¶ Spirometry and Lung-Function Testing
| Mechanism | Forced expiratory pneumotachography & flow-sensing |
| Key Specs | FEV1, FVC, FEV1/FVC, FEF25-75% |
| Protocols | Forced expiratory maneuvers, Bronchodilator testing |
| FDA Class | Class II Diagnostic Device |
| Entry Cost | $150 - $2,500 (clinic-grade setups) |
Spirometry is the primary and most widely accessible pulmonary function test (PFT) used to measure the volume and flow of air during forced exhalation. It serves as a foundational diagnostic and monitoring tool in respiratory medicine, providing quantitative data on ventilatory capacity, airway resistance, and lung mechanics [1]. Proper clinical utility requires a structured approach to screening, diagnosis, and longitudinal monitoring [1:1].
¶ At a glance
Key points
- Does it work? Yes. Quality-controlled spirometry is the gold standard for diagnosing and managing obstructive ventilatory defects, such as asthma and chronic obstructive pulmonary disease (COPD) [1:2][2].
- Who needs it? Symptomatic patients, individuals with chronic occupational or environmental exposures, preoperative patients undergoing high-risk cardiothoracic procedures, and those requiring systematic monitoring of known pulmonary diseases [1:3][3][4].
- Verdict: A highly validated, inexpensive, and clinically indispensable diagnostic tool. Clinical utility is optimized when performed in accordance with standardized quality-control and reproducibility standards [1:4][5].
¶ Evidence summary table (human outcomes)
| Clinical Scenario | Measured Parameter | Consistency | Evidence Quality | Key Findings & Quantitative Efficacy |
|---|---|---|---|---|
| Occupational Dust Exposure | FEV1, FVC, PEFR | High | High | Chronic exposure to organic dust is associated with an overall small but significant excess loss in FEV1 of 4.92 mL/year (95% CI 0.14 to 9.69 mL/year), with no significant association seen overall for FVC [6]. |
| Preserved Ratio Impaired Spirometry (PRISm) | FEV1 < 80% predicted, FEV1/FVC ≥ LLN | High | High | PRISm is associated with a significantly elevated risk of all-cause mortality (HR 1.60), cardiovascular mortality (HR 1.68), and respiratory-related mortality (HR 3.09), especially among active smokers [7]. |
| Post-Tuberculosis Lung Impairment | FEV1, FVC, Mixed Defects | High | High | Drug-susceptible TB survivors present with FEV1 of 76.6% predicted and FVC of 81.8% predicted [8]. Mixed ventilatory defects are highly prevalent, occurring in up to 43.0% of multidrug-resistant TB survivors [8:1]. |
| Preoperative Respiratory Muscle Training | FEV1, FVC, Maximum Voluntary Ventilation (MVV) | High | High (RCTs) | 3 days of preoperative inspiratory muscle training reduces postoperative pulmonary complications, demonstrating a significant absolute risk reduction (ARR) of -0.18 (95% CI -0.33 to -0.03) vs. sham IMT, alongside significant reductions compared to standard care [3:1]. |
| Preterm Birth Pulmonary Sequelae | Static volumes, DLCO, Oscillometry | High | High | Individuals born preterm show structural gas-transfer deficits (DLCO SMD -0.51) and elevated small airway resistance, which standard spirometry frequently fails to detect [9]. |
| Pediatric Inflammatory Bowel Disease | DLCO, Spirometry | Moderate | Moderate | Children with IBD may show a trend toward reduced gas transfer (DLCO% predicted MD -5.8, 95% CI: -12.4 to 0.9), although this finding is not statistically significant (p = 0.09) per Moriki et al., despite having largely preserved standard spirometry parameters [10]. |
¶ Mechanism & Physiology
¶ Dynamic Lung Volumes: FEV1 and FVC
The core physiological metrics derived from standard spirometry include:
- Forced Expiratory Volume in 1 Second (FEV1): The volume of air forcefully exhaled during the first second of a forced vital capacity maneuver [1:5]. It reflects both the elastic recoil of the lungs and the patency of the conducting airways.
