¶ Strength Training
Strength training, also known as progressive resistance training (PRT), is a physical exercise modality characterized by muscles contracting against an external resistance [1]. In longevity medicine, strength training serves as the primary clinical countermeasure to age-related neuromuscular decay and skeletal fragility, providing critical systemic adaptations that extend functional independence, optimize glucose metabolism, and significantly reduce all-cause mortality [2][3].
| Indication | Myofibrillar Hypertrophy, Sarcopenia Prevention, Bone Density Preservation, Insulin Sensitivity |
| Access | Behavioral Intervention |
| Dosing Sched | 2 to 3 sessions per week, targeting major muscle groups |
| Safety Profile | High (when technique and progression are managed) |
| Key Marker | 1-RM (estimated), Grip Strength, Appendicular Lean Mass (ALM), BMD T-score |
| Est. Cost | $0 (bodyweight) to Variable (gym membership/equipment) |
¶ At a glance
Key points:
- Essential for Longevity: Consistent progressive resistance training is associated with a 15% to 21% reduction in all-cause mortality [3:1].
- Combats Age-Related Decline: Effectively prevents sarcopenia (muscle loss) and osteopenia/osteoporosis (bone density loss) by stimulating muscle protein synthesis and bone remodeling [4][5].
- Metabolic Powerhouse: Skeletal muscle is the body's largest glucose clearing organ. Strength training enhances insulin sensitivity and glucose disposal, mitigating metabolic syndrome [6].
- Focus on Progressive Overload: Consistent increase in resistance, repetitions, or volume is the primary driver of continuous physiological adaptation [1:1].
- Form & Recovery First: Proper movement mechanics and adequate recovery intervals (48–72 hours) are paramount to prevent injury and optimize long-term progress [7][8].
What people use it for:
- Main goals: Muscle preservation (anti-sarcopenia), joint protection, metabolic health, skeletal density, physical power, and mobility support.
- Evidence quality: High (derived from extensive prospective cohort meta-analyses and randomized controlled trials).
¶ Safety "Traffic Light"
- ● GREEN LIGHT (Go): Individuals seeking to reverse muscle wasting, increase structural joint stability, lower metabolic risks, and protect skeletal integrity.
- ● YELLOW LIGHT (Caution): Individuals with managed hypertension, mild-to-moderate osteoarthritis, or historical joint injuries. Use machine-based movements (e.g., leg press instead of back squats) to stabilize pathways [8:1].
- ● RED LIGHT (Stop/Avoid): Individuals with acute, uncompensated cardiovascular disease (unstable angina, severe symptomatic aortic stenosis) or unhealed bone fractures [8:2].
¶ Protocol Card
| Parameter | The Foundational Strength Protocol | The Joint-Sparing/Geriatric Protocol | The Home/Minimalist Protocol |
|---|---|---|---|
| Frequency | 2–3 sessions per week | 2 sessions per week | 3 sessions per week |
| Duration | 45–60 minutes | 30–45 minutes | 15–20 minutes |
| Primary Tasks | Compound free-weight lifts: squats, deadlifts, overhead presses, rows. | Machine-dominant compound movements: seated leg press, chest press, lat pulldown. | Bodyweight or band-resisted movements: goblet box squats, push-ups, band rows. |
| Volume | 3–4 working sets of 6–10 repetitions per exercise (RPE 7-9 / RIR 1-3). | 2–3 working sets of 10–12 repetitions (RPE 6-7 / RIR 2-3). | 3 working sets of 12–15 repetitions near failure. |
¶ Bottom Line
Strength training is the gold-standard biological signal for preserving muscle mass and skeletal integrity, representing a non-negotiable cornerstone of healthy lifespan.
¶ The Neuromuscular and Bone Biology of Load
Resistance training triggers a cascade of physiological changes that extend far beyond simply "getting stronger."
¶ Henneman's Size Principle & Motor Unit Recruitment
Skeletal muscle contraction is coordinated by the nervous system. According to Henneman's Size Principle, motor units are recruited in a strict order from smallest to largest based on force demands:
- Low-Threshold Motor Units: Innervate small, fatigue-resistant Type I (slow-twitch) fibers, used for low-intensity activities (e.g., walking, posture).
- High-Threshold Motor Units: Innervate large, powerful Type II (fast-twitch) fibers, recruited only when force demands are high (e.g., lifting heavy loads, explosive movements) [9].
