| Type | Essential Mineral / Trace Element |
| Active Form | Ferrous (Fe2+), Ferric (Fe3+) |
| Source | Red Meat, Poultry, Fish (Heme); Legumes, Spinach (Non-Heme) |
| Dose Range | 15–25 mg (prophylactic); 50–100 mg (therapeutic) |
| Main Benefit | Hemoglobin synthesis, fatigue reduction, cognitive well-being |
| Absorption | Enhanced by Vitamin C; Inhibited by Calcium, Phytates, Polyphenols |
¶ Iron
¶ At a Glance
Iron is an essential dietary mineral required for the synthesis of hemoglobin (which transports oxygen in the blood) and myoglobin (which provides oxygen to muscles). While dietary iron comes in two forms—heme (from animal products) and non-heme (from plants)—supplemental iron is exclusively non-heme. It is widely used to prevent and treat iron deficiency anemia (IDA) and non-anemic iron deficiency, a common cause of unexplained fatigue, poor exercise recovery, and brain fog, especially in menstruating women and endurance athletes.
¶ Safety & Warnings
Traffic Light: YELLOW
- Hemochromatosis Warning: Individuals with hereditary hemochromatosis or other iron-overload disorders must strictly avoid iron supplementation, as excess iron accumulates in organs (liver, heart, pancreas) leading to severe toxicity and organ failure [1].
- Toxicity Risk: Iron is toxic in high doses. Accidental overdose of iron-containing products is a leading cause of fatal poisoning in children under 6. Keep all iron supplements out of reach of children [1:1].
- Pro-Ox-Dant Nature: Free un-bound iron acts as a strong pro-oxidant, generating harmful free radicals via the Fenton reaction. Only supplement if a deficiency is confirmed via blood tests (ferritin, iron saturation).
¶ Protocol Card
- Therapeutic Dosage: 50–100 mg of elemental iron daily or every other day, depending on the severity of deficiency and medical guidance [2].
- Prophylactic/Maintenance Dosage: 15–25 mg of elemental iron daily (often found in multivitamins) [3].
- Preferred Forms:
- Administration Rules:
- Take on an empty stomach: Ideally 1 hour before or 2 hours after meals for maximum absorption.
- Synergy: Pair with 250–500 mg of Vitamin C (ascorbic acid) to enhance absorption [4:1].
- Inhibitors (Avoid): Do not take within 2 hours of dairy (calcium), coffee/tea (tannins), high-fiber foods (phytates), or antacids/PPIs, as these drastically reduce absorption [4:2].
- Alternate-Day Dosing: Recent guidelines suggest taking iron every other day (rather than daily) maximizes fractional absorption by avoiding spikes in hepcidin, the hormone that blocks iron uptake [2:1].
¶ Bottom Line
For individuals with confirmed iron deficiency or anemia, iron supplementation is a highly effective, restorative intervention that rapidly reverses fatigue, improves exercise capacity, and restores cognitive function. However, because excess iron is toxic and accelerates oxidative aging, it should never be taken "just in case" without biomarker confirmation.
¶ The "Why": Benefits & Outcomes
¶ Reversing Unexplained Fatigue and Brain Fog
The most immediate and noticeable benefit of restoring iron levels is the resolution of chronic fatigue and cognitive sluggishness. Iron is a non-negotiable cofactor in the mitochondrial electron transport chain (specifically cytochromes) necessary for ATP (energy) production. Even in the absence of clinical anemia (normal hemoglobin but low ferritin), iron deficiency causes profound physical and mental fatigue. Supplementation in non-anemic iron-deficient adults has been shown in randomized trials to significantly reduce fatigue scores and improve subjective well-being [5].
¶ Athletic Performance and Oxygen Delivery
Iron dictates the body's ability to transport and utilize oxygen. Depleted iron stores throttle VO2 max and muscular endurance, as myoglobin cannot adequately supply oxygen to working muscles. Endurance athletes (particularly female runners) are highly susceptible to "foot-strike hemolysis" and sweat-induced iron loss. Restoring ferritin levels above 30-50 ng/mL often yields rapid improvements in aerobic capacity and recovery metrics [6].
¶ Hair Growth and Restless Leg Syndrome
Iron is a critical cofactor for ribonucleotide reductase, an enzyme required for DNA synthesis in rapidly dividing cells like hair follicles. Chronic diffuse hair loss (telogen effluvium) is frequently linked to sub-optimal ferritin (<50 ng/mL) [7], making iron level restoration vital for maintaining hair quality. Additionally, iron deficiency in the brain alters dopamine signaling, making it the primary reversible cause of Restless Legs Syndrome (RLS). Supplementation frequently resolves nighttime leg twitching and associated insomnia [8].
