¶ TL;DR
- Diverse Presentation: Facial redness encompasses transient flushing, persistent erythema, visible broken capillaries (telangiectasia), and inflammatory papules/pustules, each requiring distinct approaches [1].
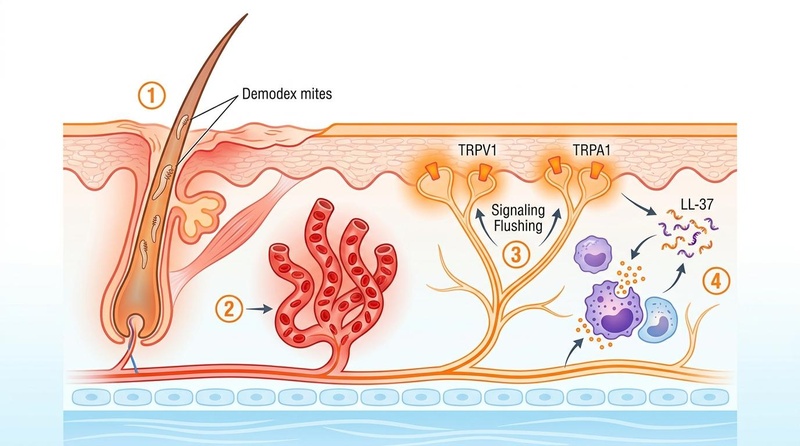
- Core Pathophysiology: Rosacea involves neurovascular dysregulation, innate immune activation (especially cathelicidin LL-37 and kallikrein-5), Demodex folliculorum mites, and TRP channel sensitivity (TRPV1, TRPA1) [2][3][4][5].
- Effective Topicals: Azelaic acid (15-20%), metronidazole (0.75-1%), and ivermectin (1%) are first-line topical treatments for inflammatory lesions, with ivermectin often showing superior efficacy for papulopustular types [6][7].
- Clinical Interventions: Vascular lasers (PDL, KTP, IPL) are highly effective clinical procedures for persistent redness and telangiectasias [8][9], while low-dose oral doxycycline (40mg sub-antimicrobial) is the key systemic therapy for inflammatory rosacea [10][11].
- Avoid Triggers: Strict avoidance of known triggers (heat, spicy food, alcohol, UV exposure) and harsh skincare is foundational for managing all forms of facial redness [12].
¶ Quick Answer
Managing facial redness, rosacea, and broken capillaries effectively requires a precise understanding of the specific type of redness and its underlying causes. For inflammatory rosacea (papules and pustules), topical treatments like azelaic acid, metronidazole, or ivermectin are often the first line of defense, targeting inflammation and Demodex mites [6:1]. For persistent background redness and visible broken capillaries (telangiectasias), vascular lasers (e.g., Pulsed Dye Laser, KTP, IPL) offer the most effective long-term solutions by selectively targeting blood vessels [8:1]. Oral sub-antimicrobial dose doxycycline can address systemic inflammation in more severe cases [10:1]. A gentle skincare routine, strict sun protection, and trigger avoidance are crucial for all forms of redness [12:1].
¶ Type-Identification Table
Accurate identification of redness type is critical for effective management.
