¶ Clinical Contraindications: Frontier Blood, Plasma, Immune, and Regenerative Therapies
This page outlines critical safety considerations, risks, and clinical contraindications for advanced blood, plasma, immune, and regenerative therapies. Understanding these limitations is crucial for patient safety and appropriate clinical application.
| Type | Advanced Clinical Interventions |
| Focus | Safety, Risks, Contraindications |
| Main Concerns | Hypocalcemia, Anaphylaxis, Malignancy, Infection, Immunosuppression |
| Evidence Quality | High (Clinical Guidelines, Systematic Reviews) |
| Context | Professional Reference, Clinical Education |
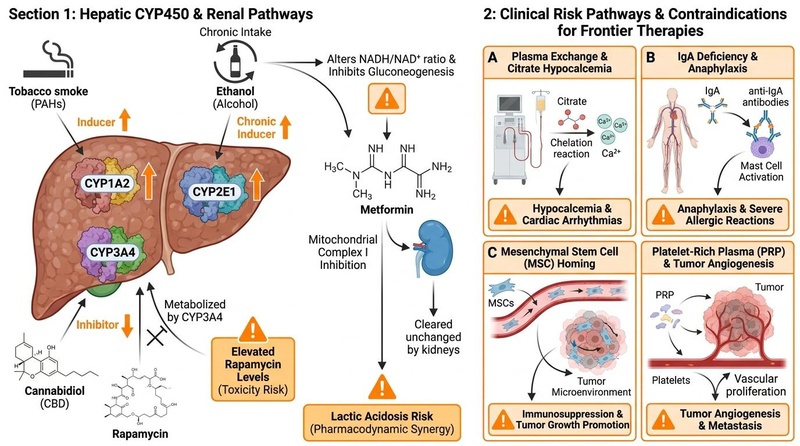
Frontier therapies, including therapeutic plasma exchange, immunoglobulin therapy, stem cell therapy, exosomes, and platelet-rich plasma, offer significant potential but carry inherent risks. Careful assessment of contraindications and potential adverse events is paramount to ensure patient safety and optimize outcomes within the field of regenerative medicine and blood-based interventions.
¶ At a glance
Key points (high-level summary)
- Therapeutic Plasma Exchange (TPE): Absolute contraindications include active sepsis, uncorrectable coagulopathy, severe hemodynamic instability, and severe allergy to replacement fluids. Relative contraindications exist for ACE inhibitor use within 24 hours of the procedure [1][2].
- Immunoglobulin Therapy (IVIG/SCIG): Absolute contraindications include a history of severe anaphylactic or systemic hypersensitivity reactions to human immunoglobulin, particularly in IgA-deficient patients with anti-IgA antibodies [3][4].
- Mesenchymal Stem Cell (MSC) Therapy: While generally considered safe, risks include transient fever, infection, and theoretical concerns regarding malignant transformation or tumor promotion, though evidence for the latter in clinical trials is generally low [5][6]. Unregulated products pose higher risks [7].
- Exosome Therapy: Currently, no exosome products are FDA-approved. Unapproved exosome products have been linked to serious adverse events including bacterial infections, allergic reactions, and tumor formation. Regulatory warnings are in place due to patient safety concerns [8][9][10].
- Platelet-Rich Plasma (PRP): Contraindications include active infection at the injection site, significant hematologic abnormalities (e.g., severe thrombocytopenia), and systemic malignancy, especially in the area of treatment due to theoretical concerns of growth factor stimulation [11].
What people use it for
- Main goals: Understanding clinical limitations, ensuring patient safety, guiding appropriate therapeutic selection.
- Evidence quality (overall): High (based on clinical guidelines, systematic reviews, and meta-analyses).
¶ What are the main contraindications and risks for Frontier Therapies?
This section provides a brief narrative summary of the main safety concerns and contraindications for each therapy, supported by the best available evidence.