¶ Reality Check: Bioavailability & GI Distress
The defining challenge of iron supplementation is not efficacy, but tolerability. The human body tightly regulates iron absorption because it lacks an active excretion pathway.
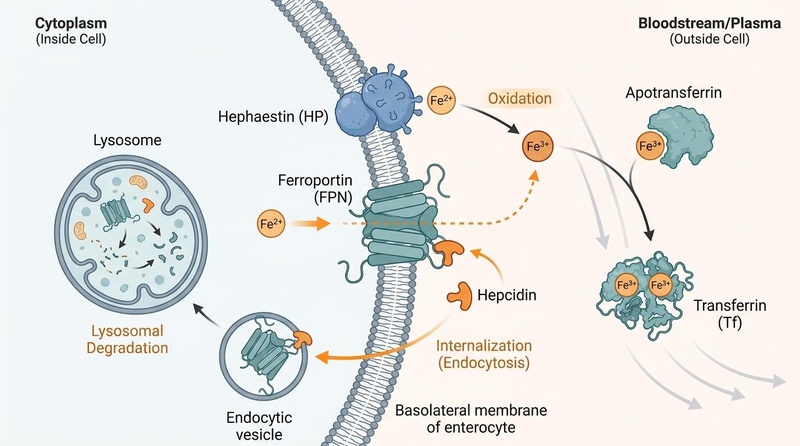
The Hepcidin Blockade: When you consume a high dose of iron, the liver releases hepcidin, a hormone that essentially shuts the "doors" of the gut lining for 24-48 hours to prevent iron overload. Taking iron multiple times a day often just causes the unabsorbed iron to sit in the gut, where it feeds pathogenic bacteria and causes severe constipation, black stools, and cramping [2:2]. This is why the modern protocol emphasizes alternate-day dosing, which bypasses the hepcidin block and dramatically improves both absorption and tolerability [2:3].
Figure 1: The Hepcidin-Ferroportin regulatory mechanism. Circulating hepcidin binds to the basolateral iron exporter Ferroportin (FPN) on enterocytes and macrophages, inducing its internalization and subsequent lysosomal degradation. This mechanism homeostatically restricts cellular iron release and dietary absorption in response to systemic iron levels and inflammatory signals.
Forms Matter: Traditional ferrous sulfate is cheap but harsh. Approximately 30-50% of users experience significant GI side effects [4:3]. Iron bisglycinate (where iron is bound to two glycine molecules) passes through the stomach intact and is absorbed via amino acid channels in the intestine. Trials consistently show that 25 mg of iron bisglycinate is as effective at raising ferritin as 50 mg of ferrous sulfate, but with a fraction of the side effects [3:2].
¶ Mechanism of Action
Iron's biological utility stems from its ability to easily transition between ferrous (Fe2+) and ferric (Fe3+) states, making it an ideal electron donor and acceptor.
- Oxygen Transport (Hemoglobin/Myoglobin): The bulk of the body's iron is incorporated into the heme porphyrin ring. Oxygen binds reversibly to the iron atom in heme, allowing red blood cells to pick up oxygen in the lungs and release it in peripheral tissues.
- Cellular Respiration (Mitochondria): Iron-sulfur clusters and cytochromes are physical components of the mitochondrial electron transport chain (Complexes I, II, and III). Without iron, the machinery that generates ATP stalls.
- Neurotransmitter Synthesis: Iron is a necessary cofactor for tyrosine hydroxylase and tryptophan hydroxylase, the rate-limiting enzymes in the synthesis of dopamine and serotonin, respectively.