- Forced Vital Capacity (FVC): The maximum volume of air that can be exhaled forcefully and completely after a full, deep inspiration [1:6]. FVC is a surrogate measure of accessible lung volume.
- FEV1/FVC Ratio: The fraction of vital capacity exhaled in the first second [1:7]. This ratio is the primary physiologic metric used to identify airflow limitation and differentiate obstructive from restrictive ventilatory patterns [1:8][11].
¶ Multi-Ethnic Reference Standards and the Lower Limit of Normal (LLN)
Interpreting spirometric metrics requires comparing a patient’s raw values to a healthy, non-smoking, demographic-matched reference population [1:9][2:1]. Historically, clinicians relied on arbitrary, fixed cutoffs—such as an FEV1/FVC ratio below 0.70—to define airway obstruction.
Modern guidelines strongly condemn fixed cutoffs due to high rates of misclassification [1:10][2:2]:
- The Problem of Fixed Cutoffs: Because the FEV1/FVC ratio naturally declines with age due to normal senescent loss of lung elastic recoil, using a fixed 0.70 cutoff leads to significant over-diagnosis of obstruction in older adults [1:11][2:3]. Conversely, it leads to under-diagnosis of obstruction in younger adults [1:12].
- The Lower Limit of Normal (LLN): Current standards mandate comparing results to the 5th percentile (LLN) of the reference population using equations from the Global Lung Function Initiative (GLI) [12][1:13][11:1]. An FEV1/FVC ratio below the LLN defines airway obstruction [1:14][11:2].
- Ethnic and Geographic Variances: GLI reference equations incorporate age, biological sex, height, and major ethnic groups [12:1][13]. However, geographic validation studies have shown that applying the generalized GLI Global equations can sometimes overestimate or underestimate lung function in specific populations (e.g., in cohorts from Maputo, Mozambique), necessitating the ongoing development and validation of localized reference equations [13:1][2:4].
¶ Repeatability and Acceptability Criteria
To ensure clinical utility, spirometric maneuvers must adhere to quality-control standards [1:15][5:1]. Multiple forced expiratory maneuvers are performed to ensure reproducibility of FEV1 and FVC, and results are compared against healthy reference populations to identify ventilatory impairments [1:16][5:2]. If repeatability criteria are not met, testing may be continued up to a set maximum number of attempts or until the technician documents that the patient is unable to perform further maneuvers [1:17][5:3].
¶ Bronchodilator Reversibility Testing
Bronchodilator testing evaluates the acute reversibility of airflow obstruction [1:18][5:4]. The protocol involves performing baseline spirometry, administering an inhaled bronchodilator (such as albuterol), and repeating the spirometric measurements after a short waiting period [1:19][5:5].
- Diagnostic Interpretation: A significant positive response (typically characterized by an improvement in FEV1 or FVC) indicates reversible airflow limitation, which is highly characteristic of asthma [1:20][5:6].
- Clinical Nuance: While a positive response indicates significant, reversible smooth muscle constriction, it does not exclude COPD, and a negative response does not exclude asthma, as airway responsiveness can fluctuate clinically over time [1:21][5:7].
¶ Key Specs & Modalities
[Full Pulmonary Function Testing (PFT) Panel]
|
+------------------+------------------+
| |
[Spirometry] [Advanced Modalities]
|- FEV1, FVC (Dynamic Flows) |- Body Plethysmography (TLC, RV, FRC)
|- Bronchodilator Reversibility |- DLCO (Gas Transfer/Diffusion)
|- Oscillometry (FOT/IOS - Impedance)
|- Nitrogen Washout (MBW - LCI)
While spirometry is the foundational diagnostic test, comprehensive assessment of complex respiratory disorders often requires a complete PFT panel that integrates several distinct advanced modalities [1:22][14]:
¶ Standard Spirometry
Measures dynamic flows and exhaled volumes [1:23]. It is highly sensitive to airway narrowing and is the first-line tool for confirming obstructive ventilatory defects, but it cannot directly measure static lung volumes or gas transfer [1:24][11:3].
