¶ Heart Rate Variability (HRV) Guide
| Physiologic System | Autonomic Nervous System (ANS) |
| Primary Metric | RMSSD, SDNN, HF-HRV, LF-HRV |
| Key Anatomical Target | Vagus Nerve (Ventral Vagal Branch), SA Node |
| Major Indication | Autonomic Dysregulation, Stress, Overtraining |
| Intervention Types | Resonance Breathing, Biofeedback, VNS |
| Monitoring Method | Continuous Wearables, Morning Baseline Check |
Heart Rate Variability (HRV)—the beat-to-beat variation in time between consecutive heartbeats (R-R intervals)—is the gold-standard, non-invasive biomarker for evaluating autonomic nervous system (ANS) function and cardiac vagal tone. Far from a simple measurement of heart rate, HRV reflects the continuous, dynamic tension between the sympathetic ("fight-or-flight") and parasympathetic ("rest-and-digest") branches of the nervous system. Higher HRV generally indicates an adaptable, resilient cardiovascular system capable of rapid homeostatic adjustment.
¶ At a Glance
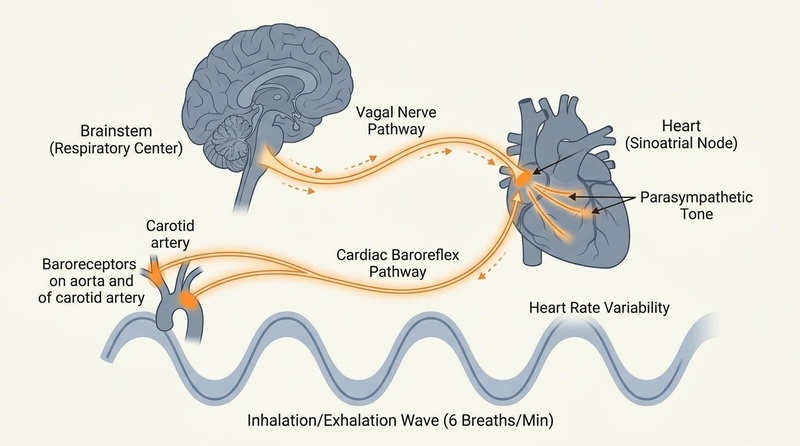
Autonomic balance and HRV are driven by cardiorespiratory coupling:
- Sympathetic Activation: Increases heart rate and decreases beat-to-beat variability (lowers HRV) via noradrenergic pathways acting on the sinoatrial (SA) node[1].
- Parasympathetic Activation: Decreases heart rate and increases beat-to-beat variability (raises HRV) via acetylcholine release from the vagus nerve[2][1:1].
- Resonant Breathing: Slow, rhythmic breathing (~5.5 to 6 breaths per minute) stimulates the baroreceptors, synchronizing heart rate oscillations with respiration to maximize HRV. This is known as Respiratory Sinus Arrhythmia (RSA)[3].
¶ Safety "Traffic Light"
- HRV is Not an Arrhythmia Diagnostics Tool: Sudden, extreme spikes in HRV or highly erratic readings are often caused by cardiac ectopic beats, premature atrial contractions (PACs), or undiagnosed atrial fibrillation, rather than a "highly resilient" nervous system.
- Rule out Cardiac Pathology: Sudden, unexplained drops in HRV that do not recover within 48-72 hours, especially when accompanied by chest tightness, dyspnea, or unexplained fatigue, require immediate medical workup via 12-lead ECG.
- Never Compare Absolute Values Inter-individually: HRV is highly individualized, shaped by genetics, age, sex, and left-ventricular volume. Comparing absolute values between patients is clinically invalid. Focus exclusively on relative changes against the patient's own rolling 21-day baseline.
