¶ Glutathione
Glutathione (GSH) is an endogenous tripeptide, often called the "master antioxidant," composed of glutamic acid, cysteine, and glycine. Crucial for cellular defense, immune modulation, and liver detoxification, it is synthesized in almost all cells [1][2]. Despite its natural presence in foods, direct oral supplementation historically faced poor absorption. However, advancements in delivery, like liposomal encapsulation and precursors such as N-Acetylcysteine (NAC), have significantly enhanced its therapeutic potential [2:1][3]. Glutathione plays a vital role in protecting against oxidative stress, reducing liver enzymes in conditions like NAFLD, and supporting immune function.
| Type | Endogenous Tripeptide |
| Active Cmpd | Reduced L-Glutathione (GSH) |
| Source | Endogenous synthesis; Diet (asparagus, avocado, meats) |
| Dose Range | 250–1,000 mg/day (Oral/Liposomal) |
| Half-life | ~1.5–15 minutes (Plasma) |
| Main Benefit | Antioxidant defense, Liver health, Skin texture |
| Absorption | Low (Standard oral); High (Liposomal) |
¶ At a glance
Aliases
- Also known as: GSH (Reduced Glutathione), GSSG (Oxidized Glutathione), Master Antioxidant.
- Chemical / botanical name: γ-L-Glutamyl-L-cysteinylglycine.
- Category: Endogenous tripeptide / Amino acid derivative.
Key points (high-level summary)
- Endogenous Redox Buffer: Glutathione is the primary regulator of cellular redox status, neutralizing reactive oxygen species (ROS) and recycling other antioxidants like Vitamin C and E [2:2][4].
- Bioavailability Breakthroughs: While standard oral glutathione was long considered poorly absorbed, 6-month randomized trials confirm it can effectively raise body stores; liposomal forms offer more rapid uptake [2:3][3:1].
- Therapeutic Applications: Clinical evidence supports its use in reducing liver enzymes in NAFLD, improving markers in chronic cardiometabolic diseases, and providing modest cosmetic skin-lightening effects [1:1][5][6].
- Precursor Synergy: Supplementing with NAC or a combination of NAC and Glycine (GlyNAC) remains a highly effective strategy to support intracellular glutathione synthesis [7][8].
What people use it for
- Main goals: Oxidative stress reduction, liver detoxification, skin lightening, immune support, neuroprotection in Parkinson's disease.
- Evidence quality (overall): Moderate (High for systemic store replenishment, Moderate for liver health and immune function, Low/Mixed for neuroprotection and cosmetic whitening).
¶ What is Glutathione?
Glutathione is a low-molecular-weight tripeptide found in high concentrations (up to 10 mM) in almost all human cells. It is not considered an "essential" nutrient because the body can synthesize it from the amino acids L-glutamate, L-cysteine, and glycine.
- Definition: A sulfur-containing tripeptide that acts as a potent electron donor to stabilize free radicals.
- Natural sources: Abundant in cruciferous vegetables (broccoli, cabbage), fruits (avocado, orange), and meats. However, dietary glutathione contributes minimally to systemic levels due to digestion [2:4].
- Traditional / historical use: Its discovery in the late 19th century led to decades of research into its role in cellular respiration and protection against radiation and toxic chemicals.
- Current regulatory status: Available as a dietary supplement in most jurisdictions (USA, EU). In some countries, intravenous glutathione is a regulated medical treatment for chemotherapy adjunct or specific poisoning.
- Key pharmacological property: The primary endogenous intracellular antioxidant and redox buffer.
¶ What are Glutathione's main benefits?
Glutathione's benefits stem from its role in maintaining cellular health and protecting tissue from chronic oxidative damage.
- Liver Health (NAFLD/NASH):
- Immune Resilience:
- Outcome: Increased Natural Killer (NK) cell activity and lymphocyte proliferation.
- Direction: Increase.
- Magnitude: Large (with liposomal delivery).
- Evidence quality: Moderate; trials demonstrate that liposomal glutathione rapidly restores immune markers in both healthy and immunocompromised (diabetic) populations [3:2][10].
