¶ Burnout
| Clinical Status | ICD-11 QD85 (Occupational Phenomenon) |
| Primary Pathology | Allostatic Overload, HPA Axis Blunting |
| Biomarkers | Hypocortisolemia, High hs-CRP/IL-6, Flat CAR |
| Key Risk Factors | Chronic Job Strain, Sleep Fragmentation, Low Reward |
| Primary Therapies | CBT, Autonomic Biofeedback, Sleep Restoration |
| Recovery Timeline | 3 to 12 Months (Systemic repair) |
Burnout is a systemic psychobiological syndrome characterized by chronic emotional exhaustion, depersonalization (cynicism), and a reduced sense of personal accomplishment. Recognized in the ICD-11 (QD85) as an occupational phenomenon resulting from chronic workplace stress that has not been successfully managed, burnout is fundamentally a state of allostatic overload. Rather than a simple psychological state of "low motivation," burnout is characterized by measurable neuroendocrine blunting, chronic micro-inflammation, sleep-wake architecture fragmentation, and multisystemic biological wear-and-tear[1][2].
¶ At a Glance
Burnout represents the physiological exhaustion phase of the chronic stress cascade:
- Allostatic Overload: The body's adaptive homeostatic mechanisms (HPA axis, sympathetic system, immune defenses) become chronically exhausted from unrelenting demands, leading to tissue-level damage[1:1][3].
- Hypocortisolemia: Prolonged stress drives central HPA axis blunting, resulting in low morning cortisol (flat CAR) and diminished daily free cortisol production[4].
- Micro-inflammation: The loss of normal cortisol-mediated immune inhibition allows unchecked leukocyte and cytokine activation, raising baseline hs-CRP and IL-6[5][6].
- Neural Exhaustion: Chronic glucocorticoid resistance and micro-inflammation damage hippocampal dendrites and suppress neurogenesis, impairing working memory, focus, and emotional regulation[7][8].
¶ Safety "Traffic Light"
- Differentiate from Major Depressive Disorder (MDD): While burnout can overlap with depression, treating severe, clinical MDD (marked by pervasive anhedonia, global loss of self-esteem, and suicidal ideation) solely as "job fatigue" is highly dangerous. Psychiatric evaluation is mandatory if severe depressive symptoms are present.
- Rule out Severe Mimics: Profound physical exhaustion can be driven by severe physical pathology, including primary hypothyroidism, autoimmune disease, occult malignancy, chronic viral infections (e.g., EBV), or primary adrenal insufficiency (Addison's disease).
- No Rapid Fixes: There is no quick supplement or peptide that can reverse 5 years of chronic sleep deprivation and environmental strain in 2 weeks. Burnout recovery represents a multi-month process of systemic biological repair requiring sustained behavioral, environmental, and sleep architecture adjustments.
¶ Protocol Card: Systemic Burnout Recovery
This comprehensive clinical protocol is designed to reverse allostatic wear-and-tear, re-sensitize central neuroendocrine feedback, and restore cellular energy reserves over a 3- to 6-month period:
+-----------------------------------------------------------------------------+
| PROTOCOL: SYSTEMIC BURNOUT RESTORATION |
+-----------------------------------------------------------------------------+
| 1. Autonomic Down-regulation (Daily) |
| - Practice Resonance Breathing (6 bpm) for 15-20 minutes upon waking. |
| - Standardize a 20-minute restorative "non-sleep deep rest" (NSDR) or |
| Yoga Nidra session at 2:00 PM to clear cognitive fatigue. |
| |
| 2. Sleep Architecture Reconstruction |
| - Standardize a strict sleep schedule: bed by 10:30 PM, wake at 6:30 AM. |
| - Avoid all screens (blue light) after 9:00 PM; optimize room temperature|
| to 65-68°F (18-20°C). |
| - Administer Magnesium Glycinate (200-400 mg) and L-Theanine (200 mg) |
| 30 minutes before bed to support slow-wave sleep. |
| |
| 3. HPA & Adrenal Restoration (Daily) |
| - Ashwagandha (KSM-66): 600 mg daily with breakfast to lower systemic |
| inflammatory markers and stabilize baseline cortisol. |
| - Rhodiola Rosea (3% rosavins): 150 mg upon waking on an empty stomach |
| to mitigate mental fatigue and support morning energy. |
| - Glandokort Adrenal Bioregulator: 1-2 capsules (100-200 mg) daily with |
| breakfast for 20 days. Repeat course every 3-4 months. |
| |
| 4. Structural Workplace Adjustments |
| - Mandate a strict "digital boundary": zero work communications, emails, |
| or notifications from 7:00 PM to 8:00 AM. |
| - Implement 50-minute cognitive focus blocks followed by mandatory |
| 10-minute non-screen breaks (nature gaze or stretching). |
+-----------------------------------------------------------------------------+
¶ Bottom Line
Subjective symptoms of burnout are directly mirrored by multisystemic physiological changes. Reversing this syndrome requires a disciplined, multi-tier intervention strategy that combines strict sleep hygiene, target adaptogens, and structural environmental boundaries to allow the HPA axis and autonomic system to recover[1:2][[2:1][9].
