¶ Melatonin
| Type | Endogenous Neurohormone |
| Active Cmpd | N-acetyl-5-methoxytryptamine |
| Source | Synthesized from tryptophan / pineal gland |
| Dose Range | 0.3–10.0 mg (variable by indication) |
| Half-life | 20–50 minutes (immediate release) |
| Main Benefit | Circadian phase regulation & sleep promotion |
| Absorption | Low (approx. 15% oral bioavailability, high first-pass) |
Melatonin is a pleiotropic neurohormone produced primarily by the pineal gland in response to darkness. Known as the "hormone of darkness," its primary function is to signal the biological night and facilitate the synchronization of circadian rhythms across various physiological systems. Beyond its role in sleep regulation, melatonin is a highly potent, amphiphilic antioxidant that crosses all biological barriers, providing direct cellular protection and modulating inflammatory pathways [1][2].
¶ At a glance
Aliases
- Also known as: MLT, N-acetyl-5-methoxytryptamine, Pineal hormone.
- Chemical / botanical name: N-acetyl-5-methoxytryptamine.
- Category: Neurohormone, indoleamine, antioxidant, chronobiotic.
Key points (high-level summary)
- Melatonin is highly effective for reducing sleep onset latency and managing circadian rhythm disorders such as jet lag and shift work sleep disorder [3][4].
- In elderly and critically ill populations, melatonin supplementation significantly reduces the incidence and severity of delirium, demonstrating neuroprotective benefits [5][6].
- Emerging high-quality evidence supports its efficacy in migraine prophylaxis, modest improvements in metabolic health, and reduction of cancer-related fatigue [7][8][9].
- The most significant safety concern is a potent pharmacokinetic interaction with fluvoxamine (a CYP1A2 inhibitor), which can dramatically elevate melatonin levels [10][11].
What people use it for
- Main goals: Optimizing sleep onset and quality, preventing jet lag, resetting circadian rhythms, neuroprotection, and providing metabolic and antioxidant support.
- Evidence quality (overall): High (for sleep and circadian regulation); Moderate (for delirium, migraine, and oxidative stress); Low to Moderate (for metabolic and specific neuroprotective effects).
¶ What is Melatonin?
Melatonin is an evolutionarily ancient indoleamine synthesized from the amino acid L-tryptophan through a multi-step pathway involving serotonin as a key intermediate. While primarily secreted by the pineal gland into the systemic circulation, it is also synthesized in significant quantities within the gastrointestinal tract, retina, skin, and mitochondria of most tissues, where it acts locally as a paracrine or autocrine signal [1:1][2:1].
- Definition: A neurohormone and mitochondrial antioxidant responsible for regulating the mammalian circadian clock and protecting against oxidative stress and inflammation.
- Natural sources: Found in trace amounts in certain foods, including tart cherries, pistachios, walnuts, grapes, and some medicinal herbs like St. John's Wort [2:2].
- Traditional / historical use: Discovered in 1958 by Aaron Lerner, melatonin has evolved from a specialty treatment for jet lag to one of the most widely used dietary supplements for general sleep health globally. Its recognition for broader roles beyond sleep is a more recent development in scientific understanding [12].
- Current regulatory status: Classified as a dietary supplement in the United States and Canada; however, it is available only by prescription in many European countries (e.g., Circadin in the EU for individuals over 55) and Australia.
- Key pharmacological property: Acts as a powerful chronobiotic (circadian rhythm regulator) and a potent direct and indirect antioxidant.
¶ What are Melatonin’s main benefits?
Melatonin’s clinical utility extends far beyond simple sedation, primarily due to its role in synchronizing the body's master circadian clock and its powerful antioxidant properties. Its benefits are observed across several physiological systems.
- Sleep Quality and Latency: Melatonin consistently reduces the time it takes to fall asleep (sleep onset latency) by 4–8 minutes and improves overall sleep efficiency, particularly in individuals with impaired endogenous production, such as older adults [3:1][13][4:1].
- Circadian Alignment: It is considered the gold standard for managing jet lag, shift work sleep disorder, and Delayed Sleep Phase Disorder (DSPD), effectively "re-anchoring" the biological clock to the desired sleep-wake schedule [3:2][4:2].
