¶ Vitiligo
Vitiligo is a chronic autoimmune pigmentary disorder characterized by the progressive destruction of epidermal melanocytes, resulting in well-demarcated depigmented macules and patches [1][2]. This clinical guide outlines the pathophysiology, diagnostic pathways, standard and novel treatment protocols, and monitoring parameters for professional reference and clinical education.
| Indication | Autoimmune Pigmentary Disorder |
| Access | Rx (Topical Ruxolitinib) / Clinical (Phototherapy, Surgery) |
| Dosing Sched | Daily (Topicals) / 2-3x Weekly (Phototherapy) |
| Safety Profile | Moderate (Low for topicals/NB-UVB, High for systemic JAKs) |
| Key Marker | VASI/VES, Thyroid Function (TSH, TPO Ab), Skin Atrophy |
| Est. Cost | Varies widely (High for novel JAKs, Low for TCS) |
¶ Safety "Traffic Light" & Boxed Warnings
- Red Light (High Risk): Systemic or oral Janus Kinase (JAK) inhibitors (such as baricitinib, upadacitinib, or abrocitinib) and the topical JAK inhibitor ruxolitinib are associated with potential risks of serious infections, thromboembolic events, and cardiovascular events [3][4][5]. Because ruxolitinib carries a class-level black box warning for these serious adverse effects, its use is carefully restricted [3:1]. Systemic JAK inhibitors necessitate rigorous patient selection and close clinical monitoring for hematologic abnormalities, infections, and cardiovascular safety [4:1][5:1]. Topical corticosteroids (TCS) require strict time limitations due to the risk of local skin atrophy [6].
- Yellow Light (Caution / Monitored): Topical ruxolitinib 1.5% cream is associated with localized adverse events including application-site acne, application-site pruritus, and nasopharyngitis [7]. While ruxolitinib carries a class-level boxed warning for serious risks such as infections and malignancies [3:2], topical treatment is generally well tolerated with minimal systemic absorption [4:2].
- Green Light (Safe / Standard Care): Topical calcineurin inhibitors (TCIs) (such as tacrolimus 0.1% ointment) are identified as evidence-based first-line therapies, particularly suitable for sensitive sites such as the face and neck, and are utilized without the strict time limitations associated with corticosteroids' atrophy risk [6:1][8]. Narrowband UVB (NB-UVB) phototherapy is highly effective and lacks systemic toxicity, making it the preferred long-term option for generalized disease [9][10].
¶ Protocol Card
- Topical Calcineurin Inhibitors (TCI): Tacrolimus 0.1% ointment or pimecrolimus 1% cream applied twice daily to affected areas (especially face/neck) [11][6:2].
- Topical JAK Inhibitor (Ruxolitinib 1.5% cream): Applied twice daily to affected areas up to 10% BSA for patients years [7:1].
- Phototherapy (NB-UVB): Highly effective treatment for generalized vitiligo, administered frequently (e.g., twice weekly in clinical trials) to stimulate melanocyte migration and achieve repigmentation [9:1][10:1].
- Systemic JAK Inhibitor (Oral Ritlecitinib - Investigational/Emerging): Under clinical evaluation for active, rapidly progressive non-segmental disease under clinical supervision [4:3].
- Maintenance: Proactive twice-weekly application of Tacrolimus 0.1% ointment to successfully repigmented areas to prevent relapse [12].
¶ Bottom Line
Medical treatments (topical calcineurin inhibitors, topical JAK inhibitors, and narrowband UVB phototherapy) are highly effective at halting disease activity and inducing perifollicular repigmentation. However, long-term maintenance is required to prevent relapse, and stable refractory lesions may necessitate surgical transplantation.
¶ Quick Answer
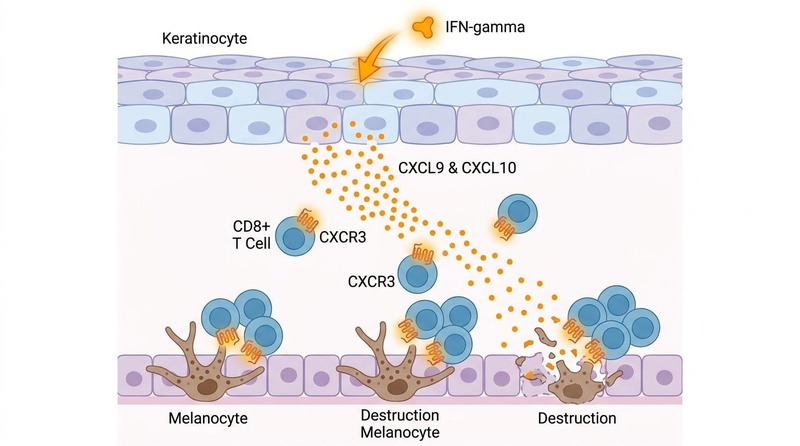
Vitiligo results from a localized autoimmune destruction of epidermal melanocytes, driven by an auto-amplifying interferon-gamma (IFN-γ) chemokine loop (CXCL9/10 recruitment of CXCR3+ cytotoxic CD8+ T cells) [13]. Clinically, it presents as chalk-white macules and patches [1:1][14][15]. Diagnostic confirmation involves Wood's lamp examination and clinical evaluation to distinguish it from mimics [16][17][18]. Treatment relies on progressive disclosure: halting disease progression using anti-inflammatory or systemic therapies, followed by promoting repigmentation via phototherapy (NB-UVB) and targeted topical therapies (TCI, JAK inhibitors) [19][20][21].
¶ The "Why": Benefits of Intervention
The primary clinical goals of vitiligo interventions are centered on changing the natural progression of the disease and restoring the skin's functional pigment barrier [19:1][22]:
- Arresting Disease Progression: Active vitiligo is characterized by the rapid expansion of existing lesions and the emergence of new macules. Early intervention with systemic or targeted therapies arrests this progressive destruction, preserving functional melanocyte populations [19:2][13:1].
- Inducing Repigmentation: Successful treatment stimulates the proliferation and migration of silent melanocyte stem cells, primarily located within the hair follicle outer root sheath, and from adjacent normally pigmented skin borders [11:1][23][8:1].
- Achieving Long-Term Stability: Maintaining restored pigment and preventing relapse in successfully repigmented lesions represents the ultimate long-term benefit, preventing the cycle of recurrent depigmentation [19:3][10:2].
- Mitigating Psychosocial Burden: Vitiligo is associated with significant psychological distress, anxiety, and diminished quality of life due to its highly visible nature [1:2][2:1][14:1]. Restoring pigment or stabilizing active lesions directly improves patient-reported quality of life and physiological resilience [22:1][14:2].
¶ Reality Check & Clinical Context
- Human Reality: While in vitro and rodent models (e.g., hair follicle-derived melanocyte transplants) demonstrate successful pigment restoration and survival [24], clinical transplantation in humans relies heavily on establishing absolute disease stability (at least 12 months of inactivity) to prevent graft failure and post-surgical Koebnerization [25][2:2].
