¶ Mobility: Deep Dive
| Primary Target | Active Range of Motion (AROM) & Fascial Hydration |
| Mechanisms | Fascial "Slide-and-Glide", Capsular Extensibility, Reciprocal Inhibition |
| Dosing Schedule | Daily micro-doses (CARs) + 2-3 sessions/week targeted mobility |
| Safety Profile | Extremely Safe (avoid high-velocity in hypermobile cohorts) |
| Key Markers | Comfortable Gait Speed, Active ROM angles, Timed Up and Go (TUG) |
| Est. Cost | $0 (Free, optional roller or ball $15-$30) |
Mobility is the neuromuscular ability to actively move a joint through its full available range of motion with coordination and control. Unlike passive flexibility, which measures the static extent to which a joint can be stretched by an external force, mobility represents active physical capacity. Developing and maintaining mobility is a vital countermeasure to the structural stiffening of aging, protecting gait speed, maintaining dynamic balance, and supporting functional independence over the lifespan.
¶ At a glance
¶ Key Takeaways
- Active Over Passive: Static flexibility programs do not consistently lower sports injury rates, whereas active range-of-motion (mobility) training under tension stimulates structural tissue remodeling and enhances joint stability [1][2].
- The Gliding Fascial Network: Immobility and aging dry out the deep fascial layers, causing pathological cross-linking. Active mobility training drives local tissue rehydration (imbibition) and stimulates fibroblasts to restore optimal "slide-and-glide" mechanics [3][4].
- Neuromuscular Calibration: Mobility gains are governed by the nervous system. Techniques like Proprioceptive Neuromuscular Facilitation (PNF) leverage autonomic reflexes (such as reciprocal and autogenic inhibition) to reset the motor pool and safely extend range of motion [5][6].
- The Balance-Mobility Link: Recent meta-analyses confirm that integrating advanced movement training (such as perturbation-based exercises) significantly improves real-world mobility, Timed Up and Go (TUG) speed, and postural stability while slashing fall incidence in older adults by large margins [7].
¶ Target Goals & Evidence Quality
- Main Clinical Target: Expansion of active pain-free range of motion, restoration of joint capsule space, and prevention of age-related declines in gait velocity and postural control.
- Evidence Quality: High (supported by extensive systematic reviews of stretching biomechanics, high-resolution shear wave elastography of deep fascia, and clinical meta-analyses of functional mobility in aging cohorts).
¶ Safety "Traffic Light"
- ● GREEN LIGHT (Go): Desk workers experiencing occupational stiffness, aging adults looking to preserve independent walking mechanics, and athletes seeking to optimize movement efficiency and force production.
- ● YELLOW LIGHT (Caution): Individuals with diagnosed joint hypermobility syndromes (e.g., Ehlers-Danlos Syndrome). Avoid aggressive passive stretching or end-range pushing; restrict activities to controlled, muscle-driven joint stabilization and strength-focused ranges [8][9].
- ● RED LIGHT (Stop/Avoid): Individuals with acute joint inflammation, unhealed fractures, unstable joint structures, or severe osteoporotic bone fragility prone to micro-fracture during high-force end-range loading.
¶ Protocol Card
| Parameter | Morning Controlled Articular Rotations (CARs) | Post-Exercise PNF Mobilizer | Self-Myofascial Release (SMR) |
|---|---|---|---|
| Frequency | Daily (upon waking or pre-workout) | 2–3 times per week | Daily or as needed |
| Duration | 5–10 minutes total | 10–15 minutes | 1–2 minutes per muscle group |
| Primary Tasks | Perform slow, isolated joint circles (neck, shoulders, hips, spine) at 10% max effort. | Hold-relax stretching targeting hamstrings, hips, and calves. | Slow, sustained rolling (1-2 cm/sec) on target muscle groups (quadriceps, calves, thoracic spine). |
| Safety Setup | Move slowly and deliberately; do not push through sharp pain, pinching, or closing-angle joint discomfort. | Perform after a warm-up or workout when tissues are warm. Do not stretch to the point of tearing or intense muscle guarding. | Maintain moderate pressure (RPE 4-6 out of 10); avoid bony landmarks, nerves, and vascular structures. |
¶ Bottom Line
Active mobility training is a clinically validated intervention for reducing tissue stiffness, enhancing active range of motion, and preserving gait speed. Pairing neuromuscular stretching with progressive balance perturbations yields optimal functional outcomes in older adults, protecting them from the "longevity cliff" of catastrophic falls [10][11][7:1].
