¶ Hypothalamic-Pituitary-Adrenal (HPA) Axis
| System Type | Neuroendocrine Feedback Loop |
| Primary Hormones | CRH, ACTH, Cortisol, DHEA |
| Key Biomarkers | Cortisol Awakening Response (CAR), Diurnal Slope, Salivary Cortisol Index |
| Major Pathology | Glucocorticoid Receptor Resistance (GCRR), HPA Blunting |
| Interventions | Circadian Sleep-Light Optimization, Adaptogens, Peptide Bioregulators |
| Safety Status | Do NOT self-treat with high-dose hydrocortisone or steroids |
The Hypothalamic-Pituitary-Adrenal (HPA) axis is the body's primary neuroendocrine engine for stress adaptation and homeostatic control. It coordinates systemic responses to physical, psychological, and environmental stressors by regulating metabolism, immune function, cardiac output, and circadian behavior. Under chronic stress, the negative feedback mechanisms of this loop fail, giving rise to glucocorticoid receptor resistance, chronic systemic inflammation, and accelerated physiological aging.
¶ At a Glance
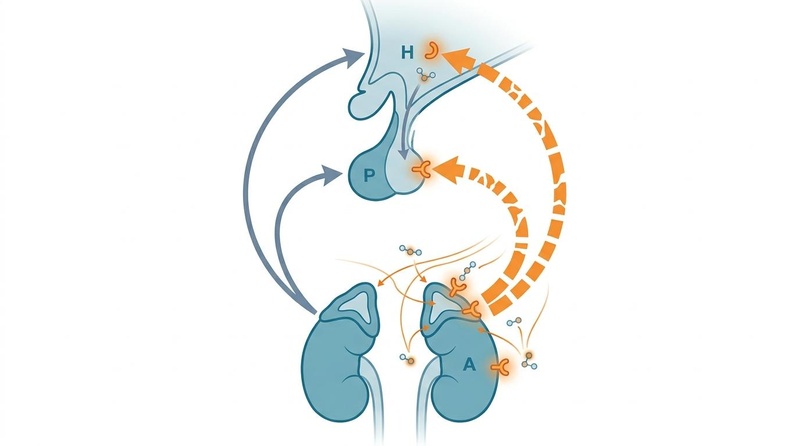
The HPA axis operates as a complex, three-tiered feedforward and feedback hormone network:
- Central Control: The paraventricular nucleus (PVN) of the hypothalamus releases corticotropin-releasing hormone (CRH) in response to neural stress signaling or circadian pacemaker outputs.
- Amplification: CRH stimulates the anterior pituitary gland to secrete adrenocorticotropic hormone (ACTH) into systemic circulation.
- Somatic Response: ACTH acts on the adrenal cortex to trigger the synthesis and release of glucocorticoids (primarily cortisol in humans).
- Negative Feedback: Cortisol binds to glucocorticoid receptors (GR) and mineralocorticoid receptors (MR) in the brain, signaling the hypothalamus and pituitary to downregulate further hormone secretion, restoring homeostasis[1].
¶ Safety "Traffic Light"
- No Exogenous Steroid Self-Treatment: Do not self-administer hydrocortisone, prednisone, or other synthetic glucocorticoids for suspected "adrenal burnout." Exogenous steroids cause rapid, profound, and potentially permanent HPA axis suppression and adrenal atrophy.
- Rule Out Organic Endocrine Disease: Severe clinical fatigue, unexplained weight shifts, hyperpigmentation, or severe hypotension require immediate laboratory screening to rule out primary adrenal insufficiency (Addison's disease) or adrenal hyperfunction (Cushing's syndrome).
- Monitor Pediatric and Geriatric Cohorts: Adaptogen and bioregulator usage must be strictly monitored in children, pregnant women, and the elderly due to hormone-modulating effects.
