¶ Resveratrol
Resveratrol is a natural polyphenolic compound of the stilbenoid class, primarily recognized for its role as a potential sirtuin-1 (SIRT1) activator and its association with the "French Paradox"—the observation of lower cardiovascular disease rates in populations with high red wine consumption. While early animal studies suggested dramatic lifespan-extending properties, human clinical evidence presents a more nuanced reality characterized by modest metabolic benefits, significant bioavailability challenges, and specific counter-indications for exercise performance in older adults.
| Type | Polyphenol / Stilbenoid |
| Active Cmpd | Trans-resveratrol |
| Source | Red grapes, Japanese knotweed, Blueberries |
| Dose Range | 150–1,500 mg daily |
| Half-life | ~14 minutes (free parent compound) |
| Main Benefit | Metabolic support & inflammation reduction |
| Absorption | High absorption (>70%); Low bioavailability (<1%) |
¶ At a glance
Aliases
- Also known as: Trans-3,5,4'-trihydroxystilbene
- Chemical / botanical name: Trans-resveratrol; Polygonum cuspidatum (Japanese knotweed)
- Category: Stilbenoid polyphenol
Key points (high-level summary)
- In adults with metabolic dysfunction or type 2 diabetes, resveratrol modestly improves fasting blood glucose and insulin sensitivity.
- Systematic reviews consistently show significant reductions in systemic inflammatory markers like C-reactive protein (CRP) and TNF-α.
- Resveratrol exhibits extremely low bioavailability due to rapid first-pass metabolism, requiring fat-based co-administration or advanced delivery forms.
- High-dose resveratrol may blunt positive cardiovascular and metabolic adaptations to aerobic exercise in older adults.
What people use it for
- Main goals: SIRT1 activation, blood glucose management, inflammation control, cardiovascular protection, and anti-aging support.
- Evidence quality (overall): Moderate (High for inflammatory/metabolic markers; Low for cognitive/longevity claims).
¶ What is Resveratrol?
Resveratrol is a secondary metabolite produced by plants in response to environmental stressors such as UV radiation, injury, or fungal infection. It is a non-flavonoid polyphenol belonging to the stilbene family, characterized by a dual-ring structure.
- Definition: A phytoalexin stilbenoid found in various dietary sources and used widely as a dietary supplement.
- Natural sources: The most concentrated dietary sources include red grape skins (Vitis vinifera), blueberries, peanuts, and cocoa. For supplements, the primary source is often Japanese knotweed (Polygonum cuspidatum) due to its high resveratrol density.
- Traditional / historical use: Extracts from knotweed (such as Kojo-kon) have been used in traditional Japanese and Chinese medicine for treating skin inflammation and circulatory issues.
- Current regulatory status: Generally recognized as safe (GRAS) in the US and sold as a dietary supplement in most jurisdictions (EU, UK, Canada).
- Key pharmacological property: A potent multi-target antioxidant and allosteric activator of sirtuin-1 (SIRT1) and AMP-activated protein kinase (AMPK).
¶ What are Resveratrol’s main benefits?
Resveratrol's primary clinical value lies in its ability to modulate metabolic and inflammatory pathways. Meta-analyses of randomized controlled trials (RCTs) indicate the following human outcomes:
- Systemic Inflammation: Resveratrol consistently reduces C-reactive protein (CRP), Interleukin-6 (IL-6), and TNF-α, particularly in patients with baseline systemic inflammation.
- Glycemic Control: In populations with type 2 diabetes or metabolic syndrome, it leads to significant (though often modest) reductions in fasting plasma glucose and improves HOMA-IR (insulin sensitivity).
- Obesity and Body Composition: Systematic reviews indicate a statistically significant reduction in body weight, BMI, and waist circumference, likely mediated by effects on lipid metabolism and adipokine secretion.
- Endothelial Function: Evidence suggests improvement in flow-mediated dilation (FMD), a key marker of vascular health and nitric oxide availability.
- Liver Health: In patients with non-alcoholic fatty liver disease (NAFLD), resveratrol helps reduce liver fat accumulation and markers of hepatic damage (ALT/AST).
