¶ Sleep Apnea
| Indication | Obstructive and Central Sleep Apnea |
| Access | Diagnostic & Prescription-based |
| Dosing Sched | Nightly compliance |
| Safety Profile | High safety (non-invasive) |
| Key Marker | AHI / REI / Hypoxic Burden |
| Est. Cost | Varies by insurance/device |
Sleep apnea is a sleep-related breathing disorder characterized by repeated reductions or pauses in breathing during sleep. Obstructive sleep apnea (OSA) is associated with cardiovascular, metabolic, cognitive, and safety risks, although the size and causality of individual long-term risks vary across populations.[1][2]
¶ At a glance
Key points
- Diagnostic utility: Identifies sleep-related breathing disorders that drive intermittent hypoxia and sympathetic nervous system overactivity.
- Primary risks: OSA is associated with hypertension, coronary disease, stroke, arrhythmias, impaired vigilance, and motor-vehicle risk; association does not prove that treatment prevents every downstream event.[1:1][2:1][3]
- What treatment reliably does: Effective treatment reduces breathing events and often improves sleepiness, quality of life, and blood pressure. Randomized trials have not established that CPAP broadly prevents major cardiovascular events.[4]
What people use it for
- Goals: Diagnosing sleep-related breathing disorders, mitigating cardiovascular risk, improving daytime vigilance, and optimizing sleep architecture.
- Evidence quality: High for diagnostic pathways, reduction of respiratory events, and symptom relief; mixed or uncertain for prevention of major cardiovascular events.[5][4:1]
¶ What is Sleep Apnea?
Sleep apnea represents a spectrum of sleep-related breathing disorders wherein respiration is repeatedly interrupted or significantly reduced. The clinical context is vital for determining the appropriate intervention, as the underlying pathophysiology dictates the risk profile and therapeutic approach [5:1].
- Obstructive Sleep Apnea (OSA): The most common form, caused by a physical collapse or narrowing of the upper airway during sleep despite ongoing respiratory effort. This leads to fragmented sleep and intermittent hypoxemia [6].
- Central Sleep Apnea (CSA): Characterized by a lack of respiratory drive. In CSA, the brain fails to send the appropriate signals to the muscles controlling breathing, resulting in cessations of airflow without respiratory effort [7].
- Complex/Mixed Sleep Apnea: Also known as treatment-emergent central sleep apnea, this presents as a combination of both obstructive and central events, often unmasked when a patient with OSA is treated with positive airway pressure therapy.
¶ Symptom & Risk Screening
Effective screening is critical to identify individuals at high risk before they undergo formal diagnostic testing. The STOP-BANG questionnaire is a validated, high-sensitivity screening tool used widely in clinical settings.
The STOP-BANG acronym evaluates:
- Snoring: Loud enough to be heard through closed doors.
- Tiredness: Daytime fatigue or sleepiness.
- Observed apnea: Someone has witnessed breathing interruptions.
- Pressure: High blood pressure or treatment for hypertension.
- BMI: Body Mass Index greater than 35 kg/m².
- Age: Over 50 years old.
- Neck circumference: Greater than 40 cm (16 inches).
- Gender: Male.
While the STOP-BANG score is highly sensitive for detecting moderate to severe OSA, its diagnostic utility has specific limitations. It exhibits high false-positive rates and low specificity, particularly for mild cases. Furthermore, gender-specific biases mean it may under-predict OSA severity in women, who often present with atypical symptoms like insomnia or morning headaches rather than classical snoring [3:1].
¶ Diagnosis: Home vs. Laboratory Testing
The diagnosis of sleep apnea involves objective monitoring of sleep physiology. The choice between home testing and in-lab polysomnography depends on the patient's comorbidities and suspected sleep disorder complexity [5:2].
- Home Sleep Apnea Testing (HSAT - Type III/IV): These portable monitors measure airflow, respiratory effort, and blood oxygenation in the patient's own bed. They are convenient and cost-effective for patients with a high pre-test probability of uncomplicated OSA.
- In-lab Polysomnography (PSG - Type I/II): The gold standard diagnostic tool conducted in a sleep laboratory. It continuously records EEG (brain waves), EOG (eye movements), EMG (muscle activity), ECG (heart rhythm), respiratory effort, and airflow.