¶ Therapeutic Plasma Exchange (TPE)
Therapeutic plasma exchange (TPE), while effective for numerous conditions, involves significant risks. Absolute contraindications include active sepsis or severe hemodynamic instability, as the procedure can exacerbate these conditions. Uncorrectable coagulopathy also poses an absolute contraindication due to the risk of bleeding. Severe allergy to replacement fluids (e.g., albumin, fresh frozen plasma) is another critical contraindication. Relative contraindications may include the use of ACE inhibitors within 24 hours of TPE, which can lead to severe hypotension [1:1][2:1]. Catheter-related complications, such as infection or thrombosis, are also notable risks [12].
¶ Immunoglobulin Therapy (IVIG/SCIG)
Immunoglobulin therapy (IVIG/SCIG) is generally safe but has specific contraindications. The most critical is a history of anaphylactic or severe systemic hypersensitivity reactions to human immunoglobulin. This is particularly relevant for individuals with IgA deficiency who have developed antibodies to IgA, as subsequent exposure to IgA-containing IVIG products can trigger life-threatening anaphylaxis [3:1][4:1]. Other potential adverse effects include renal dysfunction, acute renal failure, and osmotic nephropathy, especially in predisposed patients. Infusion-related reactions such as headaches, flushing, fever, and chills are common but usually mild and manageable [13].
¶ Mesenchymal Stem Cell (MSC) Therapy
Mesenchymal Stem Cell (MSC) therapy has shown a generally favorable safety profile in clinical trials, with no documented cases of MSC-derived malignancy. Common adverse events are typically mild and transient, such as fever, administration site reactions, constipation, fatigue, and sleeplessness. However, concerns exist regarding the potential for infection and theoretical risks of malignant transformation or tumor promotion, particularly with long-term culture or uncharacterized cells. The use of unregulated MSC products significantly increases these risks [5:1][6:1][7:1][14].
¶ Exosome Therapy
The regulatory landscape for exosome therapy is critical. There are currently no FDA-approved exosome products, and serious adverse events have been reported from unapproved products marketed as containing exosomes. These events include bacterial infections, severe allergic reactions, and even tumor formation. Patients and practitioners are strongly warned against using unapproved exosome products outside of legitimate clinical trials due to significant patient safety concerns and lack of established efficacy [8:1][9:1][10:1].
¶ Platelet-Rich Plasma (PRP) Therapy
Platelet-Rich Plasma (PRP) therapy, which utilizes autologous blood components, generally carries a low risk of allergic reactions or disease transmission. However, contraindications include active infection at the injection site, which could be exacerbated. Significant hematologic abnormalities, such as severe thrombocytopenia or platelet dysfunction, may also contraindicate PRP. While PRP is autologous, there are theoretical concerns about its use in patients with systemic malignancy, especially if injected near a known tumor, due to the presence of growth factors that could potentially stimulate tumor growth or angiogenesis [11:1]. Common side effects are usually mild and temporary, such as localized pain, swelling, or bruising at the injection site [15].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| TPE: Hypocalcemia | High | High | 5+ RCTs | Risk of citrate toxicity, particularly with large volume exchanges [1:2][12:1] | |
| IVIG: Anaphylaxis | High | High | Case Reports, Guidelines | Severe reaction in IgA-deficient patients with anti-IgA antibodies [3:2][4:2] | |
| MSC Therapy: Infection | Moderate | Moderate | 20+ RCTs | Generally low risk, but present with any invasive procedure [5:2][6:2] | |
| MSC Therapy: Tumor Growth | Low | Low | Animal/In Vitro, Theoretical | No direct clinical evidence of MSC-derived malignancy, but theoretical concerns [7:2][14:1] | |
| Exosome Therapy: Infection/Allergy | High | Not applicable | FDA Warnings, Case Reports | Unapproved products linked to serious adverse events [8:2][9:2][10:2] | |
| PRP: Infection at site | Low | High | Observational, Guidelines | Risk with any injection, mitigated by sterile technique [11:2][15:1] | |
| PRP: Tumor Stimulation | Very Low | Theoretical | Theoretical, Preclinical | Concerns due to growth factors; no strong human evidence [11:3] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ How do contraindications and risks manifest?
Understanding the mechanisms behind these contraindications helps in risk mitigation and patient selection.