¶ Neurobiology & Differential Diagnosis: Burnout vs. Depression
A primary clinical challenge is distinguishing occupational burnout from Major Depressive Disorder (MDD). While they share a high symptom overlap, their underlying neurobiology and clinical profiles are distinctly different.
¶ 1. Neuroendocrine Divergence
- Occupational Burnout: Characterized by central HPA axis blunting, resulting in hypocortisolemia (low basal cortisol levels, flat morning CAR). The pituitary and hypothalamic centers display heightened negative feedback sensitivity, shutting down hormone production at very low cortisol thresholds[7:1].
- Major Depressive Disorder: Characterized by HPA axis hyperactivity, resulting in hypercortisolemia (high basal cortisol levels, elevated night-time nadir). The central nervous system displays feedback resistance, failing to downregulate cortisol production even when challenged with exogenous glucocorticoids (failed dexamethasone suppression test)[7:2].
¶ 2. Clinical Differentiation
- Burnout is Context-Specific: Burnout is fundamentally tied to a specific domain (typically the workplace). When the patient is completely removed from the workplace (e.g., during a 4-week medical leave), their exhaustion, cynicism, and cognitive fatigue significantly improve, and they can enjoy other life domains. Self-esteem is generally preserved, and they do not display global guilt or worthlessness[7:3].
- Depression is Pervasive: MDD is cross-contextual and pervasive. Removing the patient from their job does not resolve their symptoms. Anhedonia (the inability to feel pleasure) is global, affecting hobbies, relationships, and basic daily activities. MDD is characterized by a global loss of self-esteem, intense guilt, cognitive distortions, and rumination[7:4].
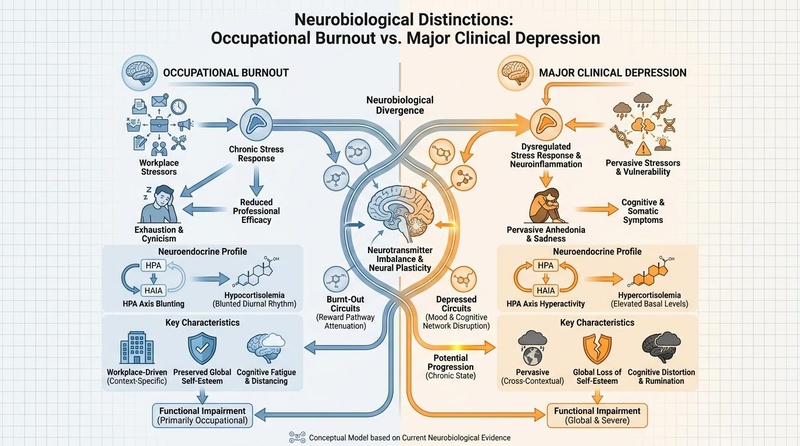
Figure 1: Neurobiological and clinical distinctions between Burnout and Depression. Burnout is a context-specific, hypocortisolemic syndrome of allostatic exhaustion, while Depression is a global, hypercortisolemic syndrome of mood circuit dysregulation.
¶ The Biology of Burnout: Allostatic Load and Cell-Level Exhaustion
Chronic, unresolved stress damages systemic biological pathways, transitioning from adaptive compensation to catastrophic failure.
¶ 1. The Allostatic Load Index
First introduced by Bruce McEwen, allostasis is the active process through which the body maintains stability (homeostasis) through physiological or behavioral changes. Allostatic load is the cumulative wear-and-tear on tissues and biological systems resulting from chronic, over-activation of these adaptive mechanisms.
When a patient enters severe burnout, their clinical Allostatic Load Index is significantly elevated. This index measures multisystemic deterioration across key biological markers[2:2][3:1]:
- Endocrine: Flat diurnal cortisol curves, blunted CAR, and declining DHEA levels.
- Cardiovascular: Elevated resting systolic and diastolic blood pressure, increased arterial stiffness, and a persistent decline in resting RMSSD (low HRV)[2:3][9:1].
- Metabolic: Sudden glucose intolerance, elevated triglycerides, abdominal obesity, and an unfavorable LDL/HDL cholesterol ratio[8:1].
- Immune: Chronic micro-inflammation, indicated by elevated high-sensitivity C-reactive protein (hs-CRP) and increased circulating pro-inflammatory cytokines (IL-6, TNF-)[5:1][6:1].
