¶ Coenzyme Q10 (CoQ10)
| Type | Vitamin-like compound, Antioxidant |
| Active Cmpd | Ubiquinone, Ubiquinol |
| Source | Endogenous synthesis, Dietary sources (meat, fish, nuts) |
| Dose Range | 100–300 mg daily |
| Half-life | ~33 hours |
| Main Benefit | Mitochondrial function, Antioxidant defense |
| Absorption | Low (lipid-soluble, requires fat for absorption) |
Coenzyme Q10 (CoQ10) is a crucial fat-soluble, vitamin-like compound integral to cellular energy production and antioxidant defense. Synthesized naturally by the body, its levels can decline with age or due to certain medications, such as statins.
¶ At a glance
Aliases
- Also known as: Ubiquinone, Ubiquinol
- Chemical / botanical name: 2,3-Dimethoxy-5-methyl-6-decaprenyl-1,4-benzoquinone
- Category: Lipid-soluble antioxidant, electron carrier
Key points (high-level summary)
- In heart failure with reduced ejection fraction, CoQ10 significantly improves symptoms and reduces cardiovascular events and mortality when used as an adjunctive therapy [1].
- CoQ10 supplementation may attenuate oxidative stress in adults and has shown mixed results in reducing statin-induced muscle pain [2][3].
- Bioavailability is a critical factor; CoQ10 is highly lipophilic and requires fat for optimal absorption [4].
- CoQ10 is generally well-tolerated, but individuals on warfarin should monitor their INR due to potential interactions [5].
What people use it for
- Main goals: Cardiovascular health, metabolic health, oxidative stress reduction, statin-associated myopathy, neurological support
- Evidence quality (overall): Moderate (due to strong evidence in specific conditions like heart failure, but limited or mixed evidence in others)
¶ What is Coenzyme Q10 (CoQ10)?
Coenzyme Q10 (CoQ10), also known as ubiquinone in its oxidized form and ubiquinol in its reduced form, is an endogenously synthesized, lipid-soluble compound vital for cellular function. It is a key component of the mitochondrial electron transport chain, where it facilitates ATP production, and acts as a powerful antioxidant, protecting cells from oxidative damage [2:1].
- Definition: A benzoquinone compound with a 10-isoprenoid side chain, functioning as an electron carrier in mitochondria and a potent antioxidant.
- Natural sources: Small amounts are found in fatty fish (salmon, tuna), organ meats (liver, kidney, heart), and whole grains.
- Traditional / historical use: CoQ10 has been studied for decades, particularly since its role in the electron transport chain was elucidated in the 1960s, leading to widespread clinical research.
- Current regulatory status: Dietary supplement in most regions.
- Key pharmacological property in one line: Mitochondrial bioenergetic and lipid-soluble antioxidant agent.
¶ What are Coenzyme Q10 (CoQ10)’s main benefits?
CoQ10 offers several potential health benefits, with the strongest evidence supporting its role in cardiovascular health and mitigating oxidative stress.
-
Heart Failure (Reduced Ejection Fraction)
- Direction of effect: Decrease (p)
- Magnitude: Large
- Population studied: Patients with moderate to severe chronic heart failure
- Evidence quality: High (meta-analyses of RCTs)
- Summary sentence: As an adjunctive therapy, CoQ10 significantly reduces major adverse cardiovascular events (MACE), cardiovascular mortality, and all-cause mortality in patients with chronic heart failure [1:1].
-
Statin-Associated Myopathy
- Direction of effect: Mixed/Unclear (x)
- Magnitude: Small to moderate
- Population studied: Statin-treated patients experiencing myopathy
- Evidence quality: Moderate (systematic reviews and meta-analyses with mixed results)
- Summary sentence: While statins deplete endogenous CoQ10, clinical trial results on CoQ10’s consistent ability to reduce statin-induced muscle pain are mixed, with some studies showing benefit and others not [3:1].
-
Oxidative Stress Reduction
- Direction of effect: Decrease (p)
- Magnitude: Moderate
- Population studied: Adults, particularly those with coronary artery disease or type 2 diabetes
- Evidence quality: Moderate (GRADE-assessed systematic review and meta-analysis of RCTs)
- Summary sentence: CoQ10 supplementation has been shown to significantly increase total antioxidant capacity (TAC) and reduce malondialdehyde (MDA) concentrations, indicating an attenuation of oxidative stress [2:2].
