¶ Sunscreen and Photoprotection
Topical photoprotection and sunscreen formulations represent the primary clinically validated intervention for mitigating ultraviolet (UV) radiation-induced DNA damage, cutaneous carcinogenesis, and premature skin aging. This review provides a comprehensive clinical evaluation of sunscreen efficacy, transdermal filter kinetics, physiological interactions with vitamin D synthesis, drug-induced phototoxicity, and practical protocols for optimal skin protection.
| Indication | Skin cancer prevention (Melanoma, SCC), solar keratosis mitigation, and photoaging delay |
| Access | Over-the-Counter (OTC) / Topical Drug Monograph |
| Dosing Sched | Daily application (minimum 2.0 mg/cm²); reapply every 2 hours of continuous exposure |
| Safety Profile | High clinical safety; organic filters undergo substantial systemic absorption |
| Key Marker | Serum 25-hydroxyvitamin D [25(OH)D], skin erythema index, minimal erythema dose (MED) |
| Est. Cost | $10 - $40 / month (depending on mineral vs. stabilized organic formulation) |
¶ TL;DR
- What it is: Topical barrier formulations designed to absorb, reflect, or scatter ultraviolet radiation (UVA and UVB) to prevent skin injury.
- Main Benefits: Long-term reduction in squamous cell carcinoma (SCC) development [1] and invasive melanoma [2], alongside deceleration of solar keratosis acquisition [3] and prevention of exacerbations in photosensitive patients [4].
- Key Actions:
- Apply 2.0 mg/cm² of sunscreen daily to all sun-exposed skin surface areas [5].
- Reapply every 2 hours during continuous outdoor exposure, or immediately after swimming or heavy sweating.
- Select mineral-based inorganic filters (Zinc Oxide and Titanium Dioxide) which are inert and have virtually zero sensitization potential, making them highly tolerated and ideal for sensitive skin to minimize irritation and allergic contact dermatitis [6].
- Supplement with oral Vitamin D3 (e.g., at least 800–1000 IU/day) if practicing strict, year-round photoprotection [7].
¶ Quick Answer
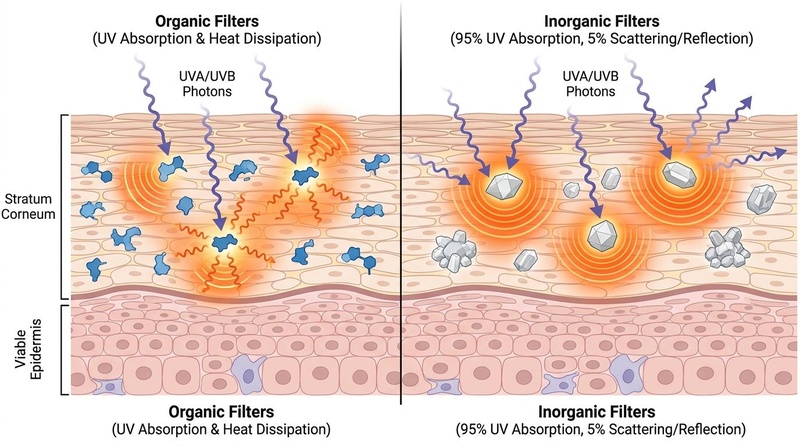
Topical sunscreens protect the skin by creating an active barrier that prevents ultraviolet photons from reaching the viable epidermis and dermis [8]. While organic filters absorb UV radiation to prevent phototoxic damage [8:1], inorganic mineral filters are historically characterized as physical blockers that reflect and scatter UV rays [6:1]. Long-term randomized clinical trials demonstrate that daily sunscreen use prevents skin malignancies and solar keratoses [2:1][1:1]. Despite laboratory evidence of complete vitamin D3 synthesis blockage under perfect application [9], real-world cohort data show that standard, sub-optimal user application does not compromise systemic vitamin D status in the general population [4:1][10].
¶ Photoprotection Modalities
Clinical photoprotection comprises several synergistic modalities designed to reduce cumulative ultraviolet radiation (UVR) exposure:
- UV Avoidance: Avoiding peak solar irradiance hours is a key behavior-based intervention. UV intensity is measured by the UV Index, with values of 3 or higher indicating a clear need for active photoprotection.
- UPF Clothing: Ultraviolet Protection Factor (UPF) clothing is rated by its ability to block both UVA and UVB transmission. A UPF 50 garment allows only 1/50th (2%) of UV radiation to pass through, representing a highly reliable barrier that is not subject to application and reapplication failures.
- Shade: Seeking shade reduces direct UV exposure [11]. However, diffuse (reflected) UV radiation from sand, concrete, water, or snow can still reach the skin, necessitating the concurrent use of topical sunscreens.
- Organic vs. Inorganic Filters: Sunscreens are classified as organic (chemical) or inorganic (mineral) based on their active filters. Organic filters (e.g., avobenzone, oxybenzone, octocrylene) are highly transparent and cosmetically elegant but carry risks of systemic absorption and allergic reactions [6:2][12]. Inorganic filters (Zinc Oxide, Titanium Dioxide) are extremely inert, photostable, and non-sensitizing, making them ideal for sensitive or hyper-reactive skin types [6:3].
