¶ AOD-9604: Benefits, Dosage, & Side Effects
| Sequence | Tyr-Leu-Arg-Ile-Val-Gln-Cys-Arg-Ser-Val-Glu-Gly-Ser-Cys-Gly-Phe |
| Formula | C78H123N23O23S2 |
| Molar Mass | 1815.1 g/mol |
| Category | Growth Hormone Fragment |
| Half-life | Short (< 1 hour) |
| Admin | Subcutaneous Injection |
| FDA Status | Unapproved; FDA safety-risk concerns for compounding |
| CAS | 221231-10-3 |
AOD-9604 is a synthetic peptide fragment derived from the C-terminus of human growth hormone (hGH), specifically designed to isolate the fat-burning (lipolytic) properties of the hormone without its growth-promoting effects. Despite early promise in animal models and generally reassuring tolerability in human trials, it failed to demonstrate convincing weight-loss efficacy in the larger obesity program and remains an unapproved drug with FDA-identified compounding safety concerns.
¶ At a glance
Aliases
- Also known as: Tyr-hGH177-191, LAT8881
- Amino acid sequence: Tyr-Leu-Arg-Ile-Val-Gln-Cys-Arg-Ser-Val-Glu-Gly-Ser-Cys-Gly-Phe
- Sequence length: 16 amino acids (Hexadecapeptide)
- Category: Lipolytic Peptide, Growth Hormone Fragment
Key points
- Primary Mechanism: Stimulates lipolysis (fat breakdown) and inhibits lipogenesis (fat storage) in animal models by upregulating beta-3 adrenergic receptors[1].
- Clinical Reality: Early obesity work suggested a possible signal, but the larger Phase 2b program using 0.25-1 mg oral doses for 24 weeks did not establish a reliable weight-loss benefit beyond placebo plus lifestyle intervention.[2][3]
- Cartilage Potential: Shows promise in rabbit models for regenerating cartilage when combined with hyaluronic acid, but no human clinical trials validate this effect[4].
- Critical Safety Status: FDA has identified potential immunogenicity, peptide impurity, and characterization concerns for compounded AOD-9604 products; AOD-9604-related nominations were later withdrawn, but the safety-risk rationale remains published by FDA.[5][6]
What people use it for
- Main goals: Fat loss (specifically stubborn adipose tissue), cartilage repair, and joint healing.
- Evidence quality: Low for obesity (negative human data); Very Low for cartilage (animal data only).
¶ Legal & regulatory status
FDA Status: AOD-9604 is not an FDA-approved drug. FDA has published significant compounding safety concerns for AOD-9604, especially immunogenicity risk for some routes, peptide-related impurities, and incomplete characterization. FDA's current page lists AOD-9604 among withdrawn bulk-substance nominations rather than as an ordinary approved compounding ingredient, so it should not be described as FDA-approved or routine clinical therapy.[^5][^6]
WADA Status: PROHIBITED at all times (in and out of competition) under section S2. Peptide Hormones, Growth Factors, Related Substances, and Mimetics. Usage will result in a doping violation.[^7]
Regulatory classification
- FDA Status: Unapproved drug. FDA does not list AOD-9604 as an FDA-approved medication, and FDA's compounding materials raise unresolved safety and quality concerns rather than endorsing routine use.[5:1][6:1]
- Prescription requirement: Any U.S. clinical use depends on ordinary drug and compounding law, state rules, route, formulation, and whether a lawful compounding basis exists. Consumer "research chemical" sales are not evidence of legal clinical approval.
Geographic legal status
- United States: Strictly regulated. It is not FDA-approved as a drug, and FDA has published safety-risk concerns relevant to compounded products.
- Australia: Originally developed here by Metabolic Pharmaceuticals. Not approved for medical use.
Sports and competition
- WADA: Banned. Anti-doping laboratories have specific detection methods for AOD-9604 metabolites in urine and blood. The "Essendon Football Club supplement saga" in Australia heavily featured AOD-9604, leading to significant sanctions.
Source quality considerations
- Research Chemical Grade: Since pharmaceutical production was terminated in 2007, all currently available AOD-9604 is "research grade" or underground.
- Contamination: The FDA has cited difficulty in manufacturing this peptide without impurities, which contributes to the immunogenicity risk (body attacking its own growth hormone)[6:2].
¶ What is AOD-9604?