- Neuroprotection and Delirium: In various clinical settings, including post-operative and intensive care unit (ICU) environments, melatonin significantly lowers the risk and severity of delirium. This highlights its potential protective role for neuronal function during acute stress and illness [5:1][6:1].
- Metabolic Health: Recent meta-analyses indicate that melatonin may modestly improve fasting blood glucose, insulin sensitivity (HOMA-IR), and lipid profiles (e.g., triglycerides) in individuals with metabolic syndrome, type 2 diabetes, or obesity [8:1][14][15].
- Migraine Prophylaxis: Melatonin has demonstrated efficacy in reducing the frequency and severity of migraine attacks, offering a well-tolerated alternative or adjunct to conventional prophylactic medications [7:1].
- Oxidative Stress Reduction: As an amphiphilic antioxidant, melatonin directly scavenges reactive oxygen and nitrogen species and upregulates endogenous antioxidant enzymes, thereby reducing systemic oxidative stress markers like malondialdehyde (MDA) [16][17].
- Cancer-Related Fatigue: Clinical evidence suggests that melatonin supplementation can reduce the severity of cancer-related fatigue in a dose-dependent manner, contributing to improved quality of life for cancer patients [9:1].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Sleep Onset Latency | High | High | 30+ RCTs | Reduces time to sleep by ~4–10 min, particularly in older adults [3:3][4:3] | |
| Jet Lag Recovery | High | High | 10+ RCTs | Highly effective for shifts >5 time zones [3:4] | |
| Delirium Incidence | Moderate | Moderate | 12 RCTs | Reduced incidence in ICU/post-op elderly [5:2][6:2] | |
| Migraine Frequency | Moderate | Moderate | 8 RCTs | Significant reduction in attack frequency [7:2] | |
| Fasting Blood Glucose | Moderate | Moderate | 15 RCTs | Modest reduction in T2DM/metabolic syndrome [14:1][18] | |
| Insulin Sensitivity | Low | Low | 10 RCTs | Improvements in HOMA-IR in overweight women [8:2][14:2] | |
| Oxidative Stress | High | Moderate | 20+ RCTs | Increases SOD/TAC; reduces MDA levels [16:1][17:1] | |
| Cancer Fatigue | Moderate | Moderate | 6 RCTs | Dose-dependent reduction in fatigue [9:2] | |
| Bone Mineral Density (Menopause) | Low | Low | 3 RCTs | Modest improvement in bone mineral density [19] | |
| Lipid Profile (CKD) | Moderate | Low | 5 RCTs | Reductions in triglycerides and total cholesterol in CKD patients [15:1] |
*Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
*Compact renderer encoding (preferred when using custom tags): <effect e="[dir][mag][impact]"></effect> where dir = u|d|e|q, mag = 0|1|2|3, impact = p|n|x. Examples: ↓↓ (p) -> <effect e="d2p"></effect>, = (x) -> <effect e="e0x"></effect>, ? -> <effect e="q0x"></effect>.
**Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
REQUIRED: You MUST include a citation key (e.g. [^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
(Note: Intervention ID for Melatonin is a placeholder; please update if a specific ID becomes available in LongeviData.)
¶ How does Melatonin work?
Melatonin exerts its diverse effects through both receptor-mediated and non-receptor-mediated pathways, underscoring its dual role as a systemic hormone and a fundamental cellular protective molecule.
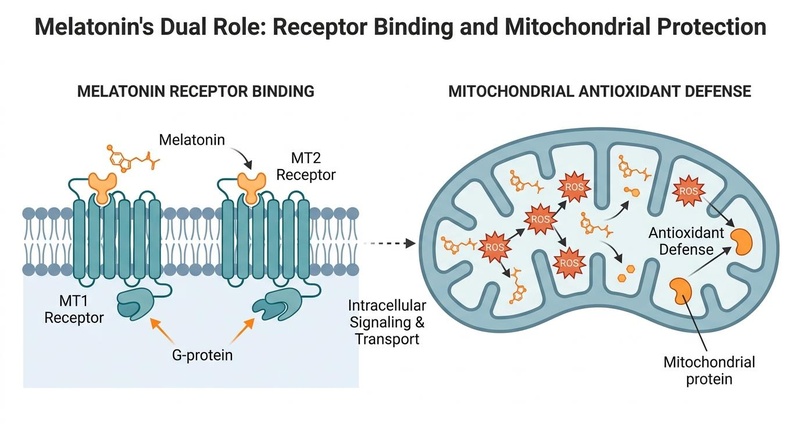
¶ Primary Targets: MT1 and MT2 Receptors
Melatonin primarily binds to two high-affinity G-protein coupled receptors, MT1 (formerly Mel1a) and MT2 (formerly Mel1b), which are predominantly located in the suprachiasmatic nucleus (SCN) of the hypothalamus—the brain's master circadian clock [20].