| Type of Redness | Description | Key Features | Common Triggers | Intervention Path |
|---|---|---|---|---|
| Transient Erythema (Flushing) | Temporary reddening of the face, often accompanied by a feeling of warmth or burning. | Comes and goes, can be intense; often symmetrical on cheeks/nose. | Heat, spicy foods, alcohol, exercise, stress, hot drinks. | Trigger avoidance, soothing topicals, oral beta-blockers (off-label for severe flushing). |
| Persistent Erythema (Permanent Redness) | Constant background redness, primarily on the central face, not resolving spontaneously. | Diffuse, persistent redness; often a precursor to telangiectasia. | Genetic predisposition, chronic inflammation, UV exposure. | Vascular lasers (PDL, KTP, IPL), topical brimonidine/oxymetazoline (temporary). |
| Telangiectasia (Broken Capillaries / Spider Veins) | Visible, permanently dilated small blood vessels near the skin surface. | Fine red or purplish lines, often branched; do not blanch with pressure. | Chronic UV exposure, genetic factors, rosacea, trauma. | Vascular lasers (PDL, KTP, IPL) are primary treatment. |
| Inflammatory Papules/Pustules (Rosacea Bumps) | Red bumps (papules) and pus-filled lesions (pustules) similar to acne, but without comedones. | Red, tender bumps; can appear in crops; concentrated on central face. | Demodex mites, innate immune dysfunction, certain foods. | Topical azelaic acid, metronidazole, ivermectin; oral doxycycline. |
| Phymatous Rosacea | Thickening of skin, irregular surface nodules, often affecting the nose (rhinophyma). | Enlarged, bumpy, disfigured nose (rhinophyma); skin thickening on cheeks, chin, forehead. | Chronic untreated rosacea. | Surgical excision, CO2 laser resurfacing. |
¶ Evidence Snapshot Table (Human Outcomes)
| Intervention | Outcome | Effect | Quality | Consistency | Trials | Notes |
| :--- | :--- | :--- | :--- | :--- | :--- |
| Topical Azelaic Acid (15-20%) | Reduction in inflammatory lesions (papules/pustules) |
| Topical Metronidazole (0.75-1%) | Reduction in inflammatory lesions (papules/pustules) |
| Topical Ivermectin (1%) | Reduction in inflammatory lesions (papules/pustules) |
| Oral Doxycycline (40 mg sub-antimicrobial) | Reduction in inflammatory lesions (papules/pustules) |
| Vascular Lasers (PDL, KTP, IPL) | Reduction in persistent erythema and telangiectasia |
| Topical Brimonidine (0.33%) / Oxymetazoline (1%) | Temporary reduction in facial erythema |
| Centella Asiatica / Madecassoside | Reduction in redness, improved skin barrier |
| Oral Isotretinoin (low-dose) | Reduction in severe inflammatory rosacea |
| Topical Niacinamide | Reduction in facial redness, barrier support |
¶ Causes Tied to Biology & Anatomy
Redness, rosacea, and broken capillaries are rooted in a complex interplay of genetic, environmental, and immunological factors that disrupt skin homeostasis.
-
Neurovascular Dysregulation:
- Vasodilation: The blood vessels in the skin become overly reactive, leading to exaggerated flushing responses and persistent dilation. This can be triggered by various stimuli (heat, spicy food, alcohol, stress).
- TRP Channels: Transient Receptor Potential (TRP) channels, particularly TRPV1 (activated by heat, capsaicin, UV) and TRPA1 (activated by cold, irritants), are overexpressed or hypersensitive in rosacea patients [4:1][22]. Their activation leads to neuronal signaling and local vasodilation, contributing to flushing and burning sensations.
-
Innate Immune System Activation:
- Cathelicidin LL-37 and Kallikrein-5: Patients with rosacea exhibit aberrant expression and processing of cathelicidin, an antimicrobial peptide. Normally, cathelicidin is cleaved by enzymes like kallikrein-5 (KLK5) into fragments. In rosacea, increased KLK5 activity leads to an overproduction of pro-inflammatory LL-37 fragments, which trigger inflammation, vasodilation, and angiogenesis (new blood vessel formation) [2:1][3:1].
- Toll-Like Receptor 2 (TLR2): Elevated expression of TLR2 on immune cells in rosacea skin can lead to an exaggerated inflammatory response to stimuli, including microbial antigens.
-
Demodex folliculorum Mites:
- These microscopic mites are a normal component of skin flora, but their density is significantly higher in rosacea patients [5:1]. Demodex mites and the bacteria (Bacillus oleronius) they carry are thought to trigger innate immune responses and inflammation through the release of bacterial antigens and waste products, contributing to papule and pustule formation.
-
Structural Weakness in Microvascular Walls (Telangiectasia):
- Chronic inflammation, UV exposure, and genetic predispositions can weaken the delicate walls of superficial capillaries. This structural compromise leads to their permanent dilation and visible appearance as broken capillaries or spider veins (telangiectasia). The persistent vasodilation and inflammatory processes contribute to this vascular fragility.
¶ Starter Protocol
An effective starter protocol for managing redness and rosacea focuses on gentle care, barrier support, and strict avoidance of identified triggers.
