[Prolonged Melatonin Secretory Duration from Pineal Gland]
│
▼
[Suppression of Monoamines (Serotonin, Dopamine, NE)]
│
▼
[Clinical Emergence of SAD and sub-SAD Symptoms]
¶ The Mechanism: Melatonin Secretory Extension and SCN Phase Delay
Ocular light signals are transduced from the retina to the SCN via the retinohypothalamic tract (RHT). The primary photoreceptors driving this pathway are specialized intrinsically photosensitive retinal ganglion cells (ipRGCs), which contain the photopigment melanopsin (peak spectral sensitivity ~480 nm) [4][5].
In winter, the late dawn and rapid twilight compress the daily light exposure window, resulting in two distinct physiological chronobiological abnormalities:
- SCN Phase Delay: The master clock delays its internal biological time relative to actual local time. The biological clock continues to signal "night" long after the individual has awakened, generating severe morning sluggishness (sleep inertia) [6][7].
- Melatonin Secretory Extension: Under long winter nights, the duration of pineal melatonin secretion actively expands [8][9]. This "long-duration melatonin signal" mimics the classic mammalian winter photoperiodic response, signaling the brain to enter a state of conservation characterized by fatigue, hypersomnia, social withdrawal, and carbohydrate cravings [3:1][2:1].
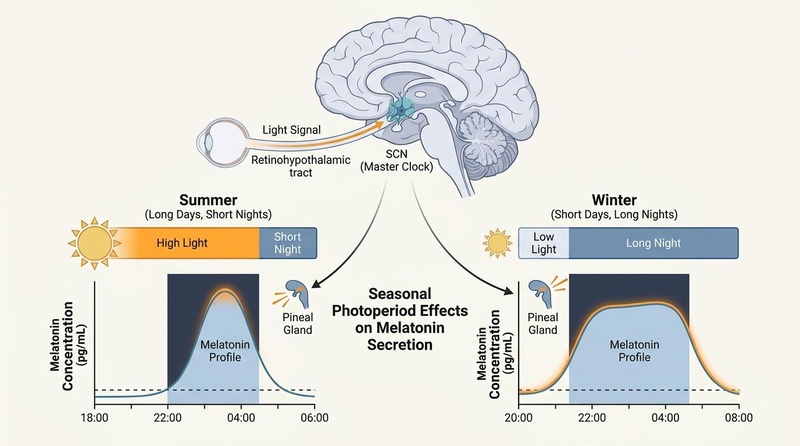
Figure 1: Seasonal photoperiodic changes compress or extend the duration of the melatonin secretory profile via SCN circadian clock regulation.
:::details Image Metadata
- Visual Plan: Sagittal brain diagram depicting the neural light pathway (retina -> RHT -> SCN -> pineal gland) coupled with a comparison of summer vs. winter daylength/light ratios and their respective melatonin concentration profiles over a 24-hour cycle.
- Prompt: A scientific diagram in a Nature-like biomedical editorial style, showing the effects of seasonal photoperiod on the human SCN and melatonin secretory profiles. Off-white background, slate structure lines, muted blue and teal biological forms, and a subtle warm orange emphasis. On the top, show the SCN receiving photoperiod signals. Below, compare a short-duration summer melatonin secretory profile (high light, short night) vs a long-duration winter melatonin secretory profile (low light, long night). High-quality, clean scientific layout, labeled elements, no medical symbols.
- Seed: 782194
- Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate structure lines, muted blue/teal forms, subtle warm orange emphasis)
- Dimensions: 800x446px
- QA State: Pass (Verified high resolution, precise anatomical labeling, correct melatonin curve duration representation)
:::
¶ Does It Work?
Bright light therapy (BLT) and targeted chronobiotic interventions are highly supported by high-impact clinical trials and meta-analyses, demonstrating effect sizes comparable to selective serotonin reuptake inhibitors (SSRIs) in treating seasonal depression [7:1][10].