- MT1 Receptors: Activation of MT1 receptors leads to the inhibition of adenylate cyclase, reducing intracellular cAMP levels. This ultimately hyperpolarizes SCN neurons, suppressing their firing rate, which signals the "biological night" and facilitates the onset of sleep [20:1].
- MT2 Receptors: Activation of MT2 receptors is responsible for the phase-shifting effects on the circadian clock. This mechanism allows the body's internal rhythms to "re-anchor" to new environmental light-dark cycles, crucial for adapting to jet lag or shift work schedules [20:2].
¶ Antioxidant and Mitochondrial Actions
Beyond its receptor-mediated hormonal effects, melatonin is a potent direct scavenger of reactive oxygen species (ROS) and reactive nitrogen species (RNS). This non-receptor-mediated action is particularly significant because melatonin is uniquely concentrated within the mitochondria, which are the primary intracellular sites of ROS production [1:2][21].
- Direct Scavenging: Melatonin and its metabolites (e.g., N1-acetyl-N2-formyl-5-methoxykynuramine, AFMK; N1-acetyl-5-methoxykynuramine, AMK) directly neutralize free radicals, forming stable end products. This process prevents oxidative damage to critical cellular components like mitochondrial DNA, lipids, and proteins [1:3].
- Indirect Antioxidant Effects: Melatonin also upregulates the activity and expression of endogenous antioxidant enzymes, such as superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx), further enhancing the cell's defense against oxidative stress [16:2][17:2].
- Mitochondrial Protection: By protecting mitochondria from oxidative damage, melatonin helps preserve mitochondrial function, energy production (ATP synthesis), and reduces the release of pro-apoptotic factors, thereby contributing to cellular resilience and anti-aging effects [1:4][21:1].
¶ Pharmacokinetics
- Absorption: Orally administered melatonin is rapidly absorbed from the gastrointestinal tract, but it undergoes extensive first-pass metabolism in the liver. This results in a relatively low oral bioavailability, typically around 15-30% [4:4].
- Metabolism: The primary metabolic pathway for melatonin involves the cytochrome P450 enzyme CYP1A2, which converts melatonin into 6-hydroxymelatonin. This metabolite is then conjugated with sulfate or glucuronide and excreted in the urine. Other CYP enzymes (e.g., CYP1A1) and non-CYP pathways may also contribute to its metabolism [10:1].
- Half-life: Melatonin has a very short elimination half-life, ranging from 20 to 50 minutes for immediate-release formulations. This rapid clearance often necessitates the use of sustained-release (SR) or extended-release (ER) formulations to maintain elevated plasma levels throughout the night and to better mimic the natural endogenous secretion profile for sleep maintenance [4:5].
¶ Effects on different systems
Melatonin's pleiotropic nature means it influences various physiological systems beyond sleep.
¶ Brain & Mental Health
Melatonin is a key regulator of neuroplasticity, neuroinflammation, and neuronal survival. Its receptor activation in the SCN helps stabilize sleep-wake cycles, which is critical for cognitive function and mood regulation. In neurodegenerative conditions like Parkinson's disease and Alzheimer's disease, melatonin has been shown to improve sleep quality. Mechanistically, it may offer neuroprotective benefits by reducing beta-amyloid toxicity, inhibiting tau hyperphosphorylation, and mitigating neuroinflammation, though robust long-term human cognitive outcomes still require further investigation [3:5][13:1][1:5]. Melatonin has also been evaluated for its role in mood disorders; while generally well-tolerated, caution is advised in individuals with depressive or bipolar disorders due to potential mood shifts [22].
