¶ SIBO
| Condition Class | Microbiome Dysbiosis / Motility Disorder |
| Primary Gases | Hydrogen ($\text{H}_2$), Methane ($\text{CH}_4$), Hydrogen Sulfide ($\text{H}_2\text{S}$) |
| Diagnostic Standard | Lactulose/Glucose Breath Test, Jejunal Aspirate |
| Key Bio-Mechanisms | Migrating Motor Complex (Phase III) Dysfunction, Visceral Adhesions |
| Eradication Agent | Rifaximin (+ Neomycin/Metronidazole for Methane; Bismuth for $\text{H}_2\text{S}$) |
| Efficacy Rate | 60–85% (varies by gas profile and motility) |
Small Intestinal Bacterial Overgrowth (SIBO) is a pathological condition characterized by the presence of abnormal numbers of bacteria in the small intestine, typically exceeding colony-forming units (CFU) per milliliter of jejunal aspirate [1][2]. While the colon is home to a massive, dense population of anaerobic microbes, the small intestine is biologically structured to maintain low microbial density. A breakdown in protective gastrointestinal barriers allows colonic microbes to migrate retrogradely and proliferate, leading to nutrient malabsorption, mucosal inflammation, and debilitating gas symptoms [3][4].
¶ TL;DR
- Motility Defect is the Core Pathology: SIBO is primarily a symptom of Migrating Motor Complex (MMC) dysfunction—specifically the loss of Phase III "housekeeper" waves during fasting [5][6].
- Gas Profiling Dictates Antimicrobial Selection: Therapy is guided by breath test results: hydrogen-producing SIBO responds to rifaximin, while methane-producing SIBO (IMO) requires combination therapy (rifaximin + neomycin or metronidazole) [7][8].
- Strict Breath Testing Rules Prevent False Positives: Diagnosed via glucose or lactulose breath testing; strict adherence to a 24-hour preparatory diet is mandatory to avoid false positives [9][10].
- Avoid Post-Antibiotic Probiotic Therapy: Introducing high-dose multi-strain probiotics immediately after antibiotics is discouraged, as it can cause rapid re-colonization and symptom relapse in the small bowel [11][12].
- Prokinetics Keep SIBO in Remission: Preventing SIBO recurrence requires stimulating fasting motility with post-treatment prokinetics (e.g., low-dose erythromycin, prucalopride, or ginger-artichoke extracts) [5:1][6:1].
¶ Quick Answer
The clinical management of Small Intestinal Bacterial Overgrowth (SIBO) focuses on identifying the specific gas profile via breath testing, executing targeted antimicrobial eradication, and correcting the underlying motility failure to prevent relapse [13][8:1]. Under the North American Consensus, SIBO is diagnosed by a rise of in hydrogen gas within 90 minutes of carbohydrate ingestion, or a methane concentration of at any point (classified as Intestinal Methanogen Overgrowth, or IMO) [7:1]. Eradication utilizes non-absorbable antibiotics: Rifaximin ( for 14 days) for hydrogen, augmented with Neomycin () or Metronidazole () for methane [7:2][8:2]. To prevent the high rate of recurrence (up to 40% within 3 months), patients must immediately transition to a prokinetic regimen (such as low-dose prucalopride) to restore the Migrating Motor Complex (MMC) "housekeeper" wave [5:2][6:2].
¶ Clinical Protocol Overview
- Diagnostic Threshold: Hydrogen rise $\ge 20\ \text{ppm}$ within 90 mins; Methane peak $\ge 10\ \text{ppm}$ at any point; Hydrogen Sulfide $\ge 3\ \text{ppm}$ at any point [^7][^21].
- Eradication (14 Days):
- Hydrogen: Rifaximin $550\ \text{mg}$ TID + PHGG $5\ \text{g/day}$ [^3][^15].
- Methane (IMO): Rifaximin $550\ \text{mg}$ TID + Neomycin $500\ \text{mg}$ BID (or Metronidazole $250–500\ \text{mg}$ TID) [^7][^8].
- Hydrogen Sulfide: Rifaximin $550\ \text{mg}$ TID + Bismuth Subsalicylate $524\ \text{mg}$ QID [^4][^10].
- Motility Restoration (Bedtime, Fasting): Prucalopride $0.5\ \text{mg}$ QHS OR Low-Dose Erythromycin $50\ \text{mg}$ QHS OR Ginger-Artichoke Blend [^13][^30].
- Dietary Transition (4–8 Weeks): Low-FODMAP, Bi-Phasic, or SIBO Specific diet, followed by systematic, high-fiber reintroduction [^3][^35].
¶ What It Is & Pathophysiology
Small Intestinal Bacterial Overgrowth occurs when the homeostatic mechanisms that restrict bacterial colonization in the small bowel fail. In healthy individuals, the small intestine is kept clear of excessive microbial accumulation through:
- Gastric Acid & Bile: Broad-spectrum chemical barriers that kill ingested microbes [14].
- The Migrating Motor Complex (MMC): Cyclic, sweeping waves of muscular contraction that occur during fasting (specifically Phase III), physically pushing food debris and bacteria down into the colon [5:3][6:3].
- An Intact Ileocecal Valve: A physical, one-way barrier preventing the retrograde reflux of colonic contents back into the terminal ileum [2:1].
- Secretory IgA: Mucosal antibodies that prevent bacterial adherence to the enterocyte wall [12:1].
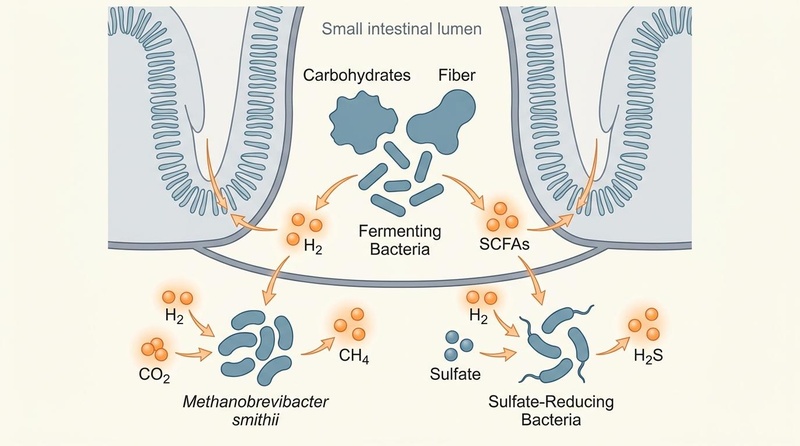
When these defenses are compromised, bacteria colonize the small bowel. They ferment incoming dietary carbohydrates, producing massive volumes of hydrogen (), carbon dioxide (), and methane () gases, causing physical bowel stretching, pain, and altered motility [3:1][7:3].
 failure versus healthy intestinal motility, structural adhesions causing stasis, and retrograde migration of colonic bacteria.")