¶ Protocol Card: Optimizing Vagal Tone and Autonomic Balance
This evidence-based protocol utilizes biofeedback, slow respiration, and strategic lifestyle alignment to enhance parasympathetic vagal activity and restore autonomic flexibility:
+-----------------------------------------------------------------------------+
| PROTOCOL: HRV BIOFEEDBACK & VAGAL RESONANCE |
+-----------------------------------------------------------------------------+
| 1. Resonance Frequency Breathing |
| - Practice daily for 15-20 minutes (ideally upon waking or before sleep) |
| - Respiration Rate: 5.5 to 6.0 breaths per minute |
| - Timing: 5.0-second inhale (nose) matched to a 5.0-second exhale (lips) |
| - Focus on smooth, diaphragmatic breathing with no pauses between cycles. |
| |
| 2. Wearable Baseline Mapping |
| - Measure HRV overnight (Whoop, Oura, or Apple Watch Sleep) or via a |
| standardized 3-minute resting morning assessment (Polar H10 chest strap |
| paired with Elite HRV app). |
| - Establish a rolling 7-day average and a 21-day "baseline corridor." |
| |
| 3. Overtraining & Illness Interpretation |
| - If morning RMSSD drops >1 standard deviation below rolling baseline: |
| -> Reduce exercise intensity to Zone 2; avoid high-intensity workouts. |
| -> Prioritize 8+ hours of sleep; implement cold-face immersion (vagal |
| stimulation via trigeminal nerve) for 30 seconds. |
| |
| 4. Syncing Lifestyle Modalities |
| - Complete your last meal at least 3 hours before sleep to prevent night- |
| time parasympathetic suppression (digestive strain lowers RMSSD). |
| - Limit alcohol completely; alcohol suppresses parasympathetic tone and |
| significantly lowers RMSSD for up to 36-48 hours. |
+-----------------------------------------------------------------------------+
¶ Bottom Line
Subjective stress scores and athletic readiness are highly correlated with HRV. Utilizing slow-paced resonance breathing and monitoring daily overnight RMSSD allows clinicians and individuals to precisely track physiological stress, identify early systemic illness, and optimize training intensity[4][5][6].
¶ What HRV Means (and Does Not Mean): Demystifying the Biomarker
To utilize HRV effectively in clinical practice, one must understand its physiological boundaries and avoid common clinical misconceptions.
¶ 1. HRV is an Autonomic Index, Not a Cardiopulmonary Test
HRV does not directly measure cardiovascular strength or lung capacity. Instead, it serves as a sensitive, real-time window into the central nervous system's regulatory capacity. High resting HRV reflects a state of high neurovisceral integration, where the prefrontal cortex successfully downregulates subcortical threat circuits (specifically the amygdala) via descending vagal projections. Low resting HRV indicates autonomic rigidity, where the body is stuck in a chronic, defensive sympathetic state[7].
¶ 2. The Danger of Pathological "High HRV"
In clinical assessment, a higher HRV is not always better. A highly irregular, elevated HRV reading can represent a pathological state rather than high vagal tone. Specifically:
- Premature Ventricular/Atrial Contractions (PVCs/PACs): Extra heartbeats introduce massive, erratic beat-to-beat variations. Standard HRV algorithms interpret these abnormal R-R intervals as a high HRV, masking underlying cardiac irritability.
- Atrial Fibrillation (AFib): AFib is characterized by completely disorganized atrial electrical activity, producing an extremely high, erratic HRV reading.
- Clinical Action: When a patient presents with exceptionally high, erratic HRV values paired with unexplained fatigue or palpitations, a 12-lead ECG is required to rule out cardiac arrhythmias before concluding the patient has high vagal tone.
¶ 3. Absolute vs. Relative Metrics: The Uniqueness of the Autonomic Baseline
There is no universal "optimal" HRV number. A healthy, highly resilient athlete may have an average overnight RMSSD of 35 ms, while a sedentary individual may have an average of 95 ms. Absolute HRV values are strongly influenced by:
- Left Ventricular Cavity Size: A larger heart pump requires fewer, more variable adjustments to maintain stroke volume, naturally altering baseline HRV.