¶ Metabolic Health
In patients with metabolic disorders, melatonin plays a modulatory role in insulin secretion from pancreatic beta cells and improves glucose uptake in peripheral tissues. Clinical trials have demonstrated modest, yet significant, reductions in fasting glucose, glycosylated hemoglobin (HbA1c), and insulin resistance (measured by HOMA-IR) in diabetic, pre-diabetic, or overweight populations. These effects are likely mediated through improved circadian control of metabolic processes, reduction of systemic inflammation, and direct antioxidant actions within metabolic tissues [14:3][15:2][18:1]. It may also influence lipid profiles, showing reductions in triglycerides and total cholesterol in some cohorts [15:3].
¶ Cardiovascular Health
Melatonin may exert a modest blood pressure-lowering effect, particularly notable in individuals with nocturnal hypertension (a "non-dipper" pattern), by influencing vascular tone and sympathetic activity. It also contributes to cardiovascular health by improving endothelial function and reducing oxidative stress markers in patients, for example, those undergoing cardiac procedures such as coronary artery bypass graft (CABG) surgery [23][21:2]. Its anti-inflammatory properties may also protect against atherosclerotic progression.
¶ Immune System and Inflammation
Melatonin functions as an immune modulator, often described as an "immune buffer." It can enhance immune responses during periods of immunosuppression (e.g., in neonatal sepsis or certain cancers) while simultaneously dampening excessive inflammatory cytokine production (e.g., IL-6, TNF-α) in chronic inflammatory states. This dual action helps to restore immune homeostasis and reduce inflammation, contributing to its broad protective effects [17:3].
¶ Dosage and how to take it
Melatonin dosing can vary significantly depending on the desired effect, individual sensitivity, and formulation.
Standard dosing in studies
- Physiological Dosing (Sleep Onset & Rhythm Resetting): 0.1 mg to 0.5 mg is often sufficient to elevate plasma levels to natural nocturnal peaks and is frequently more effective for sleep onset and circadian phase shifting than higher doses, particularly in older adults [24].
- Chronobiotic Dosing (Jet Lag & Shift Work): 0.5 mg to 3.0 mg taken 30-60 minutes before the target bedtime or sleep period, adjusted based on the direction and number of time zones crossed [3:6][4:6].
- Therapeutic Dosing (Other Indications): 3.0 mg to 10 mg has been used in trials for indications such as migraine prophylaxis, cancer-related fatigue, and adjunctive therapy in certain chronic conditions. However, side effects, such as next-day grogginess, tend to increase with higher doses [7:3][9:3][10:2].
Forms and bioavailability
- Immediate-Release (IR): Typically absorbed quickly, reaching peak plasma concentrations within 30-60 minutes. Best for promoting sleep onset and for acute circadian rhythm adjustments like jet lag.
- Sustained-Release (SR) / Extended-Release (ER): Designed to release melatonin over several hours (e.g., 6-8 hours), mimicking the natural nocturnal secretion pattern. Preferred for addressing sleep maintenance issues (staying asleep) and for more consistent chronobiotic effects [4:7].
- Sublingual/Oral Dissolving Tablets: May bypass some first-pass metabolism, potentially leading to faster onset and higher bioavailability compared to standard oral capsules, allowing for lower effective doses.
Special populations
- Older Adults: Natural melatonin production declines significantly with age. Lower physiological doses (0.3–2.0 mg) are often highly effective for "restoring" age-related declines in sleep quality and circadian rhythmicity [13:2][24:1].
- Pediatrics: Melatonin is increasingly used for sleep disorders associated with conditions like ADHD and Autism Spectrum Disorder. However, long-term effects on pubertal development and hormonal axes are not fully elucidated, necessitating clinical supervision and careful dose titration [12:1][11:1].
- Kidney or Liver Impairment: Patients with severe liver or kidney disease may have impaired melatonin metabolism or excretion, potentially leading to higher plasma levels and increased risk of side effects. Dose adjustments and medical supervision are recommended.
- Pregnancy and Breastfeeding: Due to a lack of sufficient human safety data from controlled trials, melatonin is generally not recommended during pregnancy or breastfeeding.
