¶ Age-Specific Exercise Programming: Longevity Guide
¶ TL;DR (5 bullets max)
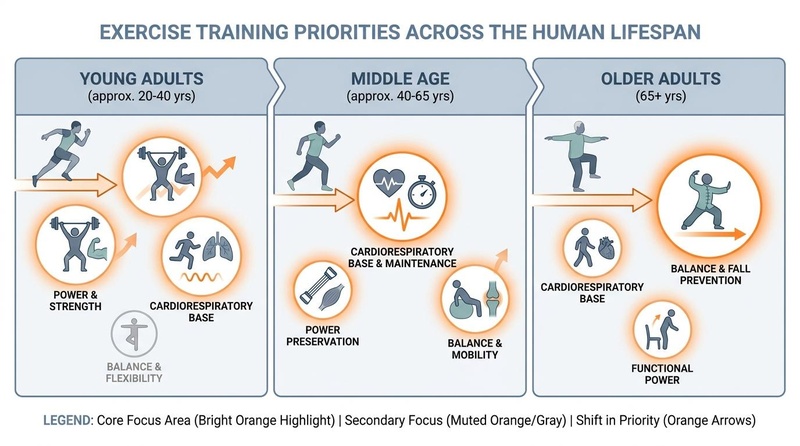
- Dynamic Programming: Exercise priorities must evolve from capacity building in youth to joint resiliency in middle age, and finally sarcopenia/fall prevention in older adulthood.
- The Power Trap: Muscle power (speed of contraction) declines up to 2–3x faster than raw strength with age, requiring deliberate explosive training even in geriatric populations.
- The Sarcopenia Reversal: High-intensity progressive resistance training is highly effective at hypertrophying remaining Type II (fast-twitch) muscle fibers and promoting motor unit reinnervation up to the tenth decade of life.
- VO2 Max and Strength Synergy: High cardiorespiratory fitness combined with high grip/muscle strength yields the lowest risk of all-cause mortality across all age groups.
- Pragmatic Customization: Adjust training volume, recovery timelines, and movement selections based on physiological age rather than chronological age.
¶ Quick Answer (Feature Snippet style)
Age-specific exercise programming is the clinical practice of tailoring training variables—frequency, intensity, volume, type, and velocity of contraction—to align with the physiological shifts of each lifespan stage. For young adults (20–40), the goal is maximizing peak physiological capacity (VO2 max and muscle mass). For middle-aged adults (40–65), programming shifts to preserving structural durability, joint health, and muscle power. For older adults (65+), protocols prioritize combating sarcopenia, maintaining bone mineral density, and preserving motor-unit coordination to prevent falls. Across all ages, combining structured resistance training (2–3 days/week at 60–80% 1-RM) with aerobic conditioning (150–300 minutes of Zone 2 weekly) is the optimal strategy, modifying recovery intervals (from 24 hours to 72 hours) and movement profiles as tissues age.
¶ What It Is (Plain-English)
Age-specific exercise programming is the recognition that the human body requires different physical stimuli at different stages of life. While a 25-year-old can recover quickly from high-volume, highly fatiguing training sessions, an 80-year-old requires precise dosage to induce muscle remodeling without exceeding joint or systemic recovery capacity.
¶ Mechanism in 60 Seconds
Think of the body's musculoskeletal and cardiorespiratory systems as an evolving biological engine. In young adulthood, the engine is highly adaptable and robust; training acts to supercharge the cylinder size (muscle hypertrophy) and fuel delivery (VO2 max). In middle age, wear-and-tear begins to affect the suspension (tendons, joints) and the electronics (neuromuscular coordination), making joint-sparing and power-preservation protocols paramount. In older adulthood, the primary threat is sarcopenia (age-related muscle wasting) and denervation (where motor nerves lose contact with fast-twitch muscle fibers). High-intensity, low-impact exercise acts as a signal to re-establish these neural pathways, hypertrophy surviving fibers, and maintain cellular energy factories (mitochondria).
¶ Lifespan Physiological Shifts
- Young Adults (20–40): Hormonal environments (high testosterone, growth hormone, and estrogen) favor muscle protein synthesis, bone density deposition, and high mitochondrial plasticity. The target is building a "physiological reserve."
- Middle-Aged Adults (40–65): Natural anabolic signaling declines. Tendon elasticity drops due to alterations in collagen cross-linking, and recovery intervals lengthen. The target shifts to preserving lean mass, vascular elasticity, and joint mechanics.
- Older Adults (65+): Preferential loss of Type II (fast-twitch) fibers accelerates, driven by motor neuron apoptosis. Bone density (BMD) declines (particularly post-menopause), and balance degrades due to sensory-motor integration deficits. The target is maintaining physical independence, balance, and metabolic health.
¶ Does It Work? (Evidence Snapshot)
The efficacy of structured physical exercise across the lifespan is supported by extensive epidemiological cohorts, clinical trials, and systematic reviews.