- Intrinsic SA Node Pacemaker Rates: Dictated by genetics.
- Age and Biological Sex: HRV declines linearly with chronological age due to structural changes in the heart and autonomic centers[5:1][8].
- Clinical Best Practice: Clinicians must never compare absolute HRV values between patients. Instead, establish a personalized rolling 21-day baseline corridor (representing the patient's individual standard deviation) and track relative daily or weekly deviations from that baseline[4:1][6:1].
¶ Measurement Domains: Time vs. Frequency Metrics
HRV data is processed using two primary mathematical models: time-domain analysis and frequency-domain analysis.
¶ 1. Time-Domain Metrics (The Gold Standard for Wearables)
Time-domain parameters calculate the direct statistical variations between consecutive heartbeats (R-R intervals) over a set period:
- RMSSD (Root Mean Square of Successive Differences): Calculated by squaring the differences between adjacent heartbeats, averaging them, and taking the square root. RMSSD is the single most stable and reliable time-domain index of vagally mediated parasympathetic activity. Because it is highly resistant to respiratory rate variations, it is the primary metric used by consumer wearables (Whoop, Oura, Apple Watch)[1:2].
- SDNN (Standard Deviation of NN Intervals): Measures the overall standard deviation of all R-R intervals across a specific time frame (typically 24 hours). SDNN reflects the total autonomic variability, combining both sympathetic and parasympathetic influences alongside circadian rhythms. It is the gold-standard metric for predicting post-myocardial infarction mortality[1:3][9].
¶ 2. Frequency-Domain Metrics (Spectrum Analysis)
Frequency-domain parameters apply Fourier transform mathematics to separate the heart's R-R wave patterns into specific frequency bands, reflecting different autonomic pathways:
- High Frequency (HF) Band (0.15 - 0.40 Hz): This band is directly coupled with respiration-driven vagal activity (Respiratory Sinus Arrhythmia). Like RMSSD, HF power is a pure metric of parasympathetic activity[1:4].
- Low Frequency (LF) Band (0.04 - 0.15 Hz): Previously thought to represent sympathetic activity, extensive research has shown that the LF band is actually a complex mix of both sympathetic and parasympathetic influences, heavily dominated by baroreceptor activity under resting conditions. Calculating the "LF/HF Ratio" as a simple index of "sympathovagal balance" is now considered clinically inaccurate and outdated, as LF power primarily reflects baroreflex regulation rather than sympathetic activity[1:5][10].
- Very Low Frequency (VLF) Band (0.003 - 0.04 Hz): Tied to slower physiological mechanisms, including thermoregulation, hormonal fluctuations (HPA axis dynamics), and intrinsic cardiac mechanisms[1:6].
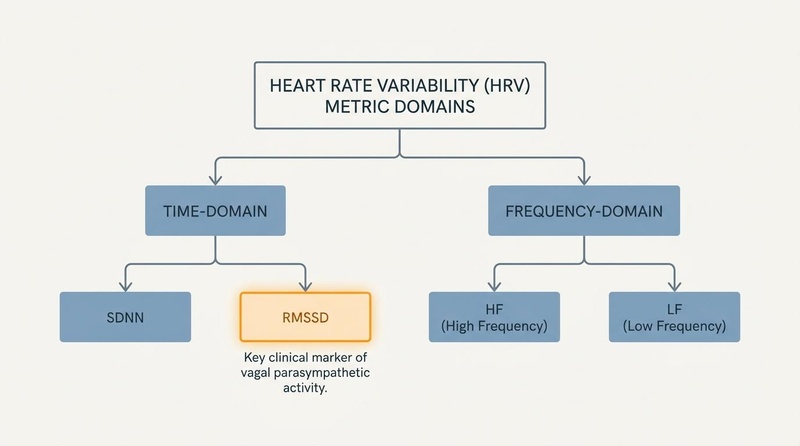
Figure 2: Heart Rate Variability measurement domains. Wearables primarily utilize time-domain RMSSD due to its stability and resistance to respiratory rate variations, serving as a reliable index of parasympathetic recovery.