¶ The Tripartite Gas Dynamics
Our clinical understanding of SIBO has evolved from a single-entity model into a triad of distinct gas-producing dysbiotic profiles, each characterized by a unique microbial ecology, symptom cluster, and therapeutic response [15][16]:
- Hydrogen-Dominant SIBO (): Primarily driven by rapid-fermenting colonic Gram-negative aerobes and facultative anaerobes (e.g., Escherichia coli, Klebsiella pneumoniae, Enterobacter spp.) [3:2][16:1]. These bacteria ferment dietary carbohydrates to produce large amounts of hydrogen gas [13:1]. Clinically, hydrogen-dominant SIBO strongly correlates with hypermotility, secretory diarrhea (IBS-D phenotype), and rapid small bowel transit [13:2][15:1].
- Methane-Dominant Overgrowth / Intestinal Methanogen Overgrowth (IMO): Driven not by bacteria, but by archaea—specifically Methanobrevibacter smithii [7:4][8:3]. Methanogens do not consume carbohydrates directly; instead, they utilize the hydrogen gas produced by neighboring bacteria as a substrate, combining four molecules of with one molecule of to generate one molecule of methane () [7:5]. Methane gas acts as a direct neuromuscular inhibitor in the gastrointestinal tract, suppressing cholinergic transmission and slowing colonic transit by up to 70% [7:6]. This results in the classic constipation-predominant phenotype (IBS-C) and severe postprandial bloating [13:3][15:2].
- Hydrogen Sulfide-Dominant SIBO (): Driven by sulfate-reducing bacteria (SRB), such as Desulfovibrio piger and Bilophila wadsworthia [17][15:3]. These microbes compete directly with methanogens for the hydrogen pool, reducing sulfate to hydrogen sulfide gas () [15:4]. is highly toxic to the gut epithelium, damaging mitochondrial respiration in colonocytes and causing profound visceral hypersensitivity [12:2]. Patients with hydrogen sulfide overgrowth characteristically suffer from severe, burning abdominal pain, urgent watery diarrhea, sulfurous-smelling gas (rotten eggs), halitosis, and systemic symptoms like brain fog and chronic fatigue [17:1][15:5].
¶ Underlying Etiologies: The "Why" behind the Overgrowth
¶ 1. Migrating Motor Complex (MMC) Failure
The MMC is a cyclic, electromechanical pattern of motility that occurs exclusively during fasting, repeating every 90 to 120 minutes [5:4][6:4]. Phase III is the most critical phase, consisting of short, high-amplitude propulsive contractions that sweep from the stomach down to the ileocecal valve, functioning as an intestinal "housekeeper" to clear undigested food and bacteria into the colon [6:5].
A major cause of Phase III MMC failure is Post-Infectious IBS [3:3][12:3]. Following acute gastroenteritis caused by pathogens like Campylobacter jejuni, Salmonella, or Shigella, the patient develops antibodies against Cytolethal Distending Toxin B (CdtB) [3:4][12:4]. Due to molecular mimicry, these anti-CdtB antibodies cross-react with vinculin, a critical cytoskeletal protein in the enteric nervous system and the interstitial cells of Cajal (ICC)—the pacemakers of gut motility [3:5][12:5]. This autoimmune-mediated damage destroys the pacemaking network, crippling Phase III MMC waves and allowing colonic bacteria to migrate retrogradely into the small intestine [12:6][6:6].
¶ 2. Structural Adhesions and Mechanical Stasis
Prior abdominal or pelvic surgeries (e.g., C-sections, appendectomies, cholecystectomies, hysterectomies) or inflammatory conditions (e.g., endometriosis, pelvic inflammatory disease, Crohn's disease strictures) frequently lead to the formation of visceral adhesions [4:1][18]. These fibrous bands of scar tissue compress, tether, or kink loops of the small intestine. Even minor mechanical restrictions create localized segments of slow transit and physical fluid stasis. In these stagnant pockets, bacteria proliferate rapidly, bypassing normal clearing mechanisms and rendering SIBO highly refractory to antibiotic therapy unless the mechanical restriction is addressed [18:1].
¶ 3. Acid Suppression and Hypochlorhydria
Gastric acid acts as a powerful broad-spectrum sterilizing barrier that destroys ingested bacteria, fungi, and viruses [14:1]. The widespread, chronic use of high-dose Proton Pump Inhibitors (PPIs) such as omeprazole or esomeprazole elevates gastric pH above 4.0, neutralizing this barrier [4:2][14:2]. This allows viable oral and environmental bacteria to survive gastric passage and colonize the duodenum and jejunum [14:3]. Long-term PPI use has been demonstrated in multiple clinical trials to significantly increase the risk of developing hydrogen-dominant SIBO [4:3][14:4].
¶ 4. Systemic Hypomotility: Hypothyroidism and Diabetes
Systemic metabolic and endocrine disorders are strong, often overlooked predisposing factors for SIBO:
- Hypothyroidism: Low circulating levels of thyroid hormones ( and ) reduce the transcriptomic and electromechanical excitability of intestinal smooth muscle cells [4:4]. This slows generalized gastrointestinal transit, impairs fasting motility, and frequently leads to severe, chronic SIBO in middle-aged and older adults [4:5].
- Diabetes Mellitus: Chronic hyperglycemia induces microvascular damage and oxidative stress in the autonomic nervous system [4:6]. This leads to diabetic gastroenteropathy and enteric neuropathy, which specifically blunts the vagally mediated activation of Phase III MMC contractions [4:7]. SIBO is exceptionally common in diabetic patients, presenting as alternating diarrhea and constipation, and has a very high rate of post-antibiotic recurrence [4:8][5:5].
¶ Clinical Demographics: Age and Sex Differences
The clinical presentation, underlying etiology, and treatment risks of SIBO vary significantly across different patient populations:
¶ Young Adults (Ages 18–35)
- Prevalent Etiology: Predominantly post-infectious SIBO following acute food poisoning (autoimmune anti-vinculin pathway) [3:6][12:7].
- Sex Distribution: Strong female-to-male ratio (approximately 3:1), matching general IBS trends.
- Presentation: Primarily presents as the hydrogen-dominant or hydrogen sulfide-dominant, diarrhea-predominant phenotype (IBS-D) [15:6]. Young adults often report significant social anxiety, academic impairment, and postprandial distress [11:1].
- Key Considerations: This cohort has the highest response rate to standard rifaximin therapy but also experiences high recurrence rates if post-infectious antibodies remain elevated, requiring aggressive prokinetic therapy [5:6].
¶ Middle-Aged Adults (Ages 36–60)
- Prevalent Etiology: Strongly linked to chronic lifestyle stress (which elevates sympathetic tone and halts parasympathetic-mediated MMC waves), long-term PPI use, and mechanical restrictions such as adhesions from previous abdominal surgeries (C-sections, laparoscopic surgeries) [4:9][14:5].
