¶ Posture and Postural Alignment: Deep Dive
| Primary Target | Spinal Alignment & Muscle Balance |
| Mechanisms | Motor Control, Myofascial Balance, Joint Centration |
| Dosing Schedule | Daily postural breaks + 2-3 sessions/week corrective training |
| Safety Profile | Extremely Safe (with proper progressive loading) |
| Key Markers | Craniovertebral Angle (CVA), Thoracic Kyphosis Angle |
| Est. Cost | $0 (Free, optional resistance band $10) |
Posture and postural alignment represent the mechanical relationship between musculoskeletal structures and the forces of gravity. Maintaining optimal alignment is critical for preventing degenerative joint diseases, maintaining pulmonary capacity, and ensuring pain-free functional movement over the lifespan.
¶ At a glance
¶ Key Takeaways
- More Than Aesthetics: Postural misalignment (e.g., hyperkyphosis, forward head posture) is a structural stressor associated with decreased respiratory efficiency, compromised gait stability, and chronic tension.
- The Upper Crossed Syndrome: The modern sedentary environment drives a predictable pattern of muscular imbalance—tightness in the pectoral and upper neck muscles crossing with weakness in the deep cervical flexors and lower/middle trapezius.
- The Power of Corrective Exercise: Systematic strength and stretching protocols consistently restore joint angles (like the Craniovertebral Angle) but must be paired with lifestyle integration and motor control re-education to yield lasting clinical and functional benefits.
- Age-Related Decline: Longitudinal data shows thoracic kyphosis naturally increases and spinal range of motion decreases over a 10-year period in aging populations, making active resistance training a vital countermeasure.
¶ Target Goals & Evidence Quality
- Main Clinical Target: Correction of Forward Head Posture (FHP), rounded shoulders, thoracic hyperkyphosis, and associated chronic cervical/thoracic neck pain.
- Evidence Quality: Moderate to High (supported by multiple systematic reviews and meta-analyses of randomized controlled trials).
¶ Safety "Traffic Light"
- ● GREEN LIGHT (Go): Individuals seeking to reverse sedentary-induced "tech neck," desk workers looking to reduce neck/shoulder fatigue, and older adults hoping to halt age-related thoracic hyperkyphosis.
- ● YELLOW LIGHT (Caution): Individuals with diagnosed cervical or lumbar radiculopathy, osteoporotic vertebral compression fractures, or structural (non-postural) scoliosis. Training must avoid high-velocity maneuvers and focus on gentle, isometric, pain-free stabilization.
- ● RED LIGHT (Stop/Avoid): Individuals with acute cervical or thoracic spinal fractures, severe spinal cord compression (myelopathy), or unstable spinal joints.
¶ Protocol Card
| Parameter | FHP & Upper Crossed Protocol | Thoracic Kyphosis Protocol | Workplace Postural Snack |
|---|---|---|---|
| Frequency | 3 sessions per week | 2-3 sessions per week | Every 60 minutes of sitting |
| Duration | 15–20 minutes per session | 15–20 minutes per session | 1–2 minutes |
| Primary Tasks | Craniocervical flexion isometrics (chin tucks), scapular retraction with bands, and chest stretching. | Prone extension exercises, thoracic foam rolling, and door-frame chest openers. | Chin tucks, scapular squeezes, and stand-and-reach overhead. |
| Safety Setup | Perform slowly; stop immediately if sharp pain or numbness radiates down the arms. | Restrict foam rolling to the thoracic spine; do not roll the lumbar spine aggressively. | Ensure chair is stable before performing dynamic stretches. |
¶ Bottom Line
Targeted corrective exercises strongly improve postural metrics (such as increasing the craniovertebral angle and reducing the kyphotic angle), but their ability to automatically resolve chronic pain depends on active lifestyle modification and consistent movement variability.
¶ The "Why" (Benefits)
¶ Reversing the Structural Cost of Sedentary Life
Modern occupational environments encourage prolonged, static flexion of the cervical and thoracic spine, colloquially known as "text neck" or "tech neck" [1]. This prolonged loading alters the biomechanics of the upper quadrant:
- Increased Structural Load: For every inch of forward head translation, the relative weight of the head on the cervical spine increases by approximately 10 pounds, accelerating disc degeneration and myofascial strain.
- Restoring the Craniovertebral Angle (CVA): Systematic reviews confirm that specific strengthening of the deep cervical stabilizers combined with pectoral stretching significantly increases the CVA, drawing the head back over the center of mass and reducing muscular strain [2][3].