¶ The "Why" (Benefits)
¶ Preventing Age-Related Mobility Restrictions
Aging is naturally associated with a progressive loss of joint range of motion and an increase in skeletal muscle and connective tissue stiffness. This deconditioning is often driven by a sedentary lifestyle, leading to changes in the extracellular matrix of deep fascia:
- Deconditioning of the Joint Capsule: Static postures lead to posterior joint capsule contractures and decreased joint space, which can accelerate degenerative conditions like osteoarthritis. Target-level capsular stretching (such as the "sleeper stretch") has been shown to reduce localized stiffness [12][13].
- Preserving Functional Gait Velocity: Active range-of-motion training at long muscle lengths increases structural sarcomeres-in-series, maintaining muscle length and preventing the "shuffling" gait pattern typical of late-stage physical decline [14][15].
¶ Mitigating Fall Risk through Dynamic Control
Mobility is not merely an aesthetic quality; it is a critical component of dynamic balance and postural recovery:
- Timed Up and Go (TUG) Improvement: Systematic reviews of older adults demonstrate that incorporating active balance and mobility interventions significantly improves performance on the TUG test, which is a powerful predictor of functional independence [7:2].
- Rapid Perturbation Recovery: When a slip or trip occurs, a senior's safety depends on their ability to execute a rapid, wide-angle recovery step. This response requires both joint mobility to reach the necessary landing angle and explosive muscle power to decelerate the falling center of mass [7:3].
¶ Reality Check & Clinical Context
¶ Mouse Biomechanics vs. Human Erect Posture
While rodent models are valuable in understanding tissue-level collagen expression and cellular fibroblast signaling, preclinical mobility and balance research does not directly translate to bipedal human biomechanics:
- Quadrupedal vs. Bipedal Load: Rodents distribute their weight across four limbs and do not experience the high-angle, gravity-challenged sagittal and frontal plane instabilities of erect bipedal standing.
- Foot-Ground Interface: The mechanics of the human ankle joint complex, the plantar fascia windlass mechanism, and the deep crural fascial systems are unique to erect walking. Consequently, clinical guidelines for human mobility and postural control must be built upon human trials, shear wave elastography, and functional movement outcomes [16][10:1][4:1].
¶ Static Stretching Does Not Prevent Injuries
For decades, athletes were instructed to perform prolonged, passive static stretches before workouts to "prevent injury." Modern clinical research has completely debunked this practice:
- No Injury Protection: Large-scale systematic reviews of randomized controlled trials demonstrate that pre-activity static stretching alone has no protective effect on injury incidence (Relative Risk: 0.96) [2:1].
- Performance Deficits: Static stretches held for longer than 60 seconds temporarily reduce muscle power, maximum voluntary contraction force, and explosive jump height by dampening the spinal reflex loop [1:1][17].
- The Active Solution: Modern pre-exercise protocols emphasize dynamic stretching and active joint mobilization, which prime the neuromuscular system without reducing force-generating capacity [1:2][14:1].
¶ Practical Integration
¶ Daily Movement Snacks: Breaking Sedentary Cross-Linking
To maintain fascial health, movement must be distributed throughout the day. Prolonged sitting causes local dehydration and collagen cross-linking in the posterior hip and lower back:
- The 60-Minute Reset: For every hour of sitting, perform 1–2 minutes of joint mobilization (e.g., active standing hip extension or gentle thoracic spine extensions).
- Hydration Dynamics: Regular, gentle movement breaks stimulate "imbibition" (the mechanical squeezing and subsequent reabsorption of water within the fascial ground substance), keeping the tissues hydrated and sliding smoothly [3:1][18].