- Vehicles: Topical sunscreens are formulated in various vehicles, including creams (ideal for dry skin/face), lotions/sprays (preferred for large body areas), and gels (ideal for oily or acne-prone skin). Sprays must be applied heavily and rubbed in to ensure an adequate, uniform 2.0 mg/cm² thickness.
¶ Evidence Snapshot
¶ Evidence Summary Table (Human Outcomes)
| Outcome / Goal | Effect | Consistency | Evidence Quality | Key Supporting Evidence | Clinical Notes (Population, Dosage, Duration) |
|---|---|---|---|---|---|
| Squamous Cell Carcinoma (SCC) | High | High (Tier 1) | Nambour Skin Cancer Trial [1:2] | Daily broad-spectrum SPF 15+ sunscreen over 4.5 years in adults; significantly reduced squamous cell carcinoma tumor counts. | |
| Invasive Melanoma | Moderate | High (Tier 1) | Nambour 15-Year Follow-up [2:2] | Daily application of SPF 15+ sunscreen; reduced invasive melanoma incidence by 73% (HR 0.27). | |
| Basal Cell Carcinoma (BCC) | = | High | High (Tier 1) | Nambour Cohort Analyses [13][1:3] | Daily sunscreen application during adulthood showed no statistically significant reduction in overall BCC. |
| Solar Keratoses (Actinic Keratoses) | High | High (Tier 1) | Nambour Skin Cancer Trial [3:1] | Daily application of SPF 15+ sunscreen significantly retards the acquisition and rate of solar keratoses in adults. | |
| Photosensitivity Disorders | High | High (Tier 2) | Passeron Consensus [4:2] | High-SPF broad-spectrum sunscreen protects against ultraviolet-induced flares in patients with photosensitivity disorders. | |
| Photoaging/Wrinkle progression prevention | High | High (Tier 1) | RCT [14] | Daily use of broad-spectrum SPF 15+ sunscreen vs. discretionary use over 4.5 years in healthy adults (<55 years); daily use resulted in 24% less photoaging and no detectable increase in skin aging [14:1]. | |
| Hyperpigmentation/Melasma management | High | Moderate (Tier 2) | RCT [15][16] | Broad-spectrum sunscreen alone (SPF 19, PA+++) thrice daily significantly improved MASI scores over 12 weeks [15:1]; tinted sunscreens blocking visible light prevent melasma relapses [16:1]. |
- Effect Magnitude: ↓↓↓ = Large clinically significant reduction; = = No statistically significant change.
- Consistency: High (most trials agree); Moderate (mixed but leaning one way).
- Evidence Quality: High (Tier 1/2) based on robust randomized controlled trials or large-scale clinical consensus.
¶ How it Works (Mechanism)
Sunscreen filters function through distinct photochemical and photophysical pathways to protect the skin from UVR damage:
¶ 1. Ultraviolet Radiation Damage Pathways
Solar radiation reaching the Earth's surface consists of ultraviolet B (UVB), ultraviolet A (UVA), and visible light [8:2][17].
- Direct DNA Damage (UVB): UVB photons are directly absorbed by epidermal DNA, leading to mutations that contribute to skin cancer (specifically squamous cell carcinoma) [8:3].
- Indirect Oxidative Damage (UVA & HEV): UVA photons penetrate deeper to generate reactive oxygen species, causing indirect oxidative damage, skin inflammation, barrier impairment, and photoaging as supported by [8:4] and [17:1].
- Visible Light Pigment Activation: High-Energy Visible (HEV) blue light (400–450 nm) contributes to cutaneous hyperpigmentation, particularly in darker Fitzpatrick skin types (IV–VI), by stimulating melanin synthesis.
¶ 2. Filter-Specific Mechanisms
- Organic (Chemical) Filters: Organic filters are carbon-based molecules—such as avobenzone, octocrylene, and homosalate [18]—that absorb UV radiation to prevent phototoxic damage [8:5]. By absorbing UV photons, these filters prevent the radiation from directly or indirectly damaging cellular structures and genetic material in the skin [8:6][17:2].
- Inorganic (Mineral) Filters: Inorganic mineral filters (such as Zinc Oxide and Titanium Dioxide) form a protective layer on the stratum corneum and are historically categorized as physical filters that reflect and scatter UV radiation [6:4].
¶ Application & Reapplication
Topical photoprotection is highly dependent on application density, uniform film formation, and reapplication frequency:
¶ 1. The 2.0 mg/cm² Density Standard
Sun Protection Factor (SPF) values are internationally standardized and tested using an application density of 2.0 mg/cm² of skin surface [5:1].
- Efficacy Reduction from Under-application: When sunscreen is applied below the standardized 2.0 mg/cm² density, the level of protection achieved is significantly lower than the labeled SPF [5:2]. Real-world application of approximately half the required amount (around 1.0 mg/cm²) fails to achieve the rated SPF, leaving the skin susceptible to UV-induced erythema and DNA damage [19][5:3].