- Bioavailability & Micronutrients: A systematic review and meta-analysis of 41 studies showed a significant decline in serum zinc and copper levels in vitiligo patients compared to healthy controls, but an increase in serum selenium [26]. While zinc and copper are important for tyrosinase activity (the rate-limiting step in melanogenesis), oral supplementation remains adjuvant, and direct clinical trials are sparse.
- Commercial Context: Opzelura (ruxolitinib 1.5% cream) is currently the only FDA-approved topical therapy for non-segmental vitiligo, but carries high commercial costs. Litfulo (ritlecitinib), an oral JAK3/TEC family kinase inhibitor, is currently approved for severe alopecia areata and is in late-stage Phase III clinical development for vitiligo, representing the vanguard of emerging systemic therapies.
¶ Clinical Classification, Subtypes & Staging
Accurate classification and staging are critical because prognosis, genetic susceptibility, and treatment responsiveness differ significantly between subtypes [19:4][14:3].
¶ 1. Non-Segmental Vitiligo (NSV)
Non-segmental vitiligo is the most common clinical form, representing the vast majority of cases [27][19:5]. It typically exhibits a bilateral, symmetrical distribution and a progressive, unpredictable course. Symmetrical lesions commonly appear on the face, dorsal hands, feet, and bony prominences. Over time, active disease can progress to involve large areas of the body surface.
- Generalized: Symmetrical depigmentation on multiple body areas [14:4].
- Acrofacial: Symmetrical involvement limited to the face (especially periorificial areas) and distal extremities [14:5].
- Mucosal: Limited to oral or genital mucosa [14:6].
- Universal: Symmetrical, near-complete depigmentation of the body, where depigmentation therapy of remaining pigmented skin can be considered (typically when involvement exceeds 50% to 80% of the body surface area) [28][8:2].
¶ 2. Segmental Vitiligo (SV)
Segmental vitiligo is a distinct clinical subtype characterized by a unilateral distribution [14:7].
- Clinical Course: It typically presents with localized lesions that stabilize early, after which further progression is rare [14:8]. Symmetrically localized patterns are absent.
- Follicular Involvement (Leukotrichia): It frequently involves hair follicles, which can result in early localized leukotrichia (hair depigmentation). Visually, this indicates a complete loss of the follicular melanocyte stem cell reservoir, making the lesion highly resistant to standard medical treatments (which rely on follicular repigmentation) [15:1].
- Therapeutic Response: Once clinical stability is established, these localized or stable recalcitrant lesions with leukotrichia are prime candidates for surgical grafting [19:6][25:1][2:3].
¶ 3. Staging & Disease Activity Tools
To guide treatment selection (e.g., medical stabilization vs. surgical grafting), clinicians use standardized scoring systems to track disease activity, severity, and extent [19:7][23:1]:
- VIDA (Vitiligo Disease Activity) Score: A clinical tool used to assess disease activity and progression to guide treatment decisions [18:1][23:2].
- Disease Activity Markers: Standardized clinical assessments, including the detection of the Koebner phenomenon, confetti-like depigmentation, and specific borders under Wood's lamp or dermoscopy, provide essential visible clues of active disease [13:2].
- VASI (Vitiligo Area Scoring Index) & VES (Vitiligo Extent Score): Standardized tools used to calculate the percentage of total body surface area (BSA) involvement and monitor treatment efficacy over time [19:8][23:3].
¶ 4. Mimics & Differential Diagnosis
Many hypopigmented or depigmented dermatoses mimic vitiligo. Accurate distinction is vital to prevent inappropriate treatment:
- Tinea Versicolor (Pityriasis Versicolor): A superficial fungal infection caused by Malassezia species. Clinically, it presents as mild, fine-scaly macules (unlike the completely smooth, non-scaly plaques of vitiligo) primarily on the trunk. Under a Wood's lamp, it exhibits a distinct yellow-gold fluorescence (rather than the bright blue-white fluorescence of vitiligo). Diagnosis is confirmed with a potassium hydroxide (KOH) preparation showing a classic "spaghetti and meatballs" pattern of fungal hyphae and yeast cells.
- Pityriasis Alba: A mild, low-grade eczematous dermatosis common in children with atopic dermatitis. It presents as poorly demarcated, slightly scaly, hypopigmented patches with indistinct borders (whereas vitiligo has sharp, chalk-white, depigmented borders). It is typically self-limiting and responds to mild moisturizers or low-potency topical steroids.
- Post-Inflammatory Hypopigmentation (PIH): A loss of pigment secondary to a preceding inflammatory cutaneous process (e.g., eczema, psoriasis, trauma). The borders are less distinct, and a history of preceding erythema or scaling is present. Unlike vitiligo, melanocytes are typically preserved but exhibit transient pigment depletion.
- Lichen Sclerosus: An inflammatory disease presenting with ivory-white, sclerotic, atrophic plaques, most commonly in the anogenital region. It is characterized by severe tissue atrophy, pruritus, and architectural distortion, which are absent in vitiligo.
- Macular Amyloidosis: Presents as small, hyperpigmented or hypopigmented macules with a characteristic "rippled" pattern, usually on the upper back, caused by amyloid deposition in the papillary dermis.
¶ 5. Confirmatory Evaluation
┌──────────────────────────────┐
│ Depigmented Skin Lesion │
└──────────────┬───────────────┘
│
[Wood's Lamp Examination]
│
┌───────────────────────┴────────────────────────┐
▼ ▼
[Bright Blue-White] [Yellow-Gold / No Fluor]
Vitiligo Suspected Alternative Mimic
│ │
├─────────────────┐ ├─────────────────┐
▼ ▼ ▼ ▼
[Dermoscopy] [Skin Biopsy (IHC)] [KOH Prep] [Clinical Eval]
Active / Stable Melan-A, SOX10, HMB-45 Spaghetti & Pityriasis Alba,
Features Markers Absent Meatballs (TV) Lichen Sclerosus
- Wood's Lamp Examination: Wood's lamp examination is a standard diagnostic tool used to confirm vitiligo by accentuating depigmented areas under ultraviolet light [17:1]. Under 365-nm narrowband black light, vitiligo lesions emit a bright, chalky blue-white fluorescence due to the loss of epidermal melanin, which normally absorbs ultraviolet radiation [17:2]. It helps clinicians identify subclinical lesions, assess disease margins, monitor repigmentation, and differentiate vitiligo from other hypopigmentation mimics [16:1][18:2].
- Skin Biopsy & Immunohistochemistry (IHC): A punch biopsy of an established vitiligo lesion can confirm the diagnosis by showing a complete absence of epidermal melanocytes and epidermal melanin in the basal layer. To confirm the diagnosis and rule out mimics, specific immunohistochemistry markers are utilized:
- Melan-A (MART-1): An epidermal marker that is completely absent in vitiligo lesions due to melanocyte destruction.
