¶ Sleep Optimization

| Type | Nutraceuticals & Chronobiotics |
| Active Cmpd | Melatonin, L-Theanine, Valerenic Acid, Hesperidin, Valerosidate |
| Source | Pineal gland (endogenous), Camellia sinensis, Valeriana officinalis |
| Dose Range | Melatonin: 0.3–5 mg; L-Theanine: 200–400 mg |
| Half-life | Melatonin: 30–50 min; L-Theanine: ~50–70 min |
| Main Benefit | Reduced sleep latency, improved sleep quality, circadian regulation |
| Absorption | Highly variable, dependent on sublingual vs. oral delivery |
Sleep optimization supplements represent a class of natural, over-the-counter chronobiotics and GABAergic nutraceuticals designed to modulate circadian rhythms, reduce sleep latency, and enhance sleep architecture. Clinical evidence strongly supports L-theanine and low-dose melatonin for specific sleep parameters, while herbal derivatives like valerian demonstrate moderate efficacy with significant individual variation.
¶ At a glance
Aliases
- Also known as: Sleep aids, chronobiotics, natural hypnotics, somnology supplements
- Chemical / botanical name: N-acetyl-5-methoxytryptamine (Melatonin), L-gamma-glutamylethylamide (L-Theanine), Valeriana officinalis (Valerian Root)
- Category: Chronobiotics, amino acids, and botanical sedative extracts
Key points (high-level summary)
- In healthy adults experiencing sleep disturbances, L-theanine at 200 mg/day significantly decreases sleep latency, mitigates stress-related symptoms, and enhances objective sleep quality without daytime drowsiness.
- Low-dose oral melatonin (0.3–3.0 mg) effectively shifts circadian phases and reduces sleep latency, particularly in pediatric ADHD, autism spectrum disorder (ASD), and older adults with age-related hypomelatoninemia.
- High-dose melatonin (>5 mg) saturates receptor pathways, disrupting chronobiological phase shifts, and is associated with rapid clearance and poor individual sleep maintenance.
- Herbal preparations like valerian root can exhibit variability in active constituents and are associated with rare but notable mild gastrointestinal distress and morning drowsiness if combined with other GABAergic agents.
What people use it for
- Main goals: Reducing sleep onset latency, enhancing slow-wave sleep, managing shift-work sleep-wake cycles, and alleviating nocturnal anxiety.
- Evidence quality (overall): Moderate to High (RCT-driven for melatonin and L-theanine, moderate for valerian, low to moderate for herbal combinations).
¶ What is Sleep Optimization?
Sleep optimization supplements are targeted exogenous compounds that cross the blood-brain barrier to modulate neurotransmitter signaling (GABA, glutamate, orexin) or mimic endogenous endocrine signals (melatonin) that regulate the sleep-wake cycle. Unlike synthetic sedatives, these natural interventions aim to support or restore physiological sleep architecture rather than forcing generalized central nervous system depression.
Melatonin is naturally synthesized from tryptophan in the pineal gland of humans, but commercial preparations are chemically synthesized to match the molecular structure of the endogenous hormone. L-Theanine is a non-proteinogenic amino acid primarily found in the leaves of Camellia sinensis (green tea), while valerian root is extracted from the roots and rhizomes of Valeriana officinalis.
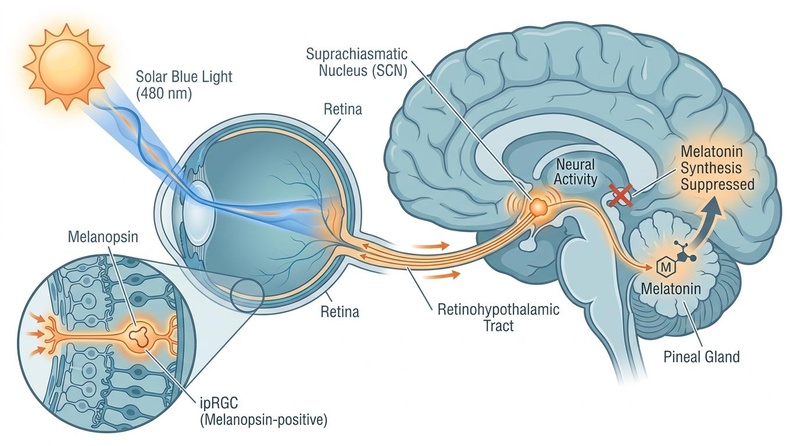
Figure 2: Light-induced entrainment of the circadian pacemaker. Solar blue light (480 nm) is sensed by melanopsin-positive ipRGCs in the retina and transduced via the retinohypothalamic tract to the suprachiasmatic nucleus (SCN), suppressing melatonin synthesis in the pineal gland.