DAILY GENTLE ROUTINE AT-A-GLANCE
- Morning: Ultra-Gentle Cleanser → Soothing Serum (e.g., Centella Asiatica, Niacinamide) → Mineral Sunscreen (SPF 30+, Zinc Oxide/Titanium Dioxide)
- Evening: Ultra-Gentle Cleanser → Soothing Serum → Barrier-Repair Moisturizer
The starter protocol emphasizes:
-
Ultra-Gentle Cleansing:
- Purpose: To remove impurities without irritating sensitive skin or disrupting the compromised skin barrier. Harsh cleansers can exacerbate redness and inflammation.
- Protocol: Use a non-foaming, pH-balanced, fragrance-free cleanser with lukewarm water twice daily. Avoid scrubbing or hot water. Gently pat skin dry with a soft, clean towel.
-
Soothing & Barrier-Supporting Serums:
- Purpose: To reduce inflammation, calm redness, and provide antioxidants while supporting the skin's natural barrier function.
- Protocol: Apply a serum containing ingredients like Centella Asiatica (Madecassoside) [19:1][20:1], niacinamide [^Draelos2005], or green tea extract. These can help reduce erythema and strengthen the skin barrier.
-
Strict Physical Mineral UV Protection:
- Purpose: UV radiation is a major trigger for rosacea flares and contributes to microvascular damage, accelerating the formation of telangiectasias. Mineral sunscreens are generally better tolerated than chemical ones for sensitive skin.
- Protocol: Apply a broad-spectrum mineral sunscreen with SPF 30 or higher (containing zinc oxide and/or titanium dioxide) every morning as the last step of the routine, and reapply as needed throughout the day.
-
Barrier-Repair Moisturizer:
- Purpose: To replenish skin lipids, reduce transepidermal water loss (TEWL), and protect the skin from environmental irritants, which is crucial for managing redness and sensitive skin.
- Protocol: Use a fragrance-free, non-comedogenic moisturizer containing ceramides, hyaluronic acid, or colloidal oatmeal nightly after cleansing and serums.
-
Trigger Avoidance:
- Purpose: Identifying and avoiding personal triggers is foundational for managing rosacea.
- Protocol: Keep a diary to track potential triggers, which commonly include spicy foods, hot beverages, alcohol, extreme temperatures, strong winds, certain cosmetics, and stress.
¶ Stronger Add-On Path
If the gentle starter protocol does not adequately control redness and inflammatory lesions, prescription-strength topical medications can be introduced under medical guidance.
-
Topical Azelaic Acid (15% gel or 20% cream):
- Mechanism: Possesses anti-inflammatory, antimicrobial, and mild comedolytic properties. It specifically targets the overproduction of cathelicidin and KLK5 in rosacea pathogenesis [23][2:2].
- Protocol: Apply a thin layer to affected areas twice daily. Often well-tolerated, but some initial stinging or itching may occur.
- Notes: Effective for both inflammatory lesions and the erythema of rosacea [12:3].
-
Topical Metronidazole (0.75% or 1% gel/cream/lotion):
- Mechanism: An antimicrobial and anti-inflammatory agent that reduces inflammatory lesions (papules and pustules) of rosacea. Its exact anti-inflammatory mechanism in rosacea is not fully understood but involves reactive oxygen species scavenging [14:1].
- Protocol: Apply a thin layer to affected areas once or twice daily.
- Notes: A long-standing first-line treatment for papulopustular rosacea.
-
Topical Ivermectin (1% cream):
- Mechanism: Exerts both anti-inflammatory effects and a direct acaricidal (mite-killing) action against Demodex folliculorum, which are implicated in rosacea pathogenesis [15:1].
- Protocol: Apply a pea-sized amount to the entire face once daily, typically in the evening.
- Notes: Clinical trials have shown superior efficacy to metronidazole in reducing inflammatory lesions and improving quality of life in patients with papulopustular rosacea [7:2][24].
¶ Clinical/Procedure Path
For persistent redness, visible telangiectasias, or severe inflammatory rosacea unresponsive to topical therapies, professional clinical interventions are necessary.
¶ Systemic Medical Treatments
-
Oral Doxycycline (Sub-antimicrobial Dose):
- Mechanism: At a low dose (e.g., 40 mg modified-release once daily), doxycycline acts primarily through anti-inflammatory pathways (e.g., inhibiting matrix metalloproteinases, reducing inflammatory cytokines) rather than its antibiotic properties [10:3][11:2].