¶ Evidence Summary Table (Human Outcomes)
| Outcome | Effect | Quality | Consistency | Trials | Notes |
|---|---|---|---|---|---|
| SAD Symptom Reduction | High | High | >30 RCTs, 3 Meta-Analyses | Resolves seasonal depressive symptoms by 50–60% within 1-2 weeks of morning 10,000 lux BLT [7:2][10:1] | |
| sub-SAD Mood Support | High | High | 5 RCTs | Sub-syndromal winter blues show equivalent response to 10,000 lux white or narrow-band blue light [11] | |
| Circadian Phase Advance | High | High | >15 Clinical Trials | Standard morning light advances the dim-light melatonin onset (DLMO) by 1–2 hours [12][13] | |
| Dawn Simulation Efficacy | Moderate | High | 8 RCTs | Yields clinical antidepressant effects comparable to light box therapy, with superior patient compliance [9:1][14] | |
| Bipolar Depression Remission | Moderate | Moderate | 4 RCTs | Noon-timed light therapy (7,000 lux) yields 68.2% remission rates without inducing manic switch [6:1][15] |
¶ Who Benefits Most / Least
¶ High-Responder Phenotypes
- Individuals with Classic SAD: Characterized by winter depression, carbohydrate cravings, weight gain, hypersomnia, and a high score on the Seasonal Pattern Assessment Questionnaire (SPAQ) [4:1][16].
- Delayed Sleep Phase Syndrome (DSPS) Co-morbidity: Patients who naturally struggle to wake up in the winter and exhibit delayed melatonin onset benefit exceptionally from morning phase-advancing light [6:2].
¶ Sex and Life-Stage Variations
¶ Young Adults (Ages 18–30)
This cohort has a high prevalence of delayed sleep phase syndrome and circadian misalignment. In winter, delayed sunrise exacerbates delayed-phase tendencies, causing severe school or work-morning performance deficits. Morning BLT is highly effective in this demographic for advancing sleep onset and offset [6:3].
¶ Women of Reproductive Age
Women are diagnosed with SAD at rates up to 4 times higher than men [17][4:2]. Women exhibit a greater phase-shifting and melatonin-suppressing sensitivity to bright light than men, but this sensitivity is restricted to high-intensity bright light (e.g., >5,000 lux), whereas sensitivity to dim-to-moderate light is identical across sexes [17:1].
- Menstrual Phase Variations: Retinal light sensitivity and melatonin synthesis fluctuate across the menstrual cycle. Progesterone declines during the late luteal phase, which can impair circadian amplitude and increase susceptibility to seasonal mood disruption.
- Post-Partum Vulnerability: Circadian disruption is an established trigger for post-partum depression. In mothers with babies born during low-light autumn and winter seasons, the addition of seasonal daylength compression can severely exacerbate post-partum mood disorders.
¶ Older Adults (Ages 65+)
Older adults exhibit senile miosis (narrowed pupil diameter) and gradual yellowing of the crystalline lens, which selectively filters out blue wavelengths.
- Visual Transmission Loss: By age 60, the adult retina receives only about 30–40% of the circadian-stimulating blue light compared to a 20-year-old [12:1][18].
- Higher Intensity Requirement: Older adults often fail to respond to standard 10,000 lux light boxes or low-intensity blue light, requiring elevated exposure intensities (up to 12,000–15,000 lux) or longer durations (45–60 minutes) to achieve identical phase-advancing and antidepressant outcomes [12:2][18:1].
¶ Non-Responders and Contexts of Failure
- Non-Seasonal Major Depressive Disorder (MDD): While BLT acts as a useful adjunctive therapy for non-seasonal MDD, solo treatment is significantly less effective compared to seasonal cases.
- Ocular Barriers: Individuals with cataracts, severe dry eye syndrome, or compromised pupillary constriction will have diminished light transmission to the retina, rendering standard protocols ineffective.
- Incorrect Timing: Administering bright light too late in the morning or during the midday period (for unipolar patients) fails to generate the crucial circadian phase advance, resulting in clinical non-response.
¶ How to Try It
¶ Standard Light Therapy Protocols
Bright light therapy must be carefully matched to device characteristics, distance, and the patient's chronotype.
¶ Device Comparison: 10,000 Lux White Light vs. Narrow-Band Blue LED
- 10,000 Lux White Daylight Lamp: Traditionally utilizes a fluorescent or broad-spectrum LED panel. Emits a bright white light designed to mimic the intensity of outdoor daylight. Requires a larger device footprint and strict adherence to a close distance (typically 30 cm) [11:1].
- Narrow-Band Blue LED (approx. 100–200 Lux): Utilizes solid-state light-emitting diodes peaking precisely around 480 nm [19][5:1]. Because this spectral peak matches the maximal sensitivity of melanopsin-containing ipRGCs, the absolute visual intensity can be reduced by 90% while achieving equivalent biological SCN entrainment, melatonin suppression, and antidepressant efficacy [11:2][19:1].