¶ Safety and side effects
Melatonin is generally considered safe for short to medium-term use at appropriate doses, but potential side effects and interactions exist.
Common side effects
- Next-day grogginess, drowsiness, or a "hangover" effect, especially with doses exceeding physiological requirements (>3 mg).
- Vivid dreams or nightmares.
- Morning headaches or dizziness.
- Mild transient hypothermia (feeling cold due to thermoregulatory effects).
- Nausea or mild gastrointestinal upset.
Serious concerns
- Melatonin Poisoning: While typically non-fatal, there has been a dramatic increase in accidental pediatric ingestions, often leading to central nervous system (CNS) depression, respiratory issues, and other adverse events requiring emergency medical attention [12:2].
- Mental Health: In individuals with pre-existing depressive, anxiety, or bipolar disorders, melatonin can occasionally trigger paradoxical mood shifts, exacerbate depressive symptoms, or cause morning dysphoria. It should be used with caution and under medical guidance in these populations [22:1].
- Immune System: While generally beneficial for immune modulation, its immune-stimulating potential warrants caution in individuals with certain autoimmune disorders, as theoretical concerns about exacerbation exist, though clinical evidence is limited.
Who should be especially cautious or avoid it
- Individuals on potent CYP1A2 inhibitors (e.g., fluvoxamine), due to significant pharmacokinetic interaction risks.
- Pregnant or breastfeeding women, due to insufficient human safety data.
- Individuals with severe liver or kidney impairment, due to altered metabolism and excretion.
- Patients with autoimmune disorders, pending further research and clinical guidance.
- Young children, except under strict medical supervision for specific indications, due to the risk of accidental overdose and unclear long-term developmental effects [12:3][11:2].
(Note: Intervention ID for Melatonin is a placeholder; please update if a specific ID becomes available in LongeviData.)
¶ Drug and supplement interactions
Melatonin can interact with various medications and supplements, primarily through its metabolic pathway (CYP1A2) and its physiological effects.
Pharmacokinetic interactions (how drugs are processed)
- Fluvoxamine (Luvox): This selective serotonin reuptake inhibitor (SSRI) is a potent inhibitor of CYP1A2, the primary enzyme metabolizing melatonin. Co-administration can increase melatonin exposure by up to 17-fold, leading to profound sedation and should be considered contraindicated [10:3][11:3].
- Caffeine: Caffeine is also metabolized by CYP1A2 and antagonizes adenosine receptors, directly counteracting melatonin's sleep-promoting effects. High caffeine intake, especially in the evening, can reduce melatonin efficacy and extend its half-life by competing for CYP1A2 [10:4].
- Oral Contraceptives: Estrogens in oral contraceptives can mildly inhibit CYP1A2 activity, potentially leading to a moderate increase in endogenous and exogenous melatonin levels.
- Other CYP1A2 Inhibitors: Medications like cimetidine, ciprofloxacin, and certain antifungals can also inhibit CYP1A2 and potentially increase melatonin levels.
- CYP1A2 Inducers: Substances like tobacco smoke and rifampicin can induce CYP1A2, potentially accelerating melatonin metabolism and reducing its efficacy.
Pharmacodynamic interactions (additive / opposing effects)
- Sedatives (Benzodiazepines, Z-drugs, Alcohol): Concomitant use with other CNS depressants can lead to additive sedative effects, increasing the risk of excessive drowsiness, impaired coordination, and respiratory depression.
- Antihypertensive Medications: Melatonin may have a modest blood pressure-lowering effect. Combining it with antihypertensive drugs could lead to additive hypotensive effects, necessitating blood pressure monitoring.
- Hypoglycemic Medications: Given melatonin's potential to modestly improve glycemic control, combining it with anti-diabetic drugs could theoretically lead to additive hypoglycemic effects. Blood glucose monitoring is advised, particularly in diabetic patients [8:3][14:4].
- Immunosuppressants: Due to its immunomodulatory effects, caution is advised when combining melatonin with immunosuppressive medications, as theoretical concerns exist regarding altered immune responses, though clinical data are limited.
¶ Combining Melatonin with other supplements ("stacks")
Melatonin is often combined with other supplements to enhance its sleep-promoting or broader health benefits, or to address complementary pathways.