- Real-World Application Gaps: In natural, uncontrolled settings, individuals typically apply only 0.5 to 1.0 mg/cm² of sunscreen (with a median of 0.79 mg/cm²), which represents less than half of the standard testing amount [5:4]. This widespread under-application results in sub-optimal photoprotection in daily practice [5:5].
¶ 2. Reapplication and Degradation Kinetics
- Photo-instability and Application Gaps: Many organic UV filters suffer from photo-instability and undergo photodegradation upon sunlight exposure, reducing their photoprotective efficacy [18:1]. Furthermore, because real-world application density is typically sub-optimal (often less than half the standardized 2.0 mg/cm² density) [5:6], implementing a double-application method before sun exposure [19:1] and regular reapplication is clinically recommended to maintain a uniform, cohesive barrier on the stratum corneum [4:3].
- Water Resistance and Formulation Care: Water-resistant sunscreen formulations are specifically engineered with hydrophobic polymers to maintain their protective film during environmental exposure. Under standardized testing, these products are certified for either 40-minute or 80-minute water resistance, representing the duration of water exposure after which reapplication is required.
¶ UVA/UVB Metrics
Evaluating a sunscreen's efficacy requires understanding different photobiological testing standards and labeling metrics:
- SPF (Sun Protection Factor): SPF measures protection against UVB-induced erythema (sunburn) [18:2]. It represents the ratio of the Minimal Erythema Dose (MED) on sunscreen-protected skin compared to unprotected skin. For example, SPF 30 means it takes 30 times more UVB energy to produce minimal redness compared to unprotected skin. It does not measure UVA protection.
- Broad-Spectrum Labeling: In the United States, a sunscreen can be labeled "Broad Spectrum" if its critical wavelength is . This indicates that the protection curve extends into the longer UVA wavelengths.
- PPD (Persistent Pigment Darkening) & PA Rating: Primarily used in Asia and Europe, PPD and the PA rating system measure protection against UVA-induced skin pigmentation, with higher ratings indicating greater protection against UVA radiation.
- Visible Light & HEV Mitigation: Standard organic and mineral filters do not absorb visible light or High-Energy Visible (HEV) blue light. To protect against visible light-induced hyperpigmentation and melasma, formulations frequently incorporate iron oxides (yellow, red, and black iron oxides) which act as visible light filters to reduce blue light-induced melanogenesis.
¶ Vitamin D Concerns
The potential impact of sunscreen use on cutaneous vitamin D synthesis is a major point of clinical interest:
¶ 1. The Photosynthesis Pathway
Vitamin D3 (cholecalciferol) is synthesized endogenously when UVB radiation strikes the skin, triggering the synthesis and activation of vitamin D3 [11:1][9:1]. Because sunscreens block UVB radiation to prevent erythema, they also theoretically block cholecalciferol synthesis [11:2].
- The Matsuoka Study: Early highly-controlled clinical evaluations demonstrated that applying sunscreen to the whole body completely blocked cutaneous cholecalciferol synthesis after a single, uniform UVB exposure in a laboratory setting [9:2]. This established that perfect, laboratory-grade sunscreen coverage acts as a complete block to photosynthesis.
¶ 2. Real-World Cohort Evidence
Despite laboratory findings, large-scale clinical cohorts and randomized field trials show that real-world sunscreen use does not cause vitamin D deficiency or compromise serum 25-hydroxyvitamin D [25(OH)D] status in healthy populations:
- The Sub-optimal Application Escape: In everyday practice, individuals apply far less than the recommended 2.0 mg/cm² density and frequently miss anatomical areas [19:2][5:7]. This sub-optimal coverage allows sufficient UVB transmission (UVB "leakage") to sustain healthy cutaneous vitamin D synthesis [19:3][10:1].
- The Nambour Cohort Findings: In an observational cohort analysis of the Nambour community, self-reported sunscreen use was not associated with lower serum 25(OH)D levels, even after adjusting for time outdoors and dietary intake [10:2].
- The Passeron International Consensus: An international panel of photobiologists, dermatologists, and endocrinologists concluded that broad-spectrum sunscreens used for daily and recreational photoprotection are highly unlikely to compromise vitamin D status in the general population [4:4].
- Meta-Analysis Nuances: A systematic review and meta-analysis of 9,470 participants by Gatta and Cappelli (2025) reported that while sunscreen use is associated with a statistically significant, but minor, reduction in serum 25(OH)D levels, this small decrease is clinically insignificant and does not induce parathyroid dysfunction or metabolic bone disease [20][21].
- Photosensitive Populations: Rigorous photoprotection protocols (including high-SPF sunscreens, protective clothing, and shade-seeking behaviors) are highly likely to compromise vitamin D status in patients with photosensitivity disorders (such as lupus erythematosus or xeroderma pigmentosum) [4:5][22]. For these clinical subgroups, serum 25(OH)D screening and oral cholecalciferol supplementation (e.g., at least 800–1000 IU/day [7:1] or at least 400 IU/day [22:1]) are recommended.