- Oxidative Stress & Aging:
- Cosmetic Skin Lightening:
¶ Evidence summary table
| Outcome / Goal | Effect | Consistency | Evidence quality | Trials | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Systemic GSH Stores | High | High | 10+ RCTs | 250–1,000 mg standard or 500–1,000 mg liposomal daily for 1–6 months [2:6][3:3] | |
| Liver Enzymes (ALT/AST) | Moderate | Moderate | 5 RCTs | 300–1,000 mg/day in NAFLD patients; improves liver function markers [1:3][9:1] | |
| NK Cell Activity | High | Moderate | 2 RCTs | Significant immune enhancement observed with 500–1,000 mg/day liposomal forms [3:4] | |
| Skin Hyperpigmentation | Moderate | Low | 6 RCTs | Oral and topical forms show modest reduction in melanin index [6:2][11:1] | |
| Parkinson's Motor Symptoms | Mixed | Low | 4 RCTs | Mixed results; improves biomarkers but motor symptom efficacy is unclear [8:1][7:1] | |
| Periodontal Inflammation | Moderate | Moderate | 1 SR | Restoration of local glutathione levels improves periodontal outcomes [12] |
Effect: u=up, d=down, 1-3=magnitude, p=positive impact, n=negative, x=neutral. SR=Systematic Review.
Mechanisms
Glutathione's primary mechanism is its ability to donate electrons to unstable reactive species, effectively "quenching" oxidative fire before it damages DNA or proteins.
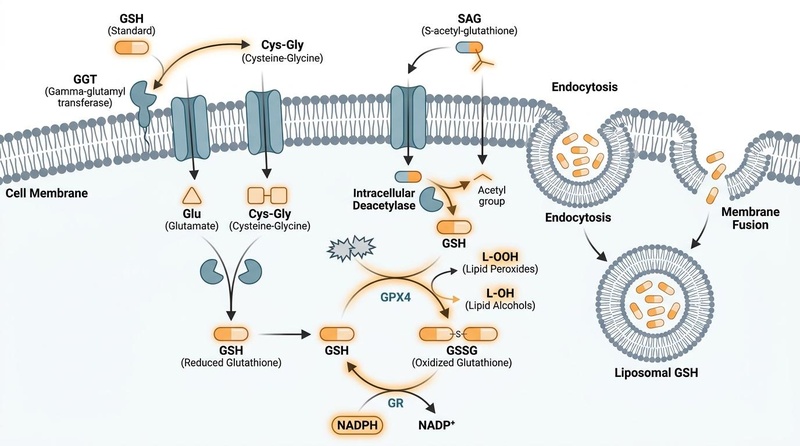
¶ The Glutathione Redox Cycle
The body maintains a high ratio of reduced glutathione (GSH) to oxidized glutathione (GSSG). When GSH neutralizes a free radical (like hydrogen peroxide), it becomes oxidized into GSSG. The enzyme Glutathione Reductase (GR) then uses NADPH to recycle GSSG back into the active GSH form [2:7][13].
¶ Phase II Detoxification
In the liver, Glutathione S-transferases (GSTs) catalyze the conjugation of GSH with diverse electrophilic compounds, including environmental toxins, heavy metals, and drugs (e.g., acetaminophen). This conjugation makes the toxins water-soluble, allowing for excretion via bile or urine [1:4][14].
¶ Ferroptosis Inhibition
Recent research has identified the System Xc-/GSH/GPX4 axis as a critical regulator of ferroptosis—a form of regulated cell death driven by iron-dependent lipid peroxidation. Glutathione is essential for the function of Glutathione Peroxidase 4 (GPX4), which prevents the lethal accumulation of lipid peroxides [15].
¶ Bioavailability and Transport
Glutathione is hydrolyzed by the enzyme gamma-glutamyl transpeptidase (GGT) on cell surfaces. While traditional oral GSH was thought to be entirely destroyed, data now suggest that a portion is absorbed intact via specific peptide transporters or reconstructed intracellularly after absorption of its constituent amino acids [2:8]. Liposomal delivery systems bypass this degradation by shielding the tripeptide in a lipid bilayer [3:5].
¶ System-specific effects
¶ Metabolic & Cardiovascular Health
Glutathione levels are frequently depleted in patients with Type 2 Diabetes due to chronic oxidative stress. Supplementation (especially in liposomal or precursor forms) has been shown to improve redox markers and may support cardiometabolic resilience [5:2][10:1].
¶ Brain & Mental Health
Depletion of glutathione in the substantia nigra is a hallmark of Parkinson's Disease (PD). While clinical trials of oral and IV glutathione show improvements in oxidative biomarkers, clinical motor benefits have been inconsistent, likely due to difficulties in crossing the blood-brain barrier [8:2][7:2].
¶ Dermatology
Topical and oral glutathione inhibit tyrosinase, the rate-limiting enzyme in melanin synthesis. Systematic reviews confirm that while glutathione can lighten skin and improve texture, the effects are modest compared to stronger bleaching agents and require consistent use [6:3][11:2].