-
Glycemic Control
- Direction of effect: Decrease (p) / No consistent effect (x)
- Magnitude: Small (for HOMA-IR), No significant change (for FBG, insulin, HbA1c)
- Population studied: Patients with metabolic disorders, impaired glucose tolerance
- Evidence quality: Moderate (umbrella review of meta-analyses, randomized controlled trials)
- Summary sentence: CoQ10 supplementation may lead to a significant reduction in HOMA-IR in prediabetic patients but shows no significant impact on fasting blood glucose, insulin, or glycated hemoglobin levels [6]. In broader metabolic disorders, effects on glycemic markers are mixed [7].
-
Depressive Symptoms and Fatigue
- Direction of effect: Decrease (p)
- Magnitude: Small to moderate
- Population studied: Adults with depressive symptoms or fatigue
- Evidence quality: Moderate (systematic reviews and meta-analyses of RCTs)
- Summary sentence: Meta-analyses suggest that CoQ10 supplementation may modestly reduce depressive symptoms and fatigue [8][9].
-
Friedreich Ataxia
- Direction of effect: No consistent effect (x) / Unclear (x)
- Magnitude: No significant difference
- Population studied: Individuals with genetically-confirmed Friedreich ataxia
- Evidence quality: Moderate to very low (Cochrane review of RCTs)
- Summary sentence: Pharmacological treatments including CoQ10 probably make little or no difference to ataxia rating scale scores after 12 months, and evidence for other outcomes like interventricular septal thickness in diastole (IVSTd) or activities of daily living (ADL) is very uncertain [10].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Heart Failure (HFrEF) | High | High | 1 RCT (Q-SYMBIO) / Meta-analyses | 300 mg/day as adjunctive therapy in moderate-severe HFrEF [1:2] | |
| Statin-Associated Myopathy | Low | Moderate | Meta-analyses of RCTs | Mixed results on muscle pain/weakness reduction [3:2] | |
| Oxidative Stress (MDA) | High | Moderate | 34 RCTs | Significant reduction in malondialdehyde (MDA) [2:3] | |
| Oxidative Stress (TAC) | High | Moderate | 34 RCTs | Significant increase in total antioxidant capacity (TAC) [2:4] | |
| Glycemic Control (HOMA-IR) | Low | Moderate | RCTs / Umbrella review | Significant reduction in HOMA-IR in prediabetes, but mixed overall [6:1][7:1] | |
| Fasting Blood Glucose | High | High | RCTs / Umbrella review | No significant changes observed [6:2][7:2] | |
| Depressive Symptoms | Moderate | Moderate | Meta-analyses of RCTs | Modest reduction in symptoms [8:1][9:1] | |
| Fatigue | Moderate | Moderate | Meta-analyses of RCTs | Modest reduction in fatigue [8:2] | |
| Parkinson's Disease Progression | High | High | RCTs | No clinical benefit in slowing functional decline [11] | |
| Friedreich Ataxia | Low | Very Low | Cochrane review of RCTs | Little or no difference on ataxia rating scale [10:1] |
*Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
**Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
REQUIRED: You MUST include a citation key (e.g. [^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
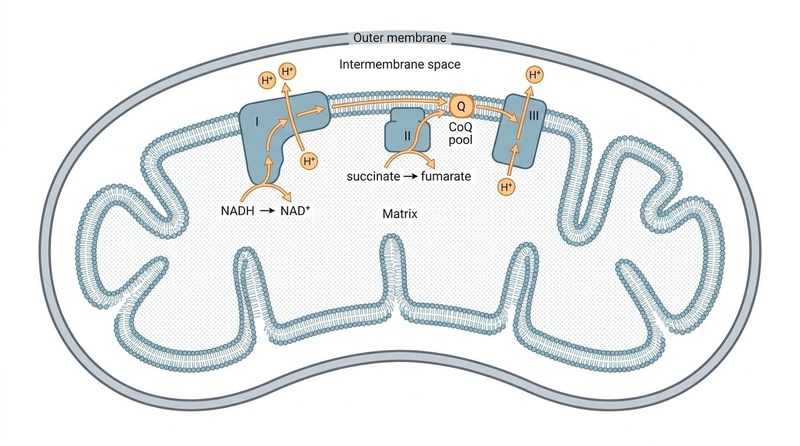
¶ How does Coenzyme Q10 (CoQ10) work?
CoQ10 functions primarily in the inner mitochondrial membrane, playing a dual role in cellular energy production and antioxidant defense.
- Primary targets: Electron transport chain complexes (I, II, III), reactive oxygen species (ROS).