¶ Maximizing Respiratory Efficiency
A critical, often overlooked consequence of poor postural alignment is its direct impact on pulmonary function. A hyperkyphotic, rounded-shoulder posture physically restricts the expansion of the rib cage and the excursion of the diaphragm.
- Impaired Breathing Mechanics: Randomized trials demonstrate that individuals with Upper Crossed Syndrome (UCS) exhibit reduced vital capacity and forced expiratory volume [4].
- Dynamic Efficiency: New clinical trials demonstrate that kyphotic posture significantly reduces respiratory efficiency during dynamic tasks like walking and running, leading to early fatigue and higher cardiovascular strain [3:1]. Corrective exercise interventions that reduce the thoracic kyphotic angle successfully improve lung capacity and respiratory muscle performance [4:1].
¶ Reality Check & Clinical Context
¶ Muscular Realignment vs. Automatic Pain Cure
While corrective exercises are highly effective at changing joint angles and improving alignment metrics, the relationship between posture and pain is complex.
- The Alignment Illusion: A high-quality meta-analysis in 2026 revealed that while corrective exercise programs strongly improve anatomical posture (such as reducing the forward head angle), they do not always produce a corresponding decrease in pain or functional limitation when compared to general, non-specific physical exercise [5].
- The Core Clinical Lesson: Posture is dynamic. Maintaining a "perfect" rigid posture is not the goal; rather, the goal is building a highly adaptable, resilient musculoskeletal system that can handle varied loads and avoid prolonged static positions. Corrective exercise works best when integrated into a lifestyle that prioritizes regular movement breaks [5:1][6].
¶ Corrective Exercise vs. Orthoses
For older adults suffering from age-related thoracic hyperkyphosis, passive spinal orthoses (braces) are often prescribed. However, systematic reviews indicate that while orthoses can temporarily reduce the kyphotic angle, they do not consistently improve long-term muscle activation or balance [7]. Active, progressive exercise programs remain the gold standard for driving neuro-muscular remodeling and long-term functional independence [7:1][8].
¶ Practical Integration
¶ Reconditioning the Upper Crossed Imbalance
The structural imbalances of the upper body follow Janda’s classic Upper Crossed Syndrome model, which is highly prevalent in desk-bound populations [6:1]. This model outlines an intersection of overactive (tight) and underactive (weak) muscle groups:
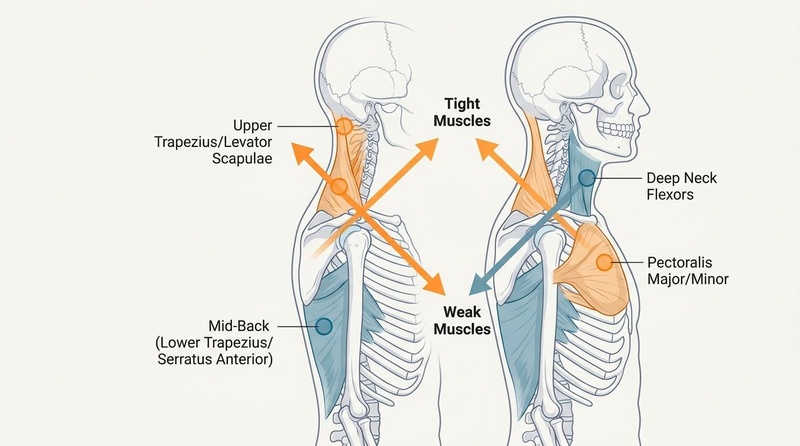
Figure 1: Upper Crossed Syndrome diagonals. Orange denotes overactive/tight groups, blue-grey indicates underactive/weak groups.
- Overactive (Tight) Muscles (Stretching Target): Upper trapezius, levator scapulae, pectoralis major, and pectoralis minor.
- Underactive (Weak) Muscles (Strengthening Target): Deep cervical flexors (longus colli, longus capitis), lower and middle trapezius, and serratus anterior.
Corrective programs must target both sides of this crossed loop to achieve lasting postural centration [6:2][9].
¶ Mechanism of Action
¶ Neural Restructuring of Cervical Proprioception
Asymptomatic forward head posture is associated with impaired cervical proprioception (the brain's awareness of where the neck is in space). Chronic lengthening of the deep cervical muscles desensitizes muscle spindles, leading to a sluggish joint-position sense and increased error in coordinating neck movements [10].