- Sex Distribution: Women in this age bracket frequently exhibit SIBO secondary to endometriosis or pelvic adhesions [4:10]. Cyclic hormonal changes (progesterone spikes during the luteal phase) can further slow transit, compounding SIBO-C/IMO symptoms. Men are more frequently diagnosed secondary to metabolic syndrome, fatty liver disease, or chronic PPI use for GERD [4:11].
- Key Considerations: Visceral manipulation, myofascial release, and osteopathic manual therapy are highly beneficial in this age group to address surgical scar tissue and adhesions [18:2].
¶ Older Adults (Ages >60)
- Prevalent Etiology: Primarily driven by age-related physiological decline [4:12][18:3]. Older adults experience progressive achlorhydria (natural loss of gastric acid production), decreased enteric neuronal density (loss of ICC cells), and polypharmacy—especially the chronic use of opioids, anticholinergics, and calcium channel blockers, which paralyze intestinal smooth muscle [4:13].
- Sex Distribution: Roughly equal distribution between older men and older women.
- Presentation: SIBO in older adults is frequently "silent" or atypical, presenting as progressive weight loss, steatorrhea (fat malabsorption), fecal urgency, and severe nutrient deficiencies rather than overt painful bloating [1:1][18:4].
- Key Risks: Older adults are highly vulnerable to SIBO-induced macrocytic anemia (due to bacterial consumption of luminal vitamin ) and osteopenia/osteoporosis (due to fat-soluble vitamin D and calcium malabsorption) [1:2][18:5]. Polypharmacy must be carefully audited, and nutritional supplementation (especially sublingual ) should be initiated alongside antimicrobial therapy [18:6].
¶ Does It Work? (Evidence Snapshot)
The clinical management of SIBO involves targeted antimicrobial therapies, the efficacy of which has been established across numerous controlled trials.
¶ Evidence Summary Table (Human Outcomes)
| Intervention | Subtype/Target | Protocol | Clinical Efficacy Rate | Evidence Quality (GRADE) | Supported Study Count | Key Clinical Outcomes & Findings | Row Citation |
|---|---|---|---|---|---|---|---|
| Rifaximin | Hydrogen ()-dominant SIBO | TID () for 14 days | 60–70% gas normalization | High | 10+ RCTs | Promotes hydrogen reduction; significantly reduces abdominal pain and bloating severity [13:4][8:4] | [3:7][13:5][8:5] |
| Rifaximin + Neomycin | Methane ()-dominant SIBO (IMO) | Rifaximin TID + Neomycin BID for 14 days | 75–85% methane eradication | Moderate-High | 3 RCTs | Superior to rifaximin monotherapy; resolves constipation by reducing methane-induced bowel stasis [7:7][8:6] | [7:8][8:7] |
| Rifaximin + Metronidazole | Methane ()-dominant SIBO (IMO) | Rifaximin TID + Metronidazole TID for 14 days | 70–80% methane eradication | Moderate | 2 Clinical Trials | Alternative for neomycin-intolerant patients or those with renal impairment; comparable efficacy [7:9][5:7] | [7:10][5:8] |
| Rifaximin + Bismuth Subsalicylate | Hydrogen Sulfide () SIBO | Rifaximin TID + Bismuth Subsalicylate QID for 14 days | 65–75% eradication (estimated) | Low | 1 Cohort, clinical guidelines | Bismuth binds sulfur in the lumen, starving sulfate-reducing bacteria; alleviates sulfurous gas and diarrhea [11:2][17:2] | [11:3][17:3] |
| Rifaximin + PHGG | All subtypes (mostly Hydrogen) | Rifaximin TID + Partially Hydrolyzed Guar Gum 5\ \text | 87% eradication (vs 62% for rifaximin alone) | Moderate | 2 RCTs | PHGG acts as a prebiotic, stimulating bacterial replication, making them highly susceptible to rifaximin [19][20] | [19:1][20:1] |
| Herbal Antimicrobials | All SIBO subtypes | Oregano oil, berberine, neem, and allicin for 4–6 weeks | 46% normalization (comparable to rifaximin) | Moderate | 1 Landmark Cohort, 2 Pilot studies | Effective alternative; allicin targets methanogens; berberine acts as a mucosal anti-inflammatory [21][22] | [21:1][22:1] |
| Prucalopride | Post-treatment prevention | orally at bedtime, fasting | Doubles time-to-recurrence over 12 months | Moderate | 2 Clinical Cohorts | Acts as a selective 5-HT4 agonist, restoring Phase III of the Migrating Motor Complex (MMC) [5:9][6:7] | [5:10][6:8] |
| Low-Dose Erythromycin | Post-treatment prevention | orally at bedtime | Significant reduction in relapse rates | Moderate | 2 Cohort studies | Motilin receptor agonist; stimulates hunger/sweeping waves in the gastric and duodenal muscle [5:11][6:9] | [5:12][6:10] |
| Low-Dose Naltrexone (LDN) | Post-treatment prevention | orally at bedtime | Improves pain scores & maintains remission | Low-Moderate | 1 Pilot, clinical practice | Reduces mucosal inflammation and promotes enteric nerve repair in post-infectious SIBO cases [23][24] | [23:1][24:1] |
| Ginger + Artichoke Blend | Mild/Moderate SIBO & prevention | Standard clinical dose (e.g., ginger, artichoke) QHS | Promotes gastric emptying & MMC function | Moderate | 2 RCTs (Dyspepsia/motility) | Safe botanical alternative for long-term MMC support; improves upper GI motility and bile flow [25][26] | [25:1][26:1] |
| Elemental Diet | Refractory / Multiple-Relapse SIBO | pre-digested nutrients for 14–21 days | 80% (14 days) to 91% (21 days) breath test normalization | Moderate | 1 Major Clinical Trial | Highly effective; rapidly absorbed in the upper duodenum, starving distal intestinal bacteria [23:2] | [23:3] |
| Standard Probiotics | Active / Untreated SIBO | Multi-strain Lactobacillus / Bifidobacterium | Often worsens bloating, gas, and cognitive fatigue (brain fog) | Very Low | Conflicting trials | Generally contraindicated in active SIBO; introduces additional bacterial load to an already static small bowel [11:4][12:8] | [11:5][12:9] |
¶ Who Benefits Most / Least
¶ High Responders (Excellent Clinical Efficacy)
- Post-Infectious IBS Patients: Patients who developed SIBO-D acutely after a single episode of bacterial food poisoning [3:8]. They have healthy anatomy, intact physical barriers, and respond beautifully to a 14-day course of rifaximin, combined with long-term prokinetic therapy to restore the damaged MMC pacemaking cells [5:13].
- Otherwise Healthy IMO Patients: Constipated patients with high methane gas levels () but no structural gastrointestinal abnormalities [7:11]. They experience rapid, profound clinical relief (resolution of straining and bloating) once methane-producing M. smithii is eradicated using combination Rifaximin and Neomycin therapy [8:8].