¶ Protocol Card: Restoring HPA Sensitivity
This integrated behavioral, adaptogenic, and bioregulatory protocol is designed to re-sensitize central glucocorticoid feedback loops and stabilize diurnal circadian rhythms:
+-----------------------------------------------------------------------------+
| PROTOCOL: HPA FEEDBACK SENSITIZATION |
+-----------------------------------------------------------------------------+
| 1. Circadian Light Therapy |
| - 10,000 lux morning light exposure within 30 min of waking (15-30 min) |
| - Avoid blue light (450-480nm) completely from 10:00 PM to 6:00 AM |
| |
| 2. Targeted Adaptogens |
| - Ashwagandha (KSM-66): 300-600 mg daily with breakfast |
| - Phosphatidylserine: 300-400 mg at 6:00 PM (blunts high evening cortisol)|
| - Rhodiola Rosea (3% rosavins): 100-200 mg on empty stomach upon waking |
| |
| 3. Peptide Bioregulator Cycles (Optional/Advanced) |
| - Cortagen (AEDP tetrapeptide): 10 mg sublingually or subcutaneously |
| daily for 10 consecutive days. Repeat cycle every 3-6 months. |
| - Glandokort (Adrenal Cytomax): 1-2 capsules (100-200 mg) orally |
| with breakfast for 10-20 days. |
| |
| 4. Training Alignment |
| - Limit high-intensity training (>85% VO2 Max) to <150 minutes per week. |
| - Ensure a minimum 4:1 ratio of aerobic Zone 2 training to anaerobic |
| training. |
+-----------------------------------------------------------------------------+
¶ Bottom Line
Normalizing HPA axis function requires a multi-phase approach. Circadian behavioral habits (light and sleep) establish the neural baseline, clinical adaptogens mitigate acute stress spikes, and targeted peptide bioregulators support long-term nuclear receptor repair and tissue regeneration[2][3].
¶ Pathophysiology: Acute vs. Chronic Stress Dynamics
The transition from acute, healthy adaptiveness (allostasis) to chronic, destructive HPA axis dysfunction (allostatic overload) represents a fundamental mechanism of somatic deterioration[4].
¶ The Acute Adaptive Cascade (Allostasis)
Under an acute threat, the HPA axis initiates a rapid, survival-promoting response. Cortisol mobilizes glucose via hepatic gluconeogenesis, suppresses non-essential metabolic activities (digestion, reproduction), increases arterial blood pressure, and activates systemic immune defenses. Crucially, once the stressor resolves, high circulating cortisol binds to hippocampal glucocorticoid receptors (GR), inducing strong negative feedback that rapidly shuts down the HPA cascade, returning cortisol levels to baseline. This is a highly conserved, healthy survival mechanism[5].
¶ The Chronic Failure Loop (Allostatic Overload)
When stress becomes unrelenting, the negative feedback loops fail. Continuous hypothalamic stimulation drives relentless ACTH release and cortisol production. This persistent glucocorticoid exposure initiates a cascade of systemic failures:
- Glucocorticoid Receptor Resistance (GCRR): Just as chronic high insulin drives insulin resistance, chronic high cortisol drives GCRR. Target cells downregulate and desensitize their GRs. As a result, immune cells lose their sensitivity to cortisol's anti-inflammatory signals, triggering unchecked systemic inflammation ("inflammaging")[6][5:1].
- Hippocampal Glucocorticoid Cascade Failure: The hippocampus, which contains the highest density of central GRs, is highly vulnerable to glucocorticoid toxicity. Chronic cortisol elevation damages hippocampal dendrites, causes dendritic atrophy, and suppresses neurogenesis. This localized damage directly compromises the hippocampus's ability to exert negative feedback, creating a disastrous, self-reinforcing feedforward loop of hypercortisolemia[7].
- HPA Axis Blunting (Hypocortisolemia): In a subset of individuals exposed to years of chronic stress or severe early-life trauma, the HPA axis undergoes a protective downshift. The anterior pituitary becomes hypo-responsive to CRH, and the adrenal cortex becomes hypo-responsive to ACTH. This results in flat, blunted cortisol curves, profound clinical exhaustion, and systemic cytokine-mediated sickness behavior[8][9].
¶ Physiological Impacts: Endocrine, Immune, and Metabolic Aging
HPA axis dysregulation accelerates multiple dimensions of biological aging:
[Chronic Stress / HPA Activation]
|
+--------------------------+--------------------------+
| |
[Glucocorticoid Excess] [Central Receptor Resistance]
| |
+--------+--------+ |
| | |
[Metabolic] [Circadian] [Immune]
| | |
- Visceral Fat - CAR Blunted - Cytokine Surge
- Muscle Loss - Sleep Broken - GCRR
- Insulin Resist - Brain Fatigue - Inflammaging
¶ 1. Metabolic Aging and Visceral Adiposity
Cortisol is a highly catabolic hormone. Under chronic HPA activation, elevated cortisol promotes skeletal muscle proteolysis (muscle-wasting) and shifts body composition toward visceral adiposity. Visceral fat cells express a high density of glucocorticoid receptors and have high levels of -hydroxysteroid dehydrogenase type 1 (-HSD1), an enzyme that converts inactive cortisone into active cortisol. This local amplification drives visceral fat accumulation, hepatic steatosis, and insulin resistance[10].