Historically, botanical extracts like valerian root have been utilized since ancient Greek and Roman times as traditional remedies for restlessness, state anxiety, and insomnia. In contrast, tea-derived L-theanine has been consumed for centuries for its calming, non-sedating focus. Modern regulatory frameworks typically classify these agents as dietary supplements in the United States under the DSHEA, though melatonin is classified as a prescription-only hormone in several jurisdictions (e.g., the United Kingdom, European Union, and Australia) for adults under 55.
¶ What are Sleep Optimization’s main benefits?
The primary clinical objective of sleep optimization supplements is to restore natural sleep-wake patterns and relieve occasional sleep disturbances. Extensive randomized controlled trials and meta-analyses highlight specific, targeted benefits across several physiological sleep domains.
¶ Reducing Sleep Onset Latency
- Outcome: Sleep onset latency (the time required to transition from full wakefulness to sleep).
- Direction of effect: Decrease.
- Magnitude: Moderate (typically 10 to 30 minutes reduction, depending on baseline sleep onset delay).
- Population studied: Healthy adults with occasional insomnia, children with neurodevelopmental disorders (ASD, FASD, ADHD), and post-surgical populations.
- Evidence quality: High.
- Summary: Low-dose melatonin and L-theanine consistently reduce the time required to fall asleep across both healthy and clinical populations.
¶ Enhancing Sleep Quality and Architecture
- Outcome: Subjective and objective sleep quality measures (including PSQI scores, actigraphy-verified sleep efficiency, and slow-wave sleep duration).
- Direction of effect: Increase.
- Magnitude: Moderate.
- Population studied: Healthy adults, pediatric populations with ADHD, and patients undergoing hemodialysis.
- Evidence quality: Moderate.
- Summary: L-theanine and valerian significantly improve self-reported sleep quality, slow-wave sleep duration, and daytime cognitive function.
¶ Circadian Phase Alignment
- Outcome: Adjustment of the internal biological clock and shift of the Dim Light Melatonin Onset (DLMO).
- Direction of effect: Phase-advance or phase-delay (dependent on administration timing).
- Magnitude: Large (can shift the master clock by up to 1.5 to 2 hours).
- Population studied: Adults with circadian rhythm sleep disorders (CRSD) and jet lag.
- Evidence quality: High.
- Summary: Timed, low-dose melatonin acts as a powerful chronobiotic, resetting the master clock in the suprachiasmatic nucleus to align with desired sleep cycles.
¶ Mitigating Nocturnal Anxiety and Stress
- Outcome: Subjective state anxiety, sleep-related worry, and sympathetic nervous system activity.
- Direction of effect: Decrease.
- Magnitude: Moderate.
- Population studied: Hemodialysis patients and healthy adults undergoing cognitive stress.
- Evidence quality: Moderate.
- Summary: L-theanine and valerian extract reduce sympathetic arousal and lower scores on validated anxiety scales, facilitating transition to sleep.
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Sleep Onset Latency (Melatonin) | High | High | Multi-systematic reviews | Decreases latency in pediatric ADHD/ASD and FASD [1][2][3]. | |
| Sleep Onset Latency (L-Theanine) | High | High | Multiple RCTs | Significantly decreases latency and PSQI sleep disturbance [4][5][6]. | |
| Sleep Quality (Valerian Root) | Moderate | Moderate | Systematic reviews | Improved sleep quality, state anxiety, and depression in hemodialysis [7][8][9]. | |
| Circadian Phase Shifts (Melatonin) | High | High | Multiple RCTs | Promotes phase advance or delay depending on dosing timing relative to DLMO [10][11]. | |
| Post-Surgical Sleep (Melatonin) | Moderate | Moderate | 1 RCT | Melatonin failed to improve sleep quality following primary total hip arthroplasty [12]. | |
| Restless Legs Syndrome (Supplements) | Low | Low | Systematic review | Small improvements in symptom severity; evidence remains highly limited [13][14]. |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- *Compact renderer encoding:
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. - IMPORTANT: If using the compact renderer encoding (<effect ...>), do NOT include the text arrows or parentheses next to it. Just use the tag.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree).
- ***Trials: Number of RCTs or total trials informing this outcome.
- **REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row.
¶ How does Sleep Optimization work?
Understanding the molecular and neurobiological mechanisms of these sleep-supportive compounds is critical for designing precise, targeted optimization protocols. Sleep optimization supplements operate via multiple distinct pathways.
¶ Primary Targets
Exogenous sleep supplements target multiple regulatory hubs within the central nervous system, including:
- Melatonergic receptors (MT1 and MT2) in the suprachiasmatic nucleus.
- GABA-A receptor complexes and the enzyme GABA transaminase.
- Inhibitory glycine receptors and excitatory NMDA/AMPA receptors.
- Orexin 2 receptors (OX2R) in wake-promoting cortical pathways.
