¶ Saccharomyces boulardii
| Type | Probiotic Yeast (Eukaryote) |
| Active Cmpd | Viable cells of Saccharomyces boulardii |
| Source | Isolated from lychee and mangosteen skins |
| Dose Range | 250–1,000 mg/day (5–20 Billion CFU) |
| Half-life | Transient (clears in 3–7 days) |
| Main Benefit | Prevents antibiotic diarrhea and dysbiosis |
| Absorption | Non-absorbable (acts in gut lumen) |
Saccharomyces boulardii is a unique, non-pathogenic, eukaryotic probiotic yeast widely utilized in clinical medicine to manage gastrointestinal dysbiosis, prevent antibiotic-associated diarrhea, and enhance standard antibiotic regimens. Backed by extensive high-quality human evidence, including dozens of systematic reviews and meta-analyses, it represents one of the most robustly validated probiotic interventions available [1] [2].
¶ At a glance
Aliases
- Also known as: Saccharomyces cerevisiae var. boulardii, S. boulardii CNCM I-745, Florastor
- Chemical / botanical name: Saccharomyces boulardii
- Category: Probiotic yeast (Eukaryote)
Key points (high-level summary)
- Co-administration of S. boulardii with standard systemic antibiotics reduces the risk of antibiotic-associated diarrhea (AAD) by approximately 50% across both pediatric and adult populations [1:1] [2:1].
- In patients undergoing eradication therapy for Helicobacter pylori, adding S. boulardii increases eradication success rates by approximately 11% while significantly reducing treatment-limiting side effects like diarrhea, nausea, and abdominal pain [3] [4] [5].
- Unlike bacterial probiotics, S. boulardii is a eukaryotic fungus, rendering it naturally and absolutely resistant to all antibacterial agents and allowing concurrent administration without timing gaps [6] [7].
- It is strictly contraindicated in patients with central venous catheters (CVCs), critical illness, or severe immunocompromise due to a documented, potentially life-threatening risk of fungemia and catheter colonization [6:1] [8].
What people use it for
- Main goals: Prevention of antibiotic-associated diarrhea, adjunctive H. pylori clearance, management of pediatric and adult acute infectious diarrhea, traveler's diarrhea prophylaxis, and support for inflammatory bowel disease (IBD) or liver disease.
- Evidence quality (overall): High
¶ What is Saccharomyces boulardii?
S. boulardii is a non-pathogenic, eukaryotic biotherapeutic yeast taxonomically classified as a subspecies of Saccharomyces cerevisiae [6:2]. It is distinct from common baker's yeast in its genetic stability, metabolic profile, and ability to thrive at high physiological temperatures and acidic environments [6:3] [9].
- Definition: Eukaryotic probiotic yeast with biotherapeutic properties.
- Natural sources: It was originally isolated in 1923 by French microbiologist Henri Boulard from the skins of lychee and mangosteen fruits in Southeast Asia [6:4].
- Traditional / historical use: Historically, Boulard observed that local populations consumed teas brewed from these fruit skins to prevent or alleviate cholera and severe diarrhea, which led to the isolation and clinical study of the yeast [6:5].
- Current regulatory status: Widely available over-the-counter as a dietary supplement or biotherapeutic probiotic in the United States and Europe (e.g., as lyophilized capsules or sachets) [6:6].
- Key pharmacological property: Non-pathogenic, non-colonizing eukaryotic probiotic with anti-toxin, pathogen-binding, and immunomodulatory properties [6:7] [9:1].
¶ What are Saccharomyces boulardii’s main benefits?
S. boulardii is primarily used to restore gut homeostasis and manage acute gastrointestinal disorders. Its eukaryotic nature and robust survival in the upper digestive tract allow it to serve as a powerful clinical adjunct to standard drug therapies.