- Core mechanisms:
- Oxidative Phosphorylation: CoQ10 acts as a mobile electron shuttle, accepting electrons from Complex I (NADH dehydrogenase) and Complex II (succinate dehydrogenase) and transferring them to Complex III (cytochrome bc1 complex). This electron transfer is coupled with proton pumping across the inner mitochondrial membrane, generating the proton-motive force essential for ATP synthesis by ATP synthase.
- Antioxidant Defense: In its reduced form (ubiquinol), CoQ10 is a potent lipid-soluble antioxidant. It directly neutralizes free radicals, preventing lipid peroxidation in cell membranes and protecting circulating low-density lipoproteins (LDL) from oxidative damage, a critical step in atherosclerosis.
- Evidence source: Extensive biochemical, cellular, and animal studies, supported by human biomarker data.
- Human data (if any): Supplementation increases circulating CoQ10 levels and markers of antioxidant capacity, such as total antioxidant capacity (TAC) and reduced malondialdehyde (MDA) [2:5].
- Animal / in vitro data: Numerous studies demonstrate CoQ10's role in mitigating oxidative stress and preserving mitochondrial function in various disease models.
- Pharmacokinetics basics: CoQ10 is poorly water-soluble and has a large molecular weight, leading to low oral bioavailability in raw powder form. Absorption is significantly enhanced when taken with fat or in specialized lipid-based formulations. It is metabolized in the liver and has a relatively long elimination half-life of approximately 33 hours, allowing for once-daily dosing [4:1].
¶ Effects on different systems
¶ Metabolic health (glucose, insulin, lipids)
CoQ10 has been studied for its potential effects on various metabolic markers, particularly in individuals with prediabetes or metabolic disorders. While it may reduce insulin resistance as measured by HOMA-IR, its impact on fasting blood glucose, insulin, and glycated hemoglobin levels is not consistently significant [6:3]. For lipid markers, some meta-analyses suggest potential benefits in reducing total cholesterol and LDL-cholesterol, but these effects can be inconsistent depending on the population and study design [7:3].
¶ Cardiovascular health (blood pressure, vascular markers)
The most robust evidence for CoQ10 is in cardiovascular health, particularly in heart failure with reduced ejection fraction. It significantly improves symptoms and reduces mortality in these patients [1:3]. Beyond heart failure, CoQ10's antioxidant properties may contribute to vascular health by protecting against oxidative stress and improving endothelial function, though direct clinical outcomes on blood pressure or hard cardiovascular events in healthy individuals are less clear. It has also shown cardioprotective effects in animal models of ischemia-reperfusion injury by decreasing apoptotic cell death and regulating gene expression [1:4].
¶ Brain & mental health (cognition, mood, sleep)
Research indicates that CoQ10 supplementation may offer some benefits for mood and fatigue. Meta-analyses have reported modest reductions in depressive symptoms and fatigue in adults [8:3][9:2]. However, high-dose CoQ10 has not shown a benefit in slowing the progression of early Parkinson's disease [11:1], suggesting its role in neurodegenerative conditions might be limited or specific.
¶ Other domains
CoQ10 is crucial for overall cellular health due to its mitochondrial and antioxidant roles. It is also explored in fertility protocols to support oocyte and sperm quality due to the high energy demands of reproductive cells.
¶ Dosage and how to take it
¶ Standard dosing in studies
- Typical daily dose range: 100–300 mg daily for general health or cardiovascular support; higher doses (up to 1,200 mg/day) have been used in some clinical trials for specific conditions.
- Common dosing schedules: Often taken once daily, preferably with a meal. Some studies utilize split doses (e.g., 100 mg three times daily) for higher total daily intakes.
- Study durations: Typically ranges from 8 weeks to several months, with heart failure trials extending over two years.
¶ Forms and bioavailability
- Common forms: Ubiquinone (oxidized form) and Ubiquinol (reduced form). Both forms are interconverted in the body.
- Relative differences, if known: While ubiquinol is often marketed as "more active" or "more bioavailable," studies show that the formulation (e.g., solubilization in a lipid matrix) is a far more critical determinant of absorption than the redox state. Well-formulated ubiquinone can be just as effective and cost-efficient [4:2].
- With or without food: Always take CoQ10 with a meal containing fats to maximize absorption, regardless of the form. Dry powder capsules are not recommended due to extremely poor bioavailability.
¶ Special populations
- Dose considerations or lack of data in:
- Kidney or liver impairment: Data is limited; caution is advised, and physician consultation is recommended.
- Older adults: Endogenous CoQ10 levels decline with age, making supplementation potentially more beneficial, with standard adult doses generally applied.