AOD-9604 is a modified form of the C-terminal fragment of the human growth hormone (hGH) molecule. The full hGH protein is 191 amino acids long; the region responsible for fat burning is located at the very end (residues 177-191).
- Definition: A synthetic hexadecapeptide (16 amino acids) consisting of the hGH 177-191 sequence with an added tyrosine at the N-terminus.
- Purpose of Modification: The natural hGH 177-191 fragment is extremely unstable and degrades within minutes in the bloodstream. The addition of tyrosine and the formation of a disulfide bond (cyclization) significantly improve its stability and resistance to proteases[7].
- Development History: Developed by Metabolic Pharmaceuticals in the late 1990s as a potential blockbuster obesity drug. The goal was to harness the fat-burning power of growth hormone without the side effects (insulin resistance, organ growth, IGF-1 elevation).
¶ What are AOD-9604's main benefits?
Note: The benefits listed below are largely theoretical or based on animal models. Human clinical trials failed to confirm the primary weight loss benefit.
¶ Targeted Fat Loss (Lipolysis)
The most touted benefit of AOD-9604 is its ability to target adipose tissue specifically.
- Mechanism: It binds to receptors on fat cells to trigger the release of stored fat (lipolysis) and inhibit the storage of new fat (lipogenesis).
- Human Data: In the Phase 2b "OPTIONS" study (n=536), AOD-9604 did not produce statistically significant weight loss compared to placebo when both groups followed a diet and exercise program. The drug failed to show an additive effect[2:1].
¶ Cartilage and Joint Repair
Following the failure in obesity trials, research pivoted to musculoskeletal applications.
- Animal Data: In rabbit models of collagenase-induced osteoarthritis, intra-articular injections of AOD-9604 combined with hyaluronic acid significantly improved cartilage regeneration scores and reduced lameness compared to hyaluronic acid alone[4:1].
- Human Data: There are no published randomized controlled trials (RCTs) in humans confirming this effect. Claims of joint repair in humans are currently anecdotal or extrapolated from animal data.
¶ Favorable Metabolic Profile
Unlike full-length hGH, AOD-9604 does not induce hyperglycemia or insulin resistance.
- IGF-1 Independence: It does not bind to the hGH receptor in the liver and does not stimulate the production of IGF-1[8]. This eliminates the risk of acromegaly and potential cancer concerns associated with elevated IGF-1.
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Weight Loss (Obesity) | ↔ (no effect) | High | High | 1 Phase 2b RCT | 536 obese adults, 24 weeks. Failed to outperform placebo + diet/exercise.[2:2] |
| Safety / Tolerability | ↔ (safe) | High | Moderate | 6 Clinical Trials | Generally well-tolerated in trials up to 24 weeks. No IGF-1 elevation.[8:1] |
| Cartilage Repair | ? (unclear) | N/A | Very Low | 0 Human Trials | No human RCTs exist. Efficacy is based entirely on rabbit models.[4:2] |
| Glucose Tolerance | ↔ (neutral) | High | Moderate | 2 RCTs | Does not impair insulin sensitivity or glucose levels (unlike hGH).[8:2] |
*Effect: ↔ (no clear effect), ? (unclear/no data). Health impact: (p) = positive, (n) = negative.
**Consistency: High (trials agree), Low (conflict).
***Trials: Number of human clinical trials.
¶ How does AOD-9604 work?
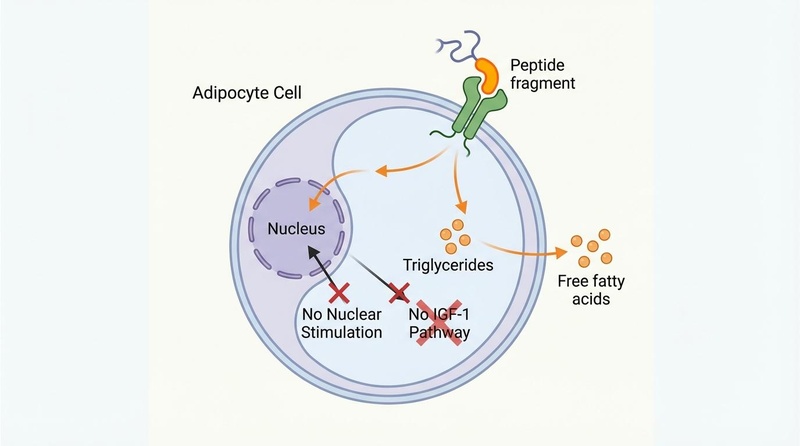
AOD-9604 functions by mimicking the lipolytic domain of the human growth hormone molecule while lacking the domain required for high-affinity binding to the hepatic growth hormone receptor.