-
Outcome: Antibiotic-associated diarrhea (AAD) prevention
-
Direction of effect: Decrease
-
Magnitude: Large (approximately 50% relative risk reduction; NNT = 10)
-
Population studied: Adults and pediatric cohorts receiving systemic antibiotic courses
-
Evidence quality: High
-
Summary sentence: S. boulardii is the premier probiotic intervention to prevent the development of diarrhea during antibiotic therapy [1:2] [2:2].
-
Outcome: Adjunctive Helicobacter pylori eradication success
-
Direction of effect: Increase
-
Magnitude: Moderate (11% relative increase in success; RR = 1.11 [95% CI: 1.08–1.15])
-
Population studied: Adult and pediatric patients undergoing bismuth quadruple therapy (BQT) or standard triple therapy
-
Evidence quality: High
-
Summary sentence: Co-administration with eradication regimens significantly improves bacterial clearance while halving the incidence of total side effects like bloating, nausea, and diarrhea [3:1] [4:1] [5:1] [10].
-
Outcome: Pediatric acute gastroenteritis (PAGE) recovery
-
Direction of effect: Decrease (duration of diarrhea)
-
Magnitude: Moderate to Large (reduces diarrhea duration by approximately 24 hours / 1 day)
-
Population studied: Pediatric patients hospitalized or treated in emergency settings for acute gastroenteritis
-
Evidence quality: High
-
Summary sentence: When added to standard oral rehydration solutions, it significantly shortens the illness duration and hospital stay length [1:3] [11] [12].
-
Outcome: Inflammatory bowel disease (IBD) maintenance of remission
-
Direction of effect: Increase (remission maintenance) / Decrease (relapse rate)
-
Magnitude: Small to Moderate
-
Population studied: Patients with mild-to-moderate Crohn's disease or ulcerative colitis
-
Evidence quality: Low to Moderate
-
Summary sentence: It serves as a helpful, non-colonizing adjunct to standard anti-inflammatory drugs to prevent flares and maintain remission [13].
-
Outcome: Pathological bacterial translocation in chronic liver diseases
-
Direction of effect: Decrease (translocation, SIBO, and endotoxemia)
-
Magnitude: Moderate
-
Population studied: Patients with liver cirrhosis or non-alcoholic fatty liver disease (NAFLD)
-
Evidence quality: Moderate
-
Summary sentence: It modulates the gut-liver axis by improving intestinal barrier permeability and lowering systemic endotoxins [14].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Antibiotic-Associated Diarrhea | High | High | ~21 RCTs | [500–1,000 mg/day during antibiotic course][1:4][2:3] | |
| H. pylori Eradication (Adjunct) | High | High | Multiple Meta-Analyses | [500 mg/day for 10–14 days in eradication therapy][3:2][4:2][5:2] | |
| Pediatric Acute Diarrhea Duration | High | High | Many RCTs | [250–500 mg/day for 5–7 days with ORS][1:5][11:1][12:1] | |
| C. difficile Recurrence | Moderate | Moderate | RCTs | [1,000 mg/day for 4 weeks with high-dose vancomycin][8:1] | |
| IBD Remission Maintenance | Moderate | Low | Small RCTs | [500–750 mg/day for maintenance of remission][13:1] | |
| Liver Cirrhosis (Endotoxemia) | Moderate | Moderate | Systematic Review | [Reduces SIBO and bacterial translocation in cirrhosis][14:1] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row.
¶ How does Saccharomyces boulardii work?
The efficacy of S. boulardii is driven by a multifactorial mode of action targeting pathogen-secreted toxins, modulating host epithelial responses, and recalibrating the mucosal immune system [6:8] [9:2].
- Primary targets: Pathogen-secreted toxins, host intestinal brush-border disaccharidases, and mucosal inflammatory pathways (NF-κB, MAPK) [6:9] [9:3].
- Core mechanisms:
- Enzymatic Toxin Cleavage: S. boulardii secretes a specific 54 kDa serine protease that directly cleaves and degrades Clostridioides difficile Toxins A and B, preventing them from binding to colonic receptors and causing fluid secretion [6:10] [8:2].