¶ Athletic Performance
Glutathione works synergistically with Vitamin C to reduce lipid peroxidation during intense exercise. Trials in athletes suggest that glutathione may help lower blood lactate levels and improve muscle fatigue markers when taken pre-exercise [4:1].
¶ Dosage
Standard dosing in studies
- Standard Oral GSH: 250 mg to 1,000 mg daily. High-quality trials (Richie 2015) used these doses over a 6-month period to achieve significant tissue store increases [2:9].
- Liposomal Oral GSH: 500 mg to 1,000 mg daily. Often preferred for more rapid restoration of immune markers [3:6].
- Topical: 2% glutathione creams applied twice daily for skin-lightening purposes [11:3].
Forms and bioavailability
- Liposomal: Superior cellular uptake; highly recommended for clinical goals requiring rapid antioxidant restoration.
- Acetyl-Glutathione (S-Acetyl-L-Glutathione): A stable form thought to resist degradation and improve cellular delivery, though human RCT data is less abundant than standard/liposomal forms.
- NAC as a Precursor: N-Acetylcysteine (600–1,800 mg/day) provides the rate-limiting cysteine and is often more cost-effective for long-term glutathione support [8:3][7:3].
Special populations
- Diabetes: May require higher doses (up to 1,000 mg) to overcome chronic depletion [10:2].
- Asthma: Inhaled glutathione is contraindicated (see Safety) [16].
¶ Safety
Common side effects
- Gastrointestinal: Mild bloating, cramping, or loose stools have been reported at doses exceeding 1,000 mg/day [2:10][16:1].
- Skin: Rare cases of skin rashes have occurred with topical or high-dose oral use [11:4].
Less common / serious concerns
- Zinc Depletion: Long-term, high-dose glutathione use has been theoretically associated with reduced zinc levels, though this is not consistently seen in short-term human trials.
- IV Risks: Unregulated intravenous "skin bleaching" clinics have been linked to severe adverse reactions, including anaphylaxis, hepatotoxicity, and Stevens-Johnson syndrome [17][6:4].
Who should be especially cautious
- Asthmatics: Inhaled or nebulized glutathione can trigger severe bronchospasm and is strictly contraindicated [16:2].
- Chemotherapy Patients: Because glutathione is a potent antioxidant, there is a theoretical concern it could interfere with the efficacy of ROS-dependent chemotherapy drugs. Consult an oncologist before use [18].
¶ Interactions
Pharmacokinetic interactions
- Phase II Enzymes: Glutathione is a substrate for Glutathione S-transferases (GSTs). It may theoretically alter the clearance of drugs metabolized via this pathway (e.g., acetaminophen, certain chemotherapy agents) [1:5][14:1].
Pharmacodynamic interactions
- Alcohol: Chronic ethanol consumption severely depletes liver glutathione, increasing the risk of toxicity from other substances [1:6].
- Antioxidant Synergy: Glutathione interacts positively with Vitamin C, Vitamin E, and Alpha-Lipoic Acid, forming a "redox network" where these molecules recycle each other [4:2].
¶ Stacks
- The GlyNAC Stack: A combination of NAC (N-Acetylcysteine) and Glycine. This stack provides the two most critical building blocks for endogenous synthesis and has been studied for its anti-aging and mitochondrial benefits.
- Redox Synergy Stack: Combining Glutathione (or NAC) with Vitamin C (500mg) and Alpha-Lipoic Acid (300mg) to maximize the recycling and duration of antioxidant activity [4:3].
- Liver Support Stack: Glutathione paired with Milk Thistle (Silymarin) and Selenium (a cofactor for glutathione peroxidase) [1:7].
¶ FAQ
How long does it take for glutathione to work?
Is oral glutathione actually absorbed?
Can I take glutathione with my medication?
Glutathione is generally safe, but it may interact with ROS-dependent chemotherapy and drugs metabolized by GST enzymes. Always consult a healthcare provider [18:1].
Which is better: Glutathione or NAC?
¶ How we evaluated evidence
We prioritized systematic reviews and randomized controlled trials (RCTs) found via PubMed and the Cochrane Library. Evidence magnitude was graded based on statistically significant changes in human biomarkers (e.g., ALT, MDA, GSH stores) and clinical outcomes.
- High: Multiple RCTs or Meta-analyses with consistent results (e.g., store replenishment).
- Moderate: Solid clinical data with minor inconsistencies or smaller sample sizes (e.g., NAFLD markers).