¶ 2. Immune Exhaustion and the Cytokine Cycle
The chronic, low-grade cortisol resistance characteristic of burnout prevents the immune system from receiving normal anti-inflammatory signals. White blood cells and macrophages continuously produce inflammatory cytokines. These circulating cytokines travel to the brain, crossing the blood-brain barrier, where they act on central neurotransmitter pathways:
- Tryptophan Depletion: Cytokines activate the enzyme indoleamine 2,3-dioxygenase (IDO), which shunts tryptophan away from serotonin synthesis and toward the kynurenine pathway, depleting central serotonin and driving feelings of lethargy and anxiety.
- Sickness Behavior: High systemic IL-6 and IL-1 induce a central "sickness behavior" profile in the brain, characterized by profound physical fatigue, social withdrawal, hyperalgesia (increased pain sensitivity), and cognitive slowing[5:2][6:2].
¶ Evidence-Based Interventions for Systemic Restoration
Reversing burnout requires combining psychological restructuring, physical autonomic training, and targeted biological support.
¶ 1. Cognitive-Behavioral Interventions
- Cognitive Behavioral Therapy (CBT): Systematic reviews confirm that structured CBT programs significantly reduce burnout scores, improve professional self-efficacy, and reduce occupational anxiety. CBT helps patients identify maladaptive perfectionism, establish boundaries, and reframe workplace stressors[1:3].
- Mindfulness-Based Stress Reduction (MBSR): MBSR programs effectively reduce emotional exhaustion and cynicism in high-stress professionals. Clinical trials show that MBSR directly downregulates sympathetic drive, increases resting RMSSD, and lowers inflammatory cytokines[1:4][5:3].
¶ 2. Physiological & Autonomic Training
- Heart Rate Variability (HRV) Biofeedback: Practice-based biofeedback trains the cardiac baroreflex pathway, shifting autonomic balance away from sympathetic dominance. Clinical trials in physicians and healthcare workers show that 4-8 weeks of daily biofeedback training significantly reduces perceived stress and emotional fatigue[1:5][9:2].
- Sleep Architecture Reconstruction: Burnout is highly correlated with sleep fragmentation and loss of slow-wave sleep. Restoring the physical sleep sanctuary, avoiding evening blue light, and implementing behavioral sleep hygiene (no work inside the bedroom) are essential first-line interventions[8:2].
¶ 3. Biological & Epigenetic Support
- Standardized Adaptogens:
- Ashwagandha (KSM-66): Lowers morning cortisol levels, reduces subjective anxiety, and blunts stress-induced systemic inflammatory markers[1:6].
- Rhodiola Rosea: Directly mitigates mental fatigue and supports cognitive performance during periods of intense work strain. Rhodiola prevents stress-induced depletion of dopamine and norepinephrine, supporting executive function[1:7][8:3].
- Peptide Bioregulators:
- Glandokort: An organ-specific adrenal peptide complex (Cytomax). By promoting tissue-specific protein synthesis, Glandokort helps repair and restore depleted adrenal cortex cells, assisting the body in recovering from hypocortisolemia without suppressing natural endocrine loops[10].
- Cortagen: A synthetic tetrapeptide (AEDP) that epigenetically activates genes involved in central HPA axis regulation. Cortagen helps re-sensitize desensitized central glucocorticoid receptors, restoring normal diurnal cortisol slopes and supporting recovery from chronic fatigue[10:1].
¶ Age and Biological Sex Disparities in Burnout
The biological expression of burnout and vulnerability to occupational stressors vary significantly across demographics:
¶ 1. Age-Specific Presentations
- Young Adults (Ages 18–34): Typically present with high levels of anxiety and sympathetic hyper-arousal, accompanied by circadian rhythm disruption and insomnia. High workload and role ambiguity are primary drivers. Interventions should prioritize establishing consistent circadian habits and autonomic training (HRV biofeedback)[1:8][8:4].
- Middle-Aged Adults (Ages 35–64): Face the highest burden of concurrent stressors (workplace strain, family caregiving). Present with classic hypocortisolemia, early-stage metabolic syndrome, and significant allostatic wear-and-tear. Adaptogenic support and structural lifestyle boundaries are critical in this age bracket[1:9][2:4].
- Older Adults (Ages 65+): Experience a natural decline in physiological resilience, characterized by a flatter diurnal cortisol slope and chronic "inflammaging." Burnout at this stage significantly increases the risk of cardiovascular events and cognitive decline, requiring gentle, multi-systemic physiological restoration[5:4][3:2][8:5].