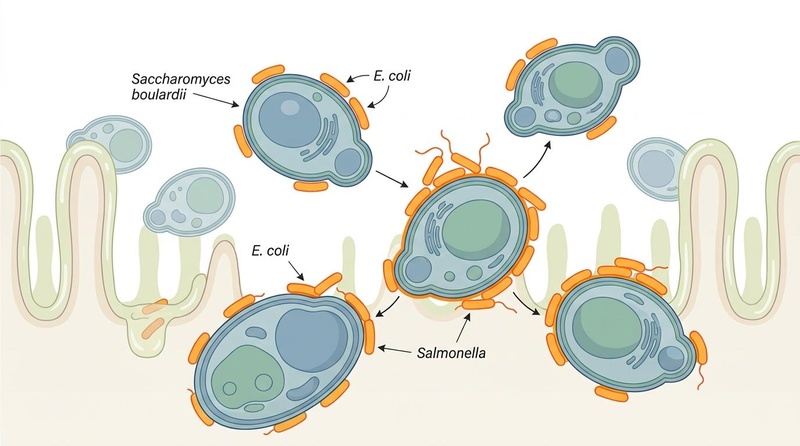
- Steric Hindrance & Pathogen Adherence: Due to its large eukaryotic cell size (approximately 10 times larger than bacteria), the yeast acts as a physical decoy. Pathogenic bacteria with mannose-binding fimbriae (such as Salmonella and E. coli) adhere directly to the S. boulardii cell wall, preventing their attachment to host enterocytes and allowing for safe fecal elimination [6:11].
- Trophic Support for the Mucosa: The yeast releases polyamines (spermine, spermidine) that stimulate the maturation of enterocytes and massively upregulate host brush-border enzymes (sucrase, maltase, lactase), which helps reverse osmotic diarrhea associated with viral infections [6:12] [9:4].
- Microbiota Resilience & SCFA Production: S. boulardii administration shifts the microbiota toward a profile rich in short-chain fatty acid (SCFA) producers like Bacteroidetes. The resulting increase in luminal butyrate provides essential energy to colonocytes, repairing tight junctions and reducing intestinal permeability [7:1] [14:2].
- Mucosal Immunomodulation: It enhances adaptive mucosal immunity by stimulating the secretion of protective secretory Immunoglobulin A (sIgA) [9:5]. Simultaneously, it secretes small factors that inhibit the activation of NF-κB and MAPK signaling pathways, suppressing the synthesis of pro-inflammatory cytokines like IL-8 and TNF-α [6:13].
- Evidence source:
- Pharmacokinetics basics: S. boulardii is non-colonizing and transient. It reaches a steady-state concentration in the colon within 3 days of daily administration and clears completely from the GI tract within 3–7 days of discontinuation [6:16]. It is highly resistant to gastric acid and bile salts, with optimal thermophilic metabolic activity at the human physiological temperature of 37°C [6:17] [9:7].
¶ Effects on different systems
¶ Gut & digestion
S. boulardii is most renowned for its effects on the gut microbiome and intestinal barrier. It is a primary clinical intervention for antibiotic-associated diarrhea, where meta-analyses show it halves the risk of developing diarrhea during broad-spectrum antibiotic treatment [1:6] [2:4]. In children, it reliably shortens the duration of acute diarrhea by approximately one day [11:2] [12:2]. For H. pylori infections, it serves as a critical adjunct that not only improves bacterial clearance but also drastically reduces treatment-associated side effects, significantly improving patient compliance with difficult quadruple therapy regimens [3:3] [10:1] [4:3].