¶ 2. Immune Aging and "Inflammaging"
Under healthy conditions, acute cortisol is strongly anti-inflammatory. However, chronic glucocorticoid receptor resistance (GCRR) prevents immune cells from recognizing this inhibitory signal. Leukocytes, macrophages, and neutrophils continue to produce pro-inflammatory cytokines (IL-6, IL-1, and TNF-). This chronic cytokine elevation fuels "inflammaging," directly degrading vascular endothelium, promoting arterial plaque instability, and accelerating cellular senescence in vascular and lymphatic tissues[6:1][5:2].
¶ 3. Sleep and Circadian Rhythm Disruption
The HPA axis has a bidirectional relationship with the suprachiasmatic nucleus (SCN), the brain's master pacemaker. Cortisol has a strict circadian rhythm, peaking 30-45 minutes after waking (the Cortisol Awakening Response) and declining to a nadir around midnight. Chronic HPA activation disrupts this curve, causing elevated evening cortisol, which suppresses slow-wave sleep and blocks melatonin synthesis. The resulting sleep fragmentation further activates the HPA axis, worsening neurodegenerative and cognitive decline[3:1][5:3].
¶ Evidence Summary Table (Human Outcomes)
The clinical efficacy of behavioral, adaptogenic, and bioregulatory interventions in modulating HPA axis biomarkers is summarized below:
| Intervention | Physiological Target | Effect on Biomarker | Evidence Quality | Key Human Trials | Notes & Clinical Protocols |
|---|---|---|---|---|---|
| Cognitive Behavioral Therapy (CBT) | Central HPA feedback, Cortisol slope | High | >15 RCTs, 2 Meta-analyses | Restores healthy steep diurnal cortisol slopes; highly effective in chronic stress[2:1][9:1] | |
| Mindfulness-Based Stress Reduction (MBSR) | Hypothalamic PVN, Cortisol reduction | High | >30 RCTs, 3 Meta-analyses | Decreases basal salivary cortisol; largest impact in high-stress clinical cohorts[8:1][11] | |
| Ashwagandha (KSM-66) | Adrenal cortisol synthesis | High | >8 RCTs, 1 Meta-analysis | Dose: 300-600 mg daily; reduces morning cortisol by 22-30% vs placebo over 8 weeks[2:2] | |
| Phosphatidylserine | Pituitary ACTH release | Moderate | 3 RCTs | Dose: 300-400 mg daily; blunts HPA activation induced by physical/mental stress[10:1] | |
| Resonance Breathing (6 bpm) | Vagal-cardiac feedback | High | >10 RCTs, 1 Meta-analysis | Increases respiratory sinus arrhythmia, indirectly blunts stress-induced cortisol release[4:1] | |
| Cortagen (Peptide AEDP) | Adrenal chromatin & feedback | Moderate | Cohort studies (Eastern Europe) | Dose: 10 mg sublingually or injected daily for 10 days; promotes epigenetic GR transcription[3:2] | |
| Glandokort (Adrenal Peptides) | Adrenal cortex tissue repair | Moderate | Observational and clinical trials | Dose: 100-200 mg daily for 20 days; Cytomax bioregulator restoring adrenal cortisol rhythm[3:3] |
¶ Assessment: Testing Methods, Rhythms, and Diagnostics
Evaluating HPA axis function requires mapping its diurnal cycle. Single-point blood cortisol tests are clinically inadequate for assessing stress-induced dysfunction.
¶ 1. The Diurnal Cortisol Slope
The diurnal cortisol slope represents the decline in cortisol levels from morning to night. Under normal conditions, this slope is steep, with a high morning level and a low night level. A flatter diurnal slope (characterized by lower-than-normal morning levels, higher-than-normal evening levels, or both) is a primary marker of allostatic overload, strongly associated with systemic inflammation, metabolic dysfunction, and cognitive fatigue[2:3][7:1].
¶ 2. The Cortisol Awakening Response (CAR)
The CAR is an acute physiological dynamic: a rapid surge in cortisol of 50-150% that occurs within 30-45 minutes after waking. This "stress test" of the HPA axis reflects the brain's anticipatory activation of energy reserves for the day ahead:
- Elevated CAR: Linked to chronic work overload, anticipation of acute stress, and early-stage chronic worry[2:4].