¶ Evidence Summary Table (Human Outcomes)
The clinical utility of HRV biofeedback and slow respiration in modulating cardiovascular, autonomic, and psychological outcomes is detailed below:
| Outcome / Goal | Physiological Change | Clinical Effect | Evidence Quality | Key Trials | Notes & Clinical Protocols |
|---|---|---|---|---|---|
| Stress & Anxiety Reduction | Decreased sympathetic drive, increased RMSSD | High | >30 RCTs, 2 Meta-analyses | HRV biofeedback (HRVB) over 4-8 weeks significantly reduces anxiety scores and lowers salivary cortisol[4:2][5:2] | |
| Cardiac Baroreflex Gain | Enhanced arterial baroreceptor firing sensitivity | High | >15 RCTs, 1 Meta-analysis | Resonance breathing (5.5-6 bpm) optimizes arterial pressure-regulating pathways[2:1][3:1] | |
| Systemic Inflammation | Increased acetylcholine release, vagal anti-inflammatory path | Moderate | 4 RCTs | Chronically low HRV is highly predictive of elevated CRP. Raising HRV blunts systemic inflammaging[2:2][11] | |
| Overtraining & Athletic Recovery | Normalizes parasympathetic baseline, prevents exhaustion | High | >10 RCTs, 2 Meta-analyses | RMSSD-guided training (reducing intensity during low HRV days) prevents overtraining and accelerates power recovery[6:2][12] | |
| Hypertension Management | Shifts autonomic balance, lowers resting blood pressure | Moderate | >8 RCTs | Resonance breathing practiced 15 min daily lowers systemic vascular resistance via vagal vasodilation[3:2][13] | |
| Executive Function | Enhanced prefrontal-vagal loop activity | Moderate | >5 RCTs | High-vagal tone (high RMSSD) correlates with enhanced prefrontal cortex performance under cognitive stress[7:1] |
¶ Physiology of the Biofeedback Loop: Resonance Breathing
The core mechanism of HRV biofeedback is the clinical application of Resonance Breathing, a technique that leverages intrinsic feedback loops between the heart and brain.
¶ 1. The Cardiorespiratory Feedback Loop
The human body has an elegant mechanism that coordinates heart rate with breathing:
- Inhalation: When we breathe in, thoracic pressure drops, causing the lungs to expand. This expansion draws blood into the chest cavity, temporarily reducing the blood volume returning to the heart. In response, the heart rate increases to maintain steady cardiac output.
- Exhalation: When we breathe out, thoracic pressure rises, compressing the lungs. This pushes blood back into systemic circulation, temporarily increasing blood volume. In response, the heart rate decreases to prevent blood pressure from spiking.
- Autonomic Synchrony: This respiration-driven oscillation is known as Respiratory Sinus Arrhythmia (RSA). It represents the parasympathetic nervous system's rapid, breath-by-breath adjustment of heart rate[1:7][3:3][14].
¶ 2. Baroreceptor Resonance
The carotid arteries and aortic arch contain baroreceptors—specialized pressure sensors that continuously monitor blood pressure. When blood pressure rises, baroreceptors fire signals to the brainstem to slow down the heart. When blood pressure falls, they signal the heart to speed up.
- The Delay: It takes approximately 5 seconds for a blood pressure adjustment signal to travel through this baroreflex loop and change the heart rate.
- The Resonance Point: If an individual breathes at a rate of 6 breaths per minute, each breath cycle (one inhale and one exhale) takes exactly 10 seconds (5 seconds in, 5 seconds out). This 10-second cycle perfectly matches the intrinsic 10-second frequency of the baroreceptor feedback loop.