¶ Immune resilience
The probiotic exerts targeted regulatory effects on the host's immune system. By upregulating the luminal secretion of secretory IgA, it reinforces the first line of mucosal defense against pathogens [9:8]. Its anti-inflammatory factors block the nuclear translocation of NF-κB, effectively dampening the "cytokine storm" (specifically IL-8 and TNF-α) that often drives epithelial damage and fluid leakage during severe dysbiosis [6:18].
¶ Metabolic and liver health
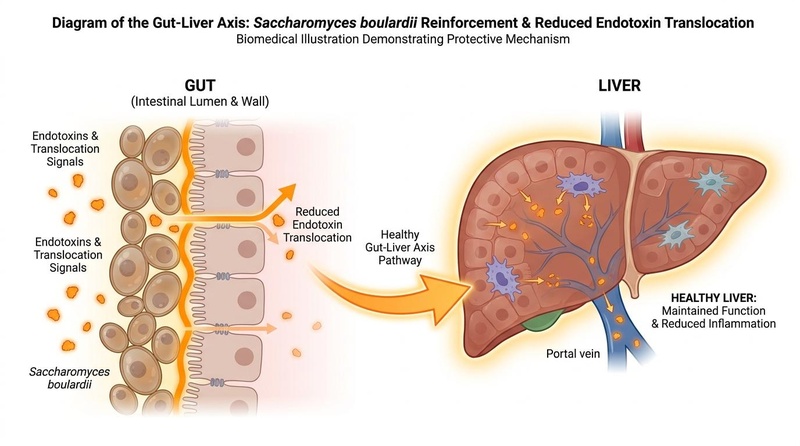
Figure 2: Diagram of the gut-liver axis illustrating how S. boulardii reinforces the intestinal barrier to reduce bacterial translocation and systemic endotoxemia.
Emerging evidence suggests S. boulardii plays a protective role in liver diseases through the gut-liver axis. Systematic reviews demonstrate that in patients with liver cirrhosis or hepatic encephalopathy, the probiotic reduces pathological bacterial translocation and systemic endotoxemia by reinforcing the intestinal wall and shifting the gut microbiota [14:3]. By decreasing the abundance of Proteobacteria and increasing Bacteroidetes, it lowers the burden of pro-inflammatory lipopolysaccharides (LPS) reaching the liver via the portal vein [14:4]. Furthermore, synergistic combinations with prebiotics like inulin or FOS can further enhance these metabolic benefits [7:2].
¶ Dosage and how to take it
Standard dosing in studies
- Typical daily dose range: 250 mg to 1,000 mg (approximately 5 to 20 billion CFU).
- Common dosing schedules: Administered in 1–2 divided doses. For H. pylori, 500 mg daily is common; for CDI or severe AAD, 1,000 mg/day is often used.
- Study durations: Typically taken for the duration of an antibiotic course plus 3–7 days after (for AAD), or for 10–14 days as part of eradication therapy. Long-term maintenance (months) has been studied in IBD [13:2].
Forms and bioavailability
- Common forms: Lyophilized (freeze-dried) capsules or sachets are standard; lyophilization ensures high viability and survival at room temperature.
- Relative differences: Lyophilized preparations are superior to heat-dried forms for ensuring the yeast remains alive until ingestion.
- With or without food: Can be taken with or without food. Crucially, as a eukaryote, it can be taken at the exact same time as antibiotics without any spacing requirements [6:19].
Special populations
- Kidney or liver impairment: No dose adjustments are generally required as the organism is not absorbed and acts locally in the gut lumen [14:5].
- Older adults: Well-tolerated, but should be used with extreme caution in hospitalized or bedridden elderly patients due to the risk of catheter colonization.
- Children and adolescents: Highly safe and effective for acute diarrhea; standard dose is 250 mg once or twice daily [1:7] [11:3] [12:3].
- Pregnancy and breastfeeding: Limited human data available; use under medical supervision.
¶ Safety and side effects
S. boulardii is remarkably safe in healthy, immunocompetent individuals. Because it is transient and non-colonizing, it does not permanently alter the human microbiome.