- Low: Based on narrative reviews, small pilots, or highly variable outcomes (e.g., cosmetic whitening, Parkinson's symptoms).
¶ References
Santacroce G, et al. (2023). Glutathione: Pharmacological aspects and implications for clinical use in non-alcoholic fatty liver disease. Frontiers in Medicine. https://pubmed.ncbi.nlm.nih.gov/37035339/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Richie JP Jr, et al. (2015). Randomized controlled trial of oral glutathione supplementation on body stores of glutathione. European Journal of Nutrition. https://pubmed.ncbi.nlm.nih.gov/24791752/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sinha R, et al. (2018). Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. European Journal of Clinical Nutrition. https://pubmed.ncbi.nlm.nih.gov/28853742/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lee E, et al. (2023). Vitamin C and glutathione supplementation: a review of their additive effects on exercise performance. Physical Activity and Nutrition. https://pubmed.ncbi.nlm.nih.gov/37946445/ ↩︎ ↩︎ ↩︎ ↩︎
Dludla PV, et al. (2023). Dietary Supplements Potentially Target Plasma Glutathione Levels to Improve Cardiometabolic Health in Patients with Diabetes Mellitus: A Systematic Review of Randomized Clinical Trials. Nutrients. https://pubmed.ncbi.nlm.nih.gov/36839303/ ↩︎ ↩︎ ↩︎
Sarkar R, Yadav V, Yadav T. (2025). Glutathione as a skin-lightening agent and in melasma: a systematic review. International Journal of Dermatology. https://pubmed.ncbi.nlm.nih.gov/39444151/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mohammed I, et al. (2026). The role of N-acetylcysteine and glutathione in the management of Parkinson's disease: a systematic review. Amino Acids. https://pubmed.ncbi.nlm.nih.gov/41874704/ ↩︎ ↩︎ ↩︎ ↩︎
Wang HL, Zhang J, Li YP. (2021). Potential use of glutathione as a treatment for Parkinson's disease. Experimental and Therapeutic Medicine. https://pubmed.ncbi.nlm.nih.gov/33376507/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nabipur L, et al. (2025). Additive Effects of Glutathione in Improving Antibiotic Efficacy in HIV-M.tb Co-Infection. Viruses. https://pubmed.ncbi.nlm.nih.gov/39861915/ ↩︎ ↩︎
To K, et al. (2021). Effects of Oral Liposomal Glutathione in Altering the Immune Responses in Individuals With Type 2 Diabetes. Frontiers in Cellular and Infection Microbiology. https://pubmed.ncbi.nlm.nih.gov/34150674/ ↩︎ ↩︎ ↩︎
Khanna R, et al. (2025). Systematic Review of the Efficacy and Safety of Topical Glutathione in Dermatology. J Clin Aesthet Dermatol. https://pubmed.ncbi.nlm.nih.gov/41416233/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mohideen K, et al. (2024). Assessment of glutathione... in patients with periodontitis-A systematic review and meta-analysis. Clin Exp Dent Res. https://pubmed.ncbi.nlm.nih.gov/38881240/ ↩︎
Katsev BD, Lee R, Kim JH. (2026). Space Radiation Effects on the Glutathione Redox Cycle and Cataract Formation. Aerospace Medicine and Human Performance. https://pubmed.ncbi.nlm.nih.gov/42044894/ ↩︎
Ezuruike UF, Prieto JM. (2014). The use of plants in the traditional management of diabetes in Nigeria. Journal of Ethnopharmacology. https://pubmed.ncbi.nlm.nih.gov/24929108/ ↩︎ ↩︎
Yi L, et al. (2026). Research Progress In Acupuncture For Parkinson's Disease: Insights Into The Mitochondrial Ferroptosis Pathway. Journal of Visualized Experiments. https://pubmed.ncbi.nlm.nih.gov/42371862/ ↩︎
Drugs.com. (2024). Glutathione Uses, Benefits & Dosage. https://www.drugs.com/npp/glutathione.html ↩︎ ↩︎ ↩︎
Alzahrani TF, et al. (2025). Exploring the Safety and Efficacy of Glutathione Supplementation for Skin Lightening: A Narrative Review. Cureus. https://pubmed.ncbi.nlm.nih.gov/40013212/ ↩︎
Morales-Borges RH, et al. (2022). N-Acetyl Cysteine and Glutathione in Health and Cancer: Hypothesis and Review. Alternative Therapies in Health and Medicine. https://pubmed.ncbi.nlm.nih.gov/33373322/ ↩︎ ↩︎