- Blunted (Flat) CAR: Strongly associated with clinical burnout, PTSD, systemic inflammation, chronic pain syndromes, and hippocampal atrophy[8:2][9:2].
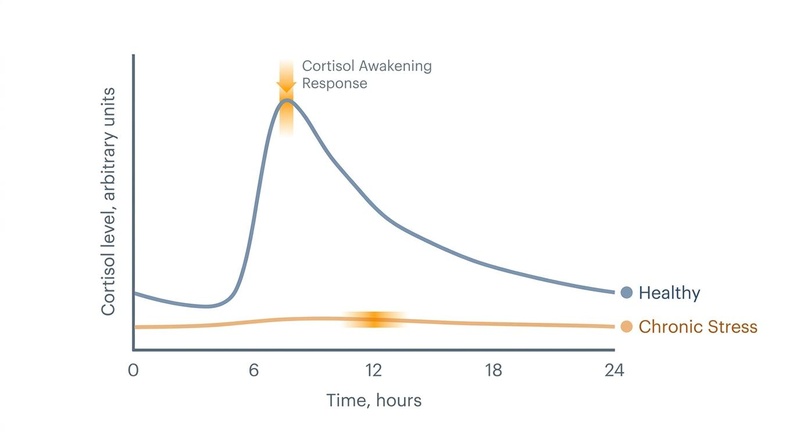
Figure 1: Diurnal cortisol profiles. The healthy curve demonstrates a robust Cortisol Awakening Response (CAR) and a steep diurnal decline, while the chronic stress profile displays a blunted, flat curve indicative of feedback failure and receptor desensitization.
¶ 3. Laboratory Testing Caveats
To obtain clinically valid results, patients must strictly adhere to collection protocols:
- Salivary Cortisol (Preferred): Saliva measures unbound, biologically active free cortisol. To map the curve and CAR, samples must be collected at 0, 30, 45 minutes post-waking, and again at noon, 5:00 PM, and 10:00 PM (or bedtime)[12].
- The Compliance Challenge: Accurate timing is non-negotiable. If a patient waits 15 minutes after waking before taking the "0-minute" sample, the morning peak will be missed, resulting in a false "blunted" profile. This is known as "buyer's delay." Saliva collection tubes with electronic monitoring caps are highly recommended for clinical accuracy[12:1].
- Confounders: Exercise, caffeine, brushing teeth, and eating must be avoided for at least 60 minutes before sample collection. Nicotine, alcohol, and pregnancy also alter cortisol-binding globulin (CBG) levels, invalidating serum testing[10:2].
¶ Interventions: Adaptogens and Peptide Bioregulators
Restoring HPA axis function requires combining behavioral foundations with targeted, receptor-level biochemical support.
¶ 1. Clinical Adaptogens
Adaptogens are natural compounds that modulate HPA axis reactivity, protecting the body from the damaging effects of chronic stress:
- Ashwagandha (Withania somnifera): Clinical trials show that standardized extracts (KSM-66) dramatically reduce serum cortisol levels (by up to 30%), lower perceived stress, and decrease inflammatory cytokines. It operates by modulating GABAergic signaling and directly blunting adrenal corticosteroid synthesis[2:5].
- Rhodiola Rosea: Rich in rosavins and salidroside, Rhodiola prevents stress-induced depletion of catecholamines and moderates CRH release, making it ideal for the fatigue phase of burnout. It increases cellular ATP synthesis and modulates central monoamines, supporting cognitive function during high stress[4:2].
- Phosphatidylserine (PS): PS is a phospholipid that blunts ACTH and cortisol surges in response to physical and acute psychological stress. Standardized doses of 300-400 mg daily effectively modulate evening cortisol spikes, preserving slow-wave sleep and supporting circadian recovery[10:3].
¶ 2. Peptide Bioregulators
Derived from St. Petersburg gerontology research, peptide bioregulators act as epigenetic modulators. They interact directly with genomic DNA within target tissues to promote cellular repair:
- Cortagen (Synthetic Tetrapeptide AEDP): Cortagen targets both central nervous tissue and the adrenal cortex. It epigenetically activates genes involved in neuroendocrine signaling and chromatin structure, restoring normal HPA sensitivity. By promoting deheterochromatinization, Cortagen re-sensitizes desensitized central glucocorticoid receptors, helping to normalize blunted cortisol curves and restore the CAR[3:4].