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Systemic Inflammation (CRP) | High | Moderate | 25+ RCTs | Consistent reduction across metabolic and inflammatory cohorts [1][2][3] | |
| Fasting Blood Glucose | Moderate | Moderate | 30+ RCTs | Modest reduction primarily seen in T2D and metabolic syndrome [4][5] | |
| Insulin Sensitivity (HOMA-IR) | Moderate | Moderate | 20+ RCTs | Improvements observed in insulin-resistant populations [6][7] | |
| Human SIRT1 Expression | High | High | 16 RCTs | Dose-dependent increase in SIRT1 mRNA and protein expression [8] | |
| Body Weight & BMI | Moderate | Moderate | 20+ RCTs | Modest reductions in obese and overweight populations [9][10] | |
| Systolic Blood Pressure | Moderate | Low | 15+ RCTs | Significant effect only at doses ≥150 mg/day [11][12] | |
| Liver Enzymes (ALT/AST) | Moderate | Moderate | 12 RCTs | Reductions seen specifically in NAFLD patients [13][14] | |
| Endothelial Health (FMD) | Moderate | Moderate | 7 RCTs | Significant improvement in flow-mediated dilation [7:1] | |
| Exercise Adaptation (Aged) | Moderate | Low | 2 RCTs | May blunt cardiovascular benefits of exercise in older men [15] | |
| Cognition (Older Adults) | Low | Low | 5+ RCTs | Inconsistent benefits for memory and mood [16][17] |
- *Effect Encoding:
<effect e="[dir][mag][impact]"></effect>(u=up, d=down, e=equal, q=unclear; 1-3 magnitude; p=positive, n=negative, x=neutral). - **Consistency: Low (conflicting), Moderate (mixed), High (consistent agreement).
- ***Trials: Number of RCTs or systematic reviews informing the outcome.
¶ How does Resveratrol work?
Resveratrol functions as a multi-target molecule that modulates energy sensing and stress response pathways.
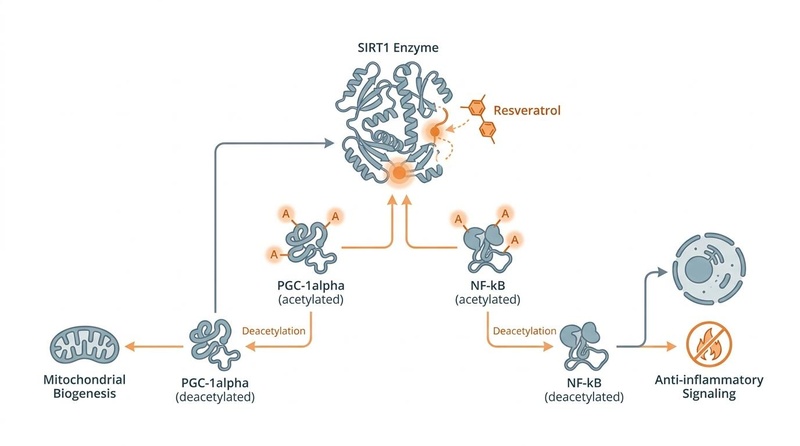
Figure 1: Molecular mechanism of trans-resveratrol acting as an allosteric activator of Sirtuin-1 (SIRT1), driving downstream deacetylation of key targets like PGC-1α and NF-κB, leading to mitochondrial biogenesis and anti-inflammatory signaling.
- Primary targets: Sirtuin-1 (SIRT1), AMP-activated protein kinase (AMPK), and Cyclooxygenase (COX-1/2).
- Core mechanisms:
- SIRT1 Activation: Resveratrol is an allosteric activator of SIRT1, which deacetylates targets like PGC-1α (promoting mitochondrial biogenesis to counter mitochondrial dysfunction) and NF-κB (reducing pro-inflammatory transcription).
- AMPK Pathway: It activates AMPK through the inhibition of cAMP phosphodiesterases, leading to increased fatty acid oxidation, glucose uptake, and autophagy.
- Antioxidant & Anti-inflammatory: It directly scavenges free radicals and inhibits the production of inflammatory eicosanoids by suppressing COX enzymes.
- Evidence source:
- Human data: Direct evidence of SIRT1 modulation and biomarker changes (CRP, glucose) supports these mechanisms in clinical settings [8:1][3:1].
- Animal data: Lifespan extension and mitochondrial enhancement in high-fat diet rodent models provided the initial mechanistic framework, though human results are less pronounced.
¶ Pharmacokinetics & Bioavailability
While ~70% of an oral dose of resveratrol is absorbed, its systemic bioavailability is extremely low (<1%) due to rapid first-pass metabolism in both the intestinal tract and the liver [18].