Home testing can underestimate disease severity because most devices do not record sleep architecture, true total sleep time, or microarousals. HSAT therefore commonly uses recording or monitoring time as the denominator, which can produce a lower REI than an in-lab AHI. It is intended mainly for uncomplicated adults with a high pre-test probability of moderate-to-severe OSA; it is not a comprehensive evaluation for central apnea, narcolepsy, parasomnias, limb movements, or other sleep disorders. A negative, inconclusive, or technically inadequate home test may require polysomnography when clinical suspicion remains.[5:3][8]
¶ Diagnostic Indices & Limitations
Quantifying sleep apnea severity relies on specific indices, which, while standard, possess critical limitations regarding long-term cardiovascular prediction.
- Apnea-Hypopnea Index (AHI): Calculated during in-lab PSG, this is the number of apneas and hypopneas per hour of actual sleep.
- Respiratory Event Index (REI): Used in home testing, representing the number of events per hour of recording time.
Limitations of AHI/REI:
Traditional metrics like AHI and REI treat all events equally, failing to capture the physiological stress of the disorder. They ignore the hypoxic burden (the depth and duration of oxygen desaturation), event duration, and the autonomic arousal index (the severity of sleep fragmentation). Research increasingly demonstrates that these unmeasured factors—particularly hypoxic burden and positional patterns—may be far superior predictors of cardiovascular outcomes and mortality than AHI alone [9].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect | Consistency | Evidence quality | Notes (population, duration, dose) |
|---|---|---|---|---|
| Blood Pressure Reduction | High | High | Validated across CPAP and MAD interventions [10][11][12]. | |
| Daytime Sleepiness/Vigilance | High | High | Significant improvement in CPAP compliance [3:2]. | |
| Cardiovascular Event Risk | Low | Moderate-High | Randomized-trial meta-analysis found no statistically established reduction in major events; adherence remains an important unresolved modifier.[4:2] | |
| Heart Rate Variability/Autonomic Balance | Moderate | Moderate | Decreased sympathetic overactivity [13][14]. | |
| Insulin Sensitivity | Low | Low | Direct treatment effects are uncertain and are difficult to separate from weight change and other care.[2:2] | |
| Endothelial Function/Arterial Stiffness | Moderate | Low-Moderate | Some studies report improvement in surrogate vascular measures; this does not establish fewer clinical events.[15][16] |
¶ Mechanisms and Cardiovascular/Functional Relevance
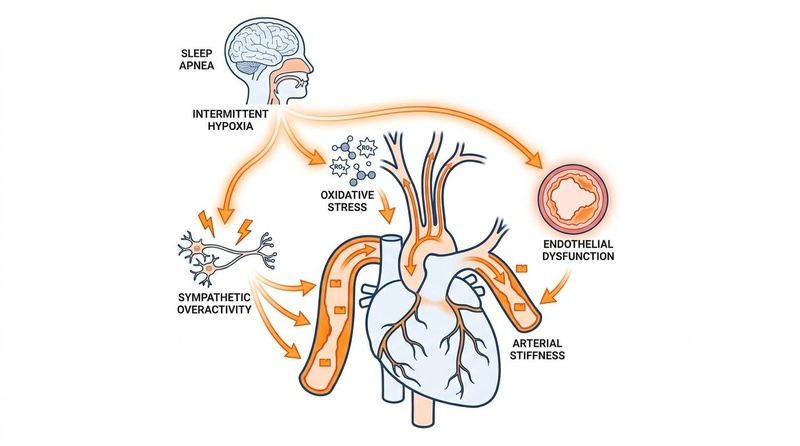
The systemic pathophysiology of sleep apnea extends far beyond sleep disruption, driving a cascade of molecular and cardiovascular consequences.
- Intermittent Hypoxia and Oxidative Stress: Repeated cycles of oxygen desaturation and reoxygenation trigger robust oxidative stress, generating reactive oxygen species (ROS) and elevating ischemia-modified albumin (IMA) [17][18].
- Sympathetic Nervous System Overactivity: Hypoxia and hypercapnia stimulate peripheral chemoreceptors, leading to a massive surge in sympathetic tone that persists into the waking hours, driving hypertension [13:1].
- Endothelial Dysfunction and Vascular Remodeling: Intermittent hypoxia and systemic inflammation impair nitric oxide availability, promoting arterial stiffness, atherosclerosis, and anatomical remodeling of the vasculature [15:1][16:1][19][20].