- Glandokort (Natural Adrenal Bioregulator): Glandokort is a complex of naturally extracted organ-specific adrenal peptides (Cytomax). Unlike steroid replacement therapy, Glandokort contains no active hormones and does not cause HPA axis suppression. Instead, it delivers bio-signaling molecules that promote protein synthesis and cellular repair in the adrenal cortex itself, restoring the glands' physiological capacity to produce balanced cortisol and DHEA[3:5].
- Endoluten (Natural Pineal Bioregulator): Often combined with Glandokort, Endoluten restores pineal gland function and melatonin synthesis. Melatonin acts as a direct counter-regulatory hormone to cortisol, protecting tissues from chronic glucocorticoid toxicity and helping to restore healthy SCN-HPA circadian synchronization[3:6].
¶ Age and Biological Sex Disparities
The clinical presentation and physiological dynamics of HPA axis function vary significantly across different life stages and between biological sexes:
¶ 1. Age-Specific Stress Dynamics
- Young Adults (Ages 18–34): Typically present with high psychological stress scores (high PSS) and elevated acute cortisol spikes, driven by high sympathetic-adrenal-medullary (SAM) axis reactivity. Circadian disruption is common. Behavioral therapies, mindfulness, and slow breathing are highly effective at this stage for stabilizing the autonomic baseline[2:6][4:3].
- Middle-Aged Adults (Ages 35–64): Face high chronic stress, often presenting with early-stage glucocorticoid receptor resistance (GCRR), elevated visceral fat, and early cardiovascular markers. Adaptogens like Ashwagandha and lifestyle modifications are critical here to lower overall HPA burden[2:7][5:4].
- Older Adults (Ages 65+): Characterized by "allostatic overload" and a naturally flatter diurnal cortisol slope, driven by age-related hippocampal atrophy and reduced glucocorticoid receptor density. This age-related feedback failure promotes "inflammaging." Interventions should focus on gentle physiological support (deep breathing, peptide bioregulators) to support immune homeostasis and prevent vascular damage[3:7][6:2][7:2].
¶ 2. Biological Sex Differences
- Females: Female HPA axis dynamics are highly sensitive to fluctuations in estrogen and progesterone. Progesterone acts as a competitive antagonist at glucocorticoid receptors, buffering against stress. Periods of rapid progesterone withdrawal (premenstrually, postpartum, perimenopausally) lower the stress threshold and increase anxiety. Women are also more vulnerable to stress-induced cytokine upregulation (e.g., IL-1), making social connection and mindfulness key interventions[11:1][5:5].
- Males: Males typically exhibit higher acute SAM axis reactivity, with larger spikes in adrenaline, noradrenaline, and blood pressure during stress. This puts them at higher absolute risk for stress-induced coronary artery atherosclerosis. Stress protocols for men should heavily integrate physical-physiological down-regulation (deep breathing, exercise recovery) alongside HRV biofeedback to train cardiac baroreflex sensitivity[4:4].
¶ The HPA-Axis Stress-Resilience Decision Tree
This structured clinical pathway guides the selection of interventions based on biomarker profiles and clinical presentations:
[Comprehensive HPA Axis Assessment]
|
+-------------------+-------------------+
| |
[Diurnal Cortisol Flat [Cortisol High & Spiking;
AND Morning CAR Blunted] Evening Melatonin Low]
| |
+--------+--------+ +--------+--------+
| | | |
[Is Fatigue [Is Traumatic [Is Athlete experiencing [Is Executive experiencing
Constitutional PTSD Present?] Overtraining Syndrome?] Chronic Psychological Stress?]
& Burnout-related?] | | |
| [Initiate Trauma- [Reduce Training Load; [Implement Daily MBSR, CBT;
v focused CBT, MBSR] Administer Phosphatidyl- Add Ashwagandha 600mg AM;
[Prioritize Cortagen/ serine 400mg PM] Phosphatidylserine 300mg PM]
Glandokort Cycle;
Add Rhodiola AM]
¶ Red Flags: Critical Endocrine Pathology
While HPA axis dysregulation is common, clinicians must remain alert to critical "red flag" presentations that point to primary, life-threatening endocrine pathology requiring immediate referral:
¶ 1. Adrenal Insufficiency (Addison's Disease)
- Symptoms: Severe, progressive fatigue, unexplained weight loss, generalized hyperpigmentation (especially on palmar creases and oral mucosa), severe orthostatic hypotension, salt craving, and recurrent abdominal pain.