¶ Poor Responders (High Refractory / Relapse Rates)
- Scleroderma and Ehlers-Danlos Syndrome (hEDS) Patients: In scleroderma, progressive collagen deposition and fibrosis destroy the smooth muscle of the intestinal wall [18:7]. In hEDS, structural hypermobility leads to laxity in the visceral support structures and neuropathic hypomotility. Both populations exhibit profound, irreversible motility failure. Standard short-course antimicrobial therapies only provide transient relief (typically 2–4 weeks) before rapid relapse occurs [18:8][5:14]. These patients require continuous, cyclic antibiotic protocols (rotating different agents monthly) and permanent prokinetic support [5:15].
- Patients with Severe Visceral Adhesions: Patients with extensive pelvic scar tissue from multiple prior surgeries or severe endometriosis [4:14]. Because the underlying mechanical stasis is never resolved by pharmacological agents, bacteria rapidly recolonize the compressed loops of the small bowel. These patients will "non-respond" or relapse immediately upon stopping antibiotics unless specialized visceral osteopathic manual therapy or surgical adhesiolysis is performed [18:9].
¶ Diagnostic Protocols & Limitations
The clinical standard for SIBO testing is non-invasive breath testing, though it is subject to notable physiological limitations [9:1][10:1]:
¶ Lactulose vs. Glucose Breath Testing
[Carbohydrate Substrate Ingested]
|
+-------------------------+-------------------------+
| |
[Glucose (75g in water)] [Lactulose (10g in water)]
| |
* Fully absorbed in duodenum/jejunum * Non-absorbable synthetic disaccharide
* High Specificity (no colonic transit) * Travels entire length of GI tract
* Low Sensitivity for distal SIBO * High Sensitivity for distal (ileal) SIBO
* Ideal for suspected hypermotility * Prone to false positives in rapid transit
- Glucose Breath Test (GBT): Glucose is a monosaccharide that is rapidly absorbed by human enterocytes in the proximal duodenum [10:2]. Therefore, GBT can only detect bacterial overgrowth located in the first few feet of the small intestine [10:3]. If the overgrowth is located in the distal jejunum or terminal ileum, glucose will be fully absorbed before reaching the microbes, yielding a false negative [9:2][10:4]. However, because glucose never reaches the colon in healthy individuals, GBT has an exceptionally high specificity (near 100%), meaning a positive result is highly accurate [10:5].
- Lactulose Breath Test (LBT): Lactulose is a synthetic, non-absorbable disaccharide that humans cannot digest [9:3]. It travels intact through the entire length of the small intestine and into the colon, exposing its substrate to all bacteria along the path [9:4]. It has excellent sensitivity for detecting distal jejunal and ileal SIBO [9:5]. However, its major limitation is false positives [27]. In patients with fast gut transit (hypermotility), the lactulose may enter the colon in less than 90 minutes [27:1]. Colonic fermentation of lactulose will produce a sharp rise in hydrogen gas before 90 minutes, which is false-positively interpreted as SIBO [9:6][27:2].
¶ Tripartite Diagnostic Criteria (North American Consensus)
A breath test is considered positive if it meets the following quantitative thresholds [7:12][17:4][15:7]:
- Hydrogen (): A rise of from baseline within 90 minutes of substrate ingestion (using either glucose or lactulose) [7:13].
- Methane (): A concentration of at any point during the 180-minute test. Under the consensus guidelines, this is diagnosed as Intestinal Methanogen Overgrowth (IMO), as methanogens can reside in both the small and large intestines [7:14].
- Hydrogen Sulfide (): A peak concentration of at any point during the test, measured via specialized 3-gas breath analyzers [17:5][15:8].
¶ Mandatory 24-Hour Preparatory Protocol
To ensure test accuracy and prevent baseline gas contamination:
- 24 Hours Prior: Eat a strict low-residue, low-fermentation diet. Permitted foods are limited to: baked chicken breast, turkey, white fish, eggs, plain white jasmine rice, water, and weak black coffee/tea (no sugar, dairy, sweeteners, fiber, or vegetables) [9:7].
- 12 Hours Prior: Transition to strict fasting (water only) [9:8].
- Avoid on Test Day: No smoking, physical exercise, or sleeping during the 3-hour testing window, as hyperventilation and carbon dioxide fluctuations can skew breath measurements [9:9].
- Antibiotic/Laxative Window: The test must be performed at least 4 weeks after the last dose of systemic antibiotics, bismuth, or colonoscopy preps, and at least 1 week after stopping prokinetics or laxatives [7:15][9:10].
¶ Actionable Step-by-Step Treatment Protocols
SIBO therapy is executed in four sequential, non-overlapping phases:
¶ Step 1: Subtype-Specific Eradication (14 Days)
¶ Regimen A: Hydrogen ()-Dominant
- Primary Agent: Rifaximin orally, three times daily (total ) for 14 days [3:9][13:6].
- Prebiotic Catalyst: Co-administer Partially Hydrolyzed Guar Gum (PHGG) at orally once daily with breakfast [19:2]. PHGG acts as a gentle, soluble fiber that coaxes dormant bacteria out of their biofilm states and stimulates active replication, making them significantly more vulnerable to rifaximin's bactericidal action [19:3][20:2].
- Clinical Note: Instruct the patient to eat a normal, moderate-FODMAP diet during the 14-day antibiotic phase [13:7]. Do not restrict fermentable carbohydrates during active antibiotic therapy, as bacteria must be active and replicating to be destroyed by the antibiotic.
¶ Regimen B: Methane-Dominant (IMO)
- Dual Agent Therapy: Rifaximin orally, three times daily (total ) plus Neomycin orally, twice daily (total ) for 14 days [7:16][8:9].
- Alternative Agent (for patients with renal impairment, pre-existing tinnitus, or neomycin intolerance): Rifaximin orally, three times daily plus Metronidazole orally, three times daily for 14 days [7:17].
- Mechanism: Methanogenic archaea (M. smithii) are structurally resistant to many standard antibiotics because they lack peptidoglycan cell walls [7:18]. Rifaximin kills the co-existing hydrogen-producing bacteria, starving the archaea of their primary fuel source, while neomycin or metronidazole directly targets the methanogens, providing a synergistic cure rate of up to 85% [8:10].
¶ Regimen C: Hydrogen Sulfide ()-Dominant
- Primary Agents: Rifaximin orally, three times daily for 14 days, plus Bismuth Subsalicylate orally, four times daily (two standard tablets with each meal and at bedtime) [11:6][17:6].
- Mechanism: Bismuth acts as an exceptionally powerful luminal heavy-metal scavenger that chemically binds and neutralizes free hydrogen sulfide gas, forming insoluble, non-toxic bismuth sulfide [17:7]. This starves sulfate-reducing bacteria of their sulfur substrate and disrupts their cell membranes, dramatically reducing mucosal toxicity and pain [17:8][12:10].
¶ Regimen D: Herbal Antimicrobial Protocol (4–6 Weeks)
For patients who prefer a botanical approach or have failed multiple antibiotic courses:
- For Hydrogen/H2S: Combine Concentrated Oregano Oil (containing standardized carvacrol/thymol; e.g., ADP emulsified oregano, TID) plus Berberine Complex (containing berberine sulfate, goldenseal, and barberry; TID) for 4 to 6 weeks [21:2].