- Children and adolescents: Limited data; use under medical supervision for specific conditions.
- Pregnancy and breastfeeding: Insufficient safety data; generally not recommended unless specifically advised by a healthcare provider.
¶ Safety and side effects
CoQ10 is generally considered safe and well-tolerated, even at higher doses.
¶ Common side effects
- Very rare (<1% of users): May include mild gastrointestinal upset, nausea, diarrhea, or loss of appetite.
- Frequency and dose-relationship where reported: Side effects are generally mild and transient, not typically dose-dependent within common ranges.
¶ Less common / serious concerns
- No serious adverse effects or organ toxicities have been consistently reported in clinical trials, even with doses up to 2,400 mg/day in certain neurodegenerative conditions.
¶ Who should be especially cautious or avoid it
- Patients on Warfarin (Coumadin): CoQ10 shares structural similarities with Vitamin K, which can interfere with the anticoagulant effect of warfarin, potentially decreasing INR. Close monitoring of INR is crucial if CoQ10 is initiated in these patients [5:1].
- Pregnant or breastfeeding individuals: Due to insufficient safety data.
¶ Drug and supplement interactions
¶ Pharmacokinetic interactions (how drugs are processed)
- No major interactions with CYP450 enzymes or P-glycoprotein have been consistently established for CoQ10 at typical supplemental doses.
- Drugs likely impacted: CoQ10 may influence the effects of warfarin (see "Safety and side effects").
- Direction of interaction: Decreased effectiveness of warfarin.
¶ Pharmacodynamic interactions (additive / opposing effects)
- Statins: Statins (HMG-CoA reductase inhibitors) deplete endogenous CoQ10 levels, making co-administration of CoQ10 a biologically rational strategy to potentially mitigate side effects, rather than an interaction risk.
- Blood pressure medications: CoQ10 may have mild blood pressure-lowering effects; caution and monitoring are advised if taken with antihypertensive drugs to avoid excessive blood pressure reduction.
- Chemotherapy drugs: Some evidence suggests CoQ10 may interfere with certain chemotherapy agents (e.g., doxorubicin). Patients undergoing chemotherapy should consult their oncologist before taking CoQ10.
¶ Combining Coenzyme Q10 (CoQ10) with other supplements (“stacks”)
- Common combos: CoQ10 is frequently combined with omega-3 fatty acids for cardiovascular health, or with other mitochondrial support compounds like PQQ or Alpha-Lipoic Acid.
- Rationale: Mechanistic complementarity; omega-3s and CoQ10 both support heart health, while other mitochondrial compounds can synergistically enhance cellular energy production and antioxidant defense.
- Evidence level: Most common combinations are based on theoretical synergy and mechanistic reasoning, with limited formal combination trials.
¶ Practical questions (FAQ)
-
How long does it take for CoQ10 to work?
Clinical benefits, particularly in cardiovascular conditions, often become apparent after several weeks to months of consistent supplementation (e.g., 2-3 months for heart failure symptoms). For antioxidant effects or statin-myopathy, some individuals report improvements within a few weeks. -
Can I take CoQ10 long term?
Yes, CoQ10 is generally considered safe for long-term use. Many clinical trials, especially for heart failure and neurodegenerative diseases, have involved continuous supplementation for one to two years or more without significant safety concerns. -
Can I take CoQ10 with statins?
Yes, it is common and often recommended to take CoQ10 with statins, as statins can deplete the body's natural CoQ10 levels. However, the evidence for CoQ10 definitively preventing or resolving statin-induced muscle pain is mixed. -
Is CoQ10 useful if I am otherwise healthy?
While the strongest evidence for CoQ10 is in specific disease states (e.g., heart failure), its role in mitochondrial function and antioxidant defense suggests potential benefits for general cellular health and healthy aging. However, large-scale studies demonstrating significant clinical outcomes in otherwise healthy individuals are limited. -
Does CoQ10 help with weight loss / energy / longevity?
CoQ10's direct impact on weight loss is not well-supported by robust clinical evidence. Its role in energy production may indirectly contribute to perceived energy levels, especially in conditions characterized by mitochondrial dysfunction. While its antioxidant properties align with longevity theories, direct evidence of CoQ10 extending human lifespan is currently lacking.
¶ How we evaluated the evidence
Our evaluation of CoQ10’s efficacy and safety is based on a hierarchical review of scientific literature, prioritizing the highest quality human evidence. A full list of vetted clinical papers, trials, and systematic reviews is compiled in the Coenzyme Q10 (CoQ10) Source Manifest.