¶ Mechanism of Action
¶ Fascial "Slide-and-Glide" Biomechanics
Deep fascia is a highly organized, three-dimensional network of dense connective tissue that wraps and connects muscles, nerves, and blood vessels:
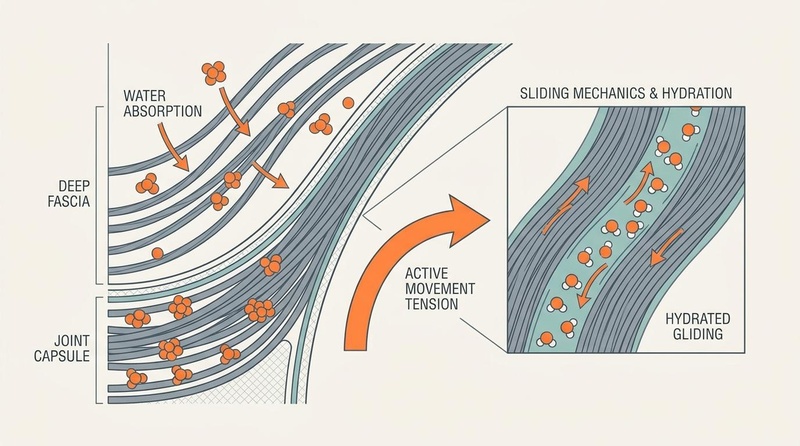
- The Hyaluronic Acid Lubricant: Specialized cells within the fascia, known as fasciacytes, synthesize hyaluronic acid (HA). Hyaluronic acid acts as a molecular lubricant, allowing adjacent fascial layers (such as the epimysium and deep aponeurotic fascia) to slide over one another during muscle contraction [4:2].
- The Viscoelastic "Squeeze-and-Release": Under mechanical tension (such as dynamic stretching), water is squeezed out of the fascial ground substance. Once the tension is released, the tissue absorbs fluid in an expanded volume. This process, called imbibition, temporarily reduces local tissue viscosity, promoting fascial glide and reducing perceived stiffness [3:2][10:2].
- Preventing Pathological Cross-Linking: In states of immobility, the ground substance becomes viscous and dehydrated, allowing collagen fibers to form random, disorganized cross-links that lock the joints in a restricted state [4:3][19].
Figure 1: Neuromuscular and fascial adaptations during active mobility vs. passive stretching.
¶ Neurophysiological Reflex Loops
Mobility gains are heavily regulated by nervous system protective reflexes:
- Autogenic Inhibition (Golgi Tendon Organs): When a muscle is contracted isometrically under tension (as in the contraction phase of a PNF stretch), the Golgi Tendon Organs (GTOs) detect the high mechanical load. The GTOs send inhibitory signals to the spinal cord, causing the muscle's alpha motor neurons to quiet down. This allows the muscle to relax and be moved into a deeper, pain-free range of motion immediately afterward [6:1].
- Reciprocal Inhibition (Muscle Spindles): When an agonist muscle contracts, the nervous system simultaneously sends inhibitory signals to its antagonist muscle, causing it to relax. For example, actively contracting the hip flexors and quadriceps during a hamstring stretch suppresses hamstring motor unit activation, facilitating greater elongation [6:2].
- Stretch Tolerance Calibration: Chronic mobility training does not necessarily permanently change the physical length of the muscle-tendon unit; rather, it recalibrates the brain's "stretch tolerance," allowing the individual to safely access end-range zones without triggering a protective, painful muscle contraction [17:1].