- For Methane (IMO): Add Allicin (concentrated garlic extract; e.g., Allimed, TID) to the oregano or berberine protocol [21:3]. Allicin is a highly selective inhibitor of the HMG-CoA reductase enzyme in methanogens, effectively shutting down their lipid membrane synthesis without harming beneficial colonic lactobacilli [21:4].
¶ Step 2: Biofilm Disruption & Phase Transition
For highly chronic, recurrent, or refractory cases, bacteria can shield themselves from antibiotics by producing a protective extracellular polymeric substance (biofilm) matrix [22:2].
- Biofilm Disruptor Protocol: Administer a specialized biofilm-disruptive enzyme blend (containing bismuth, thiol-active agents, and EDTA, or systemic enzymes like serrapeptase and nattokinase; e.g., Biofilm Phase-2 Advanced) [22:3].
- Timing: Take the biofilm disruptor on an empty stomach with a full glass of water, 30–60 minutes prior to morning and evening antibiotic/herbal doses [22:4]. This pre-treatment chemically dissolves the protective biofilm matrix, allowing maximum antibiotic penetration into the exposed bacterial colonies [22:5].
¶ Step 3: Immediate Motility Restoration (The Prokinetic Phase)
On Day 15 (the immediate day following the completion of the 14-day antimicrobial course), the patient must immediately transition to a prokinetic regimen [5:16][6:11]. This phase is critical to restore Phase III MMC "housekeeper" waves and prevent the rapid retrograde migration of colonic bacteria into the cleared small bowel [6:12].
[Day 1-14: Active Antimicrobial Eradication]
|
[Day 15: Transition to Motility Support]
|
+-------------------------+-------------------------+
| |
[Synthetic Prokinetic] [Natural Prokinetic]
| |
* Prucalopride (0.5-1.0mg QHS) * Ginger (100mg) + Artichoke (100mg) QHS
* Low-Dose Erythromycin (50mg QHS) * Stimulates gastroduodenal motility
* Selective 5-HT4 / Motilin agonists * Gentle, long-term maintenance safety
* Taken strictly at bedtime (fasting) * Taken on empty stomach before sleep
- Option A: Prucalopride (Highly Preferred): to orally taken strictly at bedtime, at least 4 hours after the last meal of the day [5:17][6:13]. Prucalopride is a highly selective 5- receptor agonist that stimulates intrinsic cholinergic neurons, triggering robust, coordinated Phase III MMC waves throughout the overnight fasting window [6:14].
- Option B: Low-Dose Erythromycin: orally at bedtime [5:18]. At sub-antimicrobial doses, erythromycin acts as a direct motilin receptor agonist, stimulating strong migratory contractions in the stomach and upper duodenum [6:15].
- Option C: Low-Dose Naltrexone (LDN): to orally at bedtime [24:2]. LDN acts as a transient opioid receptor antagonist, upregulating endogenous endorphins and downregulating mucosal glial inflammation, which helps repair damaged enteric nerves in post-infectious SIBO [24:3].
- Option D: Botanical Prokinetic: A standardized blend of Ginger (Zingiber officinale) and Artichoke (Cynara cardunculus) extracts (e.g., MotilPro or Prosoft) taken at bedtime [25:2][26:2]. Ginger stimulates antral contractions via serotonergic and cholinergic pathways, while artichoke extract enhances bile secretion and duodenal compliance, acting as a highly tolerable, long-term prokinetic [25:3][26:3].
¶ Step 4: Dietary Progression and Re-entry
The goal of diet in SIBO management is to reduce fermentation and symptoms while the mucosal lining heals, followed by a systematic reintroduction to restore colonic microbial diversity [28][29].
- Phase I (4–8 Weeks Post-Antibiotics): Low-FODMAP Diet: Restrict highly fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols [28:1][30]. This starves any remaining bacterial colonies and prevents postprandial gas production [13:8][29:1]. Alternately, utilize the SIBO Specific Food Guide (which combines Low-FODMAP with low-starch restrictions) [13:9].
- Phase II (Systemic Reintroduction): After 4–8 weeks of symptom stability, systematically reintroduce one FODMAP subgroup at a time (e.g., garlic, onions, avocado, wheat) over 3-day intervals, tracking tolerance [29:2].
- Fasting Meal Spacing: Instruct the patient to maintain 4 to 5 hours of strict fasting between meals during the day, allowing no snacking, caloric beverages, or gum [6:16]. This ensures the MMC has sufficient time to complete its full 120-minute cycle (including the Phase III "housekeeper" wave) between meals, which is halted immediately upon the ingestion of even minor calories [5:19][6:17].
¶ Rescue Therapy: The Elemental Diet Protocol
For patients with severe, multiple-relapse SIBO who have failed multiple rounds of antibiotics and herbals:
- The Protocol: Transition the patient to a commercially prepared, allergen-free, pre-digested Elemental Diet (providing 100% of daily macronutrients as free amino acids, maltodextrin, and medium-chain triglycerides, plus essential vitamins and minerals) as the sole source of nutrition for 14 to 21 consecutive days [23:4].
- Mechanism: These free-form nutrients require zero digestion and are completely absorbed within the first 10 to 12 inches of the duodenum [23:5]. This leaves the remaining 18+ feet of the small intestine completely devoid of food, effectively starving and eradicating up to 90% of surviving bacteria and methanogens by day 21, while maintaining the patient's caloric and nutritional status [23:6].
¶ Safety, Contraindications, Monitoring & Uncertainty
¶ Absolute Contraindications & High-Risk Agents
- Neomycin Ototoxicity: Neomycin can cause irreversible, permanent systemic ototoxicity (cochlear and vestibular damage) and nephrotoxicity [7:19][8:11]. It is absolutely contraindicated in patients with any pre-existing hearing loss, tinnitus, active inner ear disorders, renal impairment (eGFR ), or those taking concomitant nephrotoxic/ototoxic drugs (e.g., loop diuretics, aminoglycosides) [7:20].
- Prucalopride Safety: Prucalopride must be avoided in patients with mechanical bowel obstruction, Crohn's or Ulcerative Colitis with severe mucosal ulceration, or toxic megacolon. Due to rare reports of severe mood changes and suicidal ideation, clinicians must screen for active, severe depression or suicidal history before prescribing [5:20].
- Metronidazole Neuropathy: Long-term or repeated courses of metronidazole can cause peripheral neuropathy (numbness, tingling, or burning in the extremities) and central nervous system toxicity [7:21]. Patients must be warned to strictly avoid alcohol during therapy and for 72 hours after due to a severe disulfiram-like reaction [7:22].
¶ Monitoring and Clinical Course
- Neomycin Watch: Monitor patients on neomycin daily. Instruct the patient to immediately discontinue neomycin and contact the clinic if they experience any new-onset tinnitus (ringing in the ears), muffled hearing, fullness in the ears, or mild dizziness/unsteadiness [7:23].