Common side effects
- Mild gastrointestinal symptoms including flatulence, transient constipation, and thirst [6:20].
- These effects are generally mild and resolve upon discontinuation or dose reduction.
Less common / serious concerns
- Fungemia (Invasive Infection): The most serious risk is S. boulardii fungemia, a rare but life-threatening bloodstream infection that occurs primarily in hospitalized or critically ill patients [6:21].
- Catheter Colonization: In hospital settings, opening capsules or sachets of the lyophilized powder can aerosolize the yeast, leading to the colonization of central venous catheters (CVCs) and subsequent catheter-related bloodstream infections [6:22] [8:3].
Who should be especially cautious or avoid it
- Patients with a Central Venous Catheter (CVC) in place.
- Critically ill patients in ICU settings or on mechanical ventilation.
- Severely immunocompromised individuals (e.g., those on intensive chemotherapy or high-dose immunosuppressants).
- Healthcare workers should avoid opening S. boulardii preparations in the presence of patients with CVCs [6:23].
¶ Drug and supplement interactions
Pharmacokinetic interactions
- S. boulardii is not absorbed into the systemic circulation and does not interact with the cytochrome P450 (CYP) enzyme system [6:24].
Pharmacodynamic interactions
- Antifungals: Concurrent use of oral or systemic antifungals (e.g., fluconazole, nystatin, itraconazole) will rapidly kill the probiotic yeast, making it entirely ineffective. Avoid co-administration [6:25].
- Antibiotics: Naturally resistant to all antibacterial drugs. It can be taken simultaneously with antibiotics (e.g., amoxicillin, clarithromycin, vancomycin) to prevent AAD and improve tolerability [6:26] [8:4].
¶ Combining Saccharomyces boulardii with other supplements (“stacks”)
- Synbiotic Prebiotic Stack: Combining with prebiotics like inulin, fructooligosaccharides (FOS), or galactooligosaccharides (GOS). Prebiotics act as metabolic modulators that enhance the yeast's viability and synergistically support gut homeostasis [7:3].
- Bismuth Eradication Stack: Administered alongside bismuth quadruple therapy components for H. pylori eradication to increase clearance and reduce side effects [3:4] [10:2] [4:4] [5:3].
- Rehydration & Smectite Stack: Used with oral rehydration salts (ORS) and smectite in pediatric acute gastroenteritis for rapid symptom relief and shortened illness duration [12:4].
¶ Practical questions (FAQ)
-
Does Saccharomyces boulardii need to be refrigerated?
Lyophilized (freeze-dried) preparations are stable at room temperature and generally do not require refrigeration, making them ideal for travel. -
Can I take S. boulardii at the same time as my antibiotics?
Yes. Unlike bacterial probiotics, S. boulardii is a yeast and is not affected by antibiotics. You do not need to wait or space out the doses. -
How long does it stay in my system after I stop taking it?
It is a transient probiotic and does not colonize the gut. It usually clears the system entirely within 3 to 7 days after the last dose [6:27]. -
Is it safe for children?
Yes, it is one of the most studied and recommended probiotics for treating acute diarrhea and gastroenteritis in children [1:8] [11:4] [12:5]. -
Should I take it for Traveler's Diarrhea?
Yes, meta-analyses suggest it provides a reliable pooled relative risk reduction for preventing traveler's diarrhea when started before travel [6:28].
¶ How we evaluated the evidence
- Study types prioritized: Meta-analyses of randomized controlled trials (RCTs) and systematic reviews were the primary drivers for efficacy claims.
- How we graded evidence quality:
- High: Supported by multiple meta-analyses of high-quality RCTs with consistent findings (e.g., AAD, H. pylori, pediatric diarrhea).
- Moderate: Supported by systematic reviews or multiple RCTs with some limitations (e.g., C. diff recurrence, liver disease).
- Low: Based on small RCTs or clinical cohorts with limited data (e.g., IBD remission maintenance).