¶ Body Plethysmography
A patient sits inside a sealed, airtight cabinet (plethysmograph) and performs gentle breathing maneuvers against a shutter [1:25]. By measuring changes in cabin pressure, this technique calculates the absolute volume of air in the lungs at various phases of the respiratory cycle [1:26]:
- Total Lung Capacity (TLC): The volume of air in the lungs after maximal inspiration. True restrictive lung function is defined clinically by a TLC below the lower limit of normal (TLC < LLN) [11:4].
- Residual Volume (RV): The volume of air remaining in the lungs after maximal exhalation.
- Functional Residual Capacity (FRC): The volume of air in the lungs at the end of a normal, quiet tidal exhalation.
- Clinical Value: Spirometry alone cannot diagnose restrictive lung disease. A low FVC on spirometry (FVC < LLN) has high specificity but low sensitivity for restriction; plethysmographic measurement of TLC is required to confirm a true restrictive defect and rule out obstructive air trapping [11:5].
¶ Diffusing Capacity for Carbon Monoxide (DLCO)
DLCO measures the transfer of a trace amount of carbon monoxide from inspired gas into blood over a brief single-breath hold (typically 10 seconds) [1:27]. It quantifies the efficiency of the alveolar-capillary membrane for gas exchange [1:28].
- Reduced DLCO: Indicates parenchymal destruction (such as emphysema) or alveolar-capillary thickening (such as interstitial lung disease/pulmonary fibrosis) [10:1][15][16]. It also occurs in pulmonary vascular diseases (e.g., pulmonary hypertension) [17] and as a non-statistically significant trend (p = 0.09) in systemic inflammatory states like pediatric inflammatory bowel disease [10:2] or chronic HIV infection [15:1].
- Preserved DLCO with Obstruction: Highly characteristic of asthma, helping differentiate it from COPD (emphysema), where DLCO is characteristically reduced [1:29].
¶ Forced Oscillation Technique (FOT) & Impulse Oscillometry (IOS)
FOT is an advanced, non-invasive technique that measures respiratory mechanics [18]. FOT superimposes small-amplitude pressure oscillations on normal, quiet tidal breathing [19][18:1].
- Mechanism: Because it requires no forced expiratory maneuvers or active patient cooperation, FOT is exceptionally suited for infants and preschool children (under 6 years of age) [20][21][19:1][18:2].
- Clinical Utility: FOT data, particularly measurements taken at lower frequencies, are highly sensitive to overall airway obstruction [18:3]. It is highly useful for tracking bronchial hyperresponsiveness and monitoring respiratory mechanics, although spirometry remains superior for detecting subtle treatment effects in older cooperative children [22][18:4].
¶ Multiple-Breath Washout (MBW) & Lung Clearance Index (LCI)
MBW tracks the clearance of an inert tracer gas (either resident nitrogen, or inhaled sulfur hexafluoride) from the lungs during tidal breathing of 100% oxygen [19:2][23].
- Lung Clearance Index (LCI): The number of lung volume turnovers required to clear the tracer gas [19:3][23:1].
- Clinical Utility: LCI is a highly sensitive index of ventilation inhomogeneity [19:4][23:2]. It is widely used in early-stage cystic fibrosis monitoring, where it can detect small airway disease and early ventilation changes before standard FEV1 or FVC spirometry show any detectable decline [19:5][23:3].
¶ Protocols & Clinical Applications
¶ Diagnostic vs. Screening Pathways
Pulmonary function testing follows two distinct clinical pathways depending on the patient's presentation:
- Diagnostic Pathway: Initiated for symptomatic individuals (presenting with dyspnea, persistent cough, or wheezing) [1:30]. The pathway involves pre- and post-bronchodilator spirometry, often followed by DLCO and body plethysmography to precisely classify the nature, severity, and reversibility of any ventilatory defect [1:31][2:5].