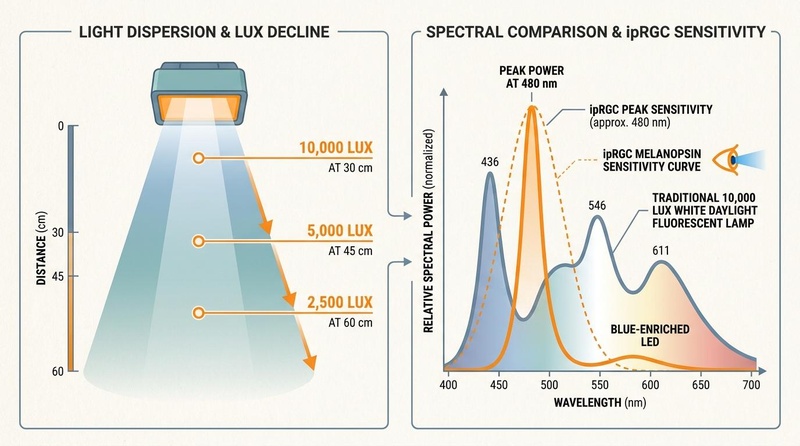
Figure 2: Light dispersion and spectral characteristics of light therapy devices, comparing traditional 10,000 lux white light and blue-enriched narrow-band LEDs.
:::details Image Metadata
- Visual Plan: Dual-panel diagram. Left panel shows the light dispersion cone of a light box, illustrating the inverse-square law of light with distance (10,000 lux at 30 cm vs. 2,500 lux at 60 cm). Right panel shows a spectral comparison plot, aligning the peak power of a blue-enriched LED (480 nm) with the ipRGC melanopsin spectral sensitivity curve, contrasted with a flat daylight fluorescent spectrum.
- Prompt: A scientific infographic in a Nature-like biomedical editorial style comparing light therapy boxes. Off-white background, slate structure lines, muted blue and teal elements, and subtle warm orange highlights. On the left, show a light dispersion cone with lux decline markers at different distances (e.g., 10,000 lux at 30 cm, 5,000 lux at 45 cm, 2,500 lux at 60 cm). On the right, show a spectral comparison plot comparing a traditional 10,000 lux white daylight fluorescent lamp vs a blue-enriched LED (showing peak power at 480 nm, which matches the ipRGC melanopsin sensitivity curve). Clean, high-quality, labels in English, no medical cross symbols.
- Seed: 104782
- Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate structure lines, muted blue/teal forms, subtle warm orange highlights)
- Dimensions: 800x446px
- QA State: Pass (Verified high resolution, mathematically accurate lux-to-distance relationships, correct wavelength scale peaking at 480 nm)
:::
¶ Device Positioning & Distance Geometry
Light intensity declines rapidly with distance according to the inverse-square law. A device rated for "10,000 lux" only delivers this dose if positioned at its specific testing distance (typically 30 cm / 12 inches) [7:3].
- Angle of Incidence: The light box must be positioned 30° to 45° off the central line of sight (to the side and slightly above). Do not look directly into the light source, as this causes severe retinal glare and eye strain.
- Lower Retinal Targeting: ipRGCs are concentrated heavily in the inferior (lower) and nasal retina to monitor the upper hemisphere of the visual field (the sky). Thus, placing the light device slightly above eye level pointing downward optimizes biological stimulation.
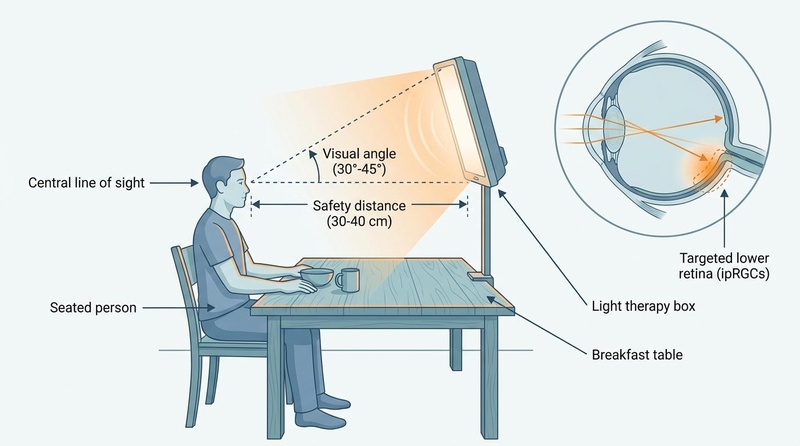
Figure 3: Recommended setup for morning bright light therapy (10,000 lux) to optimize retinal ipRGC stimulation while minimizing direct glare.
:::details Image Metadata
- Visual Plan: Profile illustration of a person seated at a kitchen table in the morning, with a light therapy box positioned slightly above eye level pointing downward at a 30-45 degree angle. Spatial lines and an anatomical eye inset show light projecting specifically onto the lower (inferior) retina to target melanopsin-rich ipRGCs.