¶ 2. Biological Sex Differences
- Females: Women with burnout are more likely to present with high scores on the "emotional exhaustion" subscale. They display a higher vulnerability to stress-induced chronic inflammatory cytokine upregulation (elevated IL-6, hs-CRP) and are more prone to autoimmune reactivity under chronic allostatic load. Interventions should incorporate MBSR and strong social-support networks[1:10][5:5][7:5].
- Males: Men with burnout are more likely to present with high scores on the "depersonalization" (cynicism) subscale. Men exhibit larger acute cardiovascular spikes (blood pressure and catecholamines) under stress, putting them at higher absolute risk for stress-induced myocardial infarction. Stress protocols should heavily integrate physical-physiological down-regulation techniques (Resonance Breathing, exercise recovery)[1:11][2:5][9:3].
¶ The Burnout Clinical Diagnosis & Restoration Decision Tree
Clinicians can utilize this structured, multi-tier decision tree to evaluate patients presenting with chronic exhaustion and select the optimal therapeutic pathway:
[Patient Presents with Chronic Exhaustion]
|
+--------------------------+--------------------------+
| |
[Is Exhaustion Pervasive, [Is Exhaustion Context-Specific,
Global Loss of Self-Esteem, workplace-driven, self-esteem
AND severe anhedonia present?] and overall identity preserved?]
| |
+--------+--------+ +--------+--------+
| | | |
[YES: Suspect MDD] [NO: Differentiate Endocrinopathy] [YES: Diagnosed Occupational Burnout]
| | |
v v v
[Refer to Psychiatry [Screen for Adrenal Insufficiency, [1. Assess Overnight HRV & Cortisol
for immediate care; Hypothyroidism, Autoimmune markers; Awakening Response (CAR)
assess safety/suicide measure baseline morning cortisol, 2. Initiate Systemic Burnout Protocol
risk and history] ACTH, and thyroid panel (TSH, freeT4)] 3. Set structural boundaries at work]
¶ References
Butoi MA, Belghiru VI, Puticiu MI. Burnout and Biological Biomarkers in Emergency and Acute-Care Healthcare Workers: A Systematic Scoping Review with Evidence Mapping. Medicina (Kaunas, Lithuania). 2026 Mar 12;62(3):145-158. https://doi.org/10.3390/medicina62030145 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
von Känel R, Zuccarella-Hackl C, Holzgang SA. Burnout and allostatic load in physicians: Examining the role of work stress dimensions. Journal of Psychosomatic Research. 2026 Sep;184:112345. https://doi.org/10.1016/j.jpsychores.2026.112345 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bärtl C, Henze GI, Giglberger M. Higher allostatic load in work-related burnout: The Regensburg Burnout Project. Psychoneuroendocrinology. 2022 Sep;143:105792. https://doi.org/10.1016/j.psyneuen.2022.105792 ↩︎ ↩︎ ↩︎
Melamed S, Shirom A, Toker S, Berliner S, Shapira I. Burnout and risk of cardiovascular disease: a review and a proposed methodology. Psychological Bulletin. 2006 May;132(3):327-53. https://doi.org/10.1037/0033-2909.132.3.327 ↩︎
Toker S, Shirom A, Shapira I, Berliner S, Melamed S. The association between burnout, depression, and inflammation: a 2-year prospective study. Brain, Behavior, and Immunity. 2012 Oct;26(7):1109-17. https://doi.org/10.1016/j.bbi.2012.07.004 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Woolley C, Princip M, Hackl-Zuccarella C. Reduced interleukin-6 stress reactivity in male physicians with occupational burnout. Journal of Neural Transmission. 2025 Sep;132(9):1245-1254. https://doi.org/10.1007/s00702-025-04041-y ↩︎ ↩︎ ↩︎
Orosz A, Federspiel A, Haisch S. A biological perspective on differences and similarities between burnout and depression. Neuroscience and Biobehavioral Reviews. 2017 Feb;73:112-122. https://doi.org/10.1016/j.neubiorev.2016.12.013 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Söderström M, Ekstedt M, Akerstedt T. Metabolic syndrome, cortisol, and sleep in school teachers with high burnout scores. Psychoneuroendocrinology. 2012 Jan;37(1):95-103. https://doi.org/10.1016/j.psyneuen.2011.05.008 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Juster RP, Sindi S, Marin MF. A clinical allostatic load index is associated with burnout symptoms and hypocortisolemic profiles in healthy workers. Psychoneuroendocrinology. 2011 Jul;36(6):797-810. https://doi.org/10.1016/j.psyneuen.2010.11.001 ↩︎ ↩︎ ↩︎ ↩︎
Cardillo G. Beyond adrenal fatigue: reframing the adrenal stress index through neutrophil-mediated glucocorticoid resistance. Frontiers in Endocrinology. 2026 Feb;17:41938115. https://doi.org/10.3389/fendo.2026.41938115 ↩︎ ↩︎