- Protocol: Prescription only, typically 40 mg once daily. Long-term use is common for inflammatory rosacea.
- Notes: Specifically formulated to provide anti-inflammatory effects without contributing to antibiotic resistance.
-
Oral Isotretinoin (Low-Dose):
- Mechanism: While primarily an acne medication, low-dose oral isotretinoin can be used off-label for severe, recalcitrant papulopustular rosacea or phymatous rosacea. It reduces sebum production, normalizes follicular keratinization, and has anti-inflammatory properties [13:2].
- Protocol: Prescription only, typically 10-20 mg daily or every other day, under strict dermatological supervision due to potential side effects.
- Notes: Reserved for severe cases due to its systemic side effect profile and need for monitoring.
¶ Clinical Procedures
-
Vascular Lasers (Pulsed Dye Laser (PDL), KTP Laser, Intense Pulsed Light (IPL)):
- Mechanism: These light-based therapies specifically target hemoglobin in dilated blood vessels, causing selective photothermolysis without damaging surrounding tissue. PDL (585-595 nm) is considered the gold standard for redness, while KTP (532 nm) and IPL (broad-spectrum, filtered) are also highly effective for telangiectasias and diffuse erythema [8:3][9:2].
- Protocol: Multiple sessions are typically required (3-5+), spaced several weeks apart. Patients may experience temporary bruising (purpura) with PDL or mild redness/swelling with IPL/KTP.
- Notes: The most effective treatments for permanent facial redness and broken capillaries.
-
Surgical Intervention (for Rhinophyma):
- Mechanism: For advanced phymatous rosacea, particularly rhinophyma (nose enlargement), surgical debulking and reshaping are necessary. Techniques include scalpel excision, CO2 laser resurfacing, electrosurgery, and dermabrasion to remove thickened tissue and restore nasal contour [25].
- Protocol: Performed by a dermatologist or plastic surgeon. Multiple modalities may be combined.
- Notes: Early intervention is key to prevent severe disfigurement.
¶ What Fails
Certain approaches can worsen redness, rosacea, and capillary fragility, making the condition more difficult to manage.
-
Physical Scrubs or Aggressive Chemical Exfoliants (High-Strength AHA/BHA):
- Why they fail: These physically abrade or chemically strip the skin barrier, increasing inflammation, sensitivity, and redness. Rosacea skin has a compromised barrier, which cannot tolerate harsh exfoliation.
- Outcome: Exacerbated erythema, burning, stinging, and potential for increased flares.
-
High-Strength Ascorbic Acid (L-Ascorbic Acid) Serums:
- Why they fail: While Vitamin C is beneficial, high concentrations (especially >10-15%) of L-Ascorbic Acid can be highly acidic and irritating to sensitive, rosacea-prone skin, leading to redness and stinging.
- Outcome: Increased irritation and reactive redness. gentler forms like sodium ascorbyl phosphate or magnesium ascorbyl phosphate may be tolerated better.
-
Steroid-Induced Rosacea:
- Why it fails: Prolonged or inappropriate use of topical corticosteroid creams on the face can lead to a rosacea-like eruption. Initially, steroids may reduce redness, but chronic use causes paradoxical worsening, skin thinning, telangiectasias, and rebound flares upon withdrawal [26][27].
- Outcome: Severe rebound erythema, papules, pustules, skin atrophy, and increased vascular fragility. Requires careful, tapered withdrawal under medical supervision.
-
Treating Rosacea Papules/Pustules as Standard Acne:
- Why it fails: While rosacea can present with "acne-like" bumps, it is not acne. Using typical acne treatments like high-strength benzoyl peroxide, salicylic acid, or aggressive retinoids without considering rosacea's unique pathophysiology can severely damage the compromised skin barrier and worsen inflammation.
- Outcome: Significant irritation, dryness, increased redness, and a lack of improvement in rosacea symptoms.
¶ Tracking Plan
Systematic tracking helps monitor progress, identify triggers, and evaluate the effectiveness of interventions over time.
-
Flush Frequency and Intensity Diary (Daily):
- Metric: Document the number, duration, and intensity (1-10 scale) of flushing episodes each day.