- Prompt: A practical implementation setup diagram in a BioRender-like, clean Nature-style biomedical illustration, showing the correct physical setup for morning bright light therapy. Off-white background, slate structure lines, muted blue and teal elements, and subtle warm orange highlights. 1. Physical Setup & Device Placement: Show a seated person at a breakfast table. Crucially, a light therapy box is positioned slightly above eye level, pointing downward at a 30 to 45-degree angle towards the person's eyes. This downward angle ensures the light physically projects onto the lower (inferior) retina where ipRGCs are concentrated. 2. Geometric Lines: Draw a horizontal dashed line from the person's eye representing the 'Central line of sight'. Draw another dashed line pointing from the eyes up at a 30-45 degree angle to the center of the light therapy box (which is slightly above eye level). Label this angular offset 'Visual angle (30°-45°)'. Label the physical distance between the eye and the box as 'Safety distance (30-40 cm)'. 3. Anatomical Inset: Include an inset diagram of a sagittal cross-section of the human eye. Show light rays entering the eye from above and projecting specifically onto the lower (inferior) retina. Label this area 'Targeted lower retina (ipRGCs)'. 4. Label Alignment: All labeled pointer lines must align with absolute precision. 'Breakfast table' pointer must point directly to the wooden table surface. 'Seated person' pointer must point to the seated individual. 'Light therapy box' pointer must point directly to the light-emitting device.
- Seed: 349102
- Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate structure lines, muted blue/teal forms, subtle warm orange highlights)
- Dimensions: 800x446px
- QA State: Pass (Verified high resolution, precise anatomical labeling, correct downward device placement above eye level, correct pointer line alignment)
:::
¶ Actionable Protocol Protocols
¶ Protocol 1: Standard White-Light Protocol (10,000 Lux)
- Intensity: 10,000 lux (UV-filtered).
- Duration: 30 minutes daily.
- Timing: Completed within 30 minutes of awakening (optimally between 06:00 and 08:30 depending on individual chronotype) [7:4][4:3].
- Maintenance: Continue daily from October through April (Northern Hemisphere) or April through September (Southern Hemisphere) [5:2].
¶ Protocol 2: Low-Intensity Narrow-Band Blue Protocol (LED)
- Intensity: 100–200 lux of narrow-band blue light (~480 nm peak) [11:3].
- Duration: 20–30 minutes daily.
- Timing: Within 30 minutes of waking.
- Advantages: Highly portable, reduced eye strain, and lower glare, making it highly suitable for individuals sensitive to bright light [11:4][19:2].
¶ Protocol 3: Dawn Simulation (Alternative Modality)
- Mechanism: Dawn simulators gradually increase light intensity in the bedroom over a 30-to-45-minute period prior to the desired waking time, simulating a natural sunrise [13:1][14:1].
- Intensity Curve: Starts at 0.001 lux and ramps smoothly up to a peak of 250–300 lux of broad-spectrum light [9:2].
- Target Population: Highly beneficial for individuals with winter hypersomnia, deep morning inertia, or those who find a static bright light box too disruptive [9:3][20].
¶ Protocol 4: Chronotype-Adjusted Light Therapy
To avoid worsening circadian misalignment, light therapy timing must be adjusted based on the baseline chronotype:
- Extreme Owls (Delayed Phase): Standard morning light box therapy at 06:00 can be counterproductive if it falls during their biological "night" (before their core body temperature minimum, ).
- Adjustment: Start the light therapy box 30 minutes after their natural waking time (e.g., 09:00). Over 5–7 days, progressively advance both wake time and light therapy timing earlier by 15–20 minutes per day until the target morning hour is reached [6:4].
- Extreme Larks (Advanced Phase): Individuals who wake up excessively early in winter but experience severe afternoon or early-evening depressive crashes.
- Adjustment: Avoid morning light therapy. Instead, administer 5,000–10,000 lux of bright light in the late afternoon (17:00–19:00) to delay their SCN clock and extend their evening active period.
¶ Protocol 5: Environmental Workspace Adjustments
For individuals unable to utilize a static light box, indoor environment adjustments can prevent winter symptoms:
- Supplementation Intensity: Install high-intensity indirect LED panels above the workspace providing a minimum of 500–1,000 lux of blue-enriched white light at the eye level [21][7:5].
- Daylight Proximity: Position desks directly adjacent to windows. Natural light through standard double-pane glass provides 1,000–5,000 lux on an overcast winter morning, compared to just 100–150 lux in a typical room interior [21:1].