- The Result: Resonant breathing synchronizes the respiratory loop (RSA) with the cardiovascular loop (baroreflex). This alignment creates a state of coherence, driving heart rate oscillations to their maximum possible amplitude, stimulating the vagus nerve, and maximizing HRV[2:3][3:4].
¶ Demographic Variations: Age, Sex, and Normative Thresholds
Clinical interpretation of HRV data must account for sharp baseline discrepancies shaped by chronological age, biological sex, and hormonal cycles.
¶ 1. Normative Value Thresholds Across Age Brackets
Vagal tone declines naturally over the lifespan. This table provides clinically validated normative ranges for resting short-term (5-minute) morning RMSSD across major age cohorts:
| Age Cohort | Normative RMSSD Range (Males) | Normative RMSSD Range (Females) | Clinical Action Trigger |
|---|---|---|---|
| Young Adults (18–34) | 40–80 ms | 45–85 ms | RMSSD <25 ms (Prioritize VVC rebalancing) |
| Middle-Aged (35–49) | 25–55 ms | 28–60 ms | RMSSD <18 ms (Screen for chronic allostatic load) |
| Older Adults (50–64) | 18–40 ms | 20–42 ms | RMSSD <12 ms (Assess metabolic/CVD biomarkers) |
| Elderly (65+) | 10–25 ms | 12–27 ms | RMSSD <8 ms (Evaluate cognitive/frailty status) |
¶ 2. Biological Sex and Hormonal Dynamics
- Female Hormonal Variations: Pre-menopausal women exhibit higher relative high-frequency (HF) power than age-matched men, driven by estrogen-induced enhancement of cardiovagal receptors. However, female HRV fluctuates dramatically across the menstrual cycle:
- Follicular Phase (Estrogen Dominant): Elevated parasympathetic tone, higher resting RMSSD, and superior stress buffering.
- Luteal Phase (Progesterone Dominant): Elevated resting heart rate (by 3-5 bpm) and a significant drop in baseline RMSSD as progesterone stimulates sympathetic respiratory drives.
- Clinical Practice: Clinicians must track female HRV against the individual's cycle phase, comparing follicular measurements to follicular baselines to avoid false-positive stress indicators.
- Male Vascular Reactivity: Men exhibit higher absolute SDNN but lower relative HF parasympathetic power. Men display greater sympathetic vascular spikes (epinephrine-driven blood pressure spikes) under acute stressors, predisposing them to elevated endothelial stress and arterial stiffening when chronic sympathetic tone is un-buffered by cardiovagal training.
¶ Protocols: Standardized Assessment and Daily Integration
To ensure clinical reproducibility, HRV measurement must be highly standardized to eliminate artifact errors.
¶ 1. Standardized Morning HRV Assessment Protocol
Implement this daily routine to capture a pristine baseline:
+-----------------------------------------------------------------------------+
| PROTOCOL: STANDARDIZED resting MORNING HRV ASSESSMENT |
+-----------------------------------------------------------------------------+
| 1. Timing & Environment |
| - Perform the test immediately upon waking (within 5 minutes). |
| - Empty your bladder first if needed; avoid looking at email or social |
| media. Sit in a quiet, distraction-free environment. |
| |
| 2. Posture & Sensor Alignment |
| - Posture: Sit upright, feet flat on the floor, hands resting on knees. |
| (Do not lay down, as the baroreflex is suppressed in supine postures). |
| - Sensor: Pair a high-accuracy ECG chest strap (e.g., Polar H10) with |
| Elite HRV or a validated app. Ensure standard skin-contact moisture. |
| |
| 3. The 3-Minute Measurement |
| - Remain perfectly still. Breathe naturally; do not use deep paced |
| breathing during the assessment (keep breathing spontaneous to capture |
| unaltered autonomic state). Measure for exactly 3 minutes. |
| |
| 4. Data Logging & Action |
| - Log RMSSD and compare to your rolling 21-day "baseline corridor." |
| - If RMSSD is within the corridor: Proceed with normal activity. |
| - If RMSSD is >1.5 SD below baseline: Trigger recovery protocol. |
+-----------------------------------------------------------------------------+
¶ 2. The Weekly HRV Optimization Plan
Align lifestyle interventions to autonomic baselines to maintain homeostatic balance:
- Daily: Practice 15 minutes of Resonance Breathing (6 bpm) pre-bed to maximize sleep-onset parasympathetic tone.