- Notes: Record potential triggers encountered prior to each flush (e.g., specific foods, stress, temperature changes).
-
Erythema Index / Redness Scale (Weekly/Bi-weekly):
- Metric: Use a standardized clinical erythema grading scale (e.g., from 0 = clear to 4 = severe redness) or self-assessment with consistent lighting and background.
- Notes: Consistent self-photography under identical lighting conditions (e.g., bathroom mirror, same time of day) can provide objective visual documentation of changes over 3-6 months.
-
Lesion Counts (Bi-weekly for Papulopustular Rosacea):
- Metric: Count the number of inflammatory papules and pustules on predefined facial areas (e.g., forehead, each cheek, chin, nose).
- Notes: Track separately from non-inflammatory bumps.
-
Skin Barrier Integrity Assessment (Monthly):
- Metric: Subjective assessment of dryness, tightness, peeling, and sensitivity. Tools like a corneometer can objectively measure hydration and TEWL if available.
- Notes: Aim for reduced sensitivity and improved comfort as indicators of barrier health.
¶ Safety & Red Flags
Understanding potential adverse effects and recognizing critical warning signs is essential for individuals managing redness and rosacea.
-
Rebound Erythema (from Brimonidine/Oxymetazoline):
- Concern: Topical vasoconstrictors like brimonidine (Mirvaso®) and oxymetazoline (Rhofade®) temporarily reduce redness by constricting blood vessels. However, upon wearing off, some individuals experience a "rebound effect" where redness returns worse than baseline, potentially with severe flushing and burning [18:1].
- Action: Use with caution. If rebound occurs, discontinue use and focus on soothing, barrier-repairing treatments.
-
Steroid-Induced Rosacea:
- Concern: Misuse or prolonged use of potent topical corticosteroids on the face can induce a rosacea-like dermatitis, characterized by persistent redness, papules, pustules, increased skin fragility, and severe flares upon withdrawal [26:1][27:1].
- Action: Avoid applying topical steroids to the face unless specifically prescribed and monitored by a dermatologist for a very short duration. If steroid-induced rosacea is suspected, seek medical advice for a careful, tapered withdrawal and alternative management.
-
Rhinophyma Progression (Phymatous Rosacea):
- Concern: In severe, long-standing rosacea, particularly in men, the skin of the nose can thicken and enlarge (rhinophyma). This disfigurement results from sebaceous gland hyperplasia and connective tissue overgrowth.
- Action: Early recognition and treatment of inflammatory rosacea are crucial. If rhinophyma develops, surgical intervention (e.g., laser ablation, scalpel excision) is often necessary to restore nasal contour [25:1]. Regular dermatological check-ups are important.
-
Ocular Rosacea:
- Concern: Rosacea can affect the eyes, causing symptoms like dryness, irritation, redness, a gritty sensation, sensitivity to light, and blurred vision. If left untreated, severe cases can lead to corneal damage.
- Action: Any new or worsening eye symptoms in a person with facial rosacea warrant prompt ophthalmological evaluation. Treatment often involves warm compresses, lid hygiene, artificial tears, and sometimes oral doxycycline.
¶ FAQs
What is the difference between rosacea and acne?
While both rosacea and acne can cause red bumps and pustules, a key differentiator is the absence of comedones (blackheads and whiteheads) in rosacea [13:3]. Rosacea primarily involves facial redness, flushing, and vascular changes, whereas acne is characterized by clogged pores, sebum overproduction, and Cutibacterium acnes bacteria [12:4]. The underlying inflammatory pathways also differ, with rosacea often linked to innate immune dysfunction and Demodex mites [2:3].
Can diet impact rosacea?
Yes, diet can influence rosacea symptoms for many individuals. Common dietary triggers include spicy foods, hot beverages, and alcohol, which can induce flushing and exacerbate redness [12:5]. While specific dietary recommendations vary, identifying and avoiding personal triggers through a food diary can significantly help manage symptoms.
Are broken capillaries (telangiectasias) the same as rosacea?
Telangiectasias, or visible broken capillaries, are a common feature of rosacea, particularly the erythematotelangiectatic subtype [1:1]. However, telangiectasias can also occur independently due to factors like sun damage, genetics, or trauma. While they are often associated with chronic rosacea, not everyone with telangiectasias has rosacea, and vice versa.
