¶ Vitamin B12
| Type | Essential Water-Soluble Vitamin |
| Active Cmpd | Methylcobalamin, Adenosylcobalamin |
| Source | Animal products, Bacteria, Fortified foods |
| Dose Range | 2.4 mcg (RDA) to 2,000 mcg (Therapeutic) |
| Half-life | Approx. 6 days (serum); months to years (liver stores) |
| Main Benefit | Neurological function, RBC formation, DNA synthesis |
| Absorption | Complex (Intrinsic Factor-dependent + Passive Diffusion) |
Vitamin B12 (cobalamin) is an essential, cobalt-containing water-soluble vitamin required for DNA synthesis, erythropoiesis, and the maintenance of the myelin sheath in the central nervous system. It is uniquely synthesized by bacteria and obtained primarily through animal-derived foods or supplementation.
¶ At a glance
Aliases
- Also known as: Cobalamin, Cyanocobalamin, Methylcobalamin, Adenosylcobalamin, Hydroxocobalamin.
- Chemical / botanical name: Cobalamin.
- Category: Essential B-complex vitamin.
Key points (high-level summary)
- Universal Efficacy for Deficiency: High-dose oral B12 (≥1,000 mcg) is clinically equivalent to intramuscular injections for correcting deficiency, regardless of absorption etiology.[1], [2]
- Homocysteine Reduction: Supplementation reliably lowers plasma homocysteine by 25–30%, though this translates to modest stroke risk reduction rather than broad cardiovascular protection.[3], [4], [5]
- Neuroprotective Limitations: While critical for preventing neurological damage, high-dose B12 does not reverse existing [[pages/cognitive-decline|cognitive decline]] in patients without baseline deficiency.[6], [7]
- Metformin & PPI Risks: Chronic use of [[supplements/metformin|metformin]] or gastric acid inhibitors significantly increases the risk of clinical and subclinical B12 deficiency.[1:1], [8], [9]
What people use it for
- Main goals: Cognitive health, nerve repair, anemia prevention, homocysteine lowering, energy support.
- Evidence quality (overall): High (for deficiency and homocysteine); Low to Moderate (for age-related cognitive decline).
¶ What is Vitamin B12?
Vitamin B12 is a structurally complex organometallic compound characterized by a central cobalt atom within a corrin ring. It is the only vitamin that contains a trace mineral element.
- Definition: A water-soluble vitamin that serves as a vital coenzyme in two major metabolic pathways: the conversion of homocysteine to methionine and the conversion of methylmalonyl-CoA to succinyl-CoA.
- Natural sources: Exclusively synthesized by bacteria. Humans obtain it from meat, fish, poultry, eggs, and dairy products. Plant-based diets require fortified foods or supplements.
- Traditional / historical use: Its discovery stemmed from research into pernicious anemia, a once-fatal autoimmune condition characterized by the inability to absorb B12.
- Current regulatory status: Dietary supplement (worldwide); Prescription drug (injections and high-dose formulations for clinical deficiency).
- Key pharmacological property: Essential enzymatic cofactor for one-carbon metabolism and mitochondrial energy production.
¶ What are Vitamin B12’s main benefits?
Vitamin B12 is most clinically significant for its role in correcting megaloblastic anemia and preventing irreversible subacute combined degeneration of the spinal cord.
-
Outcome: Plasma Homocysteine Reduction
-
Direction of effect: Decrease
-
Magnitude: Moderate to Large (25–30% reduction)
-
Population studied: Adults with hyperhomocysteinemia, CVD history, or healthy elderly.
-
Evidence quality: High (Numerous Meta-analyses)
-
Summary sentence: B12, often in combination with folate, is the most effective intervention for lowering elevated homocysteine levels.[5:1]
-
Outcome: Treatment of B12 Deficiency Anemia
-
Direction of effect: Decrease (Correction of symptoms)
-
Magnitude: Large
-
Population studied: Children and adults with nutritional or malabsorptive deficiency.
