¶ Mold
| Type | Environmental Contaminant / Biotoxin |
| Primary Molds | Aspergillus, Penicillium, Stachybotrys, Chaetomium |
| Key Mycotoxins | Aflatoxins, Ochratoxin A, Trichothecenes, Gliotoxin |
| Clinical Impacts | Mycotoxicosis, CIRS, Asthma, Hypersensitivity Pneumonitis |
| Environmental Tests | ERMI, HERTSMI-2, Spore Trap, Bulk Testing |
| Main Interventions | HEPA Filtration, Remediation, Binders (CSM, Charcoal, Bentonite) |
| Clinical Validation | Urine tests lack clinical utility; Binders lack large-scale RCTs |
Mold, a common environmental contaminant, produces various mycotoxins that can significantly impact human health. Understanding its biological effects, health implications, detection methods, and remediation strategies is crucial for mitigating exposure and managing associated health conditions. This page provides a comprehensive overview of mold and mycotoxins, including clinical and supplemental interventions.
¶ At a glance
Aliases
- Also known as: Mycotoxins, Fungal Toxins, Toxic Mold
- Chemical / botanical name: Various fungal species and their metabolites
- Category: Environmental contaminant, Toxin
Key points (high-level summary)
- Mold and its mycotoxins (e.g., aflatoxin, ochratoxin, trichothecenes) can cause diverse health effects, ranging from allergies to systemic mycotoxicosis and Chronic Inflammatory Response Syndrome (CIRS).
- Detection involves environmental testing (ERMI, HERTSMI-2) and, controversially, urine mycotoxin tests, which lack FDA approval and can show positive results from dietary exposure in healthy individuals [1], [2].
- Exposure reduction strategies include humidity control, HEPA filtration, and professional remediation of water-damaged buildings [3], [4].
- Clinical and supplemental interventions often involve toxin binders like cholestyramine, activated charcoal, bentonite clay, and other natural compounds.
- Cholestyramine has demonstrated clinical efficacy in reducing mycotoxin-induced nephrotoxicity and improving symptoms in some individuals with CIRS [5], [6], [7].
What people use it for
- Main goals: Detoxification from mold exposure, alleviation of CIRS symptoms, reduction of respiratory and allergic issues.
- Evidence quality (overall): Moderate for environmental remediation and cholestyramine in specific contexts; Low to Very low for many supplemental interventions and unvalidated urine testing.
¶ What is Mold?
Mold refers to various types of fungi that grow in multicellular filaments called hyphae, reproducing by spores. They thrive in damp, warm, and humid environments, commonly found in water-damaged buildings. Many species of mold produce mycotoxins, which are secondary metabolites that can be toxic to humans and animals.
- Definition: Molds are filamentous fungi that produce spores and can grow on various organic materials, particularly in the presence of moisture. Mycotoxins are toxic compounds naturally produced by certain types of molds [8], [9].
- Natural sources: Molds are ubiquitous in nature, found indoors and outdoors. Common indoor molds include Aspergillus, Penicillium, Stachybotrys (black mold), and Chaetomium. Mycotoxins are often found in contaminated foods like grains, nuts, spices, and dried fruits [8:1].
- Traditional / historical use: Historically, some molds have been used in food production (e.g., cheese) and medicine (e.g., penicillin from Penicillium). However, mycotoxin-producing molds are generally recognized as harmful contaminants.
- Current regulatory status: Mycotoxins in food are regulated by various national and international bodies to limit human exposure. Environmental mold detection and remediation are subject to industry standards.
- Key pharmacological property in one line: Mycotoxins are secondary fungal metabolites exhibiting diverse toxicological effects including nephrotoxicity, hepatotoxicity, immunosuppression, carcinogenicity, and teratogenicity [10], [8:2], [9:1].
¶ What are Mold’s main health impacts?
Exposure to mold and mycotoxins can lead to a wide range of health issues, often depending on the type of mold, mycotoxin, duration of exposure, and individual susceptibility.
For each major health domain:
-
Mycotoxicosis:
-
Direction of effect:
Large Worsening (Large increase, negative for health) -
Magnitude: Large
-
Population studied: Individuals exposed to high levels of mycotoxins, often through contaminated food or severe environmental exposure [9:2].
-
Evidence quality: High (Based on documented outbreaks and toxicological studies)
-
Summary sentence: Acute or chronic exposure to mycotoxins can lead to mycotoxicosis, presenting with a variety of symptoms affecting multiple organ systems, including gastrointestinal, neurological, and immunological effects [10:1], [9:3].