- Intrathoracic Pressure Swings: Forced inspiratory efforts against a closed airway cause severe negative intrathoracic pressure, altering cardiac hemodynamics, increasing transmural stress on the heart, and predisposing the atria to structural changes [14:1].
Long-term cardiovascular relevance: OSA is associated with hypertension, coronary disease, atrial fibrillation and other arrhythmias, stroke, and metabolic dysfunction. Risk is heterogeneous and is influenced by hypoxic burden, sleepiness, comorbidities, and other factors.[1:2][2:3][21]
¶ Therapies & Management Protocols
Management of sleep apnea is highly individualized, requiring a multimodal approach to achieve optimal compliance and symptom resolution [5:4].
- Continuous Positive Airway Pressure (CPAP): A standard first-line therapy for many people with moderate-to-severe OSA. CPAP acts as a pneumatic splint, keeping the upper airway open, and is highly effective at reducing respiratory events when used. It improves sleepiness and can modestly lower blood pressure, but randomized-trial evidence has not shown broad prevention of major cardiovascular events.[4:3] Pressure adjustment, mask selection, troubleshooting, and sometimes heated humidification can improve comfort; humidification does not consistently increase nightly use.[22]
- Mandibular Advancement Devices (MAD): A primary alternative for mild-to-moderate OSA or CPAP-intolerant patients. MADs pull the lower jaw forward to enlarge the upper airway, demonstrating significant efficacy in blood pressure reduction [10:1][11:1][12:1].
- Weight Loss and Lifestyle Interventions: Higher body weight is an important modifiable risk factor for many people with OSA, but it is not the cause in everyone. In INTERAPNEA, an intensive lifestyle program reduced AHI among 89 Spanish men with overweight or obesity who had moderate-to-severe OSA; 29% of assessed intervention participants were in remission at six months, so the result should not be generalized as a cure for every patient.[23] Bariatric procedures can also reduce severity in selected patients, but follow-up testing is needed before changing apnea therapy.[24]
- Positional Therapy: For patients whose apneas are strongly tied to sleeping on their back, positional therapy (using devices to prevent supine sleep) can be a highly effective conservative measure [25].
- Surgical Options: In cases of anatomical abnormalities or severe CPAP intolerance, interventions like Hypoglossal Nerve Stimulation offer targeted neuromuscular control to maintain airway patency.
¶ Safety, Driving, and Functional Risks
Sleep apnea carries immediate, life-threatening functional risks that require urgent clinical attention.
- Driving Safety and Microsleeps: The most critical functional risk for untreated patients is the danger of microsleeps while operating a vehicle. Sleep-deprived individuals have a sharply increased risk of motor vehicle accidents and occupational injuries [3:3].
- Perioperative and Anesthesia Dangers: Sleep apnea complicates anesthesia. Sedatives and anesthetics relax the airway muscles and depress the respiratory drive, significantly elevating the risk of postoperative complications, respiratory failure, and difficult intubation.
- Clinical Follow-up Requirements: Management is not "set it and forget it." It requires ongoing partnership with a board-certified sleep specialist. Protocols include initial titration, continuous compliance tracking via connected devices, and periodic efficacy reassessments to adjust to weight fluctuations or aging.
¶ Access, Equity, and Longevity Perspectives
The landscape of sleep apnea management sits at the intersection of standard clinical care and proactive longevity wellness.
- Standard of Care vs. Longevity Wellness: Standard care includes evaluation when symptoms, observed breathing pauses, risk factors, or relevant comorbidities raise suspicion; it is not limited to people who have already had a cardiovascular event. Consumer interest in tracking oxygen or “hypoxic burden” should not be treated as a substitute for validated testing or evidence that screening asymptomatic, low-risk adults improves outcomes. CPAP requires appropriate diagnosis, prescription, fitting, and follow-up.
- Socioeconomic and Racial Disparities: Substantial disparities exist in sleep apnea care. Minority populations and lower socioeconomic groups often face delayed diagnosis, severe cost barriers for CPAP equipment and supplies, and lower overall compliance rates due to lack of follow-up care and educational resources. Exhaled breath analysis and scalable diagnostics remain active areas of research to lower the barrier to entry [26].