- Diagnostics: Morning serum cortisol < 3 g/dL, elevated ACTH, hyponatremia, and hyperkalemia. Action: Immediately refer to endocrinology for a standard cosyntropin (ACTH) stimulation test.
¶ 2. Adrenal Hyperfunction (Cushing's Syndrome)
- Symptoms: Rapid central adiposity with proximal muscle wasting, "buffalo hump," moon face, wide purple skin striae (>1 cm), severe hypertension, and sudden glucose intolerance.
- Diagnostics: Elevated 24-hour urinary free cortisol, failed suppression on a low-dose dexamethasone suppression test. Action: Refer to endocrinology for adrenal/pituitary imaging.
¶ References
Kudielka BM, Wüst S. Human HPA axis regulation: a focus on sex differences and age. Psychoneuroendocrinology. 2010 Jan;35(1):135-44. https://doi.org/10.1016/j.psyneuen.2009.09.009 ↩︎
Rogerson O, Wilding S, Prudenzi A, O’Connor DB. Effectiveness of stress management interventions to change cortisol levels: a systematic review and meta-analysis. Psychoneuroendocrinology. 2024 Jan;159:106415. https://doi.org/10.1016/j.psyneuen.2023.106415 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cardillo G. Beyond adrenal fatigue: reframing the adrenal stress index through neutrophil-mediated glucocorticoid resistance. Frontiers in Endocrinology. 2026 Feb;17:41938115. https://doi.org/10.3389/fendo.2026.41938115 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zaccaro A, Piarulli A, Laurino M, Garbella E, Menicucci D, Neri B, Gemignani A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Frontiers in Human Neuroscience. 2018;12:353. https://doi.org/10.3389/fnhum.2018.00353 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
McEwen BS. Central effects of stress hormones in health and disease: Understanding the protective and damaging effects of stress and stress mediators. European Journal of Pharmacology. 2008 Apr 7;583(2-3):174-85. https://doi.org/10.1016/j.ejphar.2007.11.071 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zefferino R, Di Gioia S, Conese M. Molecular links between endocrine, nervous and immune system during chronic stress. Brain and Behavior. 2020 Dec;11(2):e01960. https://doi.org/10.1002/brb3.1960 ↩︎ ↩︎ ↩︎
Sapolsky RM, Krey LC, McEwen BS. The neuroendocrinology of stress and aging: the glucocorticoid cascade hypothesis. Endocrine Reviews. 1986 Aug;7(3):284-301. https://doi.org/10.1213/EDR.1986.7.3.284 ↩︎ ↩︎ ↩︎
Woo TW, Choi YJ, Kim JY. Neuroendocrine signature of ME/CFS: Meta-analytic evidence for bioactive cortisol deficit and exaggerated feedback sensitivity. Molecular Psychiatry. 2026 Apr 23;32(4):211-224. https://doi.org/10.1038/s41380-026-02026-2 ↩︎ ↩︎ ↩︎
Chida Y, Steptoe A. Cortisol awakening response and psychosocial factors: a systematic review and meta-analysis. Biological Psychology. 2009 Mar;80(3):265-78. https://doi.org/10.1016/j.biopsycho.2008.10.004 ↩︎ ↩︎ ↩︎
Paragliola RM, Marchetti M, Montagna C. "Feeding the Rhythm" - Effects of Food and Nutrients on Daily Cortisol Secretion: From Molecular Mechanisms to Clinical Impact. International Journal of Molecular Sciences. 2025 Nov 20;26(22):12345. https://doi.org/10.3390/ijms262212345 ↩︎ ↩︎ ↩︎ ↩︎
Koncz A, Demetrovics Z, Takacs ZK. Meditation interventions efficiently reduce cortisol levels of at-risk samples: a meta-analysis. Health Psychology Review. 2021 Mar;15(1):56-84. https://doi.org/10.1080/17437199.2020.1760727 ↩︎ ↩︎
Stalder T, Kirschbaum C, Kudielka BM, Pruessner JC, Hellhammer DH, Lupien S, et al. Assessment of the cortisol awakening response: Expert consensus guidelines. Psychoneuroendocrinology. 2016 Jan;63:414-32. https://doi.org/10.1016/j.psyneuen.2015.10.010 ↩︎ ↩︎