¶ Therapeutic Plasma Exchange: Citrate Toxicity and Vascular Access
TPE often uses citrate as an anticoagulant. Citrate chelates calcium, and rapid or large-volume exchanges can lead to hypocalcemia, manifesting as paresthesias, muscle cramps, and in severe cases, cardiac arrhythmias or seizures [12:2]. Vascular access, typically via a central venous catheter, carries risks of pneumothorax, hemothorax, infection, and thrombosis. The procedure also involves potential for fluid shifts and hemodynamic instability, especially in critically ill patients [2:2].
¶ Immunoglobulin Therapy: Allergic Reactions and Renal Concerns
For IgA-deficient individuals, the presence of anti-IgA antibodies can lead to severe anaphylactic reactions upon exposure to IgA in IVIG products [3:3]. These reactions can include urticaria, bronchospasm, hypotension, and angioedema. Additionally, IVIG products can contribute to acute kidney injury, particularly in patients with pre-existing renal impairment, diabetes, or those receiving high doses. This is often linked to the sucrose content in some formulations, which can cause osmotic nephropathy [13:1].
¶ Mesenchymal Stem Cell Therapy: Immunomodulation and Unintended Effects
MSCs are known for their immunomodulatory properties, which can be beneficial in some contexts but problematic in others. While MSCs generally do not form tumors themselves, there is a theoretical concern that they could home to existing tumor microenvironments and potentially promote tumor growth or metastasis through paracrine effects or by suppressing anti-tumor immunity [7:3][14:2]. The primary safety concerns observed in clinical trials are fever and local reactions, with severe adverse events like infection being rare but possible with any invasive procedure [5:3][6:3].
¶ Exosome Therapy: Unregulated Products and Systemic Risks
The primary risk associated with exosome therapy outside of regulated clinical trials is the use of unapproved and uncharacterized products. These unregulated preparations can contain contaminants, lack sterility, and have inconsistent exosome content, leading to serious adverse events such as severe bacterial infections, systemic inflammatory responses, and allergic reactions. The lack of robust safety and efficacy data for most commercially available exosome products makes their use highly risky [8:3][9:3][10:3].
¶ Platelet-Rich Plasma Therapy: Growth Factors and Infection Risk
PRP contains a concentrated mixture of growth factors that promote tissue repair and angiogenesis. While beneficial for regenerative purposes, the application of these growth factors in proximity to a pre-existing or undiagnosed malignancy theoretically could stimulate tumor growth or metastasis [11:4]. Although this remains largely a theoretical concern with limited clinical evidence, it necessitates careful patient screening. As with any injection, there is an inherent risk of local infection, pain, and bruising at the injection site [15:2].
¶ Safety and side effects
¶ Common side effects
- Therapeutic Plasma Exchange: Citrate-induced paresthesias, lightheadedness, nausea, chills, hypotension [1:3][12:3].
- Immunoglobulin Therapy: Headache, flushing, fever, chills, fatigue, nausea, diarrhea, mild allergic reactions (e.g., rash, pruritus) [13:2].
- Mesenchymal Stem Cell Therapy: Transient fever, mild administration site reactions (pain, redness), fatigue, constipation [5:4].
- Exosome Therapy (Unapproved Products): Severe bacterial infections, allergic reactions, systemic inflammatory responses, and potentially tumor formation [8:4][9:4][10:4].
- Platelet-Rich Plasma: Localized pain, swelling, bruising, and tenderness at the injection site [15:3].
¶ Less common / serious concerns
- Therapeutic Plasma Exchange: Severe hypocalcemia (cardiac arrhythmias, seizures), severe hypotension, air embolism, anaphylaxis to plasma products, severe bleeding from coagulopathy, catheter-related complications (pneumothorax, hemothorax, thrombosis, infection) [1:4][12:4].
- Immunoglobulin Therapy: Anaphylaxis (especially in IgA-deficient patients with anti-IgA antibodies), acute kidney injury, aseptic meningitis, thrombotic events (stroke, myocardial infarction), hemolytic anemia [3:4][4:3][13:3].
- Mesenchymal Stem Cell Therapy: Systemic infections, pulmonary embolism, theoretical risk of tumor promotion (though not clinically observed with characterized MSCs), inadvertent differentiation or immune reactions [7:4][14:3].