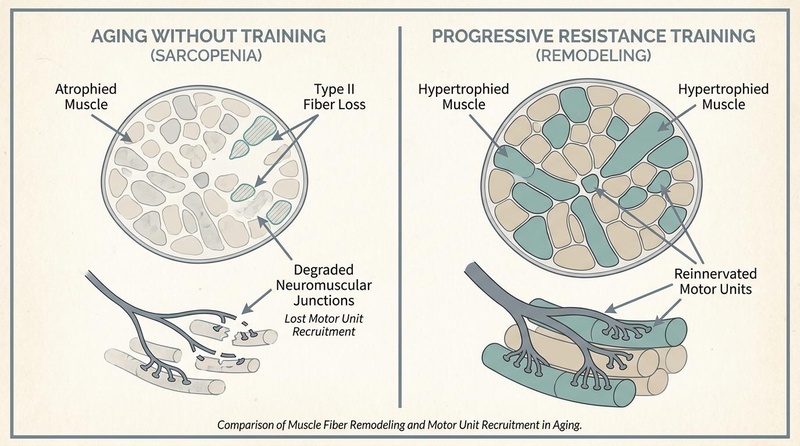
In sedentary aging, high-threshold motor units suffer from selective denervation. Because daily life rarely demands high-force outputs, the motor neurons connecting to Type II fibers atrophy and die, leading to irreversible loss of these fast-twitch fibers. Engaging in progressive resistance training forces the central nervous system to recruit high-threshold motor units, stimulating and preserving these critical neural pathways [4:1][[9:1]][[10]].
¶ Type II Fiber Preservation and the Strength-Power Continuum
Sarcopenia is primarily a disease of Type II fiber atrophy. While Type I fibers remain relatively preserved with age, Type II fibers shrink preferentially and can decrease in number by up to 50% over the lifespan if unmitigated [9:2].
This atrophy directly impacts:
- Absolute Strength: The maximum force a muscle can exert at any velocity (critical for carrying heavy loads, preventing joint failure).
- Power (Rate of Force Development): The ability to exert force quickly (force × velocity). Power is the single most critical motor metric in aging; it is the ability to rapidly contract muscles to catch oneself during a slip or trip. Power declines at twice the rate of absolute strength in older adults, making high-velocity or explosive resistance training a clinical necessity for fall prevention [5:1].
¶ Bone Remodeling and Mechanotransduction
During progressive resistance training, the mechanical pull of muscle tendons on bone tissue creates local shear stress. This load activates osteocytes—the sensory cells within bones—which trigger the activity of osteoblasts to lay down calcium phosphate [5:2]. This mechanotransduction process is highly load-dependent: high-intensity resistance training (>70-80% 1-RM) is required to successfully stimulate bone remodeling and prevent osteopenia and osteoporotic fracture risk [5:3][11].
¶ Does It Work? (Evidence Snapshot)
The efficacy of strength training across various biological and functional outcomes is supported by extensive human literature:
| Outcome | Typical Effect | Certainty | Timeframe | Citations |
|---|---|---|---|---|
| All-Cause Mortality | High | Cohort longitudinal | [2:1][3:2][1:2] | |
| Sarcopenia (Muscle Mass) | High | 10–12 weeks | [4:2][12] | |
| Bone Density (BMD) | High | 6–12 months | [5:4][11:1] | |
| Insulin Sensitivity | High | 6–12 weeks | [6:1][13] | |
| Cardiovascular Protection | High | Cohort longitudinal | [3:3][8:3] |
¶ Practical Protocols: Progressive Overload & Integration
To build a program that matches your background, lifestyle, or physiological age, focus on the core principles of Progressive Overload and Symmetric Movement Patterns:
¶ The 4 Pillars of Movement Selection
A complete resistance routine should incorporate these four fundamental movements:
- Knee-Dominant (Squat/Lunge): Targets quadriceps, gluteus maximus, and calves.
- Hip-Dominant (Hinge/Deadlift): Targets gluteal complex, hamstrings, and erector spinae.
- Upper-Body Push (Press/Push-up): Targets pectorals, anterior deltoids, and triceps.
- Upper-Body Pull (Row/Pull-up): Targets latissimus dorsi, rhomboids, biceps, and grip.
¶ progressive overload Strategies
The body adapts quickly to resistance. To trigger continuous muscle protein synthesis and tissue remodeling, you must gradually increase the mechanical stress over time:
- Load Increase: Increase the weight lifted once you can easily complete your target reps.
- Repetition Increase: Keep the weight the same but perform more repetitions per set.
- Volume Increase: Perform an additional set of an exercise.
- Tempo and Control: Perform the eccentric (lowering) portion of the lift more slowly, increasing time-under-tension.
¶ Safety, Contraindications, and Red Flags
¶ Absolute Contraindications (Avoid exercise until cleared by a physician)
- Unstable angina
- Recent heart attack (within 2 days)
- Uncontrolled cardiac arrhythmias causing symptoms
- Decompensated heart failure [8:4]
¶ Drug and Supplement Interactions
- Statins: Some patients on lipid-lowering statins experience muscle pain or weakness (statin-induced myalgia), which can be exacerbated by intense resistance training. Monitor symptoms and adjust loads if needed.
- Corticosteroids: Chronic use of oral glucocorticoids blocks muscle protein synthesis, accelerating muscle wasting (steroid myopathy). Resistance training is highly indicated to combat this loss, but progressive intensity must be closely monitored to protect thinner connective tissues.
- Creatine Monohydrate: A highly researched, safe compound that enhances phosphocreatine resynthesis, leading to significant increases in absolute strength, muscle mass, and bone density when paired with resistance exercise in older cohorts [11:2].