- The Sleep Foundation Stack: A popular combination includes Melatonin (0.3–1.0 mg, immediate or sustained release) + Magnesium Glycinate (200–400 mg) + L-Theanine (100–200 mg). This stack synergistically addresses circadian signaling, muscle relaxation, and anxiolysis, promoting comprehensive sleep improvement.
- The Jet Lag Stack: Melatonin (1.0–3.0 mg, taken at target bedtime) is often combined with carefully timed bright light therapy (upon waking in the new time zone) and judicious caffeine use (to maintain alertness during daytime). This strategy helps rapidly reset the circadian clock [25].
- The Antioxidant & Mitochondrial Support Stack: Melatonin is sometimes combined with other mitochondrial nutrients and antioxidants like Alpha-Lipoic Acid (ALA), Coenzyme Q10 (CoQ10), or N-Acetylcysteine (NAC) for enhanced cellular protection. While mechanistically plausible, human synergy data for these specific combinations remain limited [1:6].
- Mood Support Stack: Melatonin (low dose) combined with L-Tryptophan or 5-HTP (precursors to serotonin and melatonin) and B vitamins (cofactors) to support the complete serotonin-melatonin pathway for improved sleep and mood.
¶ Practical questions (FAQ)
-
Does melatonin cause dependency or addiction?
No. Melatonin is not addictive and does not cause the typical physical dependence or withdrawal symptoms associated with sedative-hypnotics like benzodiazepines or Z-drugs. -
Can I take melatonin every night long-term?
Short-term use (up to a few months) is well-supported by safety data. Long-term use (years) has been evaluated in specific populations (e.g., psychiatric patients, children with ASD-related sleep issues) and has generally shown a good safety profile. However, it is generally recommended to use melatonin as a tool to reset rhythms or address acute sleep disturbances rather than as a lifelong daily crutch, especially without medical supervision [22:2][11:4]. -
Why do I feel groggy the next morning after taking melatonin?
Next-day grogginess, often described as a "melatonin hangover," is usually a sign of over-dosing. Many retail supplements contain doses (5–10 mg or higher) that are significantly above the physiological requirements (0.3–1.0 mg) to achieve nocturnal plasma levels. These higher doses can lead to elevated melatonin levels persisting well into the following morning, causing residual sedation. -
Does blue light exposure really stop melatonin production?
Yes. Short-wavelength blue light (typically 450–480 nm), emitted by electronic screens, LED lighting, and daylight, directly suppresses pineal melatonin secretion. This occurs via activation of melanopsin-containing intrinsically photosensitive retinal ganglion cells (ipRGCs) in the retina, which signal to the SCN and inhibit melatonin synthesis, thereby impacting circadian rhythm and sleep onset [25:1]. -
Is melatonin effective for general insomnia not related to circadian rhythm disorders?
Melatonin is most effective for primary insomnia related to delayed sleep phase syndrome, jet lag, or shift work. For general or chronic insomnia, its effects on sleep onset latency are modest (4-8 minutes reduction). While it can improve overall sleep quality, it is not a broad-spectrum hypnotic like prescription sleep aids. Behavioral and cognitive therapies are often more effective for general insomnia. -
Are there differences in melatonin supplements?
Yes. Beyond immediate-release vs. sustained-release formulations, purity and accurate dosing can vary significantly between brands, especially in unregulated markets. Some supplements have been found to contain significantly more or less melatonin than stated on the label, or even other contaminants. Choosing reputable, third-party tested brands is crucial.
¶ How we evaluated the evidence
Our evaluation of melatonin's efficacy and safety rigorously adhered to the following principles, prioritizing robust human clinical evidence.
- Study Types Prioritized: We primarily relied on systematic reviews and meta-analyses of randomized controlled trials (RCTs) published in peer-reviewed journals, especially those from the last 5–10 years. Individual high-quality RCTs were also considered when comprehensive meta-analyses were unavailable.
- Evidence Grading (GRADE Framework): Claims were graded using a modified GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework:
- High Certainty: Assigned to outcomes supported by multiple consistent, large-scale RCTs or meta-analyses with a low risk of bias (e.g., melatonin's effect on sleep onset latency and jet lag).