-
Chronic Inflammatory Response Syndrome (CIRS):
-
Direction of effect:
Medium Worsening (Moderate increase, negative for health) -
Magnitude: Moderate
-
Population studied: Genetically susceptible individuals exposed to water-damaged buildings [5:1], [6:1].
-
Evidence quality: Moderate (Clinical trials and observational studies, though diagnostic criteria are debated)
-
Summary sentence: CIRS is a complex, multi-system illness characterized by a persistent inflammatory response in genetically susceptible individuals following exposure to biotoxins, often from water-damaged buildings [5:2], [6:2].
-
Respiratory and Allergic Issues:
-
Direction of effect:
Large Worsening (Large increase, negative for health) -
Magnitude: Large
-
Population studied: Individuals living or working in damp and moldy environments, particularly those with pre-existing allergies or asthma [4:1].
-
Evidence quality: High (Extensive epidemiological and clinical evidence)
-
Summary sentence: Mold exposure is strongly linked to respiratory symptoms, asthma exacerbation, allergic rhinitis, and hypersensitivity pneumonitis, especially in susceptible individuals [4:2].
-
Nephrotoxicity and Hepatotoxicity:
-
Direction of effect:
Large Worsening (Large increase, negative for health) -
Magnitude: Large
-
Population studied: Individuals with chronic dietary exposure or significant acute exposure to specific mycotoxins like ochratoxin A (nephrotoxic) and aflatoxins (hepatotoxic) [10:2], [8:3].
-
Evidence quality: High (Animal studies and human epidemiological data from endemic regions)
-
Summary sentence: Mycotoxins like ochratoxin A are potent nephrotoxins, while aflatoxins are recognized hepatocarcinogens, posing significant risks to kidney and liver health respectively [10:3], [8:4].
Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Symptoms of CIRS | High | Moderate | 1 RCT | Reduction in group-mean symptoms (22.8 to 3.9) in patients with water-damaged building illness after cholestyramine treatment [6:3] | |
| Ochratoxin A-induced nephrotoxicity | High | High | 2 Animal Studies | Cholestyramine reduced plasma levels and prevented nephrotoxicity in rats [7:1], [10:4] | |
| Aflatoxin biomarkers (human) | High | High | 1 Human Trial | Calcium bentonite clay (NovaSil) reduced urinary aflatoxin biomarkers in exposed populations [11], [2:1] | |
| Respiratory allergies/asthma | High | High | Many Observational/Epidemiological Studies | Remediation of damp buildings associated with reduced respiratory symptoms [4:3] | |
| Other mycotoxin-related symptoms | Low | Low | Insufficient human data | Varied and non-specific symptoms, difficult to attribute solely to mycotoxins without specific biomarkers [12] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- *Compact renderer encoding (preferred when using custom tags):
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. Examples:↓↓ (p)-><effect e="d2p"></effect>,= (x)-><effect e="e0x"></effect>,?-><effect e="q0x"></effect>. - IMPORTANT: If using the compact renderer encoding (<effect ...>), do NOT include the text arrows or parentheses next to it. Just use the tag.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
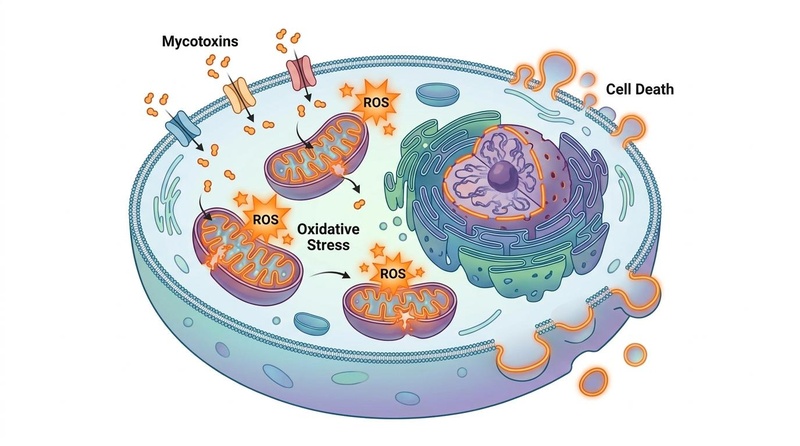
¶ How does Mold work? (Mechanisms of Mycotoxin Toxicity)
Mycotoxins exert their toxic effects through various mechanisms, often targeting essential cellular processes and leading to oxidative stress, immune dysregulation, and DNA damage [13].