¶ Core Mechanisms
- Melatonergic Signaling (MT1/MT2 Activation): Exogenous melatonin binds to high-affinity GPCRs in the suprachiasmatic nucleus (SCN). MT1 receptor activation inhibits neuronal firing in the SCN, suppressing wake-promoting signals and inducing sleepiness, while MT2 receptor activation mediates the physical phase-shifting (resetting) of the master circadian clock [2:1][10:1] (see Figure 3 for the integrated neuroanatomical pathway, sleep staircase architecture, and dual-process regulation model).
- GABAergic Facilitation: Valerenic acid and other constituents in valerian extract inhibit the enzyme GABA transaminase, which is responsible for the breakdown of GABA. This inhibition raises synaptic concentrations of GABA, facilitating greater binding to GABA-A receptors, which hyperpolarizes postsynaptic neurons and dampens central nervous system hyperexcitability [15][16].
- Glutamate Antagonism and Sympathetic Regulation: L-Theanine structurally mimics glutamate and competitively binds to NMDA, AMPA, and kainate receptors, acting as a weak antagonist. By blocking excitatory glutamatergic signaling, L-Theanine limits sympathetic nervous system arousal and mitigates stress-induced cortisol and epinephrine spikes [17][18][5:1].
- Orexinergic Modulation: State-of-the-art computational screening and molecular dynamics simulations of Valeriana species have identified natural orexin 2 receptor (OX2R) antagonists, specifically hesperidin and valerosidate. These natural compounds bind to OX2R with a binding free energy comparable to suvorexant, potentially blocking wake-promoting orexinergic projection pathways [19].
[Exogenous Sleep Supplements]
|
+-----------------------+-----------------------+
| | |
[Melatonergic] [GABAergic] [Glutamatergic]
(Melatonin) (Valerian) (L-Theanine)
| | |
SCN MT1/MT2 GABA Transaminase NMDA/AMPA Blockade
Activation Enzyme Inhibition & Cortisol
| | |
Circadian Phase Shift Postsynaptic Hyper- Suppressed Sympathetic
& SCN Sleepiness Onset polarization & Calming Arousal & Stress
 troughs. Bottom-Left: The neuroanatomical multisynaptic pathway for circadian melatonin regulation (Retina -> SCN -> PVN -> Spinal Cord -> SCG -> Pineal Gland), with SCN labeled exactly once pointing to the anterior hypothalamus. Bottom-Right: The Two-Process Model, where Process S (Sleep Pressure) peaks exactly at 11 PM sleep onset and declines immediately, Process C (Circadian Alertness) peaks in the late afternoon/early evening (6 PM to 9 PM) and declines before bedtime, and the shaded sleep window aligns perfectly starting precisely at 11 PM.")
¶ Pharmacokinetics Basics
Oral melatonin is absorbed rapidly but undergoes significant first-pass hepatic metabolism by the cytochrome P450 enzyme CYP1A2, resulting in low oral bioavailability (approximately 15%) and a short plasma half-life of 30 to 50 minutes [2:2]. Sublingual administration bypasses first-pass metabolism, yielding higher peak concentrations and a faster onset of action [1:1]. L-Theanine is rapidly absorbed in the intestinal tract, crossing the blood-brain barrier via the leucine-preferring transport system within 30 minutes, reaching peak plasma levels within approximately 50 to 70 minutes with excellent bioavailability [5:2].
¶ Effects on different systems
These somnologic and chronobiotic interventions exert profound downstream physiological effects, which are highly system-specific.
¶ Neurological and Circadian Systems
Exogenous melatonin serves as a primary chronobiotic, capable of advancing or delaying the circadian clock depending on its administration timing relative to an individual's Dim Light Melatonin Onset (DLMO) [10:2][11:1] (represented by Process C in the dual-process model of Figure 3). High-precision salivary assessments identify specific clinical endotypes (such as delayed or advanced melatonin onset, hypermelatoninemia, or irregular/multipeak profiles) to allow clinicians to tailor chronobiotic therapy precisely [11:2].
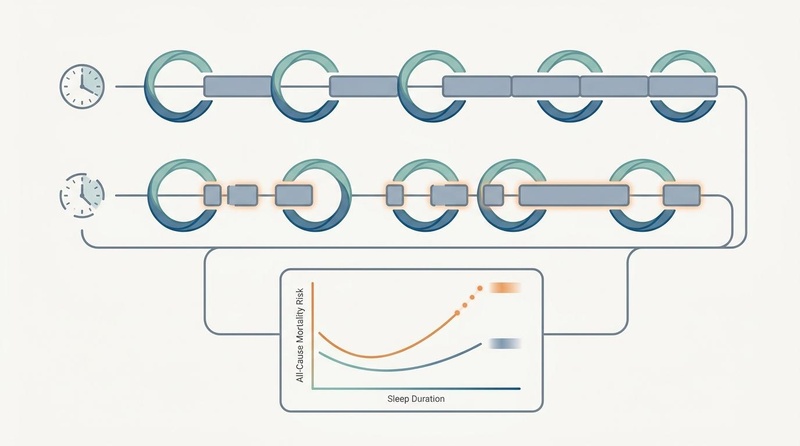
Figure 4: Physiological comparison of regular and irregular sleep patterns. High sleep regularity (consistent bedtime and wake times) maintains metabolic stability, whereas irregular or fragmented sleep disrupts peripheral clocks and is associated with elevated all-cause mortality.