¶ FAQ Section
¶ References
Obstructive Sleep Apnea and Coronary Artery Disease. https://pubmed.ncbi.nlm.nih.gov/41898162/ ↩︎ ↩︎ ↩︎
Cardiovascular morbidities of obstructive sleep apnea. https://pubmed.ncbi.nlm.nih.gov/31852426/ ↩︎ ↩︎ ↩︎ ↩︎
Obstructive Sleep Apnea With or Without Excessive Daytime Sleepiness. https://pubmed.ncbi.nlm.nih.gov/29997573/ ↩︎ ↩︎ ↩︎ ↩︎
Labarca G, Dreyse J, Drake L, et al. Efficacy of continuous positive airway pressure (CPAP) in the prevention of cardiovascular events in patients with obstructive sleep apnea: systematic review and meta-analysis. Sleep Med Rev. 2020;52:101312. https://pubmed.ncbi.nlm.nih.gov/32248026/ ↩︎ ↩︎ ↩︎ ↩︎
Guidelines for the diagnosis and treatment of obstructive sleep apnea in adults (2025). https://pubmed.ncbi.nlm.nih.gov/41820035/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Phenotyping obstructive sleep apnea. https://pubmed.ncbi.nlm.nih.gov/41984137/ ↩︎
Central sleep apnea: cessation of central respiration control. https://pubmed.ncbi.nlm.nih.gov/41065809/ ↩︎
Update on Research and Practices. https://pubmed.ncbi.nlm.nih.gov/31512821/ ↩︎
Apnea-Hypopnea Index Versus Hypoxic Burden. https://pubmed.ncbi.nlm.nih.gov/42171113/ ↩︎
Blood pressure response with obstructive sleep apnoea treatment (MAD vs CPAP). https://pubmed.ncbi.nlm.nih.gov/41485464/ ↩︎ ↩︎
Mandibular Advancement vs CPAP for Blood Pressure Reduction. https://pubmed.ncbi.nlm.nih.gov/38588926/ ↩︎ ↩︎
CPAP vs Mandibular Advancement Devices and Blood Pressure. https://pubmed.ncbi.nlm.nih.gov/26624827/ ↩︎ ↩︎
The pulse of sleep: sleep-cardiovascular connection. https://pubmed.ncbi.nlm.nih.gov/39238992/ ↩︎ ↩︎
Obstructive Sleep Apnoea and Cardiac Arrhythmias (OSCA) trial. https://pubmed.ncbi.nlm.nih.gov/36792325/ ↩︎ ↩︎
Changes of carotid artery elasticity before and after CPAP. https://pubmed.ncbi.nlm.nih.gov/34304531/ ↩︎ ↩︎
Impact of CPAP on arterial stiffness. https://pubmed.ncbi.nlm.nih.gov/33094411/ ↩︎ ↩︎
The relationships between intermittent hypoxia and oxidative stress. https://pubmed.ncbi.nlm.nih.gov/39300984/ ↩︎
Obstructive sleep apnea and CPAP effect on IMA levels. https://pubmed.ncbi.nlm.nih.gov/29948857/ ↩︎
Intermittent Hypoxia-Induced Cardiovascular Remodeling. https://pubmed.ncbi.nlm.nih.gov/26836908/ ↩︎
Obstructive sleep apnea and heart disease (biomarkers point of view). https://pubmed.ncbi.nlm.nih.gov/23277071/ ↩︎
CPAP and Stroke Risk Reduction. https://pubmed.ncbi.nlm.nih.gov/26731604/ ↩︎
Pressure modification or humidification for improving usage of CPAP. https://pubmed.ncbi.nlm.nih.gov/31792939/ ↩︎
Effect of an Interdisciplinary Weight Loss and Lifestyle Intervention (INTERAPNEA RCT). https://pubmed.ncbi.nlm.nih.gov/35452108/ ↩︎
Anatomical Remodeling of the Upper Airway after Laparoscopic Sleeve Gastrectomy. https://pubmed.ncbi.nlm.nih.gov/41231327/ ↩︎
Understanding Phenotypes of Obstructive Sleep Apnea. https://pubmed.ncbi.nlm.nih.gov/27861433/ ↩︎
Exhaled Breath Analysis in Obstructive Sleep Apnea. https://pubmed.ncbi.nlm.nih.gov/31461988/ ↩︎