- Primary targets: Mitochondria, ribosomes, DNA, immune cells, and various enzyme systems.
- Core mechanisms:
- Mitochondrial Dysfunction: Many mycotoxins, such as ochratoxin A and trichothecenes, impair mitochondrial function, leading to decreased ATP production, increased reactive oxygen species (ROS), and activation of apoptotic pathways [13:1].
- Oxidative Stress: Mycotoxins can directly generate ROS or deplete antioxidant defenses, leading to oxidative damage to lipids, proteins, and DNA [13:2].
- Immunosuppression/Immunomodulation: Some mycotoxins (e.g., aflatoxins, trichothecenes) can suppress the immune system, increasing susceptibility to infections, while others may trigger excessive inflammatory responses [13:3].
- Protein Synthesis Inhibition: Trichothecenes, for example, are potent inhibitors of protein synthesis, which contributes to their cytotoxic effects [13:4].
- DNA Damage and Carcinogenesis: Aflatoxin B1 is a known human carcinogen, forming DNA adducts that can lead to mutations and liver cancer [8:5].
- Evidence source: Mechanistic studies using in vitro cell cultures and animal models primarily, with some human biomarker data correlating with exposure [13:5], [8:6].
- Human data (if any): Biomonitoring studies detect mycotoxin metabolites in human urine, indicating exposure, but direct mechanistic studies in humans are limited to observational correlations [14], [15], [16].
- Animal / in vitro data: Extensive research in animal models and cell lines demonstrates the specific molecular targets and pathways disrupted by various mycotoxins, providing strong evidence for their toxicity [13:6], [8:7].
- Pharmacokinetics basics: Mycotoxin absorption and metabolism vary by compound. Many are metabolized in the liver and excreted through urine or bile, undergoing enterohepatic recirculation, which can prolong their systemic presence [7:2], [8:8], [14:1].
¶ Detection and Environmental Testing
Accurate detection of mold and mycotoxins is critical for identifying exposure sources and guiding remediation efforts.
¶ Environmental Mold Testing
- ERMI (Environmental Relative Moldiness Index):
- What it is: A DNA-based method that uses quantitative polymerase chain reaction (qPCR) to identify and quantify 36 different mold species in dust samples collected from buildings. It provides a numerical score indicating the relative moldiness of a building [17].
- How it is interpreted: ERMI scores typically range from -10 to +30, with higher scores indicating a greater presence of water-damage-related molds. It is often used as a research tool and should be interpreted with professional guidance [17:1].
- HERTSMI-2 (Health Effects Roster of Type-Specific Mold Secondary Index-2):
- What it is: A subset of the ERMI analysis focusing on five specific mold species (e.g., Stachybotrys chartarum, Aspergillus versicolor, Chaetomium globosum) most commonly associated with inflammatory responses in susceptible individuals [17:2].
- How it is interpreted: A HERTSMI-2 score below 10 is generally considered indicative of a safer environment for re-occupancy, especially for individuals with CIRS. Scores above 15 typically suggest the need for remediation [17:3].
- Air Sampling and Bulk Sampling:
- Air sampling: Involves collecting airborne mold spores over a period to determine their concentration. Useful for identifying active mold growth and assessing potential exposure [3:1].
- Bulk/surface sampling: Direct collection of samples from visibly moldy surfaces or suspected areas. Used to identify the species of mold present and confirm contamination [3:2].
¶ Human Biomonitoring (Urine Mycotoxin Testing)
- Controversy and Limitations:
- Urine mycotoxin tests aim to detect mycotoxin metabolites in human urine. However, these tests are highly controversial in clinical practice [1:1], [2:2], [12:1].
- Lack of FDA Approval: The CDC and FDA do not approve these tests for diagnostic purposes, citing a lack of clinical validation [1:2], [18], [19].
- Dietary Overlap: Mycotoxins are common in many foods. Therefore, positive urine results can reflect recent dietary intake from healthy food sources rather than an ongoing internal "mold illness" from environmental exposure [1:3], [14:2], [15:1]. Healthy individuals often test positive for mycotoxins in their urine due to normal dietary exposure [1:4], [15:2].