- Phase II Conjugation: Resveratrol is rapidly metabolized by UDP-glucuronosyltransferases (UGTs) and sulfotransferases (SULTs) to form conjugated metabolites, primarily trans-resveratrol-3-O-glucuronide, trans-resveratrol-4'-O-glucuronide, and trans-resveratrol-3-O-sulfate [17:1].
- Transporters: Active efflux of resveratrol and its metabolites is mediated by key membrane transporters, including Organic Anion Transporting Polypeptides (OATPs), Multidrug Resistance-associated Proteins (MRPs), and Breast Cancer Resistance Protein (BCRP).
- Metabolic Clearance: The half-life of free, parent trans-resveratrol in human plasma is estimated at just 14 minutes, whereas its conjugated metabolites persist significantly longer [17:2].
- Bioavailability Strategies: Fat co-administration is essential to increase solubility and absorption [18:1][17:3]. Advanced delivery options like micronization, self-emulsifying drug delivery systems (SEDDS), and liposomal or phytosomal formulations are utilized to bypass first-pass degradation and enhance systemic exposure.
¶ Effects on different systems
¶ Metabolic Health
Resveratrol’s strongest clinical signals are in metabolic regulation. Umbrella reviews of meta-analyses confirm that resveratrol improves fasting plasma glucose, insulin levels, and HbA1c in patients with type 2 diabetes [4:1][6:1]. It appears most effective at higher doses (≥500 mg/day) and in those with existing metabolic dysfunction.
¶ Cardiovascular Health
Beyond blood pressure reduction at high doses (≥150 mg), resveratrol improves vascular endothelial health by increasing nitric oxide bioavailability and flow-mediated dilation (FMD) [7:2][11:1]. However, it does not consistently improve the overall lipid profile (LDL/HDL) across healthy populations.
¶ Obesity and Body Composition
Resveratrol acts as an "energy mimetic," leading to modest reductions in body weight, body mass index (BMI), and waist circumference [10:1][16:1]. These effects are often accompanied by favorable changes in adipokines, such as increased adiponectin levels.
¶ Gut & Digestion
Emerging clinical and preclinical evidence indicates that resveratrol participates in a bidirectional interaction with the gut microbiome, behaving similarly to a prebiotic [19][20].
- Microbiota Remodeling: Supplementation has been shown to remodel the gut microbiota by increasing the Bacteroidetes-to-Firmicutes ratio, promoting the proliferation of beneficial taxa (such as Bifidobacterium, Lactobacillus, and butyrate-producing families), and suppressing pro-inflammatory proteobacteria [19:1].
- Intestinal Barrier Integrity: Resveratrol upregulates tight junction proteins (including zonula occludens-1 [ZO-1], occludin, and claudins), strengthening the gut barrier and reducing systemic lipopolysaccharide (LPS)-induced endotoxemia [20:1].
- Interindividual Variability: Human gut microbiota play a significant role in metabolizing parent resveratrol into active secondary metabolites. Differences in individual microbiome profiles (microbial enterotypes) contribute to the observed variation in clinical responsiveness (responders vs. non-responders) [21].
¶ Liver and Renal Health
In patients with Non-Alcoholic Fatty Liver Disease (NAFLD), resveratrol reduces hepatic steatosis and lowers serum ALT and AST levels [13:1][14:1]. Emergent evidence also suggests a protective role in renal function, mildly improving estimated glomerular filtration rate (eGFR) and serum creatinine [22].
¶ Brain and Cognitive Health
Resveratrol can cross the blood-brain barrier and has been studied for its potential to reduce neuroinflammation and improve glymphatic clearance [23][24]. Clinical trials in older adults show inconsistent improvements in verbal memory and mood, warranting further high-quality research [16:2].
¶ Skeletal & Bone Health
Resveratrol plays a role in bone metabolism, stimulating osteoblast differentiation and inhibiting osteoclast activity. Human systematic reviews demonstrate that resveratrol can improve bone mineral density (BMD) and modulate bone turnover markers (such as alkaline phosphatase and osteocalcin) in specific cohorts, including postmenopausal women [25].
¶ Dosage and how to take it
Standard dosing in studies
- Typical daily dose: 150 mg to 1,500 mg.
- Metabolic goals: Often use 500–1,500 mg daily.