- SOX10: A highly sensitive nuclear marker for cells of melanocytic lineage, showing zero epidermal staining in lesional skin.
- HMB-45: Highlights active GP100-expressing melanocytes, which are absent within the lesion.
- Active Margins: Biopsies of active, expanding margins characteristically demonstrate a dense dermal-epidermal junction infiltrate of CD8+ cytotoxic T lymphocytes targeting surviving melanocytes [13:3].
- Dermoscopy: Dermoscopy is an invaluable, non-invasive bedside tool used to identify disease stages [29]:
- Active Disease: Characterized by the micro-Koebner phenomenon (linear depigmentation along minor trauma or scratch lines), a peripheral trichrome pattern, and the comet tail phenomenon [29:1].
- Stable Disease: Characterized by sharp, well-defined borders and peripheral hyperpigmentation, with absence of active markers [29:2].

¶ 6. Pediatric Vitiligo
Childhood vitiligo (defined as onset before 12 years of age) presents unique epidemiological and therapeutic considerations compared to adult-onset vitiligo [30]:
- Clinical Presentation: Children frequently present with segmental vitiligo or localized patterns, and the psychosocial impact on both children and parents is particularly profound [30:1].
- Safe First-Line Interventions: Standard pediatric guidelines prioritize topical calcineurin inhibitors (TCIs) twice daily and topical corticosteroids (TCS) with strict time limits to avoid local skin atrophy [6:3].
- Age and Safety Restrictions for JAK Inhibitors: Topical ruxolitinib 1.5% cream is FDA-approved only for patients 12 years of age and older [7:2]. Its use in patients younger than 12 years is considered off-label and requires careful consideration of the limited pediatric safety data [6:4].
- Phototherapy: Narrowband UVB (NB-UVB) phototherapy is a commonly used and highly effective treatment modality for childhood vitiligo [11:2][30:2].
¶ 7. Skin-of-Color Nuances
In patients with darker skin phenotypes (Fitzpatrick phototypes IV–VI), vitiligo presents distinct clinical, aesthetic, and psychological challenges [1:3]:
- Visual Disparity and Psychosocial Burden: The sharp, high-contrast boundary between chalk-white vitiligo patches and deeply pigmented normal skin creates an extremely visible appearance [1:4]. This stark visual difference significantly amplifies the psychosocial burden and social stigma associated with the disease [14:9].
- Risk of Paradoxical Dyspigmentation: Darker skin is highly susceptible to post-inflammatory pigmentary alterations. Clinicians must exercise extreme caution during phototherapy titration and when prescribing irritating topical therapies (e.g., highly potent corticosteroids or topical retinoids), as localized irritation can trigger paradoxical hyperpigmentation (dark halos) at the active margins, or rebound hypopigmentation, compounding cosmetic distress.
- Aesthetic Preservation and Early Camouflage: Combining active medical therapies with early cosmetic camouflage counseling is highly recommended [11:3][28:1]. Specialized camouflage cosmetics help manage the visual contrast during the many months required for slow repigmentation treatments to take effect [11:4][28:2].
¶ 8. Safe Self-Care, Photoprotection & Camouflage
Patient education regarding daily self-care and environmental exposure is essential to optimize therapeutic outcomes and prevent disease flares [19:9]:
- Daily Broad-Spectrum Photoprotection: Depigmented vitiligo skin is devoid of protective epidermal melanin, rendering it highly vulnerable to acute actinic damage and sunburn [28:3]. Patients must use a high-SPF, broad-spectrum sunscreen daily. This not only protects the depigmented patches from burning but also prevents tanning of the surrounding unaffected skin, which would otherwise exaggerate the visual contrast of the lesions [28:4].
- Mitigating the Koebner Phenomenon: Patients must be educated to avoid mechanical trauma, chronic friction, vigorous scratching, and tight clothing [13:4]. Mechanical micro-injury to the skin can trigger localized autoimmune destruction of melanocytes, leading to new depigmented patches at the site of trauma (Koebnerization) [13:5].
- Safe Cosmetic Camouflage: The use of specialized cosmetic camouflage, cover-up makeup, or self-tanning preparations containing dihydroxyacetone (DHA) is a safe and highly effective method to temporarily disguise white areas [28:5].
- Diagnostic Pearl: Clinicians must note that DHA-infused camouflage makeup produces a distinct salmon-colored fluorescence under Wood's lamp examination [31]. This pattern can mimic the coral-red fluorescence of erythrasma (a superficial bacterial infection caused by Corynebacterium minutissimum), requiring careful history-taking and diagnostic vigilance to prevent misdiagnosis [31:1].
¶ 9. Psychosocial Burden & Quality of Life
Vitiligo frequently inflicts a profound psychosocial toll on patients, manifesting as elevated rates of anxiety, psychological distress, and social stigmatization [1:5][2:4][14:10]:
- Quality of Life Impairment: The visible nature of depigmentation, particularly on exposed anatomical sites such as the face, hands, and genitalia, directly impairs quality of life [14:11]. The psychological distress and overall quality of life impact are significantly shaped by ethnic, cultural, and sociocultural factors [1:6][14:12].
- Psychological Support: Expert guidelines emphasize that psychological support is indicated and should be offered alongside active medical or surgical interventions to address the holistic needs of the patient [22:2][23:4].
¶ Pathophysiology & Cellular Mechanisms
The pathogenesis of vitiligo involves a multi-step, auto-amplifying pathway of oxidative stress and adaptive autoimmune destruction.
¶ 1. Intracellular Oxidative Stress
Melanocytes in vitiligo patients exhibit inherent morphological and functional susceptibilities [1:7]. Under genetic influence, these cells suffer from excessive intracellular oxidative stress [32][15:2]. The accumulation of Reactive Oxygen Species (ROS) drives cellular stress and progressive melanocyte destruction, which triggers downstream inflammatory pathways and the activation of dysregulated immune responses targeting the remaining melanocytic populations [32:1][15:3].
¶ 2. The IFN-γ-Induced Chemokine CXCL9/10 Loop
The released inflammatory signals recruit and activate epidermal resident dendritic cells, which process and present melanocyte-specific antigens to autoreactive CD8+ cytotoxic T lymphocytes (CTLs) [13:6].
- Cytotoxic Infiltration: These CTLs home to active vitiligo borders and secrete Interferon-gamma (IFN-γ) [13:7].
- Keratinocyte Amplification: IFN-γ binds to receptors on neighboring epidermal keratinocytes, activating the Janus Kinase 1/Janus Kinase 2 (JAK1/JAK2) pathway [21:1][13:8].
- Chemokine Secretion: This pathway drives the transcription and secretion of chemokines CXCL9 and CXCL10 [13:9].