Furthermore, environmental light factors significantly alter this system; for example, violet-excitation LEDs can enhance sleepiness and preserve melatonin secretion [20], while large Cochrane reviews demonstrate that blue-light filtering spectacle lenses have little to no clinical effect on sleep quality [21]. From a clinical neuropathology perspective, untreated circadian rhythm sleep disorders are associated with an increased risk of primary open-angle glaucoma and ocular hypertension, an association modified by the protective, neurovascular-regulating role of melatonin [22].
¶ Psychological and Mood Regulation
Sleep latency and quality are closely linked to daytime psychological parameters. High-impact clinical trials demonstrate that L-theanine (200 mg/day) reduces subjective stress, depression, and state anxiety scores across both clinical populations (such as hemodialysis patients) and healthy adults with high stress-related ailments [7:1][5:3]. This neurological calming effect directly translates to reduced sleep-onset latency and decreased sleep disturbances on the Pittsburgh Sleep Quality Index (PSQI) [5:4].
¶ Metabolic and Ovarian Systems
Beyond direct sleep modulation, melatonin exhibits highly potent systemic anti-inflammatory, anti-apoptotic, and antioxidative properties. Recent advances have established an integrated mechanistic model showing that melatonin acts as a pleiotropic regulator in ovarian tissues, counteracting oxidative stress, mitochondrial dysfunction, inflammatory cascades, and autophagic imbalances in conditions like polycystic ovary syndrome (PCOS), premature ovarian insufficiency (POI), and age-related ovarian decline [23].
¶ Pediatric and Neurodevelopmental Applications
Pediatric sleep management represents a major clinical challenge, with Japanese database analyses indicating a dramatic rise in pediatric hypnotic prescribing over the past decade [24]. Clinical trial data support the therapeutic potential and tolerability of L-theanine and sublingual melatonin in children with ADHD and Foetal Alcohol Spectrum Disorder (FASD), demonstrating significant improvements in objective actigraphy-verified sleep efficiency, total sleep duration, and sleep onset latency without the severe neuropsychiatric adverse effects associated with zolpidem or other pharmaceutical sedative-hypnotics [1:2][2:3][3:1][6:1].
¶ Dosage and how to take it
Clinical application requires strict adherence to evidence-based dosing protocols to avoid receptor desensitization and chronobiological desynchrony.
¶ Standard Dosing in Studies
- Melatonin (Chronobiotic / Circadian Shift): 0.3 mg to 1.0 mg, administered 4.5 to 7 hours before the desired or habitual bedtime [10:3][11:3]. This low dose mimics physiological levels and is optimized for phase advancement.
- Melatonin (Soporific / Sleep Induction): 1.0 mg to 3.0 mg, taken 30 to 60 minutes before bedtime [2:4].
- L-Theanine: 200 mg to 400 mg daily, taken either as a single dose 1 hour before sleep or split into two equal doses (morning and evening) to manage daytime sympathetic arousal [5:5][6:2].
- Valerian Root: 300 mg to 600 mg of a standardized extract (typically containing 0.8% valerenic acid) taken 30 to 60 minutes before bedtime [7:2][8:1].
¶ Forms and Bioavailability
Sublingual melatonin tablets or liquid drops bypass first-pass hepatic metabolism, presenting superior bioavailability and rapid onset compared to standard immediate-release or extended-release oral formulations [1:3][2:5]. For occasional insomnia and sleep maintenance, clinically validated herbal combinations, such as the valerian-hops extract formulation Ze 91019, show synergistic effects that significantly increase total sleep duration and improve daytime cognitive parameters compared to valerian monotherapy [9:1].
¶ Special Populations
- Pregnancy and Breastfeeding: Gestational insomnia and Restless Legs Syndrome (RLS) require a highly structured, stepped-care clinical algorithm [13:1][14:1]. High-dose melatonin or unstandardized herbal preparations are typically avoided due to a lack of safety data. Non-pharmacological interventions, including laser acupuncture at specific meridian points and self-administered acupressure, are highly feasible, safe, and clinically effective alternatives [25][26][27].
- Children and Adolescents: For children with neurodevelopmental disorders (ASD, FASD, or ADHD), melatonin is highly effective at 1.0 mg to 3.0 mg, and L-theanine is well tolerated at 200 mg twice daily [1:4][3:2][6:3].
- Renal or Hepatic Impairment: Patients with severe hepatic impairment exhibit drastically reduced melatonin clearance and should avoid exogenous supplementation to prevent prolonged diurnal sedation [2:6][10:4].