- No Established Disease-Predictive Levels: There are no established and validated urine mycotoxin levels that definitively predict disease or clinical illness [1:5], [18:1].
- ACMT Position: The American College of Medical Toxicology (ACMT) position statement indicates that urine mycotoxin testing has not been validated in well-designed epidemiological studies and is not recommended for assessing human exposure [19:1].
¶ Exposure-Reduction & Remediation Guides
Effective mold remediation involves a multi-step process focused on identifying and eliminating the source of moisture, removing contaminated materials, and preventing re-growth.
¶ Humidity Control and Ventilation
- Maintain low indoor humidity: Keep indoor humidity levels below 60% (ideally 30-50%) using dehumidifiers, air conditioners, and proper ventilation [3:3].
- Ensure adequate ventilation: Use exhaust fans in bathrooms and kitchens, and ventilate crawl spaces and attics to reduce moisture buildup [3:4].
¶ HEPA Filtration
- Use HEPA air purifiers: High-efficiency particulate air (HEPA) filters can capture mold spores and other airborne contaminants, improving indoor air quality.
- HEPA vacuum cleaners: Use vacuum cleaners equipped with HEPA filters to effectively remove mold spores from carpets and other surfaces during cleaning [3:5].
¶ Professional Remediation
- Identify and fix moisture sources: The first critical step is to find and repair any leaks, water intrusions, or sources of dampness [3:6].
- Containment: Isolate the contaminated area using plastic sheeting and negative air pressure to prevent the spread of mold spores to other parts of the building [3:7].
- Source removal: Physically remove all mold-contaminated porous materials (e.g., drywall, insulation, carpeting). Non-porous materials can sometimes be cleaned [3:8].
- Cleaning and drying: Thoroughly clean all surfaces with appropriate antimicrobial agents and ensure that the remediated area is completely dry before reconstruction [3:9].
- Preventative measures: After remediation, implement ongoing moisture control and maintenance to prevent future mold growth.
- IICRC S520 Standard: Professional mold remediation should follow industry standards like the Institute of Inspection Cleaning and Restoration Certification (IICRC) S520 Standard, which outlines best practices for safe and effective mold removal [3:10].
¶ Clinical/Supplemental Interventions and Binders
Various interventions are employed to support detoxification and mitigate the effects of mycotoxin exposure, with different levels of evidence.
¶ Cholestyramine (CSM)
- Mechanism of Action: Cholestyramine is a bile acid sequestrant resin that binds to bile acids and other compounds (including certain mycotoxins like ochratoxin A) in the gastrointestinal tract, preventing their reabsorption via enterohepatic circulation and promoting their fecal excretion [7:3], [10:5].
- Dosing: Typically prescribed off-label in powder form, mixed with water. Dosing varies significantly in clinical practice, often starting at low doses and titrating up based on tolerance and clinical response [6:4].
- Evidence:
- Ochratoxin A: Animal studies demonstrate that cholestyramine significantly reduces plasma levels of ochratoxin A and prevents ochratoxin A-induced nephrotoxicity by disrupting its enterohepatic recirculation [7:4], [10:6].
- CIRS: A double-blind, placebo-controlled crossover trial by Shoemaker and House (2006) showed that cholestyramine treatment led to statistically significant improvement in symptoms in patients with illness from water-damaged buildings [6:5]. This supports its use in protocols for CIRS [5:3].
¶ Activated Charcoal
- Mechanism of Action: Activated charcoal is a highly porous substance with a large surface area that can adsorb a wide range of toxins, including many mycotoxins (e.g., aflatoxins, trichothecenes) in the digestive tract, preventing their absorption into the bloodstream and promoting their elimination [13:7], [20].
- Dosing: Doses vary widely, typically ranging from 250 mg to 1000 mg or more, taken between meals or away from other medications/supplements to avoid binding essential nutrients [13:8].
- Evidence:
- Aflatoxins: In vitro studies and early animal research have shown activated charcoal to be effective in binding aflatoxins and reducing their toxicity [13:9], [21].
- Broad-spectrum binding: Due to its broad-spectrum binding capacity, it is often used for acute toxin exposures, though its efficacy for chronic, low-level mycotoxin exposure in humans is less established in rigorous clinical trials [13:10], [20:1].
¶ Bentonite Clay (e.g., Calcium Bentonite, NovaSil)
- Mechanism of Action: Bentonite clay, particularly calcium bentonite, is an aluminosilicate clay with a layered structure and negative charge, allowing it to bind to positively charged toxins, including certain mycotoxins like aflatoxins and ochratoxin A, in the gastrointestinal tract [11:1], [13:11].