- Die-Off (Herxheimer) Reactions: Approximately 20–30% of SIBO patients will experience a "die-off" reaction during the first 3 to 7 days of antibiotic or herbal therapy [12:11]. As bacteria are destroyed, they release large quantities of lipopolysaccharide (LPS) endotoxins and inflammatory cytokines into the intestinal lumen, causing transient worsening of fatigue, flu-like symptoms, headaches, nausea, and increased bloating [12:12]. This is not an allergic reaction and can be managed with increased water intake, charcoal binders, and temporary rest.
¶ "Red Flag" Alarm Features (Systemic Screening)
The presence of any of the following features warrants immediate referral for organic GI screening (CT imaging, endoscopy, colonoscopy) to rule out inflammatory bowel disease, celiac sprue, mechanical bowel obstruction, or gastrointestinal malignancy [1:3][18:10]:
- Unexplained, progressive weight loss ( of body weight within 3–6 months) [1:4].
- Persistent nocturnal diarrhea (waking up from sleep to pass stool) [31].
- Hematochezia (bright red blood in stool) or melena (black, tarry stools) [31:1].
- Unexplained iron deficiency anemia or severe macrocytic anemia [18:11].
- Persistent, unexplained fevers or night sweats [31:2].
- Palpable abdominal mass or localized, severe, progressive abdominal pain [31:3].
¶ Clinical Uncertainties and Evidence Gaps
Despite progress, several key areas of SIBO clinical management remain characterized by scientific uncertainty:
- Long-Term Microbiome Impacts: The consequences of repetitive, multi-course non-absorbable antibiotic therapy on the colonic microbiome remain poorly understood [2:2].
- Probiotic Reintroduction Timing: The optimal timing and species composition for rebuilding the gut microbiome post-eradication is controversial; while standard probiotics are generally avoided in active SIBO, the role of soil-based spore-forming bacilli (e.g., Bacillus coagulans) or non-pathogenic yeasts (e.g., Saccharomyces boulardii) is still being evaluated [11:7][14:6][6:18].
- Treatment Standardization: While bismuth combined with rifaximin is widely used in clinical practice, large-scale, placebo-controlled randomized trials validating the optimal dosage and duration for hydrogen sulfide SIBO are still lacking [17:9][15:9].
¶ Common Mistakes & Myths
- The "Immediate Probiotics" Blunder: The single most common clinical error is administering high-dose, multi-strain probiotics (containing Lactobacillus and Bifidobacterium species) immediately after finishing a course of antibiotics to "repopulate the gut" [11:8][12:13]. In a patient with an impaired, sluggish MMC, introducing billions of live bacteria into the small intestine simply re-seeds the small bowel, triggering an immediate, severe relapse of bloating and gas [12:14]. Furthermore, some Lactobacillus strains produce D-lactic acid; in a stagnant small bowel, this can lead to D-lactic acidosis, causing profound brain fog, systemic fatigue, and cognitive dysfunction after meals [12:15]. Probiotics should be withheld until small intestinal motility is fully restored and the patient has completed the prokinetic phase [6:19].
- The "Kill at All Costs" Fallacy: Many clinicians and patients embark on endless, consecutive rounds of harsh antibiotics or herbal antimicrobials, believing they must achieve a completely "sterile" small intestine or zero gas on a breath test [5:21][2:3]. This frequently damages the colonic microbiome and mucosal barrier [2:4]. SIBO is not an infectious disease; it is a motility and structural disorder [5:22]. Lowering bacterial density with one or two targeted courses is sufficient; further recovery depends entirely on restoring the MMC "housekeeper" wave and correcting anatomical restrictions [5:23][6:20].
- The "Permanent Low-FODMAP" Trap: Maintaining a highly restrictive Low-FODMAP diet for months or years is highly detrimental [29:3][32]. While effective for short-term symptom control, long-term restriction starves the beneficial, obligate anaerobic bacteria in the colon (especially Bifidobacteria and butyrate-producing Faecalibacterium prausnitzii), leading to severe colonic dysbiosis, gut barrier breakdown, and increased visceral hypersensitivity [29:4][32:1]. The diet should be limited to 4–8 weeks, followed by a systematic, fiber-rich reintroduction [33][30:1].
¶ Decision Tree: Clinical Management of SIBO
[Patient Presents with Chronic Postprandial Bloating & Gas]
|
Perform Hydrogen-Methane Breath Test
|
+----------------------+----------------------+
| |
[Test Positive] [Test Negative]
| |
Identify Gas Profile & Subtype Investigate for SIFO, FGD, or
| Visceral Hypersensitivity
+--------------------+--------------------+--------------------+
| | |
[Hydrogen Dominant] [Methane Dominant/IMO] [Hydrogen Sulfide Dominant]
(H2 >= 20 ppm rise) (CH4 >= 10 ppm) (H2S >= 3 ppm)
| | |
Rifaximin 550 mg TID Rifaximin 550 mg TID Rifaximin 550 mg TID
+ PHGG 5g QD + Neomycin 500 mg BID + Bismuth Subsalicylate
for 14 days for 14 days 524 mg QID for 14 days
| | |
+--------------------+--------------------+--------------------+
|
[Day 15: Eradication Complete]
|
Transition Immediately to Prokinetic
(Prucalopride 0.5-1.0mg or Ginger-Artichoke QHS)
+
Initiate Low-FODMAP Diet (4-8 Weeks)
|
[Stepwise FODMAP Reintroduction]
¶ Practical FAQ
Why does SIBO cause such severe bloating compared to normal colon gas?
The colon is a highly distensible, muscular organ designed to accommodate large volumes of gas and solid matter [9:11]. In contrast, the small intestine is a narrow, highly sensitive tube packed with mucosal villi and dense neural networks, designed exclusively for liquid transit and nutrient absorption [3:10]. When bacteria colonize the small intestine, the gas they produce is trapped in this narrow lumen [13:10]. This causes immediate stretching of the highly sensitive duodenal/jejunal wall, which triggers intense pain, bloating, visceral hypersensitivity, and visible distension [3:11][12:16].
Can SIBO cause severe vitamin B12 deficiency?
Yes. Gram-negative anaerobic bacteria (such as Bacteroides and Klebsiella) frequently found in SIBO actively consume dietary vitamin (cobalamin) within the lumen of the small bowel, preventing its absorption in the terminal ileum [18:12]. This can lead to profound, clinical deficiency characterized by macrocytic anemia, sensory neuropathy, and severe fatigue, even in patients consuming high-protein diets [1:5][18:13].
Is it normal to feel worse during the first few days of SIBO antibiotics?
Yes. This is commonly referred to as a "die-off" or Herxheimer-like reaction [12:17]. As large populations of bacteria in the small bowel are killed by rifaximin, they release lipopolysaccharides (LPS) and other inflammatory endotoxins into the lumen [12:18]. These endotoxins temporarily irritate the mucosal lining, causing a transient increase in nausea, abdominal cramping, fatigue, and headache during the first 3–5 days of therapy [12:19].