- Positive Feedback Loop: CXCL9 and CXCL10 bind to the CXCR3 receptor on autoreactive CD8+ CTLs, recruiting more cytotoxic T cells to the border. These T cells destroy melanocytes via cytolytic mechanisms, completing an auto-amplifying cycle of depigmentation [21:2][13:10].
¶ Evidence & Science
¶ Evidence Summary Table (Human Outcomes)
The following table summarizes the clinical efficacy, consistency, and certainty of evidence for vitiligo interventions based on human clinical data.
| Outcome / Goal | Effect* | Consistency** | Evidence Quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Facial Repigmentation (F-VASI75) | High | High | Phase III RCTs | Topical Ruxolitinib 1.5% cream twice daily. Significantly increases the odds of achieving F-VASI75 (OR 4.34) and F-VASI50 (OR 4.71) at 24 weeks compared to vehicle [20:1]. | |
| Corporal Repigmentation (T-VASI50) | High | High | Phase III RCTs | Topical Ruxolitinib 1.5% cream twice daily. Significantly increases the odds of achieving T-VASI50 (OR 4.47) and T-VASI75 (OR 2.78) at 24 weeks compared to vehicle [20:2]. | |
| Disease Stabilization (Active NSV) | High | Moderate | Multiple RCTs | Systemic Corticosteroids. Oral or systemic corticosteroids are used to arrest rapidly progressive, active non-segmental disease [19:10][23:5]. | |
| Follicular Repigmentation (Generalized) | High | High | Meta-analyses | Narrowband UVB (NB-UVB) phototherapy 2–3 times weekly for 6–12 months. Gold standard for generalized disease ( BSA) [11:5][9:2]. | |
| Synergistic Repigmentation Speed | High | High | Systematic Reviews | Combination of Oral JAK Inhibitors + NB-UVB. Phototherapy accelerates and deepens oral JAK-inhibitor induced pigment [21:3]. | |
| Stable Lesion Clearance (SV & NSV) | Moderate | Moderate | Cohort Studies | Autologous Surgical Grafting. Shown to achieve significant repigmentation in stable cases depending on the grafting technique [33][2:5]. | |
| Enhanced Graft Pigment Spread | Low | Low | Systematic Reviews | Surgical Grafting + Postoperative Phototherapy. There is limited evidence that phototherapy improves outcomes after melanocyte transplantation, and insufficient evidence to recommend specific phototherapy types [34]. | |
| Adjuvant Anti-Inflammatory Repigmentation | Moderate | Moderate | RCTs & Meta-analyses | Topical Calcineurin Inhibitors (TCI) (Tacrolimus 0.1%) twice daily on facial/neck lesions. Achieves high repigmentation comparable to TCS without atrophy [11:6]. | |
| Adjuvant Vitamin D Repigmentation | Moderate | Low | Meta-analyses | Topical Calcipotriol or Tacalcitol combined with NB-UVB. Calcipotriol or tacalcitol slightly enhances treatment efficacy when combined with NB-UVB [35][36]. | |
| Adjuvant Microneedling / Ablative Laser | Moderate | Moderate | Systematic Reviews | Microneedling or Ablative Laser combined with NB-UVB phototherapy. May improve repigmentation outcomes [37]. | |
| Adjuvant Lipid Lowering & Anti-Inflam | Moderate | Moderate | 6-RCT Meta-analysis | Oral Simvastatin (adjuvant). Enhances VASI improvements and excellent repigmentation (OR 6.54) due to systemic immunomodulatory effects [38]. | |
| Complementary Immunomodulation | Moderate | Low | 39-RCT Meta-analysis | Compound Glycyrrhizin + conventional therapy. Significantly increases repigmentation rate (RR 1.28) over phototherapy/TCS alone [39]. |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome.
¶ In-Depth Clinical Treatment Protocols
¶ 1. First-Line Topical Therapies
For localized vitiligo (affecting BSA), topical anti-inflammatory treatments are the standard first-line therapies [27:1][19:11]:
¶ Topical Corticosteroids (TCS)
- Anatomical Tailoring:
- Body and Extremities: Use potent or highly potent topical corticosteroids (e.g., clobetasol propionate 0.05% or mometasone furoate 0.1%) on suitable areas under careful medical supervision [19:12][28:6].
- Face, Neck, and Intertriginous Areas: Use topical calcineurin inhibitors or mild-to-moderate potency topical corticosteroids, especially on the face and neck [11:7][8:3].
- Regimen: Topical potent or highly potent corticosteroids are typically applied once daily [11:8].
- Long-Term Monitoring: Patients using topical corticosteroids must be monitored for the risk of skin atrophy, which prompts strict time limitations on their use [6:5].
¶ Topical Calcineurin Inhibitors (TCI)
- Agents: Tacrolimus 0.1% ointment or Pimecrolimus 1% cream [11:9].
- Regimen: Apply a thin layer twice daily to affected patches [6:6].
- Efficacy & Safety: TCIs are identified as evidence-based first-line therapies, particularly suitable for sensitive sites such as the face and neck [6:7][8:4], and are utilized without the strict time limitations associated with corticosteroids' atrophy risk [6:8].
¶ 2. Approved & Investigational JAK Inhibitors
Janus Kinase inhibitors target the intracellular signaling pathway of IFN-γ, shutting down keratinocyte chemokine production [20:3][21:4][4:4].
- Approved Topical Agent (Ruxolitinib 1.5% cream):
- Mechanism: Inhibits JAK1 and JAK2, targeting the downstream JAK/STAT pathway and reducing local chemokine expression [4:5].
- Indication: FDA-approved for non-segmental vitiligo in patients years of age. Currently, topical ruxolitinib 1.5% cream is the only FDA-approved therapy specifically for vitiligo as of the cited literature [3:3].
- Dosing: Apply a thin layer twice daily to affected lesions, up to a maximum of 10% BSA [7:3].
- Clinical Efficacy: Phase III trials demonstrate that topical ruxolitinib significantly increases the likelihood of achieving F-VASI75 (OR 4.34, 95% CI 2.67–7.06) and F-VASI50 (OR 4.71, 95% CI 3.24–6.84) compared to vehicle [20:4]. There is also a significant likelihood of achieving T-VASI75 (OR 2.78, 95% CI 1.10–7.00) and T-VASI50 (OR 4.47, 95% CI 2.52–7.92) at 24 weeks [20:5].
- Systemic Oral JAK & TEC Kinase Inhibitors:
- Oral Ritlecitinib (Approved for severe alopecia areata; Phase III for vitiligo):
- Mechanism: A selective dual inhibitor of Janus kinase 3 (JAK3) and the tyrosine kinase expressed in hepatocellular carcinoma (TEC) family of kinases [4:6]. By selectively blocking these kinases, it prevents the cytolytic activity and IFN-γ production of cytotoxic T cells and NK cells.
- Therapeutic Protocol: Under clinical evaluation for active, rapidly progressive non-segmental vitiligo, demonstrating high rates of disease stabilization and perifollicular repigmentation, especially when paired with NB-UVB phototherapy [4:7].