- Study types prioritized: We primarily relied on systematic reviews, meta-analyses of randomized controlled trials (RCTs), and individual high-quality RCTs. Observational studies, case reports, and animal/in vitro data were considered for mechanistic understanding or when human trial data was sparse, but their findings were weighted lower for clinical claims.
- How we graded evidence quality: We used a modified GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach:
- High: Multiple high-quality RCTs or meta-analyses with consistent results, low risk of bias, and adequate sample sizes.
- Moderate: Some RCTs with minor limitations, or mixed but generally consistent results from otherwise high-quality studies.
- Low: Few RCTs, significant limitations in study design, small sample sizes, or inconsistent results.
- Very low: Primarily observational studies, case reports, or animal/in vitro data; or serious methodological flaws in available human trials.
- Sample size, risk of bias, consistency, directness, effect size: These factors were critically assessed for each outcome to determine the overall strength and applicability of the evidence.
- Clinical relevance: We focused on whether reported effects were not only statistically significant but also clinically meaningful for patient outcomes.
- Updating policy: This page is updated regularly, especially when new meta-analyses, large-scale RCTs, or significant clinical guidelines related to CoQ10 are published.
¶ References
Mortensen SA, Rosenfeldt F, Kumar A, et al. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: results from Q-SYMBIO: a randomized double-blind trial. JACC Heart Fail. 2014. https://www.jacc.org/doi/10.1016/j.jchf.2014.06.008 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhang Y, He Y, Ma M. Effects of Coenzyme Q10 Supplementation on Biomarkers of Oxidative Stress in Adults: A GRADE-Assessed Systematic Review and Updated Meta-Analysis of Randomized Controlled Trials. The Journal of international medical research. 2026. https://pubmed.ncbi.nlm.nih.gov/41657017/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kovacic S, Habicht SD, Eckert GP. Effects of coenzyme Q10 supplementation on myopathy in statin-treated patients: a systematic review and meta-analysis. Journal of nutritional science. 2025. https://pubmed.ncbi.nlm.nih.gov/41158831/ ↩︎ ↩︎ ↩︎
López-Lluch G, Del Pozo-Cruz J, Sánchez-Cuesta A, et al. Bioavailability of coenzyme Q10 supplements depends on carrier lipids and solubilization. Nutrition. 2019. https://pubmed.ncbi.nlm.nih.gov/30153575/ ↩︎ ↩︎ ↩︎
Sood B, Keenaghan M. Coenzyme Q10. StatPearls. 2022. https://www.ncbi.nlm.nih.gov/books/NBK531491/ ↩︎ ↩︎
Musazadeh V, Falahatzadeh M, Mahmoudinezhad M. Effects of Coenzyme Q10 Supplementation on Glycemic Control Biomarkers: An Umbrella Review of Meta-Analyses of Randomised Controlled Trials. Endocrinology, diabetes & metabolism. 2026. https://pubmed.ncbi.nlm.nih.gov/41859772/ ↩︎ ↩︎ ↩︎ ↩︎
Zhang Z, Liu Z, Geng Y. Effects of Coenzyme Q10 on Lipid, Glycemic, and Inflammatory Markers in Metabolic Disorders: A Systematic Review and Meta-Analysis. Journal of diabetes research. 2026. https://pubmed.ncbi.nlm.nih.gov/42192187/ ↩︎ ↩︎ ↩︎ ↩︎
Magalhães PLM, da Silva AMP, Maximiano MLB. Effects of Coenzyme Q10 Supplementation on Depressive Symptoms and Fatigue: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of clinical psychopharmacology. 2026. https://pubmed.ncbi.nlm.nih.gov/41294251/ ↩︎ ↩︎ ↩︎ ↩︎
Akwan R, Elsharkawy MM, Zrineh A. The effect of coenzyme Q10 supplementation on depressive symptoms and anxiety: a systematic review and meta-analysis of randomized controlled trials. European journal of clinical pharmacology. 2025. https://pubmed.ncbi.nlm.nih.gov/40833470/ ↩︎ ↩︎ ↩︎
Lyons S, Kearney M, Fahey MC. Pharmacological treatments for Friedreich ataxia. The Cochrane database of systematic reviews. 2026. https://pubmed.ncbi.nlm.nih.gov/42117563/ ↩︎ ↩︎
The Parkinson Study Group QE3 Investigators. A randomized clinical trial of high-dosage coenzyme Q10 in early Parkinson disease: no evidence of benefit. JAMA Neurol. 2014. https://pubmed.ncbi.nlm.nih.gov/24664227/ ↩︎ ↩︎