¶ Photosensitizing Medications
A wide variety of systemic and topical medications act as exogenous photosensitizing agents, altering the skin's response to ultraviolet radiation:
¶ 1. Phototoxicity vs. Photoallergy Pathways
- Phototoxicity (Non-immunological): In phototoxicity, the photosensitizing drug interacts with solar UV radiation present on the skin, inducing direct tissue damage [23]. This typically manifests as an exaggerated sunburn-like response localized to sun-exposed areas [23:1][24].
- Photoallergy (Cell-Mediated Immunity): In photoallergy, the photosensitizing agent undergoes a UV-induced chemical change that triggers an immunologic cell-mediated reaction, which can present as an eczematous eruption [23:2][6:5].
¶ 2. High-Risk Drug Classes
For patients prescribed these medications, strict daily broad-spectrum photoprotection is clinically necessary to prevent severe cutaneous eruptions [23:3][25]. Best-practice clinical advice recommends high-SPF, broad-spectrum mineral sunscreens () due to their photostability and extremely low skin sensitization potential.
- Cardiovascular Agents: Amiodarone (a photosensitizing cardiac agent) and Thiazide Diuretics (a frequent cause of phototoxicity) [23:4][25:1][24:1].
- Antibiotics: Tetracyclines (which can induce phototoxic reactions presenting as easy sunburn) [25:2], as well as general photosensitizing antibiotics [23:5].
- Nonsteroidal Anti-inflammatory Drugs (NSAIDs): NSAIDs are associated with phototoxic and photoallergic responses [23:6], while drug-induced pseudoporphyria represents an uncommon phototoxic dermatosis that can be triggered by various medications [26].
- Retinoids: Retinoids are capable of inducing phototoxic reactions [23:7].
¶ 3. Drug-Induced Pseudoporphyria
Pseudoporphyria is an uncommon, drug-induced phototoxic dermatosis that clinically and histologically mimics Porphyria Cutanea Tarda (PCT) but presents with normal porphyrin profiles in the blood, urine, and stool [26:1].
- Etiology: Associated with chronic renal failure, hemodialysis, or certain medications [26:2].
- Pathophysiology: Phototoxic metabolites of these drugs accumulate in the skin and, upon UV exposure, trigger skin fragility, subepidermal tense bullae (blisters), milia, and scarring on the dorsum of the hands and face [26:3].
- Clinical Management: Diagnosis requires confirming normal porphyrin levels and performing a Wood's lamp examination of the urine (which does not show the coral-red fluorescence characteristic of true porphyria) [26:4]. Treatment involves discontinuing the photosensitizing drug, administering oral hydroxychloroquine in refractory cases, and implementing strict broad-spectrum UV protection [26:5].
¶ 4. Phytophotodermatitis
Phytophotodermatitis is a phototoxic skin reaction induced by cutaneous contact with certain plants or plant extracts followed by exposure to sunlight [27]. These phototoxic agents can be found in botanicals, including carrots [27:1].
- Carrot-Extract Sunscreens: Some commercial "natural" sunscreens incorporate botanical oils or plant extracts. Clinical case reports have documented severe phytophotodermatitis after the use of carrot-extract-containing sunscreens [27:2]. Patients present with burning, erythema, patches, plaques, vesicles, bullae, or hyperpigmented patches in well-demarcated and unusual shapes [27:3].
¶ Allergy, Irritation, and Safety
Sunscreen formulations are generally well-tolerated, but adverse cutaneous and systemic pharmacokinetic behaviors require clinical monitoring:
¶ 1. Adverse Dermatological Reactions
- Irritant Contact Dermatitis: The most common adverse reaction, presenting as immediate localized burning, stinging, or erythema, particularly in areas with a compromised skin barrier [6:6]. This is a non-immunological reaction typically driven by product excipients (such as alcohols, emulsifiers, or preservatives) rather than the active UV filters [6:7][28].
- Allergic Contact Dermatitis: A Type IV cell-mediated hypersensitivity reaction [6:8]. Organic UV filters, particularly Oxybenzone (Benzophenone-3), are the most frequent culprits, followed by avobenzone, octocrylene, and fragrance compounds [6:9]. Inorganic filters (Zinc Oxide, Titanium Dioxide) are extremely inert and possess virtually zero sensitization potential [6:10].
- Photoallergic Contact Dermatitis: A rare reaction where a UV filter only becomes immunologically active after absorbing UV light, which alters its chemical structure and forms a hapten that binds to skin proteins [6:11]. Avobenzone and oxybenzone are the most common causes [6:12].
¶ 2. Systemic Absorption Kinetics
The transdermal absorption of organic UV filters has been a primary subject of regulatory scrutiny:
- The FDA Maximal-Use Trials: In randomized clinical trials conducted by the FDA under maximal-use conditions (applying 2.0 mg/cm² sunscreen to 75% of body surface area, 4 times daily for 4 days), all 6 tested organic UV filters (avobenzone, oxybenzone, octocrylene, homosalate, octisalate, and octinoxate) exceeded the FDA's systemic absorption threshold of 0.5 ng/mL [12:1].