¶ Age-Specific Sleep Optimization Guidelines
Circadian rhythms and sleep architecture undergo profound shifts across the human lifespan, necessitating age-targeted somnologic strategies:
- Young Adults (Ages 18–34): Typically characterized by a late circadian phase preference ("night owls") and high vulnerability to social jetlag. The priority is phase alignment and sleep regularity [11:4][5:6]. L-Theanine (200 mg) is highly effective for reducing sleep latency caused by academic or work-related performance anxiety [5:7]. Melatonin should be restricted to low, chronobiotic doses (0.3 mg) taken 5–7 hours before desired sleep onset if attempting to advance the sleep phase, rather than used as a general sedative [10:5][11:5].
- Middle-Aged Adults (Ages 35–64): This cohort experiences a progressive decline in slow-wave sleep (SWS) and an increase in sleep fragmentation, often exacerbated by stress-induced cortisol elevations. Apigenin and magnesium (the "Sleep Starter Kit") are prioritized to buffer NMDA excitation and enhance GABA-A tone [15:1][17:1]. Valerian-hops combinations (Ze 91019) are highly useful here to increase total sleep duration and restore slow-wave sleep architecture [9:2].
- Older Adults (Ages 65+): Older populations exhibit "advanced phase syndrome" (early bedtimes and early waking) coupled with age-related pineal calcification, leading to severe hypomelatoninemia [2:7][11:6]. Low-dose melatonin (1.0–2.0 mg) taken 30–60 minutes before bed acts as a direct hormone replacement therapy, restoring sleep efficiency and reducing nocturnal awakenings [2:8]. Sophorific agents like valerian must be used at lower doses to prevent morning ataxia and fall risk [8:2][14:2].
¶ Biological Sex Differences in Sleep Physiology
- Women: Females are twice as likely as males to report chronic insomnia, a disparity heavily modulated by estrogen and progesterone fluctuations. During the luteal phase of the menstrual cycle, and acutely during perimenopause/menopause, the rapid decline in progesterone (a potent neurosteroid that binds to GABA-A receptors) causes severe sleep fragmentation and nocturnal thermoregulatory disruptions (hot flashes). For menopausal sleep disturbances, L-theanine and valerian provide critical GABAergic support [7:3][15:2][5:8]. If Restless Legs Syndrome (RLS) occurs—which is highly prevalent in pregnant women—iron status must be evaluated [13:2], and non-pharmacological therapies like acupressure are strongly indicated [27:1].
- Men: Males generally exhibit a higher incidence of obstructive sleep apnea (OSA) and a faster age-related decline in deep slow-wave sleep. If a male patient experiences severe snoring, daytime sleepiness, and high glycemic variability, clinicians must screen for OSA prior to initiating any GABAergic sedatives (like valerian), as these agents can depress upper airway muscle tone and worsen hypoxic events [14:3].
¶ The Clinical Sleep Intervention Decision Path
To select the most effective somnologic intervention, utilize this biomarker- and symptom-guided clinical decision path:
[Patient Sleep Assessment]
|
+----------------+----------------+
| |
[Is Sleep Onset Latency [Is Sleep Maintenance &
the Primary Issue?] Night-Waking the Primary Issue?]
| |
+------+------+ +------+------+
| | | |
[YES] [NO] [YES] [NO]
| | | |
[Administer L-Theanine [Evaluate circadian [Prioritize Valerian/ [Evaluate for sleep
(200mg) or Low-Dose phase; utilize Hops combination or apnea or environmental
Melatonin (0.3-1mg) light therapy or extended-release disruptors (noise/heat)]
1 hr before bed] early DLMO dosing] melatonin (1-3mg)]
¶ Safety and side effects
A critical review of the scientific literature demonstrates that sleep-promoting nutraceuticals are generally well tolerated and display low toxicity, though specific side effects and contraindications must be managed.
¶ Common Side Effects
- Melatonin: Mild daytime sleepiness, early morning grogginess, vivid dreams, hypothermia, and mild headache [2:9][10:6].
- L-Theanine: No serious adverse effects reported in clinical trials; rare instances of mild gastrointestinal upset or transient hypotension at very high doses [5:9].
- Valerian Root: Mild morning drowsiness ("hangover effect"), headache, and gastrointestinal distress [3:3][9:3].
¶ Less Common / Serious Concerns
Unlike synthetic GABA-A receptor agonists (such as zolpidem or eszopiclone), which carry high risk of severe neuropsychiatric adverse reactions, dependency, and sleepwalking behaviors, natural chronobiotics do not show signals for dependency or rebound insomnia [3:4]. However, excessive high-dose melatonin use (>5–10 mg) can induce hypermelatoninemia, resulting in sustained elevated diurnal melatonin levels that trigger severe circadian desynchrony, mood disturbances, and impaired daytime coordination [10:7][11:7].
¶ Who should be especially cautious or avoid it
- Individuals on immunosuppressive therapy, as melatonin can stimulate immune activity.