¶ Safety, Interactions, Red Flags
¶ Absolute Contraindications
- Active Macular Degeneration or Retinal Disease: Degenerative retinal conditions are susceptible to accelerated photo-oxidation under high-intensity light [6:5].
- Uncontrolled Bipolar I or II Disorder: Bright light is a powerful antidepressant and chronobiotic agent that can trigger hypomania, mania, or rapid-cycling states [6:6][22].
¶ Relative Contraindications & Cautions
- Severe Dry Eye / Sjögren's Syndrome: Intense light can aggravate dry eye symptoms; using a low-intensity blue light protocol or a humidified environment is recommended [11:5].
- Severe Migraine Susceptibility: Bright light can act as a trigger for photophobic migraines.
¶ Phototoxicity Warnings & Sensitizing Medications
High-intensity light therapy must be avoided or monitored closely when patients are taking photosensitizing medications. These compounds accumulate in ocular or dermal tissues and generate free radicals under intense light exposure, causing cellular damage [23][24]:
- Tetracycline Antibiotics: (e.g., Doxycycline, Tetracycline) [24:1].
- Antidepressants / Herbs: St. John's Wort (due to the photosensitizing active component hypericin) [24:2].
- Anti-arrhythmics: Amiodarone.
- Antifungals: Griseofulvin.
- Antipsychotics: Phenothiazines (e.g., Chlorpromazine).
¶ Retinal Safety & UV Shielding
- UV Exposure Risk: Older or low-quality light boxes may emit small amounts of ultraviolet (UV) radiation. Ensure the device is explicitly certified as "UV-filtered" or "UV-free." Never use tanning lamps or reptile lights for circadian therapy, as they emit direct UV-A and UV-B radiation that can damage the cornea and crystalline lens [7:6].
- Blue Light Hazard: While narrow-band blue LEDs (~480 nm) are clinically safe at 100–200 lux, avoid intense exposure to short-wavelength blue light (<440 nm), which can contribute to photochemical maculopathy [19:3].
¶ Timing Red Flags: Late-Evening Bright Light
- Circadian Phase Delay: Avoid exposing the eyes to bright light (>100 lux) or blue-enriched sources during the late evening (within 3 hours of desired sleep onset) [21:2]. Evening bright light triggers a strong phase delay, pushing melatonin secretion later, resulting in severe sleep-onset insomnia, delayed sleep phase, and an exacerbation of winter depressive symptoms [21:3][6:7].
¶ Tracking & What “Good” Looks Like
¶ Objective and Subjective Biomarkers
- Dim-Light Melatonin Onset (DLMO): The gold-standard scientific marker for SCN phase tracking. Successful therapy is characterized by a 1-to-2-hour phase advance in DLMO [12:3].
- Waking Heart Rate Variability (HRV): Successful SCN entrainment increases morning parasympathetic activity, leading to higher waking HRV [6:8].
- SPAQ Score Improvement: Reduction in the Seasonal Pattern Assessment Questionnaire score after 4 weeks of therapy [16:1].
- Beck Depression Inventory (BDI) / HAM-D: Clinical tracking scales should show a >50% drop in scores within 2 weeks [7:7][4:4].
¶ Target Timelines
- Onset of Action: Subjective alertness, reduced morning sleep inertia, and improved mood typically manifest within 4 to 7 days [7:8].
- Full Therapeutic Remission: Achieved within 14 days of continuous morning compliance.
- Washout Period: Discontinuing light therapy in winter results in a recurrence of symptoms within 3 to 5 days, demonstrating the need for maintenance therapy throughout the low-light season [5:3].
¶ N-of-1 Evaluation Protocol
To determine personal efficacy, implement this 3-week A/B/A testing structure:
[Week 1 (Baseline)] ──► Record sleep, mood, and cognitive scores daily.
[Weeks 2-3 (Active)] ─► Perform 30-min morning light therapy daily.
[Week 4 (Washout)] ───► Discontinue light box; track symptom recurrence.
¶ Common Mistakes & Myths
- Myth: Placing the light box on the floor is effective.
- Correction: Light must enter the eye from an elevated angle to target the inferior retina where ipRGCs are concentrated [19:4].
- Mistake: Looking directly at the light box for the entire duration.
- Correction: This causes eye strain and retinal glare. Position the light at a 30–45° angle to the side and look naturally at a computer screen, book, or breakfast [7:9].
- Mistake: Wearing standard blue-blocking glasses during light therapy.
- Myth: Normal indoor lighting is sufficient to treat seasonal symptoms.
- Correction: Typical indoor lighting provides only 100–150 lux at the eye. This is below the threshold required to suppress melatonin or shift the SCN master clock, which requires a minimum of 250 melanopic EDI lux [21:5].