- Plasma Concentrations: Organic UV filters undergo significant systemic absorption, with oxybenzone demonstrating the highest plasma concentrations followed by other active ingredients such as avobenzone and octocrylene [12:2][29]. In randomized trials under maximal-use conditions, organic filters were absorbed into systemic circulation, exceeding the FDA threshold of 0.5 ng/mL, with blood concentrations monitored over multiple days [12:3][29:1].
- Pharmacokinetic Modeling: Physiologically based pharmacokinetic (PBPK) modeling and in vitro skin permeation testing (IVPT) confirm that these lipophilic organic filters cross the stratum corneum and distribute systemically [30][31].
- Clinical Context: The FDA has classified these organic filters as Category III (requiring additional safety and nonclinical toxicology data to be declared GRASE - Generally Recognized as Safe and Effective) [18:3][28:1]. However, there is currently no human clinical evidence linking systemic organic filter exposure to endocrine disruption or adverse health outcomes [28:2].
¶ Environmental Claims & Regulatory Differences
The regulation and marketing of UV filters vary significantly between geographical regions and jurisdictions:
¶ 1. "Reef-Safe" and Environmental Claims
- Coral Bleaching: In vitro and laboratory-based studies suggest that organic UV filters represent an additional contributing factor to coral bleaching, which has led several localities to ban certain organic filters [28:3].
- Legislative Bans: These findings have led several jurisdictions to implement legislative bans on the sale and use of sunscreens containing certain organic filters [18:4][28:4].
- The "Reef-Safe" Designation: While often used as a commercial marketing term, it is frequently associated with formulations that exclude certain organic filters linked to environmental concerns, in response to regulatory evaluations of filter safety [28:5].
¶ 2. FDA vs. European Union Regulatory Frameworks
- United States (FDA): Sunscreens are regulated as Over-the-Counter (OTC) drugs [32]. Under the FDA's regulatory framework, several organic UV filters—including avobenzone, octocrylene, oxybenzone, octinoxate, octisalate, and homosalate—are classified as Category III Non-GRASE (Generally Recognized as Safe and Effective) due to ongoing evaluation regarding their systemic absorption and photostability [18:5][28:6].
- European Union (EMA/EC): European regulatory frameworks treat sunscreens as cosmetics rather than OTC drugs, employing different regulatory pathways and approval criteria for UV filters.
¶ Starter Protocol
To ensure uniform film formation and optimal photoprotection, implement this standardized daily protocol:
- Skin Preparation: Apply sunscreen as the final step of the morning topical routine. Ensure any underlying serums or moisturizers are fully absorbed to prevent diluting or disrupting the sunscreen's protective film.
- The 2-Finger Rule: To achieve the recommended 2.0 mg/cm² density on the face and neck, extrude two continuous strips of sunscreen along the entire length of the index and middle fingers (equivalent to approximately 1.0 to 1.25 mL).
- Application Technique: Apply the sunscreen evenly to the face, neck, ears, and posterior neck. Use gentle, sweeping motions rather than aggressive rubbing, which can disrupt film formation.
- The Double-Application Technique: For optimal coverage and to minimize human error, apply two consecutive layers of sunscreen before sun exposure [19:4].
- Drying Window: Allow the sunscreen to dry and bind to the stratum corneum for 15 to 30 minutes before outdoor activity or applying cosmetics.
¶ Common Application Failures
- Anatomical Omission: Failing to apply sunscreen to high-risk areas, particularly the ears, lateral neck, dorsum of the hands, and the scalp (especially in individuals with thinning hair).
- Sub-optimal Thickness: Under-applying the product (applying <1.0 mg/cm²) due to concerns over cosmetic elegance or white cast, which exponentially reduces the achieved SPF [19:5][5:8].
- Spraying and Praying: Using aerosol or pump sprays without rubbing the product in, or spraying in windy conditions, which results in a patchy, uneven protective film.
- Neglecting Cloudy or Overcast Days: Failing to apply sunscreen on cloudy days. Up to 80% of solar UV radiation (especially UVA) penetrates light cloud cover, leading to cumulative, unmonitored dermal damage [8:7].
- Failing to Reapply: Omitting regular reapplication during continuous sun exposure, which is necessary to maintain a uniform and effective photoprotective film on the stratum corneum [4:6][19:6].
¶ Tracking Plan
- Clinical Skin Examinations: Schedule annual or bi-annual full-body skin checks with a dermatologist to screen for early cutaneous malignancies or solar keratoses.
- Serum 25-Hydroxyvitamin D [25(OH)D] Testing: Vitamin D screening should be restricted to those at risk of hypovitaminosis, such as patients with photosensitivity disorders who require rigorous photoprotection [4:7].
- Erythema Monitoring: Monitor for any occurrences of sunburn or post-exposure erythema as a clinical sign of potential photoprotection failure.