¶ Primary Targets
- Adipocytes (Fat Cells): AOD-9604 interacts with receptors on the surface of fat cells. In rodent models, it has been shown to increase the expression of beta-3 adrenergic receptors (-AR)[1:1].
- Mechanism: By upregulating -AR RNA, it enhances the cell's sensitivity to catecholamines (like adrenaline), promoting the breakdown of triglycerides into glycerol and free fatty acids.
¶ Downstream Effects
- Inhibition of Lipogenesis: It appears to reduce the activity of enzymes responsible for synthesizing new fat, such as acetyl-CoA carboxylase[1:2].
- Chondrocyte Differentiation (Proposed): In cartilage, it may stimulate the differentiation of mesenchymal stem cells into chondrocytes (cartilage cells), promoting the synthesis of collagen type II and proteoglycans, though the specific receptor pathway for this is less understood than the lipolytic pathway[4:3].
¶ Administration, reconstitution, and storage
¶ Routes of Administration
- Subcutaneous Injection: This is the most common and effective route. It is typically injected into the abdominal fat pad or thigh.
- Oral: While Metabolic Pharmaceuticals attempted an oral formulation (protected by a specialized coating), bioavailability was a major challenge. Standard research peptides are not orally bioavailable and will be destroyed by stomach acid.
- Topical: Transdermal creams exist but lack data on absorption efficiency.
¶ Reconstitution
AOD-9604 is typically supplied as a lyophilized (freeze-dried) white powder that must be reconstituted with bacteriostatic water.
- Diluent: Bacteriostatic water (water with 0.9% benzyl alcohol) is preferred to maintain sterility for multiple doses.
- Technique: Inject the water slowly down the side of the vial to avoid damaging the peptide. Swirl gently; do not shake.
- Example: Adding 2 mL of water to a 5 mg vial yields a concentration of 2.5 mg/mL (2500 mcg/mL).
¶ Storage
- Powder: Store at -20°C (freezer) for long-term stability.
- Reconstituted: Must be stored in the refrigerator (2-8°C). Use within 2-4 weeks.
¶ Dosage and protocols
¶ Standard Dosing (Historical Trials)
In the Metabolic Pharmaceuticals trials, doses ranged from 0.25 mg to 1 mg daily.
- Paradoxical Dose Response: Early Phase 2a data suggested that lower doses (1 mg) might be more effective than higher doses (10-30 mg), a phenomenon known as a "U-shaped" or "Bell-shaped" dose-response curve. However, the larger Phase 2b trial found no significant effect at any dose[2:3].
¶ Community Protocols (Anecdotal)
Users in the body composition community often follow this protocol, though it is not validated by successful trials:
- Dose: 300 mcg (0.3 mg) per day.
- Timing: Administered in the morning on a completely empty stomach (fasted).
- Fasting Window: Users typically wait 30-60 minutes after injection before eating, as insulin release is believed to blunt the lipolytic effect.
- Cycle Length: 4 to 8 weeks.
¶ Safety and side effects
¶ Common Side Effects
In clinical trials involving over 900 patients, AOD-9604 was generally well-tolerated with a safety profile similar to placebo[8:3].
- Injection site reactions: Redness, swelling, or mild pain at the injection site.
- Headache: Reported in a small percentage of users.
- GI Distress: Mild nausea or indigestion (mostly with oral formulation).
¶ Serious Safety Concerns (FDA 2024-2026 Update)
Despite reassuring tolerability in earlier sponsored trials, FDA raised significant flags in its compounding materials regarding compounded AOD-9604 products.[5:2][6:3]
- Immunogenicity: FDA warns that compounded AOD-9604 may pose immunogenicity risk for certain routes of administration. Because the peptide overlaps with native hGH sequence, antibody formation is a biologically plausible concern that requires careful product-specific evaluation.
- Impurities and characterization: FDA notes peptide-related impurities and API characterization concerns. This matters because small changes in peptide synthesis, purification, storage, or formulation can change aggregation and immune risk.
¶ Contraindications
- Pregnancy/Breastfeeding: No safety data exists. Strictly avoid.
- Active Cancer: While AOD-9604 does not raise IGF-1, any growth-hormone-derived agent should be treated with extreme caution in the context of malignancy.