- Screening Pathway: Aimed at identifying subclinical impairment in asymptomatic high-risk populations [1:32][14:1]. Screening protocols focus on identifying patients with significant exposure histories or risk factors [1:33][14:2]. When clinical indicators suggest underlying pathology, further diagnostic PFTs are recommended to ensure comprehensive assessment [14:3].
¶ Patient Cohort Monitoring
Spirometry is essential for tracking disease course and therapeutic efficacy in specific patient cohorts:
- Chronic Obstructive Diseases: In patients with established COPD, tracking the annual rate of FEV1 decline is a key clinical metric [24]. Huber regression is clinically useful for minimizing the confounding effects of outlier measurements and short test intervals when calculating individual FEV1 slopes from clinical datasets [24:1].
- Pre-COPD Risk Factors: In individuals without established COPD, monitoring longitudinal lung function decline helps identify those at high risk for disease development [25]. Pre-COPD indicators, such as chronic bronchitis, low peak expiratory flow (PEF), and small airway dysfunction, are associated with excessive lung function decline in both smoking and non-smoking cohorts [25:1].
- Post-Infectious Recovery: Survivors of severe respiratory infections require monitoring. While children recovering from uncomplicated SARS-CoV-2 show no long-term spirometric or gas-transfer abnormalities [26], post-tuberculosis patients present a high burden of chronic impairment, requiring systematic monitoring to guide post-TB clinical care [27][8:2].
- Systemic Inflammatory and Immune Disorders: Patients with primary immunodeficiency diseases (PIDs) on immunoglobulin replacement therapy often develop progressive, silent bronchiectasis due to subclinical infections [28]. However, surveys show wide clinical variation in monitoring frequency and a lack of standardized clinical pathways between centers, highlighting the need for consensus guidelines to optimize monitoring [28:1].
¶ Occupational, Environmental, and Smoking Contexts
- Smoking Behavior: Standard spirometry is highly sensitive to the toxic effects of tobacco smoke [29][17:1]. Early-onset smoking (initiating before age 18) is independently associated with severe ventilatory dysfunction, accelerated lung volume loss, and comorbid pulmonary hypertension in adulthood [17:2]. Switching to electronic cigarettes has been shown in randomized trials to significantly improve peripheral airway function (FEF25-75%) and rapidly resolve respiratory symptoms in quitters [29:1].
- Occupational Dusts: Workers exposed to industrial dusts, such as coal mining, require structured medical surveillance [30][4:1]. Longitudinal cohort studies show that new underground coal miners experience a non-linear, rapid decline in FEV1 within their first year of exposure, necessitating frequent early testing and rigorous interpretation of initial drops [4:2].
- Pre-COPD and Air Trapping: Non-smoking individuals exposed to secondhand tobacco smoke or occupational irritants may present with preserved standard spirometry but severe air trapping (RV/TLC > 0.35) and expiratory flow limitation [31]. In secondhand smoke-exposed cohorts, the presence of air trapping identifies a subset of patients with worse symptoms and reduced exercise capacity [31:1].
¶ Home Spirometers and Digital Health
The availability of consumer-facing digital home spirometers has enabled remote monitoring of lung function.
- Efficacy in Chronic Disease: In patients with progressive fibrotic disorders (such as unclassifiable progressive fibrosing interstitial lung disease), daily home spirometry has been utilized to monitor forced vital capacity (FVC) over time and evaluate treatment response [16:1].
- Longevity and Biological Age Extrapolation: While low FEV1 is a powerful independent predictor of all-cause and cardiovascular mortality in epidemiological cohorts [7:1], utilizing home spirometry in healthy, asymptomatic, non-exposed individuals to track "lung age" is a commercial extrapolation. In healthy adults, FEV1 and FVC follow a progressive decline without a plateau phase after peak maturation, while the FEV1/FVC ratio trajectory exhibits a gradual decline starting from childhood [2:6]. Routine testing in healthy consumer cohorts does not alter clinical management and can introduce unnecessary anxiety or false reassurance.