- Minimal Erythema Dose (MED) & Photosensitivity Assessment: In clinical settings, phototesting and photoprovocation tests can be utilized to evaluate patient photosensitivity, though they are rarely required for routine diagnosis [25:3]. Additionally, photopatch testing is utilized to diagnose photocontact dermatitis and identify specific contact photoallergens, such as sunscreen ingredients or fragrances [24:2].
¶ Safety & Red Flags
¶ 1. The ABCDE Criteria for Melanoma
Clinically evaluate any pigmented lesions using the standardized ABCDE criteria:
- A - Asymmetry: One half of the mole or lesion does not match the other.
- B - Border: The borders are irregular, scalloped, poorly defined, or notched.
- C - Color: The color is non-uniform, featuring shades of brown, black, red, white, or blue.
- D - Diameter: The lesion's diameter is greater than 6 mm (the size of a pencil eraser), though melanomas can sometimes be smaller.
- E - Evolving: The mole or lesion is changing in size, shape, color, or elevation, or is associated with new symptoms such as bleeding, itching, or crusting.
¶ 2. Clinical Warning Signs of Non-Melanoma Skin Cancers (NMSCs)
- General Skin Monitoring: High-risk populations should monitor for any new, changing, or persistent skin lesions, which warrants regular dermatologist checks for basal cell carcinoma, squamous cell carcinoma, and solar keratoses as supported by clinical evaluations [3:2][1:4].
¶ FAQs
¶ Does daily sunscreen use cause Vitamin D deficiency?
No. While perfect, laboratory-controlled sunscreen application blocks UVB absorption and cutaneous cholecalciferol synthesis, real-world application does not compromise vitamin D status in healthy populations [4:8][33]. Normal human application is sub-optimal in quantity and coverage, leaving sufficient skin exposed to synthesize baseline vitamin D requirements [19:7]. Healthy individuals do not need to avoid sunscreen to maintain vitamin D levels [33:1].
¶ What is the clinical difference between organic and mineral sunscreens?
Organic (chemical) sunscreens contain carbon-based molecules that absorb UV photons and dissipate them as heat. They are transparent and cosmetically elegant but can undergo systemic absorption and cause contact allergies [6:13][12:4]. Mineral (inorganic) sunscreens contain Zinc Oxide or Titanium Dioxide, which function through both absorption and reflection/scattering of UV radiation. They are highly photostable, inert, and have virtually zero sensitization potential, making them highly tolerated and ideal for sensitive skin to minimize irritation and allergic contact dermatitis [6:14].
¶ What are "reef-safe" sunscreens?
"Reef-safe" is a commercial marketing term frequently associated with formulations that exclude certain organic filters linked to environmental concerns [28:7]. While climate change is the primary driver of coral bleaching, some laboratory studies suggest that certain organic filters represent an additional contributing factor, prompting several localities to implement bans on products containing these filters [28:8].
¶ How do photosensitizing medications interact with sunlight?
Upon interaction of solar UV radiation with the chemical present in significant levels on the skin, phototoxic or photoallergic reactions may occur in susceptible patients [23:8]. Common photosensitizing drug classes include diuretics, cardiac agents (such as amiodarone), antibiotics, retinoids, and nonsteroidal anti-inflammatory drugs [23:9][25:4]. These reactions can present as easy sunburn or eczematous eruptions, requiring strict daily broad-spectrum photoprotection [23:10][25:5].
¶ What is drug-induced pseudoporphyria?
Pseudoporphyria is an uncommon dermatosis mimicking Porphyria Cutanea Tarda, characterized by extreme skin fragility, blistering, and scarring on sun-exposed areas [26:6]. It is a phototoxic reaction triggered by certain medications or chronic hemodialysis in the presence of UV light [26:7]. Porphyrin levels in these patients are completely normal [26:8].