- Exosome Therapy (Unapproved Products): As above, but with higher frequency and severity due to lack of quality control, sterility, and regulatory oversight [8:5][9:5][10:5].
- Platelet-Rich Plasma: Local infection (rare with sterile technique), nerve injury (very rare), theoretical risk of stimulating dormant malignancy [11:5][15:4].
¶ Who should be especially cautious or avoid it
- Therapeutic Plasma Exchange: Patients with active sepsis, uncorrectable coagulopathy, severe hemodynamic instability, known allergy to replacement fluids. Caution with ACE inhibitor use.
- Immunoglobulin Therapy: Individuals with IgA deficiency and anti-IgA antibodies; patients with severe renal impairment, hyperviscosity, or a history of thrombotic events.
- Mesenchymal Stem Cell Therapy: Patients with active infections, uncontrolled systemic inflammation, or existing malignancies (due to theoretical concerns and need for careful assessment). Caution in pregnant or breastfeeding individuals due to lack of data.
- Exosome Therapy: Unapproved exosome products are clinically contraindicated across all applications due to high risk of contamination and lack of standard characterization. Legitimate administration is restricted to FDA-approved clinical trials.
- Platelet-Rich Plasma: Patients with active infection at the injection site, severe thrombocytopenia or platelet dysfunction, or systemic malignancy (especially if the treatment site is near a tumor). Caution in pregnant or breastfeeding individuals due to lack of data.
¶ Drug and supplement interactions
¶ Pharmacokinetic interactions (how drugs are processed)
- Therapeutic Plasma Exchange: Can remove certain drugs (e.g., antibiotics, immunosuppressants, highly protein-bound drugs) from circulation, potentially necessitating dose adjustments. Close monitoring of drug levels is required [1:5].
- Immunoglobulin Therapy: Can interfere with the immune response to live virus vaccines; may affect serologic tests for antibodies [3:5].
- Mesenchymal Stem Cell Therapy: Limited data on direct drug interactions. Potential for interactions with immunosuppressants or immunomodulators if MSCs significantly alter immune responses.
- Exosome Therapy: No established interaction profile due to lack of approved products. Unapproved products may contain unknown substances that interact with medications.
- Platelet-Rich Plasma: Antiplatelet drugs (e.g., aspirin, NSAIDs) and anticoagulants may theoretically reduce the effectiveness of PRP by impairing platelet function or increasing bleeding risk at the injection site. Corticosteroids may also counteract the beneficial effects of growth factors [11:6].
¶ Pharmacodynamic interactions (additive / opposing effects)
- Therapeutic Plasma Exchange: Can exacerbate hypotension when combined with antihypertensive medications, especially ACE inhibitors [2:3].
- Immunoglobulin Therapy: None specifically noted outside of vaccine interference.
- Mesenchymal Stem Cell Therapy: Potential for additive immunosuppression if combined with other immunosuppressive agents.
- Exosome Therapy: Unknown due to lack of approved products.
- Platelet-Rich Plasma: None specifically noted.
¶ Practical questions (FAQ)
-
Are frontier therapies generally safe for longevity purposes?
The safety of frontier therapies for explicit longevity purposes is largely unproven, and many interventions lack robust clinical trial data for healthy aging populations. While some therapies are safe for approved indications, their use solely for anti-aging is often experimental and carries uncharacterized risks, especially with unregulated products [9:6][14:4]. -
What criteria define a legitimate clinical setting for administering frontier therapies?
Legitimate administration occurs within regulated medical facilities by licensed clinicians. Appropriate protocols utilize either FDA-approved products or are conducted under authorized investigational protocols registered on platforms such as ClinicalTrials.gov [8:6][9:7]. -
How are adverse events from frontier therapies documented and reported?
Adverse events are typically documented in clinical records and reported to regulatory pharmacovigilance databases, such as the FDA's MedWatch system. This reporting is essential for updating clinical safety databases and refining safety protocols [9:8].
¶ How we evaluated the evidence
Our evaluation prioritizes the highest tiers of evidence:
- High: Clinical guidelines from authoritative bodies (e.g., ASFA for apheresis), systematic reviews, and meta-analyses of randomized controlled trials (RCTs) with consistent results and low risk of bias.