¶ Safety, Contraindications & Quality Control
¶ Clinical Contraindications
To ensure patient safety, spirometry testing requires general clinical stability and the patient's physical capacity to cooperate with forced expiratory maneuvers [1:34][5:8]. Testing is typically deferred in patients who are unable to cooperate or perform the forced maneuvers safely [1:35][5:9].
¶ Infection Control
Because high-velocity expiratory maneuvers can aerosolize respiratory droplets, clinical testing environments require strict infection prevention protocols to minimize cross-contamination risk and ensure patient and technician safety.
¶ False Reassurance and Longevity Extrapolation
- The Hazard of Normal Spirometry: Standard spirometry measures overall flow at the mouth; it is notoriously insensitive to early-stage or localized pathology in the peripheral airways (the "silent zone" of the lungs, representing airways <2 mm in diameter) [32][9:1][31:2]. A patient can have extensive subclinical emphysema, early pulmonary fibrosis, or severe small-airway dysfunction with a perfectly normal FEV1, FVC, and FEV1/FVC ratio [32:1][9:2][31:3].
- Extrapolating to Longevity: Maintaining a high FEV1 is correlated with healthspan and resistance to respiratory senescent decline. However, tracking FEV1 via daily or weekly home spirometry in asymptomatic, healthy individuals is clinically unsupported. Variations are more likely to reflect transient, harmless physiological fluctuations (such as recent cold water ingestion, which temporarily reduces FEV1 and FVC [33], or temporary acute fatigue) rather than actual structural changes.
¶ Symptom Red Flags
The presence of significant clinical indications—such as abnormal radiographic findings, chronic respiratory symptoms, or persistent exposures—regardless of a normal spirometry result, mandates advanced diagnostic assessment, including gas transfer analysis (DLCO) or thoracic imaging [1:36][14:4][2:7].
¶ FAQ
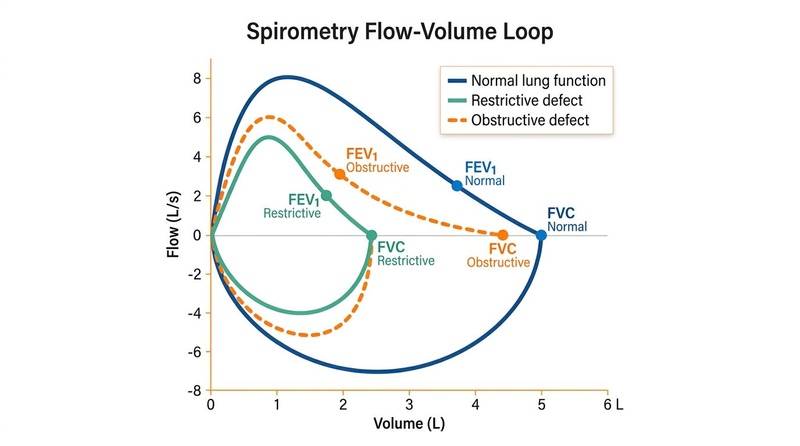
¶ What is the difference between a restrictive and an obstructive pattern on spirometry?
An obstructive pattern is defined by a disproportionate reduction in airflow relative to lung volume, indicated by an FEV1/FVC ratio below the Lower Limit of Normal (LLN) [1:37][11:6]. It is characteristic of asthma and COPD [1:38]. A restrictive pattern is characterized by a reduction in all lung volumes with a preserved FEV1/FVC ratio (ratio ≥ LLN but FVC < LLN) [11:7]. However, a low FVC on spirometry is not diagnostic of restriction; it merely suggests it, and true restrictive lung function must be confirmed by measuring Total Lung Capacity (TLC < LLN) via body plethysmography [11:8].
¶ Why is using a fixed 70% (0.70) cutoff for the FEV1/FVC ratio discouraged?