¶ Tracking & What “Good” Looks Like
| Metric | Target Goal | Frequency of Measurement |
|---|---|---|
| Appendicular Lean Mass (ALM) | Maintain in the upper quartiles for age/sex | Annually (via DEXA scan) [1:3] |
| Bone Mineral Density (BMD) | T-Score above -1.0 (Normal) | Every 1–2 years (via DEXA scan) [5:5] |
| Grip Strength (kg) | >27 kg for men; >16 kg for women | Quarterly (using hand dynamometer) [1:4] |
| 1-RM Squat/Leg Press | Maintain a 1.0–1.5x bodyweight equivalent capacity | Quarterly |
| Fasting Insulin | < 5.0 uIU/mL (improved glycemic clearance) | Annually |
¶ FAQs
¶ How often should I strength train for longevity?
For general health and longevity, 2 to 3 sessions per week targeting all major muscle groups is highly effective and supported by clinical evidence [1:5][14].
¶ Can older adults safely lift heavy weights?
Yes. Numerous clinical trials, including studies on frail individuals in their late 80s and 90s, prove that progressive high-intensity resistance training is exceptionally safe and highly effective at reversing frailty and improving bone density when properly progressed [4:3][[5:6]].
¶ References
¶ Update Log
- 2026-07-07: Initial publication of the canonical Strength Training page.
Momma H, Kawakami R, Honda T, et al. Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: a systematic review and meta-analysis of cohort studies. British Journal of Sports Medicine. 2022;56(13):755-763. https://bjsm.bmj.com/content/56/13/755 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Saeidifard F, Medina-Inojosa JR, West CP, et al. The association of resistance training with mortality: A systematic review and meta-analysis. European Journal of Preventive Cardiology. 2019;26(15):1647-1665. https://pubmed.ncbi.nlm.nih.gov/31104484/ ↩︎ ↩︎
Shailendra P, Baldock KL, Li LSK, et al. Resistance Training and Mortality Risk: A Systematic Review and Meta-Analysis. American Journal of Preventive Medicine. 2022;63(2):277-285. https://pubmed.ncbi.nlm.nih.gov/35599175/ ↩︎ ↩︎ ↩︎ ↩︎
Fiatarone MA, O'Neill EF, Ryan ND, et al. Exercise training in very elderly people. New England Journal of Medicine. 1994;330(23):1769-1775. https://www.nejm.org/doi/full/10.1056/NEJM199406233302501 ↩︎ ↩︎ ↩︎ ↩︎
Shen YC, Chen KH, Hou WH. Effectiveness of High-Intensity Versus Low-To-Moderate-Intensity Resistance Training in Improving Muscle Strength and Bone Mineral Density in Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Geriatrics & Gerontology International. 2026;26(7):112-121. https://pubmed.ncbi.nlm.nih.gov/42366614/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Młynarska E, Leszto K, Katańska K. Creatine Supplementation Combined with Exercise in the Prevention of Type 2 Diabetes: Effects on Insulin Resistance and Sarcopenia. Nutrients. 2025;17(17):2890. https://pubmed.ncbi.nlm.nih.gov/40944248/ ↩︎ ↩︎
Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. British Journal of Sports Medicine. 2014;48(11):871-877. https://pubmed.ncbi.nlm.nih.gov/24100287/ ↩︎
Williams MA, Feigenbaum MS, Jerôme GJ, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update: A Scientific Statement From the American Heart Association. Circulation. 2023;148(24):1962-1985. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001189 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lexell J, Taylor CC, Sjöström M. Ageing atrophy: number/size/proportion of fiber types in vastus lateralis (15–83 y). Journal of the Neurological Sciences. 1988;84(2-3):275-294. https://www.sciencedirect.com/science/article/abs/pii/0022510X88901245 ↩︎ ↩︎ ↩︎
Casolo A, Del Vecchio A, Goodlich BI, et al. Ageing does not impair motor neuron adaptations: comparable motor unit responses to strength training in young and older adults. The Journal of Physiology. 2026;604(1):21-39. https://pubmed.ncbi.nlm.nih.gov/41823343/ ↩︎
Naddafha S, Antonio J, Kreider RB. Creatine monohydrate for lean mass, strength, and bone density in postmenopausal women: a systematic review and meta-analysis. Journal of the International Society of Sports Nutrition. 2026;23(1):45-56. https://pubmed.ncbi.nlm.nih.gov/42141930/ ↩︎ ↩︎ ↩︎
Frontera WR, Meredith CN, O'Reilly KP, et al. Strength conditioning in older men: hypertrophy and function. Journal of Applied Physiology. 1988;64(3):1038-1044. https://journals.physiology.org/doi/abs/10.1152/jappl.1988.64.3.1038 ↩︎
Rosa JL, Dos Santos Lino MH, Grecco MV, et al. Effect of resistance training combined with carbohydrate and protein supplementation on the HOMA-IR, glycemic, lipid profile and hypertrophy of older adults with Type II Diabetes: secondary data analysis of a triple-blind RCT. Aging Clinical and Experimental Research. 2026;38(1):45-56. https://pubmed.ncbi.nlm.nih.gov/41931150/ ↩︎
World Health Organization. WHO guidelines on physical activity and sedentary behaviour. WHO Guidelines. 2020. https://www.who.int/publications/i/item/9789240015128 ↩︎