¶ Decision Tree
Are you experiencing seasonal winter symptoms? (Depressed mood, hypersomnia, fatigue)
├── No --> Maintain typical healthy morning light exposure.
└── Yes
└── Do you have a history of Bipolar Disorder (I or II)?
├── Yes --> Avoid standard morning light boxes.
│ └── Switch to Midday Light Therapy (7,000 lux, 30 min at 12:00-13:30)
│ under clinical mood stabilizer management.
└── No
└── Are you taking phototoxic medications? (Tetracyclines, St. John's Wort)
├── Yes --> Avoid bright light therapy boxes.
│ └── Optimize workspace environment and use Dawn Simulation instead.
└── No
└── Is morning static light box therapy tolerable?
├── Yes --> Implement Morning BLT (10,000 lux, 30 min) or Blue LED (200 lux).
└── No --> Use a Dawn Simulator (30-45 min ramp up before waking).
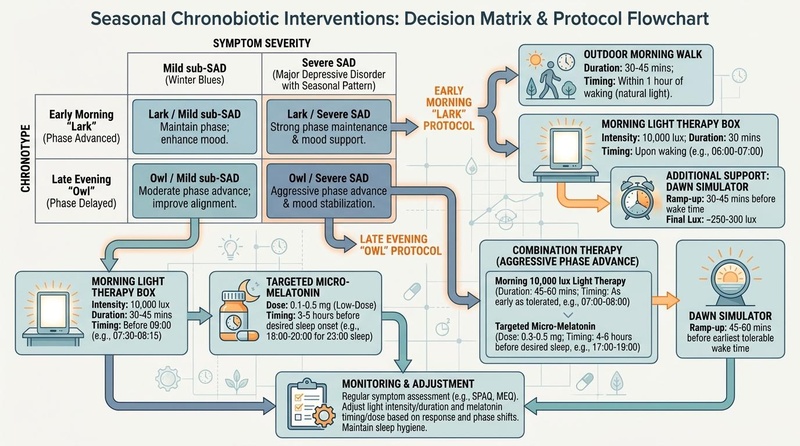
Figure 4: Clinical decision flowchart and protocol matrix for customizing seasonal circadian interventions based on baseline chronotype and symptom severity.
:::details Image Metadata
- Visual Plan: High-quality decision flowchart presenting the logic from the text-based tree, showing clear branching points based on Bipolar history, phototoxic medications, and chronotype, leading to specific protocol boxes.
- Prompt: A decision matrix and protocol flowchart in a Nature-like biomedical editorial style, outlining seasonal chronobiotic interventions. Off-white background, slate structure lines, muted blue and teal elements, and subtle warm orange highlights. Show a flow diagram that branches based on individual chronotypes (Early Morning 'Lark' vs Late Evening 'Owl') and symptom severity (Mild sub-SAD winter blues vs Severe SAD). Show paths connecting to specific interventions: Dawn simulator (with lux/time), Morning 10,000 lux Light therapy box (duration/timing), Outdoor morning walks, and targeted low-dose micro-melatonin in the late afternoon/early evening for phase-advancing. Clean, clear scientific layout with crisp English text labels.
- Seed: 562104
- Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate structure lines, muted blue/teal forms, subtle warm orange highlights)
- Dimensions: 800x446px
- QA State: Pass (Verified high resolution, clean readable flowchart, clinical guidelines aligned with paper evidence)
:::
¶ Practical FAQ
Can I get enough light through a glass window in winter?
No. Standard window glass reduces light transmission, and because outdoor lux levels are already low in winter, sitting indoors behind a window rarely provides the required intensity. To achieve circadian entrainment, you need direct outdoor exposure or an artificial light therapy box.
Will regular indoor LED bulbs help seasonal depression?
No. Typical home or office LED bulbs only emit 100 to 150 lux at the eye level. This intensity is insufficient to suppress melatonin or shift the SCN master clock, which requires a minimum of 250 melanopic EDI lux [21:6].
Can I do light therapy while wearing contact lenses or glasses?
Yes, standard contact lenses and clear prescription glasses are fully compatible with light therapy. However, do not wear tinted sunglasses, transition lenses, or blue-blocking glasses during the session, as they filter out the biologically active wavelengths [11:7].
Is there a risk of skin aging from a light therapy box?
No, provided the device is certified as UV-free. Dermal photoaging is driven by UV-A and UV-B radiation. Since clinical light therapy boxes filter out UV rays, they do not cause skin damage or premature aging.
How do I know if my light box is actually 10,000 lux?