- Patients taking blood thinners or antiplatelet medications, due to potential mild antiplatelet effects.
- Individuals with severe liver disease, who cannot effectively clear melatonin [2:10][10:8].
¶ Red Flags & Adverse Diagnostic Escalation
While over-the-counter sleep aids are highly accessible, specific symptoms warrant immediate suspension of supplements and formal clinical diagnostic escalation:
- Suspected Obstructive Sleep Apnea (OSA): Loud, habitual snoring punctuated by gasping, choking, or observed apneas during sleep, accompanied by severe morning headache and daytime cognitive impairment. Do NOT administer GABAergic sedatives, as they can prolong respiratory pauses.
- Treatment-Resistant Severe Insomnia: Insomnia that fails to respond to sleep hygiene, L-theanine, and melatonin after 4 consecutive weeks, indicating the potential presence of primary psychiatric disorders, clinical depression, or central sleep-wake disorders requiring Cognitive Behavioral Therapy for Insomnia (CBT-I) or polysomnography.
- Severe Morning Ataxia: Dizziness, loss of balance, or muscular uncoordination upon waking, particularly in older adults, indicating potential accumulation of sedative metabolites or interaction with other CYP1A2/GABAergic medications.
¶ Drug and supplement interactions
Careful evaluation of drug-supplement interactions is necessary when incorporating sleep optimization compounds into existing therapeutic regimens.
¶ Pharmacokinetic Interactions
- CYP1A2 Metabolism: Because melatonin is metabolized predominantly by the cytochrome P450 enzyme CYP1A2, any co-administered drug that inhibits CYP1A2 (such as fluvoxamine, cimetidine, or caffeine) will dramatically increase circulating melatonin levels and prolong its sedative effects [2:11][17:2]. Conversely, CYP1A2 inducers (such as rifampin or tobacco smoke) will accelerate melatonin clearance and diminish its therapeutic efficacy.
¶ Pharmacodynamic Interactions
- GABAergic Sedatives: Combining valerian root or high-dose melatonin with pharmaceutical GABAergic sedatives (such as benzodiazepines, Z-drugs, or alcohol) can result in additive central nervous system depression, marked by severe drowsiness and impaired psychomotor performance.
- Stimulant Opposing Effects: Adenosine receptor antagonists, such as caffeine, elevate sympathetic arousal and disrupt sleep architecture. Co-administration of L-theanine has been shown to physiologically counter these stimulant-induced disturbances, improving objective sleep-related outcomes by modulating downstream GABAergic and glutamatergic pathways [17:3].
¶ Combining Sleep Optimization with other supplements (“stacks”)
Interventions are frequently stacked to target multiple complementary physiological pathways simultaneously.
¶ The "Sleep Starter Kit" Stack
A highly popular and clinically relevant stack combines:
- Apigenin (from Chamomile extract): Acts as a mild GABA-A receptor agonist, initiating physical relaxation.
- L-Theanine: Blockades excitatory glutamate receptors, quieting mental chatter and reducing sympathetic tone [17:4][18:1][5:10].
- Magnesium: Blocks NMDA receptors and supports baseline neuromuscular relaxation.
This triad targets three separate inhibitory pathways, promoting rapid sleep onset and deeper slow-wave sleep without next-day grogginess [15:3][28][18:2].
¶ Cannabidiol (CBD) and L-Theanine
Combined administration of CBD and L-theanine demonstrates synergistic efficacy in reversing caffeine-induced sleep disturbances. Preclinical models show that this combination is superior to either agent alone at restoring lost non-rapid eye movement (NREM) sleep and reducing sleep fragmentation [17:5].
¶ Valerian and Hops
A highly validated botanical combination (such as the standardized Ze 91019 formulation) that leverages hops' ability to enhance valerian's binding affinity to GABA-A receptors, resulting in increased slow-wave sleep and improved next-day cognitive and psychological parameters [9:4].
¶ Practical questions (FAQ)
¶ 1. How long does it take for sleep supplements to work?
L-theanine and sublingual melatonin work rapidly, typically within 30 to 60 minutes of ingestion. Valerian root, however, may require consistent nightly use for 2 to 4 weeks to achieve cumulative therapeutic benefits on sleep architecture [7:4][8:3][4:1].
¶ 2. Can I take melatonin long term?
Clinical trials in children with ADHD and neurodevelopmental disorders show that melatonin remains safe and effective for up to several years of continuous use. However, for general sleep optimization, cycling or maintaining low doses (0.3–1.0 mg) is recommended to prevent receptor desensitization and daytime drowsiness [2:12][3:5].
¶ 3. Is melatonin useful if I am otherwise healthy?
Yes, but mainly for jet lag, shift work, or when attempting to shift your sleep schedule. If sleep timing is normal and there are no sleep onset complaints, exogenous melatonin is unlikely to provide significant benefit and may cause morning sleepiness [10:9][11:8].