Using a fixed 0.70 cutoff does not account for the natural physiological aging of the lung [1:39]. As healthy individuals age, their lungs lose elastic recoil, causing the normal FEV1/FVC ratio to decline [1:40][2:8]. Applying a fixed 0.70 cutoff in older adults (e.g., over age 65) leads to high rates of false-positive diagnoses for COPD (over-diagnosis) [1:41]. Conversely, in young adults, the normal ratio is often 80–85%; a young patient with mild obstruction could have a ratio of 72%, which is abnormal for their age but would be missed by a fixed 0.70 threshold (under-diagnosis) [1:42]. Current standards require using the demographic-matched Lower Limit of Normal (LLN) [1:43][11:9].
¶ Can a person have lung disease if their spirometry results are completely normal?
Yes. Spirometry primarily assesses larger conducting airways and gross ventilatory capacity [32:2][9:3]. It is highly insensitive to early-stage small airway disease (airways <2 mm in diameter) [31:4], pulmonary vascular disorders (e.g., pulmonary hypertension) [17:3], and subclinical gas-transfer impairments (e.g., early interstitial lung disease, a non-statistically significant trend in pediatric IBD, or post-infectious parenchymal changes) [10:3][9:4]. Diagnosing these conditions requires advanced modalities such as Diffusing Capacity for Carbon Monoxide (DLCO), Multiple-Breath Washout (MBW), Forced Oscillation Technique (FOT), or high-resolution chest CT imaging [10:4][9:5][2:9].
¶ How does cold water ingestion affect spirometry results?
Ingesting large volumes of cold water (~2°C) has been shown in randomized crossover trials to cause a significant temporary reduction in lung function parameters [33:1]. Drinking 1000 mL of cold water significantly reduces FVC for at least 10 minutes and FEV1 for at least 15 minutes, whereas room-temperature water has no such effect [33:2]. To avoid confounding the measurement of lung function, individuals should avoid drinking cold water immediately prior to undergoing testing [33:3].
¶ What is Preserved Ratio Impaired Spirometry (PRISm)?
PRISm is a distinct category of abnormal lung function where a patient has a reduced FEV1 (FEV1 < 80% predicted) but a normal FEV1/FVC ratio (FEV1/FVC ≥ LLN) [34][7:2]. It is a highly heterogeneous state characterized by progressive longitudinal changes in lung function [34:1]. Despite the absence of classic airflow obstruction, patients with PRISm are at a significantly higher risk for acute respiratory exacerbations, cardiovascular diseases, and all-cause mortality, particularly if they are active smokers [34:2][7:3].
¶ References
Barkous B, Briki C, Boubakri S. Routine pulmonary lung function tests: Interpretative strategies and challenges. Chronic respiratory disease. 2024. https://pubmed.ncbi.nlm.nih.gov/39644209/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chen BX, Gao Y, Zheng JP. [Annual advances in clinical applications of pulmonary function testing 2025]. Zhonghua jie he he hu xi za zhi. 2026. https://pubmed.ncbi.nlm.nih.gov/41912392/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yu P, Luo Z, Wang Y. Preoperative inspiratory muscle training improves lung function prior to elective heart valve surgery and reduces postoperative lung function impairment and pulmonary complications: a randomised trial. Journal of physiotherapy. 2025. https://pubmed.ncbi.nlm.nih.gov/39675947/ ↩︎ ↩︎
Wang ML, Wu ZE, Du QG. A prospective cohort study among new Chinese coal miners: the early pattern of lung function change. Occupational and environmental medicine. 2005. https://pubmed.ncbi.nlm.nih.gov/16234407/ ↩︎ ↩︎ ↩︎