-
Evidence quality: High (Systematic Reviews)
-
Summary sentence: Both oral and parenteral routes effectively normalize hematological parameters and mean corpuscular volume (MCV).[10], [11]
-
Outcome: Neuroprotection in Mild Cognitive Impairment (MCI)
-
Direction of effect: No consistent effect / Unclear
-
Magnitude: Small
-
Population studied: Elderly with MCI and high homocysteine.
-
Evidence quality: Moderate
-
Summary sentence: Supplementation may slow brain atrophy in specific high-homocysteine subgroups but has not shown consistent cognitive benefits across general aging populations.[6:1], [12]
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Homocysteine Reduction | High | High | 50+ RCTs | 250–1,000 mcg/day reduces Hcy by ~25% in diverse populations [5:2] | |
| Correction of B12 Deficiency | High | High | 20+ RCTs | Oral dose ≥1,000 mcg/day is equal to IM injection [2:1], [11:1] | |
| Stroke Risk Reduction | Moderate | Moderate | 15+ RCTs | B-vitamin combos show ~10% reduction in stroke risk [3:1], [4:1] | |
| Cognitive Decline (MCI/AD) | High | High | 10+ RCTs | No significant improvement in cognitive scores without baseline deficiency [6:2], [7:1], [12:1] | |
| Depression Symptoms | Low | Low | 5 RCTs | Mixed results; may be beneficial as adjunctive therapy in those with low B12 [13], [14] | |
| Diabetic Neuropathy | Moderate | Low | 7 RCTs | Methylcobalamin may modestly improve nerve conduction and pain [15] | |
| Herpetic Neuralgia Pain | Moderate | Moderate | 4 RCTs | Local or systemic B12 may reduce pain associated with shingles [16] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome.
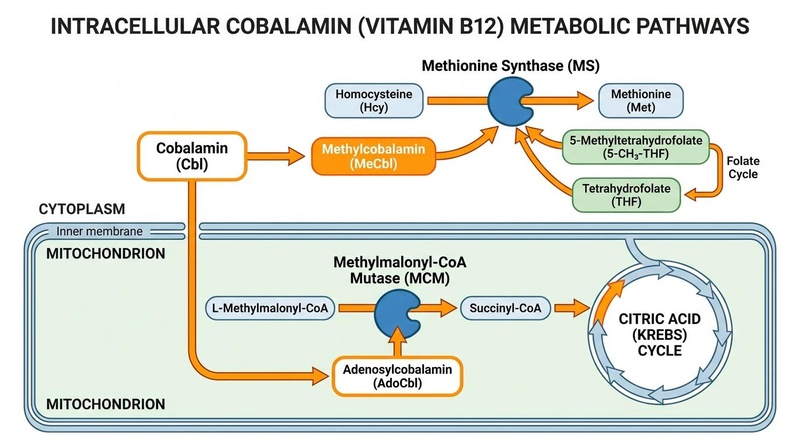
¶ How does Vitamin B12 work?
Vitamin B12 acts through two distinct coenzyme forms in different cellular compartments.
- Primary targets: Methionine Synthase (cytosol) and L-Methylmalonyl-CoA Mutase (mitochondria).
- Core mechanisms:
- Methylation Pathway: As methylcobalamin, it transfers a methyl group to homocysteine, forming methionine and regenerating tetrahydrofolate (THF). This is essential for DNA/RNA synthesis and the production of S-adenosylmethionine (SAMe), the universal methyl donor.[17]
- Mitochondrial Pathway: As adenosylcobalamin, it facilitates the conversion of methylmalonyl-CoA to succinyl-CoA. Failure of this step leads to the accumulation of methylmalonic acid (MMA), which disrupts myelin synthesis and causes neurological dysfunction.[18], [17:1]
- Pharmacokinetics:
- Absorption: Dietary B12 requires gastric acid to be released from protein, followed by binding to Intrinsic Factor (IF) in the duodenum and absorption in the terminal ileum via receptor-mediated endocytosis.