How do I prevent rosacea flares?
Preventing rosacea flares primarily involves consistent trigger avoidance, a gentle skincare routine, and daily sun protection [12:6]. Identifying and avoiding personal triggers (e.g., heat, spicy foods, alcohol, stress, harsh skincare products, UV exposure) is crucial. Using mild, non-irritating cleansers and moisturizers, along with broad-spectrum mineral sunscreen, helps maintain skin barrier integrity and reduce reactivity.
What are vascular lasers, and how do they work for redness?
Vascular lasers, such as Pulsed Dye Laser (PDL), KTP laser, and Intense Pulsed Light (IPL), are light-based therapies that specifically target and heat the hemoglobin within dilated blood vessels without damaging the surrounding skin [8:4]. This process, called selective photothermolysis, causes the abnormal blood vessels to coagulate and be reabsorbed by the body, leading to a significant reduction in persistent facial redness and visible broken capillaries [9:3]. Multiple sessions are typically required for optimal results.
¶ References
van Zuuren, E. J., et al. Interventions for rosacea based on the phenotype approach: an updated systematic review including GRADE assessments. British Journal of Dermatology. 2019. https://academic.oup.com/bjd/article/181/1/65/6747190 ↩︎ ↩︎
Muto, Y., et al. Increased Expression of Cathelicidin by Direct Activation of Protease-Activated Receptor 2: Possible Implications on the Pathogenesis of Rosacea. Journal of Investigative Dermatology. 2014. https://ncbi.nlm.nih.gov/pmc/articles/PMC4205707/ ↩︎ ↩︎ ↩︎ ↩︎
Yamasaki, K., et al. Accelerated processing of cathelicidin by kallikrein-5 in the stratum corneum promotes rosacea. Nature Medicine. 2007. https://pubmed.ncbi.nlm.nih.gov/17982468/ ↩︎ ↩︎
Sulk, M., et al. Distribution and Expression of Non-Neuronal Transient Receptor Potential (TRPV) Ion Channels in Rosacea. Experimental Dermatology. 2012. https://ncbi.nlm.nih.gov/pmc/articles/PMC3305847/ ↩︎ ↩︎
Zelenkova, B., & Kazandjieva, J. Rosacea as a manifestation of Demodex mite infestation. Advances in Dermatology and Allergology. 2015. https://pmc.ncbi.nlm.nih.gov/articles/PMC4509536/ ↩︎ ↩︎
Li, Z., et al. The efficacy and safety of minocycline, metronidazole, ivermectin, and azelaic acid in moderate-to-severe papulopustular rosacea: A systematic review and network meta-analysis. ScienceDirect. 2024. https://www.sciencedirect.com/science/article/pii/S2666328724000075 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Taieb, A., et al. Superior Efficacy with Ivermectin 1% Cream Compared to Metronidazole 0.75% Cream Contributes to a Better Quality of Life in Patients with Severe Papulopustular Rosacea: A Subanalysis of the Randomized, Investigator-Blinded ATTRACT Study. Dermatology and Therapy. 2015. https://pmc.ncbi.nlm.nih.gov/articles/PMC4972739/ ↩︎ ↩︎ ↩︎
Zhai, C., et al. Meta‐Analysis of the Efficacy of Intense Pulsed Light and Pulsed‐Dye Laser Therapy in the Management of Rosacea. Journal of Cosmetic Dermatology. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11626304/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kakar, R., & Sahoo, L. K. Efficacy and safety of intense pulsed light in rosacea: A systematic review. Indian Journal of Dermatology, Venereology and Leprology. 2023. https://ijdvl.com/efficacy-and-safety-of-intense-pulsed-light-in-rosacea-a-systematic-review/ ↩︎ ↩︎ ↩︎ ↩︎
Dohlman, M., et al. Long‐term inflammatory rosacea management with subantibiotic dose oral doxycycline 40 mg modified‐release capsules once daily. Journal of Cosmetic Dermatology. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9285068/ ↩︎ ↩︎ ↩︎ ↩︎