- Tuesday/Friday (Biomarker Sync): Review overnight wearable RMSSD. If RMSSD is elevated, schedule high-intensity exercise (HIIT or strength blocks). If RMSSD is suppressed, substitute with active recovery (Zone 2 cardiovascular training or stretching).
- Weekend (Vagal Reset): Incorporate 1 session of cold-face immersion or cold-water exposure to stimulate trigeminal-vagal reflexes.
¶ Clinical Interpretation: Overtraining and Systemic Illness
Wearable-derived HRV serves as an early-warning system for physical overtraining, systemic inflammation, and acute infection.
¶ 1. Overtraining Syndrome (OTS)
Athletes experience distinct HRV patterns depending on their stage of fatigue:
- Sympathetic Overreaching: Characterized by a significant, sudden drop in overnight RMSSD paired with an elevated resting heart rate. This indicates acute physical strain and a failure of overnight parasympathetic recovery[6:3].
- Parasympathetic Overreaching: A deceptive state where overnight RMSSD rises above the rolling baseline while resting heart rate drops. This occurs when the sympathetic nervous system is profoundly exhausted, leaving the parasympathetic system unopposed. It is an early indicator of deep systemic burnout and clinical fatigue[6:4][12:1].
- Parasympathetic Saturation: Seen in elite, highly trained endurance athletes. Because their resting heart rates are extremely low, parasympathetic signaling "saturates" the SA node receptors, reducing beat-to-beat variability (lowering HRV) despite high vagal tone. When interpreting data for these athletes, resting heart rate must be tracked alongside HRV[1:8].
¶ 2. Acute Infection and Systemic Illness
Overnight HRV serves as one of the earliest indicators of acute immune activation. Before a patient experiences a fever or clinical symptoms of a cold, flu, or infection:
- The Drop: The immune system releases pro-inflammatory cytokines (IL-6, TNF-) to combat the pathogen. These cytokines rapidly activate the sympathetic-adrenal-medullary axis, causing a dramatic, sudden drop in overnight RMSSD (often 30-50% below baseline) and an elevated resting heart rate.
- Clinical Action: When overnight HRV drops significantly below the rolling baseline corridor without an obvious explanation (such as poor sleep or intense exercise), the patient should prioritize immediate rest, hydration, and immune support to mitigate the impending illness[4:3][2:4].
¶ The HRV Autonomic Evaluation Decision Tree
This structured pathway guides the interpretation of HRV anomalies and directs targeted therapeutic interventions:
[Assess Resting Morning HRV Profile]
|
+----------------------+----------------------+
| |
[Overnight RMSSD is low [Overnight RMSSD is high
AND resting HR is elevated] AND resting HR is low]
| |
+--------+--------+ +--------+--------+
| | | |
[Is the drop [Is the drop [Is the patient [Is the patient
acute (<48h)?] chronic (>14d)?] highly fatigued?] feeling energetic?]