¶ Combining AOD-9604 with other peptides
Note: These combinations are purely anecdotal and lack clinical validation.
- AOD-9604 + BPC-157: Popular for injury recovery. BPC-157 is used for soft tissue (tendon/ligament) repair, while AOD-9604 is added for potential cartilage regeneration.
- AOD-9604 + CJC-1295/Ipamorelin: A "fat loss stack." CJC/Ipamorelin increases endogenous growth hormone pulses, while AOD-9604 is added to theoretically maximize lipolysis. However, given AOD-9604's lack of efficacy in isolation, the additive benefit is questionable.
¶ Practical questions (FAQ)
1. Did AOD-9604 actually work for weight loss in trials?
No. In the definitive Phase 2b trial (OPTIONS study), it failed to produce more weight loss than placebo. Both groups lost weight due to diet and exercise, but the drug added no extra benefit[2:4].
2. Why is it banned by the FDA for compounding if it was "safe" in trials?
The FDA distinguishes between "safe to eat" (GRAS food status) and "safe to inject." The recent ban is based on the risk of impurities and immunogenicity (antibody attacks) associated with injectable peptides that haven't gone through the rigorous modern drug approval process[6:4].
3. Will AOD-9604 show up on a drug test?
Yes. WADA-accredited laboratories have sensitive tests for AOD-9604. It is banned for athletes at all times. Standard employment drug screens (5-panel, 10-panel) typically do not test for peptides, but sports anti-doping panels do.
4. Can I take it orally?
Technically yes, but bioavailability is very poor for standard peptide powders. The clinical trials used a specialized protected formulation, and even then, efficacy was lacking. Injection is the only reliable method for delivery, though efficacy remains unproven.
¶ How we evaluated the evidence
- Obesity Efficacy: We relied on the published results of the METAOD005 (OPTIONS) Phase 2b trial. This is high-quality evidence (large sample, randomized, placebo-controlled) that demonstrated a negative result (lack of efficacy).
- Cartilage Efficacy: We assessed the Kwon et al. (2015) rabbit study. This is low-quality evidence for human application because animal results often fail to translate to human joint repair.
- Safety: We incorporated both the historical trial data and the more recent FDA compounding safety-risk materials to separate "tolerated in sponsored trials" from "quality, immunogenicity, and legal concerns for compounded products."
¶ References
Heffernan M, et al. The effects of human GH and its lipolytic fragment (AOD9604) on lipid metabolism following chronic treatment in obese mice and beta(3)-AR knock-out mice. Endocrinology. 2001;142(12):5182-5189. https://doi.org/10.1210/endo.142.12.8522 ↩︎ ↩︎ ↩︎
Metabolic Pharmaceuticals Limited. Metabolic's obesity drug - Phase 2B clinical trial results. ASX Announcement. 2007. https://www.sec.gov/Archives/edgar/vprr/0702/07021963.pdf ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ng FM, et al. Metabolic studies of a synthetic lipolytic domain (AOD9604) of human growth hormone. Hormone Research. 2000;53(6):274-278. https://doi.org/10.1159/000053183 ↩︎
Kwon DR, Park GY. Effect of Intra-articular Injection of AOD9604 with or without Hyaluronic Acid in Rabbit Osteoarthritis Model. Annals of Clinical and Laboratory Science. 2015;45(4):426-432. http://www.annclinlabsci.org/content/45/4/426.long ↩︎ ↩︎ ↩︎ ↩︎
U.S. Food and Drug Administration. Safety Risks Associated with Certain Bulk Drug Substances Nominated for Use in Compounding. FDA.gov. Current as of April 22, 2026. https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks ↩︎ ↩︎ ↩︎
U.S. Food and Drug Administration. December 4, 2024 Pharmacy Compounding Advisory Committee Briefing Document. https://www.fda.gov/media/183583/download ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
More M, et al. Safety and Metabolism of AOD9604, a Novel Nutraceutical Ingredient for Improved Metabolic Health. Journal of Endocrinology and Metabolism. 2014;4(3):64-77. https://jofem.org/index.php/jofem/article/view/213/278 ↩︎
Stier H, Vos E, Kenley D. Safety and Tolerability of the Hexadecapeptide AOD9604 in Humans. Journal of Endocrinology and Metabolism. 2013;3(1-2):7-15. https://www.jofem.org/index.php/jofem/article/view/157/194 ↩︎ ↩︎ ↩︎ ↩︎