Oliva Hernández C, Gómez Pastrana D, Sirvent Gómez J. [Respiratory function assessment in cooperative patients. Part I. Spiromery and bronchodilator reversibility testing]. Anales de pediatria. 2007. https://pubmed.ncbi.nlm.nih.gov/17430717/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bolund AC, Miller MR, Sigsgaard T. The effect of organic dust exposure on long-term change in lung function: a systematic review and meta-analysis. Occupational and environmental medicine. 2017. https://pubmed.ncbi.nlm.nih.gov/28404791/ ↩︎
Li M, Chen M, Li Y. Association of preserved ratio impaired spirometry with mortality and cardiovascular diseases: a systematic review and meta-analysis. Systematic reviews. 2024. https://pubmed.ncbi.nlm.nih.gov/38971833/ ↩︎ ↩︎ ↩︎ ↩︎
Ivanova O, Hoffmann VS, Lange C. Post-tuberculosis lung impairment: systematic review and meta-analysis of spirometry data from 14 621 people. European respiratory review. 2023. https://pubmed.ncbi.nlm.nih.gov/37076175/ ↩︎ ↩︎ ↩︎
Gibbons JTD, Beaven ML, Course CW. Lung volumes, gas transfer and oscillometry after preterm birth: systematic review and meta-analysis. European respiratory review. 2025. https://pubmed.ncbi.nlm.nih.gov/40436611/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Moriki D, Drosakis I, Koumpagioti D. Pulmonary Function in Pediatric Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Pediatric pulmonology. 2026. https://pubmed.ncbi.nlm.nih.gov/41865300/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Myrberg T, Lindberg A, Eriksson B. Restrictive spirometry versus restrictive lung function using the GLI reference values. Clinical physiology and functional imaging. 2022. https://pubmed.ncbi.nlm.nih.gov/35225428/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Plantier L. [GLI reference values for lung function testing in France: At last! Now what next?]. Revue des maladies respiratoires. 2023. https://pubmed.ncbi.nlm.nih.gov/36801047/ ↩︎ ↩︎
Ivanova O, Khosa C, Bakuli A. Lung Function Testing and Prediction Equations in Adult Population from Maputo, Mozambique. International journal of environmental research and public health. 2020. https://pubmed.ncbi.nlm.nih.gov/32599726/ ↩︎ ↩︎
Task Forces on Pulmonary Function Testing from CACP, CTS, CGS. [Expert consensus on optimizing the multidisciplinary clinical pathways and management models for pulmonary function testing]. Zhonghua jie he he hu xi za zhi. 2026. https://pubmed.ncbi.nlm.nih.gov/41912385/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Konstantinidis I, Zou RH, Papageorgiou SN. Effect of Human Immunodeficiency Virus on Lung Function and Structure: A Systematic Review and Meta-Analysis. Annals of the American Thoracic Society. 2025. https://pubmed.ncbi.nlm.nih.gov/39417747/ ↩︎ ↩︎
Maher TM, Corte TJ, Fischer A. Pirfenidone in patients with unclassifiable progressive fibrosing interstitial lung disease: a double-blind, randomised, placebo-controlled, phase 2 trial. The Lancet. Respiratory medicine. 2020. https://pubmed.ncbi.nlm.nih.gov/31578169/ ↩︎ ↩︎
Gao H, Song Y, Liu K. The Impact of Different Smoking Behavior on Pulmonary Function and Pulmonary Hypertension Among Chinese Male Patients with Chronic Obstructive Pulmonary Disease. International journal of chronic obstructive pulmonary disease. 2024. https://pubmed.ncbi.nlm.nih.gov/38895046/ ↩︎ ↩︎ ↩︎ ↩︎