- Dosing: Typical doses range from 1 to 3 grams per day, often mixed with water.
- Evidence:
- Aflatoxins: Clinical trials and field studies have demonstrated the efficacy of specific bentonite clays (e.g., NovaSil) in binding aflatoxins in food and reducing biomarkers of aflatoxin exposure in humans, particularly in populations with high dietary exposure [11:2], [2:3].
- Ochratoxin A: In vitro and animal studies suggest bentonite clay can also bind ochratoxin A [13:12].
¶ Chlorella and Modified Citrus Pectin
- Chlorella:
- Mechanism of Action: Chlorella, a green algae, is proposed to bind heavy metals and some toxins due to its fibrous cell wall [13:13].
- Evidence: Primarily in vitro and animal data; human evidence for direct mycotoxin binding and clinical benefit is limited.
- Modified Citrus Pectin (MCP):
- Mechanism of Action: MCP is a soluble fiber believed to bind heavy metals and potentially other toxins in the gut, preventing reabsorption [13:14].
- Evidence: Limited direct human evidence for mycotoxin binding; more research is needed.
¶ Other Supportive Interventions
- Antioxidants: Mycotoxins induce oxidative stress; antioxidants like N-acetylcysteine (NAC), glutathione, and vitamins C and E may help mitigate cellular damage [13:15].
- Liver Support: Supplements such as milk thistle (silymarin) are often used to support liver detoxification pathways [13:16].
- Gut Health: Probiotics and prebiotics may help restore gut barrier function and support healthy microbial metabolism, which can influence mycotoxin detoxification [8:9].
¶ Safety and Contraindications
¶ General Safety Considerations for Mold Exposure
- Avoidance is primary: The most critical safety measure is to avoid or remediate mold exposure, especially in water-damaged buildings [3:11], [4:4].
- Masking symptoms: Relying solely on supplements without addressing the environmental source of mold will not resolve chronic health issues and may mask critical symptoms.
¶ Toxin Binders
- Constipation: Common side effect, especially with activated charcoal and bentonite clay. Adequate fluid intake is essential [20:2].
- Nutrient Malabsorption: Non-specific binders like activated charcoal can also bind essential nutrients, vitamins, minerals, and medications. They should be taken at least 1-2 hours away from food, medications, and other supplements [13:17], [20:3].
- Drug Interactions: Cholestyramine can interfere with the absorption of many medications (e.g., thyroid hormones, warfarin, fat-soluble vitamins). Close medical supervision is required when co-administering with other drugs [7:5], [20:4].
- Contraindications: Individuals with severe constipation, bowel obstruction, or certain gastrointestinal conditions should use binders with caution or avoid them. Cholestyramine is contraindicated in complete biliary obstruction.
- Professional Guidance: The use of binders for mycotoxin illness should be done under the guidance of a qualified healthcare professional, particularly due to potential interactions and the need for individualized protocols [20:5].
Safety row provenance requirements (required for DB-backed safety rows)
- Every safety row must include
reference_id,reference_url, andreviewed_at. reference_urlshould be a DOI, PubMed, clinical guideline, or direct primary source URL.- If a safety row cannot meet provenance requirements, do not include it in the DB widget.
¶ Drug and supplement interactions
¶ Pharmacokinetic interactions (how drugs are processed)
- Cholestyramine:
- Major enzymes or transporters affected: Binds to bile acids and can directly bind many orally administered drugs in the GI tract, reducing their absorption.
- Drugs likely impacted: Thyroid hormones (levothyroxine), warfarin, fat-soluble vitamins (A, D, E, K), thiazide diuretics, digoxin, beta-blockers, statins.
- Direction of interaction: Decreased absorption and effectiveness of co-administered drugs. Requires spacing doses by several hours [7:6], [20:6].
- Activated Charcoal:
- Major enzymes or transporters affected: Non-specific adsorbent in the GI tract.
- Drugs likely impacted: Most orally administered medications, including antibiotics, antidepressants, oral contraceptives, and many supplements.
- Direction of interaction: Decreased absorption of medications, leading to reduced therapeutic effect [13:18], [20:7].
- Bentonite Clay:
¶ Pharmacodynamic interactions (additive / opposing effects)
- Additive effects with drugs that: Cholestyramine's primary use is to lower cholesterol by binding bile acids. It may have additive effects with other lipid-lowering agents.