- Moderate: Individual high-quality RCTs, or multiple RCTs with minor limitations or mixed but leaning results.
- Low: Observational studies, case series, or mechanistic studies in humans. Significant limitations in study design or small sample sizes.
- Very Low: Primarily animal or in vitro data, theoretical concerns, or case reports with serious flaws.
We assess the magnitude of effect, consistency across studies, risk of bias, and directness of evidence to human outcomes. This page will be updated as new, high-quality clinical evidence emerges.
¶ References
Sergent SR, Ashurst JV. Plasmapheresis. StatPearls. 2023. https://www.ncbi.nlm.nih.gov/books/NBK560566/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Winters JL. Complications of therapeutic plasma exchange. Transfusion. 2011;51(8):1781–1801. https://pubmed.ncbi.nlm.nih.gov/?term=Winters+complications+therapeutic+plasma+exchange ↩︎ ↩︎ ↩︎ ↩︎
Orange JS, et al. Use of intravenous immunoglobulin in human disease: review and update. J Allergy Clin Immunol. 2006;117(4):S525–S553. https://www.jacionline.org/article/S0091-6749(08)01561-3/fulltext ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Gammagard Liquid. Important Safety Information. https://www.gammagard.com/hcp/pidd/dosing-administration (Referencing specific product warnings for IgA deficiency) ↩︎ ↩︎ ↩︎ ↩︎
Baranovskii DS, et al. Adverse events, side effects and complications in mesenchymal stromal cell-based therapies. Stem Cell Investig. 2022;9:40. https://pmc.ncbi.nlm.nih.gov/articles/PMC9659480/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Levy ML, et al. Cell therapy with intravascular administration of mesenchymal stromal cells continues to appear safe: An updated systematic review and meta-analysis. EClinicalMedicine. 2020;18:100258. https://pmc.ncbi.nlm.nih.gov/articles/PMC6970160/ ↩︎ ↩︎ ↩︎ ↩︎
The Pros and Cons of Mesenchymal Stem Cell-Based Therapies. Cells. 2019;8(9):946. https://pmc.ncbi.nlm.nih.gov/articles/PMC6719501/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
U.S. FDA. Public Safety Notification on Exosome Products. 2019. https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/public-safety-notification-exosome-products ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Top Doctor Magazine. Exosome Therapy Regenerative Medicine Explained (2026). https://topdoctormagazine.com/news/exosome-therapy-regenerative-medicine-explained/ (Referencing FDA violations and reported adverse events) ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cell Communication and Signaling. A review on exosomes application in clinical trials: perspective, questions, and challenges. 2022;20(1):153. https://biosignaling.biomedcentral.com/articles/10.1186/s12964-022-00959-4 (Discusses safety and side effects, and unclear results of exosome therapy) ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sampson S, et al. Platelet-rich plasma: a review of current evidence and clinical applications. J Am Acad Orthop Surg. 2008;16(11):625-635. https://pubmed.ncbi.nlm.nih.gov/19001699/ (Review of PRP applications, safety, and general considerations) ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mokrzycki MH, Balogun RA. Therapeutic apheresis: a review of complications and management. Transfus Apher Sci. 2011;45(3):160–167. https://pubmed.ncbi.nlm.nih.gov/?term=Mokrzycki+Balogun+apheresis+complications+2011 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
J Allergy Clin Immunol. Intravenous immunoglobulin: adverse effects and safe administration. 2005;116(6):1340-1349. https://pubmed.ncbi.nlm.nih.gov/16391392/ ↩︎ ↩︎ ↩︎ ↩︎
Stem Cell News. The Dark Side of Exosomes: Risks, Unknowns & Future Potential. 2025. https://stemcell.news/2025/03/10/exosome-therapy-risks-and-side-effects/ (Discusses risk of unwanted effects and limited research on exosomes) ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Johns Hopkins Medicine. Platelet-Rich Plasma (PRP) Injections. https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/plateletrich-plasma-prp-treatment (Discusses PRP safety and side effects) ↩︎ ↩︎ ↩︎ ↩︎ ↩︎