Oostveen E, MacLeod D, Lorino H. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. The European respiratory journal. 2003. https://pubmed.ncbi.nlm.nih.gov/14680096/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Jat KR, Agarwal S. Lung Function Tests in Infants and Children. Indian journal of pediatrics. 2023. https://pubmed.ncbi.nlm.nih.gov/37261706/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gangell CL, Hall GL, Stick SM. Lung function testing in preschool-aged children with cystic fibrosis in the clinical setting. Pediatric pulmonology. 2010. https://pubmed.ncbi.nlm.nih.gov/20425849/ ↩︎
Elenius V, Chawes B, Malmberg PL. Lung function testing and inflammation markers for wheezing preschool children: A systematic review. Pediatric allergy and immunology. 2021. https://pubmed.ncbi.nlm.nih.gov/33222297/ ↩︎
Tepper RS, Milner K, Harris J. Spirometry Versus Forced Oscillation to Assess Lung Function Outcome at 5 Years of Age. Pediatric pulmonology. 2025. https://pubmed.ncbi.nlm.nih.gov/39565207/ ↩︎
Amin R, Stanojevic S, Kane M. A randomized controlled trial to evaluate the lung clearance index as an outcome measure for early phase studies in patients with cystic fibrosis. Respiratory medicine. 2016. https://pubmed.ncbi.nlm.nih.gov/26856191/ ↩︎ ↩︎ ↩︎ ↩︎
Balasubramanian A, Cervantes C, Gearhart AS. Estimating rate of lung function change using clinical spirometry data. BMJ open respiratory research. 2024. https://pubmed.ncbi.nlm.nih.gov/39362797/ ↩︎ ↩︎
Fan J, Cong S, Zhang Y. Associations of pre-COPD indicators with lung function decline and their longitudinal transitions. Pulmonology. 2025. https://pubmed.ncbi.nlm.nih.gov/40353713/ ↩︎ ↩︎
Bakhtiari E, Moazzen N. Pulmonary function in children post -SARS-CoV-2 infection: a systematic review and meta-analysis. BMC pediatrics. 2024. https://pubmed.ncbi.nlm.nih.gov/38302891/ ↩︎
Lew YL, Tan AF, Yerkovich ST. Pulmonary function outcomes after tuberculosis treatment in children: a systematic review and meta-analysis. Archives of disease in childhood. 2024. https://pubmed.ncbi.nlm.nih.gov/37979964/ ↩︎
Jolles S, Sánchez-Ramón S, Quinti I. Screening protocols to monitor respiratory status in primary immunodeficiency disease. Clinical and experimental immunology. 2017. https://pubmed.ncbi.nlm.nih.gov/28708268/ ↩︎ ↩︎
Cibella F, Campagna D, Caponnetto P. Lung function and respiratory symptoms in a randomized smoking cessation trial of electronic cigarettes. Clinical science. 2016. https://pubmed.ncbi.nlm.nih.gov/27543458/ ↩︎ ↩︎
Ashuro Z, Debela BG, Daba C. The effect of occupational exposure to organic dust on lung function parameters among African industrial workers: a systematic review and meta-analysis. Frontiers in public health. 2024. https://pubmed.ncbi.nlm.nih.gov/39555040/ ↩︎
Zeng S, Nishihama M, Weldemichael L. Effect of twice daily inhaled albuterol on cardiopulmonary exercise outcomes, dynamic hyperinflation, and symptoms in secondhand tobacco-exposed persons with preserved spirometry and air trapping: a randomized controlled trial. BMC pulmonary medicine. 2024. https://pubmed.ncbi.nlm.nih.gov/38245665/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Brusasco V, Barisione G, Crimi E. Pulmonary physiology: future directions for lung function testing in COPD. Respirology. 2015. https://pubmed.ncbi.nlm.nih.gov/25257934/ ↩︎ ↩︎ ↩︎
Turner LA, Tiller NB. Lung function responses to cold water ingestion: A randomised controlled crossover trial. Respiratory physiology & neurobiology. 2023. https://pubmed.ncbi.nlm.nih.gov/37703924/ ↩︎ ↩︎ ↩︎ ↩︎
Yoon SM, Jin KN, Lee HJ. Acute Exacerbation and Longitudinal Lung Function Change of Preserved Ratio Impaired Spirometry. International journal of chronic obstructive pulmonary disease. 2024. https://pubmed.ncbi.nlm.nih.gov/38414720/ ↩︎ ↩︎ ↩︎