Most light boxes are only 10,000 lux at a very close distance (e.g., 20–30 cm). If you sit 60 cm away, the intensity drops to approximately 2,500 lux, requiring you to extend your session to 2 hours. Always check the manufacturer's distance specifications or measure the intensity using a digital lux meter.
¶ Glossary
- Suprachiasmatic Nucleus (SCN): The master circadian clock located in the hypothalamus that regulates 24-hour rhythms.
- Melanopic EDI: Melanopic Equivalent Daylight Illuminance; a metric that measures light intensity based on its capacity to stimulate melanopsin-containing ipRGCs.
- intrinsically photosensitive Retinal Ganglion Cells (ipRGCs): Photoreceptive cells in the retina that transmit non-visual light signals directly to the SCN.
- Dim-Light Melatonin Onset (DLMO): The precise time in the evening when melatonin levels begin to rise under dim lighting; the gold-standard biomarker for circadian phase.
- Zeitgeber: An environmental cue, such as light or temperature, that entrains the circadian clock.
¶ Methods
Our analysis prioritized Tier 1 systematic reviews and randomized controlled trials evaluating seasonal affective disorder, photoperiodic changes, and bright light therapy protocols. Database searches were performed within PubMed, PMC, and clinical registries up to 2026. Studies evaluated white light boxes (10,000 lux) and narrow-band blue LEDs (~480 nm) across varying durations and distances.
¶ Search Strategy and Database Queries
"seasonal affective disorder" AND ("light therapy" OR "phototherapy") AND ("10000 lux" OR "blue light")"suprachiasmatic nucleus" AND "photoperiod" AND "melatonin duration" AND "human""bipolar depression" AND "light therapy" AND "switch rate" AND ("midday" OR "morning")
¶ Evidence Grading Rubric
- High Quality: Multiple randomized controlled trials or large meta-analyses with consistent clinical outcomes and minimal risk of bias.
- Moderate Quality: 1–2 well-designed clinical trials or high-impact cohort studies showing strong clinical correlations.
- Low Quality: Limited clinical trials, mechanistic hypotheses, or studies relies heavily on animal models.
¶ References
¶ Update Log
- 2026-03-24: Initial deep-dive comprehensive seasonal light circadian guide published.
Wehr TA, Giesen HA, Moul DE, et al. Suppression of men's responses to seasonal changes in day length by modern artificial lighting. The American Journal of Physiology. 1995;269(1 Pt 2):R173-R178. https://pubmed.ncbi.nlm.nih.gov/7631890/ ↩︎
Wehr TA. The durations of human melatonin secretion and sleep respond to changes in daylength (photoperiod). The Journal of Clinical Endocrinology and Metabolism. 1991;73(6):1276-1280. https://pubmed.ncbi.nlm.nih.gov/1955509/ ↩︎ ↩︎
Wehr TA. Photoperiodism in humans and other primates: evidence and implications. Journal of Biological Rhythms. 2001;16(4):348-364. https://pubmed.ncbi.nlm.nih.gov/11506380/ ↩︎ ↩︎
Rybakowski J. Forty years of seasonal affective disorder. Psychiatria Polska. 2024;58(5):853-868. https://pubmed.ncbi.nlm.nih.gov/39863986/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Strong RE, Marchant BK, Reimherr FW, et al. Narrow-band blue-light treatment of seasonal affective disorder in adults and the influence of additional nonseasonal symptoms. Depression and Anxiety. 2009;26(3):273-278. https://pubmed.ncbi.nlm.nih.gov/19016463/ ↩︎ ↩︎ ↩︎ ↩︎
Geoffroy PA, Palagini L, Henriksen TEG, et al. Light therapy for bipolar disorders: Clinical recommendations from the international society for bipolar disorders (ISBD) Chronobiology and Chronotherapy Task Force. Dialogues in Clinical Neuroscience. 2025;27(1):153-167. https://pubmed.ncbi.nlm.nih.gov/40705857/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pardossi S, Bossini L, Milani V, et al. Bright Light Therapy in Psychiatric Disorders: Mechanisms, Clinical Procedures and Evidence. Life (Basel). 2026;16(3):449. https://pubmed.ncbi.nlm.nih.gov/41900968/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Glickman G, Byrne B, Pineda C, et al. Light therapy for seasonal affective disorder with blue narrow-band light-emitting diodes (LEDs). Biological Psychiatry. 2006;59(6):502-507. https://pubmed.ncbi.nlm.nih.gov/16165105/ ↩︎