- Off-Label Systemic Agents (Baricitinib, Tofacitinib, and Abrocitinib):
- Mechanism: Oral Janus kinase (JAK) inhibitors that target JAK1, JAK2, and/or JAK3, blocking downstream IFN-γ-induced chemokine transcription (CXCL9/CXCL10) and preventing cytolytic T-cell recruitment [4:8][5:2].
- Clinical Status & Efficacy: Systemic or oral JAK inhibitors (such as baricitinib, tofacitinib, or abrocitinib) are utilized off-label [4:9][5:3]. When combined with NB-UVB phototherapy, they significantly improve repigmentation, leading to a greater reduction in total VASI scores and higher likelihood of achieving (RR = 6.87) and (RR = 15.13) repigmentation compared to phototherapy alone [21:5].
- Therapeutic Target: Indicated for adults with active, rapidly progressive, or treatment-refractory non-segmental vitiligo [21:6][10:3].
- Oversight: Because of their systemic immunomodulatory effects, oral JAK inhibitors require careful patient selection and systematic laboratory monitoring [4:10][5:4].
- Oral Ritlecitinib (Approved for severe alopecia areata; Phase III for vitiligo):
¶ 3. Phototherapy Protocols
For active, progressive disease or generalized vitiligo (affecting BSA), phototherapy is the global gold standard of care [11:10][9:3]:
- Narrowband UVB (NB-UVB):
- Efficacy: Highly effective as monotherapy or in combination with other treatments [19:13]. It serves as a standard option for generalized non-segmental disease [9:4].
- Regimen: Administered as a regular clinical regimen (such as twice weekly) [10:4] and requires frequent clinic visits or a structured home-based protocol [9:5].
- Clinic vs. Home Oversight:
- In-Office Phototherapy (IOUVB): Delivered under clinical supervision, ensuring structured dosing and safety monitoring.
- Home-Based Phototherapy (HBUVB): Systematic meta-analyses indicate HBUVB is not inferior to IOUVB in achieving and repigmentation, and exhibits a 14% lower rate of discontinuation [9:6]. However, HBUVB is associated with potential risks of adverse effects such as erythema, burning, or acute pruritus, necessitating careful patient education and clinical oversight [40][9:7].
- PUVA (Psoralen + UVA):
- Consists of oral or topical methoxsalen (psoralen) ingestion followed by exposure to long-wave UVA radiation.
- Clinical Status: Historically, guidelines like Gawkrodger 2008 [11:11] evaluated PUVA as a therapeutic option, but modern practice has increasingly shifted toward narrowband UVB (NB-UVB) due to its safety profile and ease of administration [11:12]. However, a comprehensive meta-analysis of vitiligo-specific cohorts [41] demonstrated that UV phototherapy overall (including both NB-UVB and PUVA subgroups) does not significantly increase the risk of melanoma or non-melanoma skin cancer in vitiligo patients [41:1].
¶ 4. Surgical Intervention for Stable Disease
Surgical autologous transplantation is reserved for patients with localized or segmental vitiligo that has failed first-line medical therapies [33:1][2:6]:
- Prerequisites for Surgical Candidates:
- Rigorous Stability Criteria: Surgery is indicated only for stable vitiligo that does not respond to medical treatment [25:2]. Patient selection relies heavily on establishing absolute disease stability, defined as a period of at least 12 months of no new lesions, no expansion of existing lesions, and a negative Koebner phenomenon [25:3][2:7]. This stability window is critical to prevent graft destruction and avoid triggering the Koebner phenomenon [25:4].
- Test Grafting: In doubtful cases where stability is uncertain, a test graft may be performed to detect stability and assess the likelihood of success before committing to extensive surgical procedures [25:5].
- Surgical Techniques:
- Miniature Punch Grafting: Full-thickness skin grafts are harvested from a pigmented donor site and transplanted into recipient beds spaced closely apart [33:2][25:6].
- Suction Blister Epidermal Grafting (SBEG): Blisters are induced at the donor site using negative pressure. The pure epidermal roofs are harvested and grafted onto dermabraded recipient patches [33:3][25:7].
- Non-Cultured Epidermal Cell Suspension (NCES): A small, thin split-thickness skin graft is enzymatically digested to isolate basal keratinocytes and melanocytes. The resulting cell suspension is applied directly onto a dermabraded recipient site [33:4]. NCES represents a major surgical development that offers several therapeutic advantages for repigmenting stable lesions [8:5].
¶ Comprehensive Safety, Toxicology & Adverse Events
¶ 1. Topical Therapy Side Effects
- Topical Corticosteroids (TCS): High-potency TCS can cause localized epidermal thinning, telangiectasia, striae distensae, and rosacea-like dermatoses. Systemic absorption leading to HPA axis suppression is a rare risk when applied to large areas for prolonged periods.
- Topical Calcineurin Inhibitors (TCI): Local dermatological side effects of topical immunomodulators (such as tacrolimus or pimecrolimus) are generally mild and do not necessitate treatment cessation [42].
- Topical JAK Inhibitors: Application site reactions include mild pruritus, transient erythema, and localized acneiform eruptions [20:6].
¶ 2. JAK Inhibitor Safety & Monitoring
Patients initiating Janus Kinase (JAK) inhibitors must be evaluated with care. While topical ruxolitinib carries a class-level black box warning for serious adverse effects such as infections, malignancy, and major adverse cardiovascular events [3:4], it minimizes systemic exposure and is generally well tolerated with minimal systemic absorption [4:11][5:5].
- Oral JAK Inhibitor Monitoring (Off-Label): Oral JAK inhibitors exhibit variable safety profiles and require systematic clinical monitoring owing to potential risks of infection, hematologic abnormalities, thromboembolic events, and cardiovascular events [4:12][5:6]. This necessitates careful patient selection and ongoing safety tracking [5:7].
¶ 4. Urgent Red Flags & Safety Boundaries
Patients undergoing advanced dermatological therapies (TCS, TCI, JAK inhibitors, or phototherapy) must be monitored for serious adverse events. If any of the following urgent red flags occur, immediately withhold all active therapies and refer for urgent medical evaluation:
- Eczema Herpeticum: Rapidly spreading, painful, punched-out monomorphic vesicles with umbilication, often accompanied by high fevers and lymphadenopathy. This can occur as a complication of local immunosuppression (TCS/TCI) on active eczematous or barrier-compromised skin.
- Pustular or Erythrodermic Psoriasis: The sudden development of widespread, sterile pustules on a background of painful, fiery-red, inflamed skin (erythroderma), which can be triggered by the rapid withdrawal of systemic or high-potency topical corticosteroids.
- Severe Hidradenitis and Spreading Cellulitis: Deep, painful, draining inflammatory nodules in intertriginous areas (axillae, groin) that develop severe, spreading cellulitis, high fevers, or signs of systemic sepsis.