- Passive Diffusion: Approximately 1% of an oral dose is absorbed via passive diffusion throughout the intestine, allowing high-dose oral supplements (e.g., 1,000 mcg) to bypass IF requirements.[19], [20]
- Forms: Cyanocobalamin is the most stable synthetic form. Methylcobalamin and Adenosylcobalamin are the naturally occurring active coenzymes. Sublingual and oral administration routes show equivalent bioavailability to intramuscular injections at high doses.[2:2]
¶ Effects on different systems
¶ Metabolic & Endocrine Health
The most significant metabolic interaction involves [[supplements/metformin|Metformin]], the first-line treatment for Type 2 Diabetes. [[supplements/metformin|Metformin]] interferes with the calcium-dependent absorption of the B12-IF complex. Meta-analyses show that up to 30% of long-term [[supplements/metformin|metformin]] users develop B12 deficiency, with risks increasing with dose and duration.[8:1], [9:1], [21] Periodic screening is recommended for this population.[22]
¶ Cardiovascular & Vascular Health
B12 is a primary regulator of homocysteine. While lowering homocysteine reduces stroke risk, it has not shown significant benefits for reducing myocardial infarction or overall vascular mortality in major clinical trials like SEARCH or HOPE-2.[23], [3:2], [4:2] In critical care, high-dose hydroxocobalamin is used to treat refractory shock and vasoplegia by inhibiting nitric oxide and sequestering hydrogen sulfide.[24], [25]
¶ Brain & Mental Health
- Cognition: Low B12 is associated with faster brain atrophy and [[pages/cognitive-decline|cognitive decline]]. However, supplementation trials in healthy elderly or those with AD have largely failed to demonstrate cognitive improvement.[6:3], [7:2], [26]
- Psychiatric Disorders: Low B12 status is linked to depression, autism, and suicidality.[27], [13:1], [14:1]
- Nitrous Oxide Toxicity: Recreational use of nitrous oxide ("whippets") causes rapid oxidation of the B12 cobalt atom, rendering the vitamin inactive and leading to acute, life-threatening neurological and psychiatric symptoms despite "normal" total B12 serum levels.[28], [29]
¶ Pregnancy & Child Development
Maternal B12 status is a critical determinant of child neurodevelopment. Deficiency during pregnancy is associated with an increased risk of neural tube defects, global developmental delay, and impaired cognitive outcomes in the offspring.[30], [31], [18:1], [32], [33]
¶ Other Clinical Domains
- Ophthalmology: B12 may have supportive roles in treating Dry Eye Disease and Optic Neuritis.[34], [35]
- Hypervitaminosis B12: High serum B12 levels (>1,000 pg/mL) in the absence of supplementation can be a "red flag" for underlying systemic disease, including liver cirrhosis, hematological malignancies, and solid tumors, and is associated with increased mortality.[36], [37], [38]
¶ Dosage and how to take it
Standard dosing in studies
- Maintenance: 2.4 mcg/day (RDA).
- Therapeutic (Deficiency): 1,000–2,000 mcg daily (oral or sublingual) for 1–3 months, then 1,000 mcg weekly.
- Homocysteine Management: 400–1,000 mcg daily, usually in combination with 400–800 mcg of folate.
Forms and bioavailability
- Cyanocobalamin: Most stable and cost-effective form; widely used in clinical trials.
- Methylcobalamin: Biologically active form; often preferred in neuropathy studies.
- Hydroxocobalamin: Used for high-dose clinical treatment (shock, cyanide poisoning) and as a long-acting injectable.
- Absorption: Passive diffusion allows high-dose oral intake to be as effective as injections.[2:3] Absorption is not significantly affected by food, though gastric acid inhibitors (PPIs) impair absorption of food-bound B12.[1:2], [39]
Special populations
- Vegans/Vegetarians: Essential for lifelong supplementation to avoid severe deficiency.[40], [41]
- Bariatric Patients: High risk of deficiency due to reduced IF and gastric acid; requires high-dose or parenteral supplementation.[42], [43]
- Elderly: Reduced gastric acid (atrophic gastritis) makes supplements more reliable than dietary sources.[44], [20:1]
¶ Safety and side effects
Common side effects