¶ References
Green A, Williams G, Neale R, et al. Daily sunscreen application and betacarotene supplementation in prevention of basal-cell and squamous-cell carcinomas of the skin: a randomised controlled trial. Lancet. 1999 Aug 28;354(9180):723-729. doi:10.1016/S0140-6736(98)12168-2. https://pubmed.ncbi.nlm.nih.gov/10475183/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Green AC, Williams GM, Logan V, et al. Reduced melanoma after regular sunscreen use: randomized trial follow-up. Journal of Clinical Oncology. 2011 Jan 20;29(3):257-263. doi:10.1200/JCO.2010.28.7078. https://pubmed.ncbi.nlm.nih.gov/21135266/ ↩︎ ↩︎ ↩︎
Darlington S, Williams G, Neale R, et al. A randomized controlled trial to assess sunscreen application and beta carotene supplementation in the prevention of solar keratoses. Archives of Dermatology. 2003 Apr;139(4):451-455. doi:10.1001/archderm.139.4.451. https://pubmed.ncbi.nlm.nih.gov/12707092/ ↩︎ ↩︎ ↩︎
Passeron T, Bouillon R, Callender V, et al. Sunscreen photoprotection and vitamin D status. The British Journal of Dermatology. 2019 Nov;181(5):916-931. doi:10.1111/bjd.17992. https://pubmed.ncbi.nlm.nih.gov/31069788/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Neale R, Williams G, Green A. Application patterns among participants randomized to daily sunscreen use in a skin cancer prevention trial. Archives of Dermatology. 2002 Oct;138(10):1319-1324. doi:10.1001/archderm.138.10.1319. https://pubmed.ncbi.nlm.nih.gov/12374537/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ludriksone L, Elsner P. Adverse Reactions to Sunscreens. Current Problems in Dermatology. 2021;55:140-151. doi:10.1159/000517631. https://pubmed.ncbi.nlm.nih.gov/34698020/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Holick MF. Optimal vitamin D status for the prevention and treatment of osteoporosis. Drugs & Aging. 2007;24(12):1017-1029. doi:10.2165/00002512-200724120-00005. https://pubmed.ncbi.nlm.nih.gov/18020534/ ↩︎ ↩︎
Li L, Chong L, Huang T. Natural products and extracts from plants as natural UV filters for sunscreens: A review. Animal Models and Experimental Medicine. 2023 Jun;6(3):201-213. doi:10.1002/ame2.12324. https://pubmed.ncbi.nlm.nih.gov/36536536/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Matsuoka LY, Wortsman J, Hollis BW. Use of topical sunscreen for the evaluation of regional synthesis of vitamin D3. Journal of the American Academy of Dermatology. 1990 May;22(5 Pt 1):772-775. doi:10.1016/0190-9622(90)70104-5. https://pubmed.ncbi.nlm.nih.gov/2161436/ ↩︎ ↩︎ ↩︎
Jayaratne N, Russell A, van der Pols JC, et al. Sun protection and vitamin D status in an Australian subtropical community. Preventive Medicine. 2012 Aug;55(2):145-148. doi:10.1016/j.ypmed.2012.05.016. https://pubmed.ncbi.nlm.nih.gov/22634425/ ↩︎ ↩︎ ↩︎
Stege H, Schwarz T. [Vitamin D and UV protection]. Der Hautarzt. 2017 May;68(5):341-346. doi:10.1007/s00105-017-3965-0. https://pubmed.ncbi.nlm.nih.gov/28432394/ ↩︎ ↩︎ ↩︎
Matta MK, Florian J, Zusterzeel R, et al. Effect of Sunscreen Application on Plasma Concentration of Sunscreen Active Ingredients: A Randomized Clinical Trial. JAMA. 2020 Jan 21;323(3):256-267. doi:10.1001/jama.2019.20747. https://pubmed.ncbi.nlm.nih.gov/31961417/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pandeya N, Purdie DM, Green A, et al. Repeated occurrence of basal cell carcinoma of the skin and multifailure survival analysis: follow-up data from the Nambour Skin Cancer Prevention Trial. American Journal of Epidemiology. 2005 Apr 15;161(8):748-754. doi:10.1093/aje/kwi100. https://pubmed.ncbi.nlm.nih.gov/15800267/ ↩︎
Hughes MC, Williams GM, Baker P, et al. Sunscreen and prevention of skin aging: a randomized trial. Annals of Internal Medicine. 2013 Jun 4;158(11):781-790. doi:10.7326/0003-4819-158-11-201306040-00002. https://pubmed.ncbi.nlm.nih.gov/23732711/ ↩︎ ↩︎
Sarkar R, Ghunawat S, Narang I. Role of broad-spectrum sunscreen alone in the improvement of melasma area severity index (MASI) and Melasma Quality of Life Index in melasma. Journal of Cosmetic Dermatology. 2019 Aug;18(4):1066-1073. doi:10.1111/jocd.12911. https://pubmed.ncbi.nlm.nih.gov/31033184/ ↩︎ ↩︎
Boukari F, Jourdan E, Fontas E, et al. Prevention of melasma relapses with sunscreen combining protection against UV and short wavelengths of visible light: a prospective randomized comparative trial. Journal of the American Academy of Dermatology. 2015 Jan;72(1):189-190.e1. doi:10.1016/j.jaad.2014.08.023. https://pubmed.ncbi.nlm.nih.gov/25443629/ ↩︎ ↩︎