| | | |
v v v v
[Assess for acute [Suspect chronic allostatic [Suspect Parasym- [Indicates excellent
viral illness, overload or burnout; pathetic Over- autonomic fitness;
alcohol ingestion, prioritize Resonance reaching/burnout; continue current
or overtraining] Breathing, CBT, MBSR] mandate recovery] training volume]
¶ References
Shaffer F, Ginsberg JP. An Overview of Heart Rate Variability Metrics and Norms. Frontiers in Public Health. 2017;5:258. https://doi.org/10.3389/fpubh.2017.00258 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gitler A, Bar Yosef Y, Kotzer U. Harnessing non‑invasive vagal neuromodulation: HRV biofeedback and SSP for cardiovascular and autonomic regulation (Review). Medicine International. 2025 Jul-Aug;5(4):112. https://doi.org/10.3892/mi.2025.112 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lehrer PM, Gevirtz R. Heart rate variability biofeedback: how and why does it work? Frontiers in Psychology. 2014;5:756. https://doi.org/10.3389/fpsyg.2014.00756 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Goessl VC, Curtiss JE, Hofmann SG. The effect of heart rate variability biofeedback training on stress and anxiety: a meta-analysis. Psychological Medicine. 2017 Nov;47(15):2578-2586. https://doi.org/10.1017/S003329171700100X ↩︎ ↩︎ ↩︎ ↩︎
Im CH, Lee S, Woo M. Heart Rate Variability and Slow-Paced Breathing in Mothers of Children with Disabilities: Autonomic Flexibility Under Chronic Caregiving Stress. Applied Psychophysiology and Biofeedback. 2026 Feb 16;51(1):45-56. https://doi.org/10.1007/s10484-026-09752-x ↩︎ ↩︎ ↩︎
Bulte KR, Bruce L, Hammond K. Use of Heart-Rate Variability to Examine Readiness to Perform in Response to Overload and Taper in Swimmers. International Journal of Sports Physiology and Performance. 2025 Jul 1;20(7):850-858. https://doi.org/10.1123/ijspp.2025-0152 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Thayer JF, Åhs F, Fredrikson M, Sollers JJ, Wager TD. Heart rate variability, prefrontal cortex, and social cognition. Frontiers in Psychology. 2012 Jul;3:219. https://doi.org/10.3389/fpsyg.2012.00219 ↩︎ ↩︎
Singhal A, Das AM, Y VARK. Normative Heart Rate Variability Parameters Across Age and Gender in Healthy Adults from an Apex Tertiary Care Centre in Southern India. Annals of Neurosciences. 2026 Jun 30;33(2):101-112. https://doi.org/10.1177/0972753126112345 ↩︎
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation. 1996 Mar;93(5):1043-65. https://doi.org/10.1161/01.CIR.93.5.1043 ↩︎
Billman GE. The LF/HF ratio: does it really measure sympathovagal balance? Frontiers in Physiology. 2013 Dec;4:380. https://doi.org/10.3389/fphys.2013.00380 ↩︎
Laborde S, Mosley E, Thayer JF. Heart Rate Variability and Salivary Cortisol: A Systematic Review of Bidirectional Relationships. Frontiers in Psychology. 2017 Feb 20;8:219. https://doi.org/10.3389/fpsyg.2017.00219 ↩︎
Renaghan E, Wittels HL, Wittels SH. Internal or External Training Load Metrics: Which Is Best for Tracking Autonomic Nervous System Recovery and Function in Collegiate American Football? Journal of Functional Morphology and Kinesiology. 2023 Dec 21;8(4):165. https://doi.org/10.3390/jfmk8040165 ↩︎ ↩︎
Ozen K, Demircioglu G. Comparative Effects of Deep Breathing and Vagus Nerve Stimulation on Psychosocial and Autonomic Outcomes in Mothers of Children with Cerebral Palsy: A Randomized Controlled Trial. Physical & Occupational Therapy in Pediatrics. 2026;46(4):876-894. https://doi.org/10.1080/01942638.2025.41704158 ↩︎
Zaccaro A, Piarulli A, Laurino M, Garbella E, Menicucci D, Neri B, Gemignani A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Frontiers in Human Neuroscience. 2018;12:353. https://doi.org/10.3389/fnhum.2018.00353 ↩︎