- Cardiovascular health: Doses as low as 150 mg have shown efficacy for blood pressure and FMD.
- Schedule: Often split into two daily doses (morning and evening).
Forms and bioavailability
- Trans-resveratrol: The biologically active isomer. Avoid "cis-resveratrol" as it is unstable and inactive.
- Micronized Resveratrol: Smaller particle sizes are used in some formulations to enhance absorption.
- Liposomal or Phytosomal Forms: These advanced delivery systems significantly increase bioavailability compared to standard powder.
- Taking with fat: Resveratrol is highly lipophilic. Absorption is significantly improved when taken with a fat-containing meal (e.g., olive oil, yogurt, or nuts) [18:2][17:4].
Special populations
- Older adults: Well-tolerated, but note the potential to blunt exercise adaptations.
- Renal/Liver impairment: May be protective, but clinical monitoring is advised due to CYP inhibition.
- Pregnancy/Breastfeeding: Insufficient safety data; generally recommended to avoid.
¶ Safety and side effects
Resveratrol is generally considered safe and well-tolerated at typical supplemental doses.
Common side effects
- Gastrointestinal distress: At high doses (>2,000 mg/day), patients commonly report nausea, diarrhea, abdominal pain, and flatulence [2:1][17:5].
- Exercise Blunting: In older men, chronic supplementation (250 mg) has been shown to reduce the cardiovascular improvements (VO2 max, lipids) normally gained from exercise training [15:1].
Less common / serious concerns
- Hormonal effects: Resveratrol is a phytoestrogen and may theoretically interfere with hormone-sensitive conditions, though clinical evidence for this is sparse.
Who should be especially cautious
- Medication users: Due to potent CYP450 inhibition.
- Elite athletes: Who may wish to avoid blunting exercise-induced signaling adaptations.
¶ Drug and supplement interactions
¶ Pharmacokinetic interactions
Resveratrol is a potent inhibitor of several cytochrome P450 enzymes:
- CYP3A4, CYP2C9, and CYP1A1: Resveratrol competes for these enzymes, potentially increasing the serum concentrations and toxicity of many common drugs [23:1].
- Affected Drugs: Statins (e.g., atorvastatin), calcium channel blockers, anticoagulants (e.g., warfarin), and certain immunosuppressants.
¶ Pharmacodynamic interactions
- Anti-platelet/Anticoagulant effects: Resveratrol has mild blood-thinning properties and may have additive effects when combined with aspirin, warfarin, or clopidogrel, increasing bleeding risk.
- Hypoglycemic agents: May have additive effects with metformin or insulin, potentially increasing the risk of hypoglycemia.
¶ Combining Resveratrol with other supplements (“stacks”)
- Resveratrol + NMN: A popular longevity stack. NMN provides the NAD+ substrate required for SIRT1 function, while resveratrol acts as the "accelerator" for SIRT1 activity. Evidence level: Preclinical models and strong mechanistic/theoretical rationale; human combination trials are ongoing.
- Resveratrol + Piperine: Piperine (black pepper extract) is used to inhibit glucuronidation and sulfation in the liver, theoretically extending resveratrol's half-life. Evidence level: Early clinical pharmacokinetic studies.
- Resveratrol + Quercetin: Quercetin offers synergistic anti-inflammatory effects and also inhibits the sulfation/glucuronidation of resveratrol in the gut to enhance its bioavailability. Evidence level: Mechanistic and animal co-administration studies.
¶ Practical questions (FAQ)
-
Does red wine contain enough resveratrol for clinical benefits?
No. Red wine typically contains 1–2 mg per liter. Achieving a clinical dose of 500 mg would require hundreds of liters of wine, which is physiologically toxic. -
Should I take resveratrol before or after exercise?
Current evidence in older adults suggests that taking resveratrol chronically may blunt exercise adaptations. Some users choose to avoid resveratrol on training days or cycle it away from exercise windows. -
Is Trans-resveratrol the same as Resveratrol?
Resveratrol exists as two isomers: trans and cis. Trans-resveratrol is the biologically active form found in most high-quality supplements. -
How long does it take to see results?
Inflammatory markers and blood glucose changes typically manifest within 4–12 weeks of consistent daily supplementation. -
Is it better than Pterostilbene?