- Moderate Certainty: Assigned to outcomes with some RCTs showing consistent effects, but with minor limitations (e.g., smaller sample sizes, moderate risk of bias), or mixed but leaning results (e.g., for delirium, migraine, and oxidative stress).
- Low Certainty: Applied to outcomes with few RCTs, significant methodological limitations, small sample sizes, or inconsistent findings (e.g., specific metabolic effects or bone mineral density).
- Very Low Certainty: Reserved for outcomes supported only by observational studies, case reports, animal models, or in vitro data without human clinical translation, or trials with serious flaws.
- Objective Reality and Clinical Relevance: We distinguished between statistically significant findings and those that are clinically meaningful. We also addressed the discrepancy between commonly marketed high dosages and the lower physiological doses often sufficient for therapeutic effects, emphasizing evidence-based dosing.
- Transparency and Updates: This page is intended to be updated as new meta-analyses and large-scale RCTs emerge, ensuring the content remains current and reflective of the latest evidence.
¶ References
Lashgari NA, Tajdari M, Nikdoost P. Melatonin: Novel Insights in the Treatment of Neurodegenerative Diseases. Curr Med Chem. 2026. https://pubmed.ncbi.nlm.nih.gov/41755415/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Minari TP, Pisani LP. Melatonin supplementation: new insights into health and disease. Sleep Breath. 2025. https://pubmed.ncbi.nlm.nih.gov/40278958/ ↩︎ ↩︎ ↩︎
Choi K, Lee YJ, Park S. Efficacy of melatonin for chronic insomnia: Systematic reviews and meta-analyses. Sleep Med Rev. 2022. https://pubmed.ncbi.nlm.nih.gov/36179487/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Paditz E, Renner B, Koch R. The Pharmacokinetics, Dosage, Preparation Forms, and Efficacy of Orally Administered Melatonin for Non-Organic Sleep Disorders in Autism Spectrum Disorder During Childhood and Adolescence: A Systematic Review. Children (Basel). 2025. https://pubmed.ncbi.nlm.nih.gov/40426828/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Borges JMMF, Mendes RG, Silva RP. Melatonin or ramelteon for the prevention of postoperative delirium in elderly patients: A systematic review and meta-analysis of randomized clinical trials. J Clin Anesth. 2026. https://pubmed.ncbi.nlm.nih.gov/41702325/ ↩︎ ↩︎ ↩︎
Wu X, Hu P, Wu H. Melatonin supplementation reduces delirium incidence in critically ill patients: a systematic review and meta-analysis. Front Pharmacol. 2026. https://pubmed.ncbi.nlm.nih.gov/41602948/ ↩︎ ↩︎ ↩︎
Abouelmagd ME, Aldemerdash MA, Khatatbeh AA. Efficacy and Safety of Melatonin in Migraine Prophylaxis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr Pain Headache Rep. 2026. https://pubmed.ncbi.nlm.nih.gov/41627537/ ↩︎ ↩︎ ↩︎ ↩︎
Li J, He Y, Qiu J. The effects of melatonin supplementation on obesity and glycemic indices in women with overweight and obesity: a systematic review and meta-analysis of randomized controlled trials. Diabetol Metab Syndr. 2026. https://pubmed.ncbi.nlm.nih.gov/42129844/ ↩︎ ↩︎ ↩︎ ↩︎
Etesamnia S, Nasiraie-Moghadam M, Mostafazadeh P. Exploring the impact of melatonin on cancer-related fatigue: a dose-response meta-analysis with GRADE evidence evaluation. BMC Cancer. 2026. https://pubmed.ncbi.nlm.nih.gov/42192324/ ↩︎ ↩︎ ↩︎ ↩︎