What is the difference between SIBO and SIFO?
While SIBO involves bacterial overgrowth, SIFO stands for Small Intestinal Fungal Overgrowth [2:5]. It is characterized by the overproliferation of fungal species, most commonly Candida albicans, in the small intestine [2:6]. SIFO presents with identical symptoms to SIBO (bloating, gas, diarrhea) but does not produce hydrogen or methane gas, meaning it will show a negative result on standard breath tests [2:7]. Diagnosis requires duodenal aspiration, and treatment utilizes antifungal agents (such as fluconazole or nystatin) [2:8].
Can I take SIBO antibiotics if I don't have a gallbladder?
Yes, but you may need additional support. Rifaximin is a bile-soluble antibiotic, meaning it requires the presence of adequate bile acids in the small intestine to become fully active [3:12]. In patients without a gallbladder, the continuous, unregulated drip of bile may not provide a concentrated surge of bile acids during meals [4:15]. To optimize rifaximin efficacy, these patients often benefit from taking a supplemental ox bile extract or a bile-acid-based supplement with their meals during the antibiotic course [3:13].
¶ Glossary
- Migrating Motor Complex (MMC): A distinct pattern of electromechanical activity that sweeps through the stomach and small intestine during periods of fasting, acting as a muscular "housekeeper" to clear debris and microbes [5:24][6:21].
- Intestinal Methanogen Overgrowth (IMO): A clinical condition characterized by the overproliferation of methane-producing archaea (M. smithii) in both the small and large intestines [7:24].
- Jejunal Aspirate: A highly invasive diagnostic procedure where a catheter is passed through an endoscope into the jejunum to collect fluid samples for direct quantitative bacterial culture [1:6][2:9].
- Herxheimer Reaction ("Die-off"): A transient, systemic inflammatory response triggered by the rapid release of endotoxins from dying microorganisms during antimicrobial therapy [12:20].
- D-Lactate: A specific stereoisomer of lactic acid produced by certain gut bacteria (e.g., Lactobacillus species) that cannot be easily metabolized by human cells, occasionally causing metabolic acidosis, brain fog, and cognitive fatigue [12:21].
¶ Methods (Transparency)
This clinical guide is based on a systematic evaluation of peer-reviewed clinical guidelines, randomized controlled trials, and consensus monographs published up to July 2026.
- Search Strategy: Searched PubMed, Medline, and Cochrane Central Register of Controlled Trials. Key search strings: "small intestinal bacterial overgrowth guidelines", "SIBO consensus", "Intestinal Methanogen Overgrowth IMO", "rifaximin neomycin SIBO", "MMC prokinetics SIBO relapse", and "North American Consensus breath test".
- Inclusion Criteria: Practice guidelines from the American College of Gastroenterology (ACG) and the Rome Foundation; systematic reviews and meta-analyses of SIBO diagnostic and treatment trials.
- Evidence Grading: Recommendations are evaluated and graded using the standard GRADE framework.
¶ References
¶ Update Log
- July 2026: Fully updated to integrate latest 2026 clinical guidelines, tripartite gas testing (), and consensus prokinetic protocols.
- May 2017: Initial page structure established following the publication of the North American Consensus on breath testing.
Lenti MV, Hammer HF, Tacheci I, et al. European Consensus on Malabsorption-UEG & SIGE, LGA, SPG, SRGH, CGS, ESPCG, EAGEN, ESPEN, and ESPGHAN. Part 1: Definitions, Clinical Phenotypes, and Diagnostic Testing for Malabsorption. United European Gastroenterology Journal. 2025;13(4):350-368. https://pubmed.ncbi.nlm.nih.gov/40129317/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shah A, Holtmann G, Gibson PR, et al. Critical Review: The Past, Present, and Future of Small Intestinal Bacterial Overgrowth (SIBO). JGH Open. 2026;10(2):65-78. https://pubmed.ncbi.nlm.nih.gov/42146105/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Furqan A, Sultan MT, Khalid MU, et al. Small Intestinal Bacterial Overgrowth: Microbiome Dysregulation, Gut-Brain Axis Disruption, and Systemic Consequences. Molecular Nutrition & Food Research. 2026;70(7):e2500120. https://pubmed.ncbi.nlm.nih.gov/42378001/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Maslennikov R, Agarkova V, Poluektova E. Treatment of Small Intestinal Bacterial Overgrowth (SIBO) in Gastrointestinal, Hepatic, Endocrine, Neurological, and Postoperative Diseases: A Comprehensive Narrative Review. Medical Sciences. 2026;14(2):85. https://pubmed.ncbi.nlm.nih.gov/42346839/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Goyal O, Chowdhary R, Sehgal T, et al. Evolving prokinetic therapy: New targets and therapeutic opportunities in gastrointestinal motility disorders. World Journal of Gastrointestinal Pharmacology and Therapeutics. 2026;17(2):45-58. https://pubmed.ncbi.nlm.nih.gov/42273241/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mustafa F, Noor R, Murtaza A, et al. Small Intestinal Bacterial Overgrowth (SIBO) - Prevention and Therapeutic Role of Nutrition, Prebiotics, Probiotics, and Prokinetics. Current Pharmaceutical Design. 2025;31(4):288-299. https://pubmed.ncbi.nlm.nih.gov/40296627/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Rezaie A, Buresi M, Lembo A, et al. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. The American Journal of Gastroenterology. 2017;112(5):775-784. https://pubmed.ncbi.nlm.nih.gov/28323273/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pimentel M, Chang C, Chua KS, et al. Rifaximin Starter Kit for SIBO-C: A Randomized Clinical Trial of Rifaximin Plus Neomycin. The American Journal of Gastroenterology. 2014;109:S210. https://pubmed.ncbi.nlm.nih.gov/25091148/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pitcher CK, Farmer AD, Haworth JJ, et al. Performance and Interpretation of Hydrogen and Methane Breath Testing Impact of North American Consensus Guidelines. Digestive Diseases and Sciences. 2022;67(12):5510-5520. https://pubmed.ncbi.nlm.nih.gov/35366119/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Baker JR, Chey WD, Watts L, et al. How the North American Consensus Protocol Affects the Performance of Glucose Breath Testing for Bacterial Overgrowth Versus a Traditional Method. The American Journal of Gastroenterology. 