Pterostilbene is a dimethylated analog of resveratrol with significantly higher bioavailability (80% vs <1%) and a longer half-life. While resveratrol has more human data, pterostilbene is often considered a superior delivery molecule for stilbenoid benefits. -
Can I take Resveratrol alongside Metformin or other glucose-lowering medications?
Resveratrol improves insulin sensitivity and activates AMPK, which can create additive glucose-lowering effects when combined with drugs like Metformin. While potentially beneficial, this combination warrants blood glucose monitoring to prevent hypoglycemia, and potential pharmacokinetic CYP interactions should be monitored. -
Is Resveratrol beneficial for skin health or aesthetic longevity?
Both oral and topical resveratrol have been studied for their ability to combat oxidative skin damage, protect against UV-induced photodamage, and support collagen pathways. Because of oral bioavailability limits, topical formulations are typically preferred for targeted, localized skin benefits. -
Does Resveratrol need to be stored in a specific way?
Yes. Trans-resveratrol is highly sensitive to light, oxygen, and temperature. Exposure to UV light induces isomerization into the inactive cis-form. Supplements should be kept in airtight, opaque containers in a cool, dark environment (such as a refrigerator) to prevent degradation.
¶ How we evaluated the evidence
Evidence for this monograph was evaluated using a hierarchy that prioritizes umbrella reviews, systematic reviews, and meta-analyses of randomized controlled trials (RCTs). We utilized the GRADE framework to assess certainty:
- High certainty: Multiple high-quality RCTs or meta-analyses with consistent results (e.g., SIRT1 modulation).
- Moderate certainty: Significant findings from meta-analyses with some study heterogeneity (e.g., CRP reduction, glucose control).
- Low certainty: Emerging evidence from few RCTs or conflicting meta-analyses (e.g., cognitive benefits, exercise blunting).
- Very low certainty: Claims based primarily on animal models or observational studies (e.g., lifespan extension in humans).
¶ References
Sun, J. N., et al. (2026). Effects of resveratrol supplementation on multiple health outcomes: an umbrella review of systematic reviews and meta-analyses of randomized controlled trials. Nutrition Journal. https://pubmed.ncbi.nlm.nih.gov/41987155/ ↩︎
Yadegar, A., et al. (2024). Effects and safety of resveratrol supplementation in older adults: A comprehensive systematic review. Phytotherapy Research. https://pubmed.ncbi.nlm.nih.gov/38433010/ ↩︎ ↩︎
Gorabi, A. M., et al. (2021). Effect of resveratrol on C-reactive protein: An updated meta-analysis of randomized controlled trials. Phytotherapy Research. https://pubmed.ncbi.nlm.nih.gov/34472150/ ↩︎ ↩︎
Ghalichi, F., et al. (2026). The effects of resveratrol on glycemic indices and lipid profile in patients with type 2 diabetes: an umbrella review and meta-analysis. Daru. https://pubmed.ncbi.nlm.nih.gov/42268476/ ↩︎ ↩︎
Akbari, M., et al. (2020). The effects of resveratrol on lipid profiles and liver enzymes in patients with metabolic syndrome and related disorders: a systematic review and meta-analysis of randomized controlled trials. Lipids in Health and Disease. https://pubmed.ncbi.nlm.nih.gov/32066446/ ↩︎
Zeraattalab-Motlagh, S., et al. (2021). The effects of resveratrol supplementation in patients with type 2 diabetes, metabolic syndrome, and nonalcoholic fatty liver disease: an umbrella review of meta-analyses of randomized controlled trials. The American Journal of Clinical Nutrition. https://pubmed.ncbi.nlm.nih.gov/34320173/ ↩︎ ↩︎
Mohammadipoor, N., et al. (2022). Resveratrol supplementation efficiently improves endothelial health: A systematic review and meta-analysis of randomized controlled trials. Phytotherapy Research. https://pubmed.ncbi.nlm.nih.gov/35833325/ ↩︎ ↩︎ ↩︎