¶ Evidence summary table (human outcomes)
| Outcome | Evidence Grade | Direction | Summary of Findings | Reference |
|---|---|---|---|---|
| Hemoglobin / Anemia Resolution | High | Increase | Uniformly effective at increasing hemoglobin and resolving iron deficiency anemia when dosing and compliance are adequate. | [2:4][3:3] |
| Fatigue Reduction (Non-Anemic) | High | Decrease | Significantly reduces fatigue scores in patients with low ferritin but normal hemoglobin, particularly in menstruating women. | [5:1] |
| Exercise Performance / VO2 Max | Moderate | Increase | Improves aerobic capacity and endurance in iron-depleted athletes by restoring oxygen delivery and mitochondrial efficiency. | [6:1] |
| Restless Legs Syndrome (RLS) Symptoms | Moderate | Decrease | Alleviates symptoms of RLS in patients with low systemic or central nervous system iron stores. | [8:1] |
| Gastrointestinal Distress | High | Increase | Traditional forms (sulfate/fumarate) cause high rates of constipation and nausea; bisglycinate and alternate-day dosing mitigate this. | [2:5][4:4] |
¶ Comprehensive Safety & Interactions
¶ Drug Interactions
- Thyroid Hormone (Levothyroxine): Iron binds to levothyroxine in the gut, completely blocking its absorption. They must be separated by at least 4 hours [9].
- Antibiotics (Tetracyclines & Fluoroquinolones): Iron dramatically reduces the absorption of these antibiotics. Separate by at least 2 hours [9:1].
- Proton Pump Inhibitors (PPIs) & Antacids: Stomach acid is required to keep non-heme iron in its absorbable (ferrous) state. Drugs that lower stomach acid severely impair iron absorption [4:5].
¶ Long-Term Risks of Excess Iron
Because the body cannot actively excrete excess iron (it is only lost through bleeding or shedding of skin/intestinal cells), unchecked supplementation leads to iron overload. Iron accumulation in tissues drives oxidative stress via the Fenton reaction (Fe2+ + H2O2 -> Fe3+ + OH. + OH-), accelerating cellular aging, insulin resistance, and increasing the risk of cardiovascular and neurodegenerative diseases.
¶ References
StatPearls. (2023). Hemochromatosis. National Center for Biotechnology Information. https://www.statpearls.com/point-of-care/22724 ↩︎ ↩︎
Pasupathy, E., Kandasamy, R., & Thomas, K. (2023). Alternate day versus daily oral iron for treatment of iron deficiency anemia: a randomized controlled trial. Scientific Reports, 13(1), 1851. https://pubmed.ncbi.nlm.nih.gov/36725875/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Milman, N., Jønsson, L., & Dyre, P. (2014). Ferrous bisglycinate 25 mg iron is as effective as ferrous sulfate 50 mg iron in the prophylaxis of iron deficiency and anemia during pregnancy in a randomized trial. Journal of Perinatal Medicine, 42(2), 197-206. https://pubmed.ncbi.nlm.nih.gov/24152889/ ↩︎ ↩︎ ↩︎ ↩︎
Powers, J. M., et al. (2017). Effect of Low-Dose Ferrous Sulfate vs Iron Polysaccharide Complex on Hemoglobin Concentration in Young Children With Nutritional Iron-Deficiency Anemia: A Randomized Clinical Trial. JAMA, 317(22), 2297-2304. https://www.semanticscholar.org/paper/ac35f7e2ee7b4b540191189f09acaa54fcfff531 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Houston, B. L., et al. (2018). Efficacy of iron supplementation on fatigue and physical capacity in non-anaemic iron-deficient adults: a systematic review of randomised controlled trials. BMJ Open, 8(4), e019240. https://ncbi.nlm.nih.gov/pmc/articles/PMC5892776/ ↩︎ ↩︎
Burden, R. J., et al. (2015). Is iron treatment beneficial in, iron-deficient but non-anaemic (IDNA) endurance athletes? A systematic review and meta-analysis. British Journal of Sports Medicine, 49(21), 1389-1397. https://pubmed.ncbi.nlm.nih.gov/25361786/ ↩︎ ↩︎
Trost, L. B., Bergfeld, W. F., & Calogeras, E. (2006). The diagnosis and treatment of iron deficiency and its potential relationship to hair loss. Journal of the American Academy of Dermatology, 54(5), 824-844. https://pubmed.ncbi.nlm.nih.gov/16635664/ ↩︎
Allen, R. P., et al. (2015). Restless legs syndrome/Willis-Ekbom disease pathophysiology. Sleep Medicine, 14(8), 697-701. https://pubmed.ncbi.nlm.nih.gov/26329430/ ↩︎ ↩︎
Campbell, N. R., Hasinoff, B. B., Stalts, H., Rao, B., & Wong, N. C. (1992). Ferrous sulfate reduces thyroxine efficacy in patients with hypothyroidism. Annals of Internal Medicine, 117(12), 1010-1013. https://pubmed.ncbi.nlm.nih.gov/1443969/ ↩︎ ↩︎