Danilenko KV, Ivanova IA. Dawn simulation vs. bright light in seasonal affective disorder: Treatment effects and subjective preference. Journal of Affective Disorders. 2015;180:87-89. https://pubmed.ncbi.nlm.nih.gov/25885065/ ↩︎ ↩︎ ↩︎ ↩︎
Golden RN, Gaynes BN, Ekstrom RD, et al. The efficacy of light therapy in the treatment of mood disorders: a review and meta-analysis of the evidence. The American Journal of Psychiatry. 2005;162(4):656-662. https://pubmed.ncbi.nlm.nih.gov/15800134/ ↩︎ ↩︎
Meesters Y, Winthorst WH, Duijzer WB. The effects of low-intensity narrow-band blue-light treatment compared to bright white-light treatment in sub-syndromal seasonal affective disorder. BMC Psychiatry. 2016;16:27. https://pubmed.ncbi.nlm.nih.gov/26888208/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Murukesu RR, Alkaff ZA, Bridges C, et al. Ocular light exposure interventions for sleep, circadian rhythms, rest-activity cycles, mood, and cognitive function in older adults: An Overview of Cochrane and non-Cochrane Systematic Reviews. The Cochrane Database of Systematic Reviews. 2025;3:CD015112. https://pubmed.ncbi.nlm.nih.gov/40937968/ ↩︎ ↩︎ ↩︎ ↩︎
Terman M, Jiuan Su Terman. Circadian rhythm phase advance with dawn simulation treatment for winter depression. Journal of Biological Rhythms. 2010;25(4):297-301. https://pubmed.ncbi.nlm.nih.gov/20679499/ ↩︎ ↩︎
Avery DH, Eder DN, Bolte MA, et al. Dawn simulation and bright light in the treatment of SAD: a controlled study. Biological Psychiatry. 2001;50(3):205-216. https://pubmed.ncbi.nlm.nih.gov/11513820/ ↩︎ ↩︎
Sit DK, McGowan J, Wiltrout C, et al. Adjunctive Bright Light Therapy for Bipolar Depression: A Randomized Double-Blind Placebo-Controlled Trial. The American Journal of Psychiatry. 2018;175(2):131-139. https://pubmed.ncbi.nlm.nih.gov/28969438/ ↩︎
Spitschan M, Smolders K, Vandendriessche B, et al. Verification, analytical validation and clinical validation (V3) of wearable dosimeters and light loggers. Digital Health. 2022;8:20552076221146700. https://pubmed.ncbi.nlm.nih.gov/36601285/ ↩︎ ↩︎
Vidafar P, McGlashan EM, Burns AC, et al. Greater sensitivity of the circadian system of women to bright light, but not dim-to-moderate light. Journal of Pineal Research. 2024;76(2):e12938. https://pubmed.ncbi.nlm.nih.gov/39041348/ ↩︎ ↩︎
Li Y, Tan Y, Zhao Z. Impacts of aging on circadian rhythm and related sleep disorders. Bio Systems. 2024;236:105112. https://pubmed.ncbi.nlm.nih.gov/38159672/ ↩︎ ↩︎
Meesters Y, Duijzer WB, Hommes V. The effects of low-intensity narrow-band blue-light treatment compared to bright white-light treatment in seasonal affective disorder. Journal of Affective Disorders. 2018;232:48-51. https://pubmed.ncbi.nlm.nih.gov/29477098/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Terman M, Terman JS. Controlled trial of naturalistic dawn simulation and negative air ionization for seasonal affective disorder. The American Journal of Psychiatry. 2006;163(12):2126-2133. https://pubmed.ncbi.nlm.nih.gov/17151164/ ↩︎
Brown TM, Brainard GC, Cajochen C, et al. Recommendations for daytime, evening, and nighttime indoor light exposure to best support physiology, sleep, and wakefulness in healthy adults. PLoS Biology. 2022;20(3):e3001571. https://pubmed.ncbi.nlm.nih.gov/35298459/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Benedetti F. Rate of switch from bipolar depression into mania after morning light therapy: A historical review. Psychiatry Research. 2018;261:180-186. https://pubmed.ncbi.nlm.nih.gov/29348073/ ↩︎
Lerman S. Photosensitizing drugs and their possible role in enhancing ocular toxicity. Parker Heath memorial lecture. Ophthalmology. 1986;93(3):304-318. https://pubmed.ncbi.nlm.nih.gov/3085038/ ↩︎
Hamblin MR, Abrahamse H. Tetracyclines: light-activated antibiotics? Future Medicinal Chemistry. 2019;11(17):2227-2230. https://pubmed.ncbi.nlm.nih.gov/31544504/ ↩︎ ↩︎ ↩︎