- Opposing effects, if any: None directly relevant to mycotoxin binding, but potential for reduced efficacy of any orally co-administered drug or supplement.
¶ Practical questions (FAQ)
-
How long does it take for mold-related symptoms to improve after remediation and treatment?
Improvement timelines vary widely. Environmental remediation must be completed first. For individuals with CIRS, recovery can take months to years following the Shoemaker Protocol, which includes environmental avoidance and targeted treatments [5:4]. -
Can I use urine mycotoxin tests to diagnose mold illness?
No. Urine mycotoxin tests are not approved by the FDA for diagnostic purposes and lack clinical validation. Positive results can frequently occur in healthy individuals due to common dietary exposures, making them unreliable for diagnosing environmental mold illness [1:6], [19:2]. -
Are mycotoxin binders safe for long-term use?
Long-term safety depends on the specific binder, dose, and individual health status. Non-specific binders can lead to nutrient deficiencies if not managed properly. Cholestyramine requires medical supervision due to potential drug interactions. Regular monitoring by a healthcare professional is crucial [20:9]. -
Is it possible to completely detoxify from mold and mycotoxins?
While complete detoxification may be challenging due to ongoing environmental exposure and the persistence of some toxins, significant reduction in body burden and symptom improvement are achievable with proper environmental remediation and clinical management [5:5], [3:12]. -
Does mold exposure always lead to CIRS?
No. CIRS develops in genetically susceptible individuals (approximately 25% of the population) exposed to biotoxins from water-damaged buildings. Many people exposed to mold may experience allergic or irritant symptoms without developing CIRS [5:6], [6:6].
¶ How we evaluated the evidence
- Study types prioritized: Randomized controlled trials, meta-analyses, systematic reviews, and large epidemiological studies for health impacts and interventions. In vitro and animal studies were used for mechanistic explanations and binder efficacy where human data is limited.
- How you graded evidence quality:
- High: Multiple high-quality RCTs or meta-analyses with consistent results, low risk of bias, adequate sample sizes (e.g., link between dampness/mold and respiratory issues [4:5]).
- Moderate: Some RCTs with minor limitations, or consistent results from otherwise high-quality observational studies. Often applies to CIRS treatment protocols due to diagnostic controversies and study designs [5:7], [6:7].
- Low: Few RCTs, significant limitations in study design, small sample sizes, or inconsistent results. Many supplemental binders for mycotoxins in humans fall into this category outside of specific compounds like NovaSil for aflatoxins [20:10].
- Very low: Only observational studies, case reports, or animal/in vitro data; or serious flaws in available trials (e.g., many claims for natural binders for generalized mycotoxicosis [20:11]).
- Sample size, risk of bias, consistency, directness, effect size: These factors were considered in assessing the overall quality and strength of evidence for each claim.
- How you decided on "magnitude" and "clinical relevance": Magnitude was assessed based on reported effect sizes in studies. Clinical relevance was determined by whether the observed effects translated into meaningful health improvements for patients.
- How frequently you plan to update the page: The page will be updated as new high-quality human clinical trials, systematic reviews, and consensus guidelines on mold, mycotoxins, and related interventions become available.