Mansouri, F., et al. (2025). Impact of Resveratrol Supplementation on Human Sirtuin 1: A Grading of Recommendations Assessment, Development and Evaluation-Assessed Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials. Journal of the Academy of Nutrition and Dietetics. https://pubmed.ncbi.nlm.nih.gov/40158656/ ↩︎ ↩︎
Setayesh, A., et al. (2026). The effect of resveratrol supplementation on anthropometric indices, adiponectin and leptin levels in individuals with overweight and obesity: a graded, systematic review and meta-analysis of randomized controlled trials. International Journal of Obesity. https://pubmed.ncbi.nlm.nih.gov/41455817/ ↩︎
Mousavi, S. M., et al. (2019). Resveratrol supplementation significantly influences obesity measures: a systematic review and dose-response meta-analysis of randomized controlled trials. Obesity Reviews. https://pubmed.ncbi.nlm.nih.gov/30515938/ ↩︎ ↩︎
Fogacci, F., et al. (2019). Effect of resveratrol on blood pressure: A systematic review and meta-analysis of randomized, controlled, clinical trials. Critical Reviews in Food Science and Nutrition. https://pubmed.ncbi.nlm.nih.gov/29359958/ ↩︎ ↩︎
Liu, Y., et al. (2015). Effect of resveratrol on blood pressure: a meta-analysis of randomized controlled trials. Clinical Nutrition. https://pubmed.ncbi.nlm.nih.gov/24731650/ ↩︎
Soltani, S., et al. (2023). The effect of resveratrol supplementation on biomarkers of liver health: A systematic review and meta-analysis of randomized controlled trials. Phytotherapy Research. https://pubmed.ncbi.nlm.nih.gov/36642444/ ↩︎ ↩︎
Jakubczyk, K., et al. (2020). Effects of Resveratrol Supplementation in Patients with Non-Alcoholic Fatty Liver Disease-A Meta-Analysis. Nutrients. https://pubmed.ncbi.nlm.nih.gov/32823621/ ↩︎ ↩︎
Gliemann, L., et al. (2013). Resveratrol blunts the positive effects of exercise training on cardiovascular health in aged men. The Journal of Physiology. https://physoc.onlinelibrary.wiley.com/doi/abs/10.1113/jphysiol.2013.258061 ↩︎ ↩︎
Molani-Gol, R., & Rafraf, M. (2024). Effects of resveratrol on the anthropometric indices and inflammatory markers: an umbrella meta-analysis. European Journal of Nutrition. https://pubmed.ncbi.nlm.nih.gov/38374352/ ↩︎ ↩︎ ↩︎
Cottart, C. H., et al. (2010). Resveratrol bioavailability and toxicity in humans. Molecular Nutrition & Food Research. https://onlinelibrary.wiley.com/doi/10.1002/mnfr.200900437 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Walle, T. (2011). Bioavailability of resveratrol. Annals of the New York Academy of Sciences. https://nyaspubs.onlinelibrary.wiley.com/doi/10.1111/j.1749-6632.2010.05842.x ↩︎ ↩︎ ↩︎
Sabatino, M., et al. (2022). Benefits and Implications of Resveratrol Supplementation on Microbiota Modulations: A Systematic Review of the Literature. International Journal of Molecular Sciences. https://www.mdpi.com/1422-0067/23/7/4027/ ↩︎ ↩︎
Chaplin, A., et al. (2018). Resveratrol, Metabolic Syndrome, and Gut Microbiota. Nutrients. https://www.mdpi.com/2072-6643/10/11/1651/ ↩︎ ↩︎
Bode, L. M., et al. (2013). In vivo and in vitro metabolism of trans-resveratrol by human gut microbiota. The American Journal of Clinical Nutrition. https://pubmed.ncbi.nlm.nih.gov/23283496/ ↩︎
Hajhashemy, Z., et al. (2025). Effects of resveratrol supplementation on renal function in adults: a systematic review and dose-response meta-analysis. Naunyn-Schmiedeberg's Archives of Pharmacology. https://pubmed.ncbi.nlm.nih.gov/40580309/ ↩︎
Detampel, P., et al. (2012). Drug interaction potential of resveratrol. Drug Metabolism Reviews. https://pubmed.ncbi.nlm.nih.gov/22788578/ ↩︎ ↩︎
Grandi, R., et al. (2026). Investigating the impact of resveratrol and quercetin on glymphatic function, blood-brain barrier, and neuroglial health: A systematic review. Brain Research. https://pubmed.ncbi.nlm.nih.gov/41241264/ ↩︎
Shuid, A. N., et al. (2025). A Systematic Review on the Molecular Mechanisms of Resveratrol in Protecting Against Osteoporosis. International Journal of Molecular Sciences. https://pubmed.ncbi.nlm.nih.gov/40243497/ ↩︎