- Ophthalmic or Disseminated Herpes Zoster: A painful vesicular eruption following a cranial dermatome (specifically involving the ophthalmic branch of the trigeminal nerve, risking corneal blindness) or a widespread, multi-dermatomal (disseminated) zoster rash, which are critical risks during systemic or high-dose local immunosuppressive therapy.
- Atypical or Non-Resolving Skin Infection: A localized skin lesion showing signs of atypical bacterial, fungal, or mycobacterial infection (such as progressive ulceration, nodular tracking, or failure to respond to standard first-line antibiotics) in a patient utilizing chronic immunomodulators.
¶ Response, Maintenance & Relapse Timelines
¶ 1. Repigmentation Patterns
Repigmentation occurs via two primary biological patterns:
- Perifollicular Repigmentation: The most common pattern [16:2]. It appears as small, pinpoint pigmented macules (islands) centered around hair follicles within the depigmented patch [16:3]. This signifies the activation and migration of silent melanocyte stem cells from the follicular outer root sheath.
- Marginal Repigmentation: Pigment spreads inward from the outer borders of the vitiligo patch.
¶ 2. Clinical Timelines
- Initial Response: Visible repigmentation is a gradual process; clinical guidelines indicate that a minimum therapeutic trial of 6 months or more is typically required to evaluate treatment response [25:8][6:9].
- Maximum Response: Achieving maximal repigmentation is a long-term process, with clinical trials of advanced therapies showing continued pigmentary improvement through 104 weeks (2 years) of continuous treatment [43]. Standard clinical assessments recommend evaluating treatment response at a 3 to 6 month timeline to determine early progress [11:13].
¶ 3. Relapse & Long-Term Maintenance
Stabilizing the skin after successful repigmentation is a major clinical hurdle.
- High Relapse Rate: Relapse (depigmentation of successfully repigmented lesions) is highly common after stopping active therapy, driven by localized immunological memory [22:3].
- Proactive Maintenance Regimen: To mitigate the risk of disease relapse, maintenance therapy with topical agents can be used [19:14]. This often involves a proactive, twice-weekly maintenance protocol:
- TCI Maintenance: Apply tacrolimus 0.1% ointment twice weekly to successfully repigmented patches [12:1].
- TCS Maintenance: Alternatively, apply a moderate-to-high potency topical corticosteroid twice weekly [11:14].
- This proactive approach has been shown to significantly reduce relapse and maintain repigmentation compared to observational follow-up alone [11:15][12:2].
¶ Tracking & Assessment Plan
- Visual Documentation: Standardized clinical photography at baseline, during follow-up, and annually, using identical lighting and positioning to document progress.
- Wood's Lamp Evaluation: Periodic Wood's lamp examinations to detect subclinical lesions, define boundaries, and monitor early perifollicular repigmentation islands [11:16].
- Quantitative Scoring: Assess disease extent using clinical scoring systems (such as the Facial Vitiligo Area Scoring Index [F-VASI], Total Vitiligo Area Scoring Index [T-VASI], or Vitiligo Extent Score [VES]) during baseline and follow-up clinical evaluations to objectively monitor body surface area involvement and response to therapy [19:15][20:7][23:6].
- Thyroid Function Monitoring: Baseline screening for thyroid function (TSH and thyroid autoantibodies) is recommended in patients with non-segmental vitiligo due to the high association with autoimmune thyroiditis, supported by systematic reviews of prevalence [44] and guidelines emphasizing the clinical significance of associated autoimmune disorders [11:17][1:8]. Repeat screening is guided by clinical symptoms or rapid progression.
¶ What Usually Fails
- Postoperative Phototherapy Overestimation: In surgical grafting, while postoperative phototherapy is frequently utilized to encourage pigment spread, evidence of its added benefit remains limited, and there is insufficient evidence to recommend a specific type or regimen of phototherapy [34:1].
- Surgical Grafting in Unstable Disease: Performing punch or blister grafting on a patient with active, unstable vitiligo is highly prone to failure. The active autoimmune environment will destroy the transplanted melanocytes, and the physical trauma of the surgery can trigger the Koebner phenomenon, causing severe depigmentation at both the donor and recipient sites [25:9].
- Premature Discontinuation of Medical Therapy: Discontinuing topical JAK inhibitors or TCIs at 8 to 12 weeks due to "lack of results" is a common error. Therapeutic trials must be maintained for at least 6 months before assessing efficacy [6:10].
- Inadequate Photoprotection: Neglecting daily broad-spectrum sunscreen allows UV-induced sunburns to trigger local inflammatory cascades, driving Koebnerization and expanding depigmentation [11:18][28:7].
¶ Comparisons & Engagement
¶ Compare With
To help contextualize vitiligo management, clinicians can compare its therapeutic strategies with related autoimmune or pigmentary conditions:
| Parameter | Vitiligo | Melasma | Alopecia Areata |
|---|---|---|---|
| Primary Pathology | Epidermal melanocyte destruction [1:9] | Melanocyte hyperactivity & dysregulation | Lymphocytic attack on hair follicle bulb |
| First-Line Medical | TCI (Tacrolimus) & Potent TCS [11:19] | Topical hydroquinone & retinoids | Intralesional TCS or topical minoxidil |
| JAK Inhibitor Role | Highly effective (Topical Ruxolitinib) [20:8] | No established clinical role | Established role (Oral Baricitinib, Ritlecitinib) |
| Phototherapy Efficacy | High (Narrowband UVB is gold standard) [9:8] | Contraindicated (UV triggers hyperpigmentation) | Low to Moderate efficacy |
| Surgical Options | High success in stable disease (NCES, SBEG) [33:5] | None (Surgical trauma triggers dyspigmentation) | Hair transplantation (only in long-term stable cases) |
¶ Internal Links
- Mitochondrial Dysfunction: Learn how systemic cellular stress relates to Mitochondrial Dysfunction and ROS generation.
- Post-Inflammatory Hyperpigmentation: Contrast depigmentation mechanisms with hyperpigmentation pathways in Post-Inflammatory Hyperpigmentation and Melasma.
- Frontier Regulatory Pathways: Understand the clinical trial framework and approval pathways in Regulatory Landscape for Longevity Interventions.
¶ Clinical FAQs
¶ What is the difference between segmental and non-segmental vitiligo?
Segmental vitiligo (SV) is unilateral, follows a localized pattern, has a rapid onset, and stabilizes early, but frequently causes early leukotrichia (depigmented hair) [14:13][15:4]. Non-segmental vitiligo (NSV) is bilateral, symmetrical, progressive, and can spread unpredictably throughout a lifetime [14:14][15:5][1:10].
¶ How long does it take to see results from vitiligo treatments?
Melanocyte regeneration is a highly gradual process. Clinical trials and expert consensus guidelines suggest that a minimum therapeutic trial of 6 months or more is required to evaluate the efficacy of topical or light therapies [25:10][6:11]. Achieving maximal repigmentation is a long-term process, with clinical trials of advanced therapies showing continued pigmentary improvement through 104 weeks (2 years) of continuous treatment [43:1].