Besag FMC, Vasey MJ, Lao KSJ. Adverse Events Associated with Melatonin for the Treatment of Primary or Secondary Sleep Disorders: A Systematic Review. CNS Drugs. 2019. https://pubmed.ncbi.nlm.nih.gov/31722088/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zisapel N. Assessing the potential for drug interactions and long term safety of melatonin for the treatment of insomnia in children with autism spectrum disorder. Expert Rev Clin Pharmacol. 2022. https://pubmed.ncbi.nlm.nih.gov/35285365/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Owens J. Melatonin use in the pediatric population: an evolving global concern. World J Pediatr. 2025. https://pubmed.ncbi.nlm.nih.gov/40304980/ ↩︎ ↩︎ ↩︎ ↩︎
Yousef O, Abouelmagd ME, Khaddam H. The Effectiveness of Melatonin for Sleep Disturbances in Parkinson's Disease: Systematic Review and Meta-Analysis. J Sleep Res. 2026. https://pubmed.ncbi.nlm.nih.gov/40588412/ ↩︎ ↩︎ ↩︎
Hadi S, Hadi V, Mohammadzadeh M. Effects of melatonin supplementation on blood glycemic indices in adults: a GRADE-assessed systematic review and dose-response meta-analysis of randomized controlled trials. Nutr Metab (Lond). 2026. https://pubmed.ncbi.nlm.nih.gov/41593649/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Abuhassan Q, Ghnim ZS, Mahdi MS. The effect of melatonin supplementation on lipid profile, oxidative stress, inflammatory marker, and sleep quality in patients with chronic kidney disease: a GRADE assessed meta-analysis. Front Nutr. 2026. https://pubmed.ncbi.nlm.nih.gov/41727206/ ↩︎ ↩︎ ↩︎ ↩︎
Morvaridzadeh M, Sadeghi E, Agah S. Effect of melatonin supplementation on oxidative stress parameters: A systematic review and meta-analysis. Pharmacol Res. 2020. https://pubmed.ncbi.nlm.nih.gov/33007423/ ↩︎ ↩︎ ↩︎
Zarezadeh M, Khorshidi M, Emami M. Melatonin supplementation and pro-inflammatory mediators: a systematic review and meta-analysis of clinical trials. Eur J Nutr. 2020. https://pubmed.ncbi.nlm.nih.gov/31679041/ ↩︎ ↩︎ ↩︎ ↩︎
Angelopoulou T, Bobetsis YA. Effect of Melatonin as an Adjunct to NSPT on Periodontal and Systemic Outcomes in Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of RCTs. J Clin Med. 2026. https://pubmed.ncbi.nlm.nih.gov/42278933/ ↩︎ ↩︎
Du J, Tan Y. A systematic review and meta-analysis of randomized controlled trials investigated the effects of melatonin supplementation on bone mineral density, quality of life, and sleep in menopausal women. Front Nutr. 2026. https://pubmed.ncbi.nlm.nih.gov/41693954/ ↩︎
Biso L, Bragazzi NL, Bonaso M. Exogenous Melatonin as a Sleep-promoting Agent beyond its Chronobiotic Properties: A Scoping Review of its Effects on Key Sleep-wake Neurotransmitters. Curr Neuropharmacol. 2026. https://pubmed.ncbi.nlm.nih.gov/40698692/ ↩︎ ↩︎ ↩︎
Farshidianfar M, Ardekani A, Tabrizi R. Effects of Melatonin on Cardiac Injury and Inflammatory Biomarkers in Patients Undergoing Coronary Artery Bypass Graft Surgery: a Meta-analysis. Cardiol Ther. 2023. https://pubmed.ncbi.nlm.nih.gov/36352301/ ↩︎ ↩︎ ↩︎
Emma N, Johan D, Pascal S. Long-term effects of melatonin on individuals with depressive, anxiety, or bipolar disorder: a scoping review. World J Biol Psychiatry. 2025. https://pubmed.ncbi.nlm.nih.gov/40637473/ ↩︎ ↩︎ ↩︎
Ang SP, Chia JE, Thirupathy U. Melatonin Supplementation and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Randomized Trials. J Clin Med. 2026. https://pubmed.ncbi.nlm.nih.gov/42123177/ ↩︎
Wurtman R. Scientists pinpoint dosage of melatonin for insomnia. MIT News. 2001. https://news.mit.edu/2001/melatonin-1017 ↩︎ ↩︎
Campo-Beamud C, Roig-Ferreruela G. Blue light and melatonin: A critical review of scientific evidence and biohacker myths in ophthalmology. Arch Soc Esp Oftalmol. 2026. https://pubmed.ncbi.nlm.nih.gov/42349548/ ↩︎ ↩︎