- We focused on human clinical outcomes and primary pharmacological mechanisms validated in biomedical literature.
¶ References
McFarland LV, Li T. (2025). Efficacy and safety of Saccharomyces boulardii CNCM I-745 for the treatment of pediatric acute diarrhea in China: a systematic review and meta-analysis. Frontiers in Cellular and Infection Microbiology. https://pubmed.ncbi.nlm.nih.gov/40535538/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dinleyici EC, et al. (2012). Effectiveness and safety of Saccharomyces boulardii for acute infectious diarrhea. Expert Opinion on Biological Therapy. https://pubmed.ncbi.nlm.nih.gov/22335323/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ma F, et al. (2025). Efficacy and Safety of Saccharomyces Boulardii with Standard Quadruple Therapy for Eradication of Helicobacter Pylori in Adults: Meta-Analysis. Journal of the College of Physicians and Surgeons--Pakistan. https://pubmed.ncbi.nlm.nih.gov/41247686/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Li M, Xie Y. (2025). Efficacy and safety of Saccharomyces boulardii as an adjuvant therapy for the eradication of Helicobacter pylori: a meta-analysis. Frontiers in Cellular and Infection Microbiology. https://pubmed.ncbi.nlm.nih.gov/40012609/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chen Y, et al. (2024). The effect of supplementing with Saccharomyces boulardii on bismuth quadruple therapy for eradicating Helicobacter pylori: a systematic review and meta-analysis. Frontiers in Medicine. https://pubmed.ncbi.nlm.nih.gov/38695028/ ↩︎ ↩︎ ↩︎ ↩︎
Czerucka D, et al. (2007). Review article: yeast as probiotics -- Saccharomyces boulardii. Alimentary Pharmacology & Therapeutics. https://pubmed.ncbi.nlm.nih.gov/17767461/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lottermann E, et al. (2026). Prebiotics as modulators of Saccharomyces boulardii activity: implications for gut microbiota homeostasis - a narrative review. Future Microbiology. https://pubmed.ncbi.nlm.nih.gov/42126924/ ↩︎ ↩︎ ↩︎ ↩︎
Segarra-Newnham M. (2007). Probiotics for Clostridium difficile-associated diarrhea: focus on Lactobacillus rhamnosus GG and Saccharomyces boulardii. The Annals of Pharmacotherapy. https://pubmed.ncbi.nlm.nih.gov/17595306/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Stier H, Bischoff SC. (2016). Influence of Saccharomyces boulardii CNCM I-745 on the gut-associated immune system. Clinical and Experimental Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/27695355/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Jiang YZ, et al. (2025). Effect of Saccharomyces boulardii supplementation to bismuth quadruple therapy on Helicobacter pylori eradication. BMC Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/40251486/ ↩︎ ↩︎ ↩︎
Fu H, et al. (2022). Effectiveness and Safety of Saccharomyces Boulardii for the Treatment of Acute Gastroenteritis in the Pediatric Population: A Systematic Review and Meta-Analysis. Computational and Mathematical Methods in Medicine. https://pubmed.ncbi.nlm.nih.gov/36176742/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Li T, McFarland LV. (2026). Saccharomyces boulardii CNCM I-745 and smectite treatment for pediatric acute gastroenteritis in China: a systematic review and meta-analysis. Frontiers in Pediatrics. https://pubmed.ncbi.nlm.nih.gov/41798274/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sivananthan K, Petersen AM. (2018). Review of Saccharomyces boulardii as a treatment option in IBD. Immunopharmacology and Immunotoxicology. https://pubmed.ncbi.nlm.nih.gov/29771163/ ↩︎ ↩︎ ↩︎
Maslennikov R, et al. (2024). Effect of Saccharomyces boulardii on Liver Diseases: A Systematic Review. Microorganisms. https://pubmed.ncbi.nlm.nih.gov/39203520/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