¶ Evidence Summary Table (human outcomes)
| Outcome / Goal | Typical Effect | Consistency | Evidence Quality | Supporting Studies | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Active Range of Motion (ROM) | High | High | Behm 2016, Pedrosa 2025 | Significant, lasting increases in joint angles when training is performed at long muscle lengths [1:3][11:1] | |
| Deep Fascia Stiffness Reduction | High | High | Warneke 2024, Schleip 2012 | 15–20% immediate reduction in fascial stiffness measured by shear wave elastography [3:3][10:3] | |
| Functional Mobility (TUG Speed) | High | High | Mohammadi 2025 | Significant improvements in Timed Up and Go (TUG) speed and gait velocity in older adults [7:4] | |
| Fall Rate Reduction | High | High | Mohammadi 2025, Lauersen 2014 | Highly significant reduction in fall rates when balance challenge/perturbation is combined with active range-of-motion [2:2][7:5] | |
| Joint Pain Alleviation | High | High | Hu 2026 | Clinically meaningful reductions in osteoarthritic joint pain and improved daily function using PNF protocols [5:1] | |
| Stretch Tolerance Calibration | High | Moderate | Hayes 2012, Ikeda 2025 | Increased comfort and passive/active joint excursion without immediate reflex muscle guarding [14:2][17:2] |
¶ Comprehensive Safety & Clinical Guidelines
¶ Absolute Contraindications
- Acute Orthopedic Trauma: Avoid mobilizing areas with unhealed fractures, acute muscle strains, or ligament sprains.
- Infectious Arthritis or Joint Infection: Do not mobilize joints during acute infectious flares.
- Severe Osteoporotic Compression: High-force end-range spinal mobilization is absolutely contraindicated in patients with severe osteoporosis due to fracture risk [8:1].
¶ Relative Contraindications (Requires Adaptation)
- Joint Hypermobility (Ehlers-Danlos / HSD): Patients with lax connective tissues must completely avoid passive end-range stretching. Training must focus strictly on neuromuscular joint stabilization, strength within a controlled range, and proprioceptive control (such as Pilates) [8:2][9:1].
- Moderate Joint Osteoarthritis: Modify ranges to avoid sharp pinching pain; prioritize smooth, controlled articular rotations to circulate synovial fluid and nourish cartilage [5:2][12:1].
¶ Comparisons & Engagement
¶ "Compare With": Active Mobility vs. Alternative Modalities
| Modality | Active Range-of-Motion Gain | Fascial Hydration (Imbibition) | Neuromuscular Control | Performance Safety | Cost / Setup |
|---|---|---|---|---|---|
| Active Mobility Training | Superior | Excellent | Excellent | Superior (no power loss) | Extremely Low ($0) |
| Passive Static Stretching | Good (passive only) | Moderate | Poor | Poor (reduces pre-workout power) | Extremely Low ($0) |
| Foam Rolling (SMR) | Moderate (acute only) | Excellent | Poor | Excellent (restores ROM safely) | Low ($15 - $30) |
| Yoga / Tai Chi | Excellent | Very Good | Excellent | Excellent | Low |
¶ Actionable Protocols
¶ Protocol 1: Controlled Articular Rotations (CARs) Routine
Perform this routine daily upon waking or as a warm-up to maintain joint capsule health and stimulate synovial fluid production [12:2][13:1][11:2].
[Start: Upright Standing Posture]
│
▼ (Keep torso still, rotate neck in wide circle)
[Cervical CARs: 5 slow reps per direction]
│
▼ (Draw largest possible circle with shoulder joint)
[Glenohumeral CARs: 5 slow reps per direction]
│
▼ (Trace a wide circle with hip joint on one leg)
[Hip CARs: 5 slow reps per direction]
│
▼ (Trace a circle with ankle joint, moving foot)
[Ankle CARs: 5 slow reps per direction]
- Step 1: Stand upright, brace your core, and create "irradiation" (light full-body muscular tension, about 10-20% effort) to isolate movement to the target joint.
- Step 2 (Cervical): Tuck your chin, rotate your head slowly toward one shoulder, tilt your ear back, rotate across to the other shoulder, and return to center. Repeat 5 times per side.
- Step 3 (Shoulder): Raise one arm straight overhead, rotate your palm outward as you reach backward, draw a large circle, and return to your side. Repeat 5 times per side.
- Step 4 (Hip): Balance on one leg (hold a wall for support). Lift your opposite knee toward your chest, open it wide to the side, rotate your foot upward while driving your knee backward, and circle back to center. Repeat 5 times per side.
¶ FAQ
¶ What is the difference between mobility and flexibility?
Flexibility is the passive ability of a joint and surrounding muscles to move through a range of motion, usually assisted by an external force (such as a partner or gravity). Mobility is the active, neuromuscular ability to control and move a joint through its full available range of motion under muscle-driven force and tension [1:4][2:3].