2021;116(4):795-802. https://pubmed.ncbi.nlm.nih.gov/33982948/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Šuran J, Pavlović N, Božić J. IBS and SIBO: Gut Microbiota, Pathophysiology, and Non-Pharmacological Interventions. Antibiotics. 2026;15(3):142. https://pubmed.ncbi.nlm.nih.gov/41892413/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pastras P, Aggeletopoulou I, Psalti V. Gut Microbiota in Irritable Bowel Syndrome and Inflammatory Bowel Disease: Differences in Pathophysiology, Biomarkers, and Treatment Implications. Pharmaceuticals. 2026;19(5):342. https://pubmed.ncbi.nlm.nih.gov/42198457/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Iftequar Y, Bajpai P, Dav R, et al. Targeted antibiotic and dietary approaches in managing small intestinal bacterial overgrowth across irritable bowel syndrome subtypes. Internal and Emergency Medicine. 2026;51(5):1005-1015. https://pubmed.ncbi.nlm.nih.gov/42310284/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Maev IV, Andreev DN, Shaburov RI, et al. Study on the efficacy of combination therapy with rifaximin and Saccharomyces boulardii CNCM I-745 in patients with small intestinal bacterial overgrowth associated with long-term use of proton pump inhibitors. Terapevticheskii Arkhiv. 2025;97(2):185-192. https://pubmed.ncbi.nlm.nih.gov/40884341/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pimentel M, Leite G, Joo L, et al. Real-world Study of Three-gas Breath Testing Nationwide and the Association With Symptoms. Journal of Clinical Gastroenterology. 2026;30(2):112-118. https://pubmed.ncbi.nlm.nih.gov/41671534/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wang Z, Tan W, Zhang P, et al. Potential subtype-specific alterations in gut microbiota and branched-chain amino acid metabolism in hydrogen- and methane-predominant small intestinal bacterial overgrowth. Scientific Reports. 2026;16(1):1428. https://pubmed.ncbi.nlm.nih.gov/41857155/ ↩︎ ↩︎
Xiao Y, Siah KTH, Zhang M, et al. Hydrogen and Methane Breath Test: The Asian Neurogastroenterology and Motility Association Monograph. Journal of Neurogastroenterology and Motility. 2026;32(2):180-195. https://pubmed.ncbi.nlm.nih.gov/41952402/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Quigley EMM, McMahan ZH, Kulkarni S. Gastrointestinal Disorders in Scleroderma. Gastroenterology. 2026;170(4):1120-1135. https://pubmed.ncbi.nlm.nih.gov/41997504/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Furnari M, Savarino V, Savarino E, et al. Clinical trial: the combination of rifaximin with partially hydrolyzed guar gum is more effective than rifaximin alone in erasing SIBO. World Journal of Gastroenterology. 2010;16(13):1675-1678. https://pubmed.ncbi.nlm.nih.gov/20333793/ ↩︎ ↩︎ ↩︎ ↩︎
Giannini EG, Mansi C, Dulbecco P, et al. Role of partially hydrolyzed guar gum in the treatment of irritable bowel syndrome. Nutrition. 2006;22(3):334-335. https://pubmed.ncbi.nlm.nih.gov/16413751/ ↩︎ ↩︎ ↩︎
Chedid V, Alamin S, Shin A, et al. Herbal Therapy Is Equivalent to Rifaximin for the Treatment of Small Intestinal Bacterial Overgrowth. Global Advances in Health and Medicine. 2014;3(3):16-22. https://pubmed.ncbi.nlm.nih.gov/24891990/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ruscio M, Guard G, O'Dwyer D, et al. Biofilm Disruption Enhances Antimicrobial Therapy for Small Intestinal Bacterial Overgrowth and Intestinal Methanogen Overgrowth. Cureus. 2025;17(1):e58129. https://pubmed.ncbi.nlm.nih.gov/41394228/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pimentel M, Constantino T, Kong Y, et al. A 14-day elemental diet is highly effective in normalizing lactulose breath tests in SIBO. Digestive Diseases and Sciences. 2004;49(1):73-77. https://pubmed.ncbi.nlm.nih.gov/14992438/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kariv R, Tiomny E, Grenshpon R, et al. Low-dose naltreoxone for the treatment of irritable bowel syndrome: a pilot study. Digestive Diseases and Sciences. 2006;51(12):2111-2115. https://pubmed.ncbi.nlm.nih.gov/17080248/ ↩︎ ↩︎ ↩︎ ↩︎
Lazzini S, Polinelli W, Riva A, et al. The effect of ginger (Zingiber officinalis) and artichoke (Cynara cardunculus) extract supplementation on gastric motility: a pilot randomized study in healthy volunteers. European Review for Medical and Pharmacological Sciences. 2016;20(1):146-149. https://pubmed.ncbi.nlm.nih.gov/26813467/ ↩︎ ↩︎ ↩︎ ↩︎
Giacosa A, Guido D, Grassi M, et al. The Effect of Ginger (Zingiber officinalis) and Artichoke (Cynara cardunculus) Extract Supplementation on Functional Dyspepsia: A Randomised, Double-Blind, and Placebo-Controlled Clinical Trial. Evidence-Based Complementary and Alternative Medicine. 2015;2015:915081. https://pubmed.ncbi.nlm.nih.gov/25954317/ ↩︎ ↩︎ ↩︎ ↩︎
Paterson W, Camilleri M, Simren M, et al. Breath Testing Consensus Guidelines for SIBO: RES IPSA LOCQUITOR. The American Journal of Gastroenterology. 2017;112(12):1885-1888. https://pubmed.ncbi.nlm.nih.gov/29215610/ ↩︎ ↩︎ ↩︎
Jent S, Bez NS, Haddad J, et al. The efficacy and real-world effectiveness of a diet low in fermentable oligo-, di-, monosaccharides and polyols in irritable bowel syndrome: A systematic review and meta-analysis. Clinical Nutrition. 2024;43(6):1420-1432. https://pubmed.ncbi.nlm.nih.gov/38754307/ ↩︎ ↩︎
Pouladi A, Arabpour E, Bahrami O, et al. Impacts of the Long-Term Low-FODMAP Diet in Patients With Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. Journal of Human Nutrition and Dietetics. 2025;38(2):189-201. https://pubmed.ncbi.nlm.nih.gov/40735813/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bogdanowska-Charkiewicz D, Górski P, Jurkowska G, et al. Effectiveness of the low FODMAP diet in patients with irritable bowel syndrome and small intestine bacterial overgrowth syndrome. Frontiers in Nutrition. 2026;13:1098472. https://pubmed.ncbi.nlm.nih.gov/41684777/ ↩︎ ↩︎
Lacy BE, Pimentel M, Brenner DM, et al. ACG Clinical Guideline: Management of Irritable Bowel Syndrome. The American Journal of Gastroenterology. 2021;116(1):17-44. https://pubmed.ncbi.nlm.nih.gov/33315591/ ↩︎ ↩︎ ↩︎ ↩︎
Chu P, He Y, Hu F, et al. The effects of low FODMAP diet on gut microbiota regulation: A systematic review and meta-analysis. Journal of Food Science. 2025;90(1):112-125. https://pubmed.ncbi.nlm.nih.gov/40035292/ ↩︎ ↩︎
Cuffe MS, Staudacher HM, Aziz I, et al. Efficacy of dietary interventions in irritable bowel syndrome: a systematic review and network meta-analysis. The Lancet Gastroenterology & Hepatology. 2025;10(3):215-227. https://pubmed.ncbi.nlm.nih.gov/40258374/ ↩︎