He H, Li A, Li S, et al. Natural components in sunscreens: Topical formulations with sun protection factor (SPF). Biomedicine & Pharmacotherapy. 2021 Feb;134:111161. doi:10.1016/j.biopha.2020.111161. https://pubmed.ncbi.nlm.nih.gov/33360043/ ↩︎ ↩︎ ↩︎
Safian MT, Raja PB, Muniandy K. The dual challenge of FDA-evaluated non-GRASE UV filters: Photostability and systemic absorption - A path toward safer and more effective sunscreens. International Journal of Pharmaceutics. 2025 Jul 25;678:125580. doi:10.1016/j.ijpharm.2025.125580. https://pubmed.ncbi.nlm.nih.gov/40451593/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wulf HC, Philipsen PA. Improving Photoprotection and Implications for 25(OH)D Formation. Anticancer Research. 2020 Jan;40(1):503-509. doi:10.21873/anticanres.13979. https://pubmed.ncbi.nlm.nih.gov/31892606/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gatta E, Cappelli C. Sunscreen and 25-Hydroxyvitamin D Levels: Friends or Foes? A Systematic Review and Meta-Analysis. Endocrine Practice. 2025 Jun;31(6):540-548. doi:10.1016/j.eprac.2024.11.002. https://pubmed.ncbi.nlm.nih.gov/40246233/ ↩︎
Farrerons J, Barnadas M, Rodríguez J, et al. Clinically prescribed sunscreen (sun protection factor 15) does not decrease serum vitamin D concentration sufficiently either to induce changes in parathyroid function or in metabolic markers. The British Journal of Dermatology. 1998 Sep;139(3):422-427. doi:10.1046/j.1365-2133.1998.02404.x. https://pubmed.ncbi.nlm.nih.gov/9767286/ ↩︎
Cusack C, Danby C, Fallon JC, et al. Photoprotective behaviour and sunscreen use: impact on vitamin D levels in cutaneous lupus erythematosus. Photodermatology, Photoimmunology & Photomedicine. 2008 Oct;24(5):260-267. doi:10.1111/j.1600-0781.2008.00371.x. https://pubmed.ncbi.nlm.nih.gov/18811868/ ↩︎ ↩︎
Lankerani L, Baron ED. Photosensitivity to exogenous agents. Journal of Cutaneous Medicine and Surgery. 2004 Nov-Dec;8(6):424-431. doi:10.1177/120347540400800606. https://pubmed.ncbi.nlm.nih.gov/15988550/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hawk JL. Photosensitivity in the elderly. The British Journal of Dermatology. 1990 Apr;122(4):555-561. doi:10.1111/j.1365-2133.1990.tb08301.x. https://pubmed.ncbi.nlm.nih.gov/2186782/ ↩︎ ↩︎ ↩︎
Millard TP, Hawk JL, McGregor JM. Photosensitivity in lupus. Lupus. 2000;9(1):3-10. doi:10.1177/096120330000900102. https://pubmed.ncbi.nlm.nih.gov/10713641/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Jangid SD, Saoji V, Madke B. Drug-Induced Pseudoporphyria: A Case Report. Cureus. 2024 Apr;16(4):e58122. doi:10.7759/cureus.58122. https://pubmed.ncbi.nlm.nih.gov/38707054/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bosanac SS, Clark AK, Sivamani RK. Phytophotodermatitis related to carrot extract-containing sunscreen. Dermatology Online Journal. 2018 Jan 15;24(1):13030/qt2z240576. https://pubmed.ncbi.nlm.nih.gov/29469776/ ↩︎ ↩︎ ↩︎ ↩︎
Abdel Azim S, Bainvoll L, Vecerek N, et al. Sunscreens part 2: Regulation and safety. Journal of the American Academy of Dermatology. 2025 Apr;92(4):945-955. doi:10.1016/j.jaad.2024.05.025. https://pubmed.ncbi.nlm.nih.gov/38777185/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Matta MK, Zusterzeel R, Pilli NR, et al. Effect of Sunscreen Application Under Maximal Use Conditions on Plasma Concentration of Sunscreen Active Ingredients: A Randomized Clinical Trial. JAMA. 2019 Jun 4;321(21):2082-2091. doi:10.1001/jama.2019.5588. https://pubmed.ncbi.nlm.nih.gov/31058986/ ↩︎ ↩︎
Dancik Y, Zhang Y, Telaprolu KC, et al. Physiologically based pharmacokinetic modelling of in vitro skin permeation of sunscreen actives under various experimental conditions. International Journal of Pharmaceutics. 2025 Sep 15;681:125774. doi:10.1016/j.ijpharm.2025.125774. https://pubmed.ncbi.nlm.nih.gov/40681065/ ↩︎
Zhang J, Yang Y, Ashraf M, et al. An advanced automation platform coupled with mass spectrometry for investigating in vitro human skin permeation of UV filters and excipients in sunscreen products. Rapid Communications in Mass Spectrometry. 2022 Jun 15;36(11):e9294. doi:10.1002/rcm.9294. https://pubmed.ncbi.nlm.nih.gov/35178789/ ↩︎
Wang J, Ganley CJ. Safety Threshold Considerations for Sunscreen Systemic Exposure: A Simulation Study. Clinical Pharmacology & Therapeutics. 2019 Jan;105(1):161-167. doi:10.1002/cpt.1178. https://pubmed.ncbi.nlm.nih.gov/30094825/ ↩︎
Kannan S, Lim HW. Photoprotection and vitamin D: a review. Photodermatology, Photoimmunology & Photomedicine. 2014 Apr-Jun;30(2-3):137-145. doi:10.1111/phpp.12111. https://pubmed.ncbi.nlm.nih.gov/24313629/ ↩︎ ↩︎