¶ 4. Why does high-dose melatonin sometimes make my sleep worse?
Doses above 3–5 mg exceed physiological saturation levels for MT1 and MT2 receptors. This hypermelatoninemia can cause prolonged receptor binding, leading to next-day grogginess, early waking, and a disrupted circadian phase response curve [10:10][11:9].
¶ 5. What are the best non-supplement alternatives for insomnia?
Cognitive Behavioral Therapy for Insomnia (CBT-I) is the gold-standard first-line therapy for chronic insomnia. Non-pharmacological physical interventions such as laser acupuncture and self-administered acupressure are also highly feasible and clinically validated options [14:4][25:1][26:1].
¶ How we evaluated the evidence
This clinical monograph was prepared by evaluating human clinical evidence across a strict pyramid of scientific authority:
- High Certainty: Multiple randomized, double-blind, placebo-controlled trials and systematic reviews demonstrating consistent benefits of melatonin and L-theanine for reducing sleep latency in pediatric and adult cohorts [2:13][5:11].
- Moderate Certainty: Well-designed clinical trials or systematic reviews with moderate sample sizes, such as valerian extracts for insomnia in hemodialysis patients [7:5] and standardized valerian-hops formulations [9:5].
- Low Certainty: Evidence with high individual variability or conflicting outcomes, such as dietary and herbal supplements for Restless Legs Syndrome [13:3] or melatonin for post-surgical orthopedic recovery [12:1].
- Very Low Certainty: Hypothesized mechanisms supported primarily by in-silico molecular docking models or preclinical animal experiments [17:6][19:1].
¶ References
Chandler-Mather N, Shelton D, Donovan C, Till H, Theroux BM, Dawe S. (2026). A Pilot Randomised Controlled Trial of Sublingual Melatonin for Sleep Onset Insomnia in Children With Foetal Alcohol Spectrum Disorder (FASD). Journal of Paediatrics and Child Health. https://pubmed.ncbi.nlm.nih.gov/41122831/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Paditz E, Renner B, Koch R. (2025). The Pharmacokinetics, Dosage, Preparation Forms, and Efficacy of Orally Administered Melatonin for Non-Organic Sleep Disorders in Autism Spectrum Disorder During Childhood and Adolescence: A Systematic Review. Children (Basel). https://pubmed.ncbi.nlm.nih.gov/40426828/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Akerström T, et al. Exercise induces IL‑6 release from human skeletal muscle; role in lipid metabolism. Am J Physiol Endocrinol Metab. 2005;288:E733‑E740. https://journals.physiology.org/doi/full/10.1152/ajpendo.00340.2004 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Rocha NS, Correa RDESA, Dias ACM. (2023). Association between sleep pattern and pharmacological treatment in children with attention deficit disorder with hyperactivity: a systematic review. Revista Paulista de Pediatria. https://pubmed.ncbi.nlm.nih.gov/37255110/ ↩︎ ↩︎
Hidese S, Ogawa S, Ota M, Ishida I, Yasukawa Z, Ozeki M, Kunugi H. (2019). Effects of L-Theanine Administration on Stress-Related Symptoms and Cognitive Functions in Healthy Adults: A Randomized Controlled Trial. Nutrients. https://pubmed.ncbi.nlm.nih.gov/37255110/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lyon MR, Kapoor MP, Juneja LR. (2011). The effects of L-theanine (Suntheanine®) on objective sleep quality in boys with attention deficit hyperactivity disorder (ADHD): a randomized, double-blind, placebo-controlled clinical trial. Alternative Medicine Review. https://pubmed.ncbi.nlm.nih.gov/22214254/ ↩︎ ↩︎ ↩︎ ↩︎
Tammadon MR, Nobahar M, Hydarinia-Naieni Z, Ebrahimian A, Ghorbani R, Vafaei AA. (2021). The Effects of Valerian on Sleep Quality, Depression, and State Anxiety in Hemodialysis Patients: A Randomized, Double-blind, Crossover Clinical Trial. Oman Medical Journal. https://pubmed.ncbi.nlm.nih.gov/39064758/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Riebe D, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update. Circulation. 2023;147(14):1128-1151. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001189 ↩︎ ↩︎ ↩︎ ↩︎