¶ References
CDC. (2015). Notes from the Field: Use of Unvalidated Urine Mycotoxin Tests for the Clinical Diagnosis of Illness — United States, 2014. MMWR. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6406a7.htm ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mitchell NJ, et al. (2014). NovaSil clay for the protection of humans and animals from aflatoxins and other contaminants. Applied Clay Science. https://pmc.ncbi.nlm.nih.gov/articles/PMC7494129/ ↩︎ ↩︎ ↩︎ ↩︎
IICRC. (2015). IICRC S520 Standard for Professional Mold Remediation. Institute of Inspection Cleaning and Restoration Certification. https://iicrc.org/s520/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
WHO. (2009). WHO Guidelines for Indoor Air Quality: Dampness and Mold. World Health Organization. https://www.ncbi.nlm.nih.gov/books/NBK143947/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dooley M, Vukelic A, Jim L. (2024). Chronic inflammatory response syndrome: a review of the evidence of clinical efficacy of treatment. Annals of Medicine and Surgery. https://pmc.ncbi.nlm.nih.gov/articles/PMC11623837/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shoemaker R, House D. (2006). Sick building syndrome (SBS) and exposure to water-damaged buildings: Time series study, clinical trial and double-blind, placebo-controlled crossover study. Neurotoxicology and Teratology. https://doi.org/10.1016/j.ntt.2006.07.001 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kermardi J, et al. (1999). Cholestyramine protection against ochratoxin A toxicity: role of ochratoxin A sorption by the resin and bile acid enterohepatic circulation. Journal of Food Protection. https://pubmed.ncbi.nlm.nih.gov/10606152/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
ToxRep. (2025). A comprehensive review of mycotoxins, their toxicity, and innovative detoxification methods. Toxicology Reports. https://pmc.ncbi.nlm.nih.gov/articles/PMC11954124/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Peraica M, et al. (1999). Toxic effects of mycotoxins in humans. Bulletin of the World Health Organization. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2557730/ ↩︎ ↩︎ ↩︎ ↩︎
Madhyastha MS, et al. (1992). Effect of dietary cholestyramine on the elimination pattern of ochratoxin A in rats. Food and Chemical Toxicology. https://pubmed.ncbi.nlm.nih.gov/1398352/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Phillips TD. (2008). Reducing human exposure to aflatoxin through the use of clay: A review. Food Additives & Contaminants. https://www.tandfonline.com/doi/full/10.1080/02652030701567467 ↩︎ ↩︎ ↩︎
Hope J. (2016). Urinary mycotoxin detection in patients with chronic fatigue syndrome or CIRS: a critical review of methodology. Global Advances in Health and Medicine. https://pubmed.ncbi.nlm.nih.gov/27827982/ ↩︎ ↩︎
Al-Anati L, Petzinger E. (2022). Mycotoxins' Toxicological Mechanisms Involving Humans, Livestock and Their Associated Health Concerns: A Review. Toxins (Basel). https://pmc.ncbi.nlm.nih.gov/articles/PMC8949390/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Vila-Donat P, et al. (2020). Human Mycotoxin Biomonitoring: Conclusive Remarks on Direct or Indirect Assessment of Urinary Deoxynivalenol. Toxins (Basel). https://pmc.ncbi.nlm.nih.gov/articles/PMC7076754/ ↩︎ ↩︎ ↩︎
Solfrizzo M, et al. (2014). Determination of Urinary Mycotoxin Biomarkers Using a Sensitive Online Solid Phase Extraction-UHPLC-MS/MS Method. Anal Bioanal Chem. https://pmc.ncbi.nlm.nih.gov/articles/PMC8230879/ ↩︎ ↩︎ ↩︎
Gerding J, et al. (2015). A comparative study of the human urinary mycotoxin excretion patterns. Mycotoxin Research. https://pubmed.ncbi.nlm.nih.gov/25501370/ ↩︎
Shoemaker RC. (2016). HERTSMI-2 and ERMI: Correlating Human Health Risk with Mold Specific qPCR in Water Damaged Buildings. Surviving Mold Consensus Document. https://www.survivingmold.com/Publications/HERTSMI-2_AND_ERMI_5_22_2016__CORRELATING_HUMAN_HEALTH_RISK_WITH_MOLD_SPECIFIC_QPCR_IN_WATER_DAMAGED_BUILDINGS_CLEAN.pdf ↩︎ ↩︎ ↩︎ ↩︎
Navy Medicine. (Undated). Urine Mycotoxin Testing. https://www.med.navy.mil/Portals/62/Documents/NMFA/NMCPHC/root/Industrial Hygiene/Urine_mycotoxin_testing_18Nov2024_rev2.pdf ↩︎ ↩︎
American College of Medical Toxicology (ACMT). (2019). ACMT Position Statement: Medical Toxicology Considerations in the Diagnosis and Treatment of Patients with Concerns About Mold-Related Inhalation Exposures. https://www.acmt.net/news/acmt-position-statement-medical-toxicology-considerations-in-thediagnosis-and-treatment-of-patients-with-concerns-aboutmold-related-inhalation-exposures/ ↩︎ ↩︎ ↩︎
He J, et al. (2022). The efficacy of mycotoxin binders to control mycotoxins in feeds and the potential risk of interactions with nutrients: a review. Journal of Animal Science and Biotechnology. https://doi.org/10.1186/s40104-022-00782-z ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hatch RC, et al. (1982). Activated charcoal therapy for aflatoxicosis in goats. American Journal of Veterinary Research. https://pubmed.ncbi.nlm.nih.gov/7181312/ ↩︎