¶ Is phototherapy safe for children with vitiligo?
Yes, Narrowband UVB (NB-UVB) phototherapy is safe and highly effective for children with generalized vitiligo [30:3]. It is a commonly used first-line light modality recommended in clinical guidelines [11:20][30:4].
¶ Why is daily sun protection so important in vitiligo?
Depigmented vitiligo skin completely lacks protective epidermal melanin, making it highly susceptible to sunburn. Sunburn can trigger an inflammatory cascade that induces Koebnerization, leading to the development of new vitiligo lesions. Daily broad-spectrum sunscreen is recommended to prevent this flare pathway [28:8].
¶ What is the relapse rate after successful repigmentation?
Relapse is highly common after stopping active therapy, driven by localized immunological memory. Transitioning to a proactive, twice-weekly maintenance regimen with topical calcineurin inhibitors (tacrolimus 0.1% ointment) or moderate-to-high potency topical corticosteroids significantly reduces the rate of recurrence and helps maintain long-term repigmentation compared to observational follow-up alone [11:21][12:3].
¶ References
Schild M, Meurer M. [Vitiligo: Clinical presentation and pathogenesis]. Der Hautarzt. 2016;67(2):104-111. https://pubmed.ncbi.nlm.nih.gov/26781864/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bhingradia YM, Gupta S, Ghia D. Consensus statement on the surgical management of vitiligo. Journal of Cutaneous and Aesthetic Surgery. 2025;18(1):15-28. https://pubmed.ncbi.nlm.nih.gov/40027541/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bitterman D, Kabakova M, Wang JY. The role of aryl hydrocarbon receptor agonists in the treatment of vitiligo. Archives of Dermatological Research. 2024;316(9):512-520. https://pubmed.ncbi.nlm.nih.gov/39369105/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ferreira C, King B, Torres T. JAK Inhibitors for the Treatment of Vitiligo: Current Evidence and Emerging Therapeutic Potential. Drugs. 2025;85(12):1345-1360. https://pubmed.ncbi.nlm.nih.gov/40996476/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pipitò C, Marino A, Prignano F. Label and off-label treatment of dermatological diseases with JAK and TYK inhibitors. Italian Journal of Dermatology and Venereology. 2026;161(1):50-62. https://pubmed.ncbi.nlm.nih.gov/41178404/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Renert-Yuval Y, Ezzedine K, Grimes P, et al. Expert Recommendations on Use of Topical Therapeutics for Vitiligo in Pediatric, Adolescent, and Young Adult Patients. JAMA Dermatology. 2024;160(4):420-432. https://pubmed.ncbi.nlm.nih.gov/38477910/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Rosmarin D, Passeron T, Pandya AG, et al. Two Phase 3, Randomized, Controlled Trials of Ruxolitinib Cream for Vitiligo. The New England Journal of Medicine. 2022;387(16):1445-1455. https://pubmed.ncbi.nlm.nih.gov/36260792/ ↩︎ ↩︎ ↩︎ ↩︎
Borderé AC, Lambert J, van Geel N. Current and emerging therapy for the management of vitiligo. Clinical, Cosmetic and Investigational Dermatology. 2009;2:15-25. https://pubmed.ncbi.nlm.nih.gov/21436965/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Xireaili F, Ha H, Liu ZF. The Effectiveness of Home-Based Phototherapy in Vitiligo: A Systematic Review and Meta-Analysis. Photodermatology, Photoimmunology & Photomedicine. 2026;42(2):e12345. https://pubmed.ncbi.nlm.nih.gov/41804555/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Xu Z, Xuan Y, Zhu Z. Long-term efficacy and safety of oral abrocitinib combined with narrow-band UVB phototherapy in non-segmental vitiligo: a 52-week prospective study. The Journal of Dermatological Treatment. 2025;36(12):112-119. https://pubmed.ncbi.nlm.nih.gov/41104771/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gawkrodger DJ, Ormerod AD, Shaw L, et al. Guideline for the diagnosis and management of vitiligo. The British Journal of Dermatology. 2008;159(5):1051-1076. https://pubmed.ncbi.nlm.nih.gov/19036036/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cavalié M, Ezzedine K, Vabres P, et al. Maintenance therapy of adult vitiligo with 0.1% tacrolimus ointment: a randomized, double blind, placebo-controlled study. The Journal of Investigative Dermatology. 2015;135(4):970-974. https://pubmed.ncbi.nlm.nih.gov/25521460/ ↩︎ ↩︎ ↩︎ ↩︎
Zhu Z, Zhu Y, Xuan Y. Clinical and molecular markers of vitiligo: a narrative review of early-stage insights into disease activity and treatment response. The British Journal of Dermatology. 2026;194(5):450-462. https://pubmed.ncbi.nlm.nih.gov/41703718/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Marzano AV, Alberti-Violetti S, Maronese CA. Vitiligo: Unmet Need, Management and Treatment Guidelines. Dermatology Practical & Conceptual. 2023;13(4):e2023280. https://pubmed.ncbi.nlm.nih.gov/38241398/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ismail IB, Bhat YJ, Ul Islam MS. Treatment Advances in Vitiligo: An Updated Review. Dermatology Practical & Conceptual. 2025;15(1):e2025012. https://pubmed.ncbi.nlm.nih.gov/40117616/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wang YJ, Chang CC, Cheng KL. Wood's lamp for vitiligo disease stability and early recognition of initiative pigmentation after epidermal grafting. International Wound Journal. 2017;14(6):1314-1318. https://pubmed.ncbi.nlm.nih.gov/28799192/ ↩︎ ↩︎ ↩︎ ↩︎
Bae JM, Lee RW. 365-nm narrowband Wood's lamp for vitiligo and hypopigmentation disorders. Journal of the American Academy of Dermatology. 2020;83(4):e283-e284. https://pubmed.ncbi.nlm.nih.gov/31476339/ ↩︎ ↩︎ ↩︎
Hou Y, Wei Z, Jiang Q. In-depth study of Wood's lamp examination combined with reflective confocal laser scanning microscopy for the guidance of vitiligo staging and treatment. Journal of Cosmetic Dermatology. 2024;23(4):1254-1262. https://pubmed.ncbi.nlm.nih.gov/38158739/ ↩︎ ↩︎ ↩︎