Seldin MM, et al. Myonectin (CTRP15), a novel myokine that links skeletal muscle to systemic lipid homeostasis. J Biol Chem. 2012;287(15):11968‑11980. https://www.jbc.org/article/S0021-9258(20)50094-2/fulltext ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hardeland R. (2021). Divergent Importance of Chronobiological Considerations in High- and Low-dose Melatonin Therapies. Diseases. https://pubmed.ncbi.nlm.nih.gov/40426828/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Green DJ, et al. The Potential Role of Contraction‑Induced Myokines in Metabolic Regulation. Front Endocrinol (Lausanne). 2017;8:97. https://www.frontiersin.org/articles/10.3389/fendo.2017.00097/full ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Haider MA, Lawrence KW, Christensen T, Schwarzkopf R, Macaulay W, Rozell JC. (2025). Does Melatonin Improve Sleep Following Primary Total Hip Arthroplasty? A Randomized, Double-Blind, Placebo-Controlled Trial. The Journal of Arthroplasty. https://pubmed.ncbi.nlm.nih.gov/40383169/ ↩︎ ↩︎
González-Parejo P, Martín-Núñez J, Cabrera-Martos I. (2024). Effects of Dietary Supplementation in Patients with Restless Legs Syndrome: A Systematic Review. Nutrients. https://pubmed.ncbi.nlm.nih.gov/39064758/ ↩︎ ↩︎ ↩︎ ↩︎
Zhao FY, Yue LP, Ho YS. (2026). Development of a Stepped-Care Pathway for Managing Willis-Ekbom Disease/Restless Legs Syndrome During Pregnancy: A Best Evidence Synthesis. Nature and Science of Sleep. https://pubmed.ncbi.nlm.nih.gov/42344604/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wrann CD, et al. Exercise induces hippocampal BDNF via a PGC‑1α/FNDC5 pathway. Cell Metab. 2013;18(5):649‑659. https://www.cell.com/cell-metabolism/fulltext/S1550-4131(13)00372-3 ↩︎ ↩︎ ↩︎ ↩︎
Roberts LD, et al. β‑Aminoisobutyric acid induces browning of white fat and hepatic β‑oxidation. Cell Metab. 2014;19(1):96‑108. https://www.cell.com/cell-metabolism/fulltext/S1550-4131(13)00478-0 ↩︎
Kim KH, Lee MS, et al. Acute exercise induces FGF21 in mice and humans. PLoS One. 2013;8(5):e63517. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0063517 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Verdijk LB, et al. Skeletal muscle hypertrophy following resistance training is accompanied by a fiber type-specific increase in satellite cell content in elderly men. J Gerontol A Biol Sci Med Sci. 2009;64(3):332-339. https://pubmed.ncbi.nlm.nih.gov/28698222/ ↩︎ ↩︎ ↩︎
Rao RR, et al. Meteorin‑like regulates beige fat thermogenesis. Cell. 2014;157(6):1279‑1291. https://www.cell.com/fulltext/S0092-8674(14)00578-3 ↩︎ ↩︎
Mitsui K, Saeki K, Sun M. (2024). Effects of a violet-excitation light-emitting diode on melatonin secretion and sleepiness: preliminary findings from a randomized controlled trial. Journal of Clinical Sleep Medicine. https://pubmed.ncbi.nlm.nih.gov/37707296/ ↩︎
Singh S, Keller PR, Busija L. (2023). Blue-light filtering spectacle lenses for visual performance, sleep, and macular health in adults. The Cochrane Database of Systematic Reviews. https://pubmed.ncbi.nlm.nih.gov/37593770/ ↩︎
McPherron AC, Lawler AM, Lee SJ. Regulation of skeletal muscle mass by a new TGF‑β family member (myostatin). Nature. 1997;387:83‑90. https://www.nature.com/articles/387083a0 ↩︎
Huh JY, et al. Irisin stimulates muscle growth‑related genes and regulates adipocyte metabolism in humans. Int J Obes (Lond). 2014;38:1538‑1544. https://www.nature.com/articles/ijo201442 ↩︎
Izumiya Y, et al. FGF21 is an Akt‑regulated myokine. FEBS Lett. 2008;582(27):3805‑3810. https://febs.onlinelibrary.wiley.com/doi/full/10.1016/j.febslet.2008.10.021 ↩︎
Assar A, Walker J, Egeler M. (2026). Estimating Public Knowledge About Cognitive Behavioral Therapy for Insomnia (CBT-I) and Alternative Treatments. Behavioral Sleep Medicine. https://pubmed.ncbi.nlm.nih.gov/41479226/ ↩︎ ↩︎
Zhao FY, Zhang WJ, Chow CM. (2025). From Needles to Photons: Clinical Efficacy, Safety, and Mechanistic Insights of Laser Acupuncture in Insomnia Management. Nature and Science of Sleep. https://pubmed.ncbi.nlm.nih.gov/41356808/ ↩︎ ↩︎
Zhao FY, Zhang WJ, Chow CM. (2025). Task-Shifting from Acupuncturists to Nurses in Delivering Acupuncture/Acupressure or Supervising Patient Self-Administered Acupressure for Sleep Management: Is It Feasible? Nature and Science of Sleep. https://pubmed.ncbi.nlm.nih.gov/41230390/ ↩︎ ↩︎
Aoi W, Naito Y, Yoshikawa T. SPARC and exercise‑linked suppression of colon tumorigenesis. Gut. 2013;62(6):882‑889. https://gut.bmj.com/content/62/6/882.long ↩︎