Del Rosso, J. Q., et al. Effectiveness and safety of doxycycline 40 mg (30-mg immediate-release and 10-mg delayed-release beads) once daily as add-on therapy for papulopustular rosacea. Journal of the American Academy of Dermatology. 2010. https://pubmed.ncbi.nlm.nih.gov/21229827/ ↩︎ ↩︎ ↩︎
British Association of Dermatologists guidelines for the management of people with rosacea 2021. British Journal of Dermatology. 2021. https://academic.oup.com/bjd/article/185/4/725/6599936 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
van Zuuren, E. J., et al. Interventions for rosacea: abridged updated Cochrane systematic review including GRADE assessments. British Journal of Dermatology. 2015. https://pubmed.ncbi.nlm.nih.gov/26099423/ ↩︎ ↩︎ ↩︎ ↩︎
Esmann, S., & Jemec, G. B. E. Topical metronidazole for rosacea. Cochrane Database of Systematic Reviews. 2010. https://pubmed.ncbi.nlm.nih.gov/20238318/ ↩︎ ↩︎
Schaller, M., & Dirschka, T. Rosacea: an update in diagnosis and therapy. Journal der Deutschen Dermatologischen Gesellschaft. 2010. https://pubmed.ncbi.nlm.nih.gov/20420790/ ↩︎ ↩︎
Gold, L. S., et al. Anti-inflammatory dose doxycycline (40 mg controlled-release) confers maximum anti-inflammatory efficacy in rosacea. American Journal of Clinical Dermatology. 2010. https://pubmed.ncbi.nlm.nih.gov/17786099/ ↩︎
Draelos, Z. D., et al. Topical Oxymetazoline Hydrochloride Cream 1% for the Treatment of Persistent Facial Erythema of Rosacea in Adults: A Comprehensive Review of Current Evidence. American Journal of Clinical Dermatology. 2018. https://pmc.ncbi.nlm.nih.gov/articles/PMC8021401/ ↩︎
Gold, L. S., et al. Optimizing the use of topical brimonidine in rosacea management: panel recommendations. Journal of Drugs in Dermatology. 2015. https://pubmed.ncbi.nlm.nih.gov/25607906/ ↩︎ ↩︎
Su, Y., et al. The Effectiveness and Safety of a Skin Care Product With Centella asiatica Leaf Extract, Ceramide NP, and Panthenol in Subjects With Sensitive Skin: A Prospective, Observational Study. Journal of Cosmetic Dermatology. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12274965/ ↩︎ ↩︎
Bylka, W., et al. Centella asiatica in cosmetology. Advances in Dermatology and Allergology. 2013. https://pmc.ncbi.nlm.nih.gov/articles/PMC3834700/ ↩︎ ↩︎
Schagen, S. K., & Zampeli, V. A. Topical Application of Centella asiatica in Wound Healing: Recent Insights into Mechanisms and Clinical Efficacy. Molecules. 2020. https://pmc.ncbi.nlm.nih.gov/articles/PMC11510310/ ↩︎
Steinhoff, M., et al. Transient receptor potential (TRP) channels and their role in the skin. American Journal of Clinical Dermatology. 2013. https://pubmed.ncbi.nlm.nih.gov/23720239/ ↩︎
McLane, J. Azelaic acid 15% gel for rosacea. Journal of the American Academy of Dermatology. 2011. https://pubmed.ncbi.nlm.nih.gov/21287959/ ↩︎
Stein Gold, L. F., et al. Long-term safety of ivermectin 1% cream vs azelaic acid 15% gel in treating inflammatory lesions of rosacea: results of two 40-week controlled, investigator-blinded trials. Journal of Drugs in Dermatology. 2014. https://pubmed.ncbi.nlm.nih.gov/25607706/ ↩︎
Karrer, S., et al. A Systematic Review of Surgical Techniques for Management of Severe Rhinophyma. Craniomaxillofacial Trauma & Reconstruction. 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8543596/ ↩︎ ↩︎
Bhat, Y. J., et al. Steroid-induced rosacea: a clinical study of 200 patients. Indian Journal of Dermatology. 2011. https://pmc.ncbi.nlm.nih.gov/articles/PMC3088930/ ↩︎ ↩︎
Kang, M., et al. Clinical and Laboratory Differences between Steroid-associated and Non-steroid-associated Rosacea: A Retrospective Study. Journal of Clinical and Aesthetic Dermatology. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11091907/ ↩︎ ↩︎