Prajapati VH, Lui H, Miller-Monthrope Y, et al. Canadian Consensus Guidelines for the Management of Vitiligo. Dermatology and Therapy. 2025;15(6):1201-1215. https://pubmed.ncbi.nlm.nih.gov/40253664/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yuan Y, Zhang Y, Zheng L. Short-term (24 weeks) treatment efficacy and safety of ruxolitinib cream in participants with vitiligo: a systematic review and meta-analysis. Systematic Reviews. 2024;13(1):250. https://pubmed.ncbi.nlm.nih.gov/39358803/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shuaib L, D Rai K, K Sangtiani A, et al. Efficacy of Janus kinase inhibitor combined with phototherapy in non-segmental vitiligo: systematic review and meta-analysis. Annals of Medicine. 2026;58(12):112-124. https://pubmed.ncbi.nlm.nih.gov/41454839/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Meurer M, Schild M. [Treatment of vitiligo]. Der Hautarzt. 2016;67(3):218-225. https://pubmed.ncbi.nlm.nih.gov/26909811/ ↩︎ ↩︎ ↩︎ ↩︎
Turco M, Coronella L, Picone V. The Patient Journey in Vitiligo. Dermatology (Basel). 2026;242(2):101-112. https://pubmed.ncbi.nlm.nih.gov/41308036/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fan R, Gao J, Chen J, et al. Hair follicle-derived melanocyte transplant as a promising treatment strategy for vitiligo. Stem Cell Research & Therapy. 2025;16(1):210. https://pubmed.ncbi.nlm.nih.gov/40462233/ ↩︎
Parsad D, Gupta S, IADVL Dermatosurgery Task Force. Standard guidelines of care for vitiligo surgery. Indian Journal of Dermatology, Venereology and Leprology. 2008;74(Suppl):S54-S64. https://pubmed.ncbi.nlm.nih.gov/18688102/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Anam K, Ananyan S, Rishabh M. Zinc, copper, and selenium levels in vitiligo: a systematic review and meta-analysis. Scientific Reports. 2024;14(1):23456. https://pubmed.ncbi.nlm.nih.gov/39390004/ ↩︎
Böhm M, Schunter JA, Fritz K, et al. S1 Guideline: Diagnosis and therapy of vitiligo. Journal der Deutschen Dermatologischen Gesellschaft. 2022;20(3):365-378. https://pubmed.ncbi.nlm.nih.gov/35246935/ ↩︎ ↩︎
Antoniou C, Katsambas A. Guidelines for the treatment of vitiligo. Drugs. 1992;43(4):490-498. https://pubmed.ncbi.nlm.nih.gov/1377115/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yu S, He J, Wang H, et al. Dermoscopic features in children with vitiligo and other hypopigmentation disorders. Frontiers in Pediatrics. 2025;13:e40708909. https://pubmed.ncbi.nlm.nih.gov/40708909/ ↩︎ ↩︎ ↩︎
Nicolaidou E, Mastraftsi S, Tzanetakou V. Childhood Vitiligo. American Journal of Clinical Dermatology. 2019;20(4):515-526. https://pubmed.ncbi.nlm.nih.gov/30911977/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nagshabandi KN, Shadid A, Alakresh L. Salmon colored fluorescence on Wood's lamp in a pediatric patient with vitiligo: A case report. Journal of Family Medicine and Primary Care. 2024;13(11):4123-4127. https://pubmed.ncbi.nlm.nih.gov/39723023/ ↩︎ ↩︎
Tanemura A, Oiso N, Okamura K, et al. Second Guidelines for the Diagnosis and Treatment of Vitiligo in Japan (2025). The Journal of Dermatology. 2026;53(5):31-45. https://pubmed.ncbi.nlm.nih.gov/42219812/ ↩︎ ↩︎
Ju HJ, Bae JM, Lee RW, et al. Surgical Interventions for Patients With Vitiligo: A Systematic Review and Meta-analysis. JAMA Dermatology. 2021;157(3):307-316. https://pubmed.ncbi.nlm.nih.gov/33595599/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lommerts JE, Uitentuis SE, Bekkenk MW. The role of phototherapy in the surgical treatment of vitiligo: a systematic review. Journal of the European Academy of Dermatology and Venereology. 2018;32(9):1425-1435. https://pubmed.ncbi.nlm.nih.gov/29573480/ ↩︎ ↩︎
Hu M, Liao K, Lei W. The addition of topical calcipotriol to phototherapy enhance the efficacy of treatment in patients with vitiligo: A systematic review and meta-analysis. International Immunopharmacology. 2021;98:107856. https://pubmed.ncbi.nlm.nih.gov/34198237/ ↩︎
Vitamin D analogs combined with different types of phototherapy in the treatment of vitiligo: A systematic review of randomized trials and within-patient studies. International Immunopharmacology. 2022;109:108712. https://pubmed.ncbi.nlm.nih.gov/35468365/ ↩︎
McCrary MR, Gibbs DC, Alharthi M. Utilization of Our Toolkit: A Systematic Review and Meta-analysis of Surgical Therapies in Vitiligo Treatment. Dermatologic Surgery. 2022;48(8):812-818. https://pubmed.ncbi.nlm.nih.gov/35917262/ ↩︎
Zhang S, Serag I, Olama SM. Safety and efficacy of Simvastatin in the treatment of vitiligo: a systematic review and meta-analysis of randomized controlled trials. Archives of Dermatological Research. 2025;317(4):185-195. https://pubmed.ncbi.nlm.nih.gov/40252138/ ↩︎
Efficacy and safety of compound glycyrrhizin in combination with conventional therapy in treatment of vitiligo: A systematic review and meta-analysis of randomized controlled trials. Medicine. 2023;102(43):e35689. https://pubmed.ncbi.nlm.nih.gov/37904437/ ↩︎
Ashraf AZ, Azurdia RM, Cohen SN. The effectiveness of home-based phototherapy for vitiligo: A systematic review of randomised controlled trials. Photodermatology, Photoimmunology & Photomedicine. 2022;38(5):412-421. https://pubmed.ncbi.nlm.nih.gov/34967477/ ↩︎
Wu YH, Chou CL, Chang HC. Risk of skin cancer after ultraviolet phototherapy in patients with vitiligo: a systematic review and meta-analysis. Clinical and Experimental Dermatology. 2022;47(4):715-722. https://pubmed.ncbi.nlm.nih.gov/34762747/ ↩︎ ↩︎
Alqifari SF, Gari MH, Guo JJ. Descriptive Analysis of Reported Adverse Events Associated with Vitiligo Medications Using FDA Adverse Event Reporting System (FAERS) Databases 2013-2023. Diseases. 2025;13(3):145. https://pubmed.ncbi.nlm.nih.gov/40709998/ ↩︎
Rosmarin D, Pandya AG, Passeron T, et al. Long-Term Integrated Safety Summary of Ruxolitinib Cream in Phase 3 Clinical Trials of Patients with Vitiligo. Dermatology and Therapy. 2025;15(12):2415-2425. https://pubmed.ncbi.nlm.nih.gov/41125994/ ↩︎ ↩︎
Vrijman C, Kroon MW, Limpens J, et al. The prevalence of thyroid disease in patients with vitiligo: a systematic review. The British Journal of Dermatology. 2012;167(6):1224-1235. https://pubmed.ncbi.nlm.nih.gov/22860695/ ↩︎