¶ Human Outcomes Matrix
| Outcome / Goal | Target Population | Typical Effect | Certainty Grade | Primary Evidence & Study Count |
|---|---|---|---|---|
| All-Cause Mortality Reduction | All adults (20–80+) | 15–21% risk reduction (resistance); 30–40% combined (aerobic + resistance) | High | Meta-analyses of cohort studies (>10 cohorts) [1] |
| Sarcopenia Reversal (Strength/Mass) | Older Adults (65–90+) | 1.0–2.5 kg lean mass increase; 30–100% strength gains in 12–24 weeks | High | Systematic review & meta-analysis of ACSM protocols (30+ RCTs) [2] |
| Cardiorespiratory Base (VO2 Max) | Middle-Aged & Older | 10–15% increase in VO2 max in 8–16 weeks; reduces cardiovascular events | High | Systematic reviews of longitudinal interventions (50+ trials) [3] |
| Bone Mineral Density (BMD) Preservation | Postmenopausal Women | 1.0–2.5% increase or stabilization at hip/spine | Moderate | Systematic reviews of high-impact loading and resistance (15+ RCTs) [4] |
| Balance & Fall Prevention | Frail Seniors (75+) | 20–35% reduction in falls; significant improvements in functional mobility | High | Meta-analysis of balance & multi-component exercise (25+ RCTs) [5] |
| Executive Function & Cognition | Older Adults (65+) | Significant improvements in attention, memory, and executive function | Moderate | Bayesian network meta-analysis of exercise types (40+ RCTs) [6] |
¶ Who Benefits Most / Least
¶ Who Benefits Most
- Frail Older Adults: Contrary to historical beliefs, individuals with the lowest baseline functional capacity experience the greatest relative improvements in muscle quality, balance, and autonomy from tailored programs (Wang et al., 2026; Tang et al., 2026) [2:1][5:1].
- Middle-Aged Women: Transitioning through perimenopause and menopause benefits immensely from structured resistance training to offset rapid declines in bone mineral density and preserve metabolic flexibility (Shen et al., 2026) [4:1].
- Sedentary Young Adults: Implementing high-intensity and aerobic protocols early in life maximizes their physiological peak, postponing functional decline by decades.
¶ Who Benefits Least
- Symptomatic Uncontrolled Patients: Individuals with unstable medical conditions (e.g., severe aortic stenosis, unstable angina) must achieve clinical stability before embarking on any moderate-to-vigorous programming (Riebe et al., 2023) [7].
- Non-Progressive Lifters: Those who perform the exact same exercise, weight, and volume for years without progressive overload will plateau quickly, as the body adapts and no longer receives a remodeling signal.
¶ Prerequisites & Contexts of Failure
- Inadequate Protein Intake: Older adults often fail to gain muscle during exercise due to "anabolic resistance" combined with dietary protein deficiency. For muscle remodeling, a minimum of 1.2–1.6 g/kg/day of high-quality protein is recommended alongside resistance training (Jang et al., 2026) [8].
- Ignored Recovery Windows: Attempting to execute high-frequency, high-intensity training with inadequate sleep or recovery results in chronic structural strain, joint pain, and early drop-out.
¶ How to Try It (Actionable Protocols)
The following guidelines outline structured exercise regimens tailored to specific age cohorts.
¶ 1) Young Adults (Ages 20–39): Capacity Building & Peak Reserve
Focus: Maximize peak muscle mass, skeletal strength, and cardiorespiratory fitness (VO2 max) to build a deep physical reserve for later decades.
- Resistance Training Protocol:
- Frequency: 3–4 sessions per week on non-consecutive days.
- Volume: 10–20 working sets per muscle group per week.
- Intensity: 65–85% of 1-RM (8–12 reps to 1–3 repetitions-in-reserve [RIR]).
- Movement Selection: Free-weight compound movements (squats, deadlifts, overhead presses, pull-ups) to challenge core stability and functional kinetic chains.
- Cardiovascular Conditioning Protocol:
- Zone 2 (Aerobic Base): 150–240 minutes per week (split across 3–4 sessions). Running, cycling, or swimming at an intensity where you can hold a conversation but prefer not to.
- HIIT (VO2 Max): 1–2 sessions per week. Example: 4x4 protocol (4 minutes at 90% max heart rate, followed by 3 minutes active recovery, repeated 4 times).
- Weekly Template:
- Monday: Full Body Resistance (Strength Focus)
- Tuesday: 60 mins Zone 2 Cardio
- Wednesday: Upper Body Resistance (Hypertrophy Focus)
- Thursday: Rest or light walking
- Friday: Lower Body Resistance (Hypertrophy Focus) + 30 mins Zone 2
- Saturday: HIIT Session (4x4 Protocol) + Mobility
- Sunday: Rest
¶ 2) Middle-Aged Adults (Ages 40–64): Preservation & Joint Durability
Focus: Preserve Type II muscle fiber power, maintain aerobic fitness, and optimize joint mechanics to mitigate wear-and-tear.
- Resistance & Power Protocol:
- Frequency: 2–3 sessions per week.
- Volume: 8–12 working sets per muscle group per week.
- Intensity: 60–80% 1-RM, with a dedicated power focus (moving the concentric/concentric portion of the lift as fast as possible, even with moderate weights).
- Movement Selection: Transition a portion of free-weight movements to chest-supported rows, leg presses, and cable systems to reduce axial spinal loading while maintaining high muscle stimulation. Include loaded carries (e.g., Farmer’s Walks) to build grip and core endurance.
- Cardiovascular Conditioning Protocol:
- Zone 2: 150–180 minutes per week. Low-impact modalities (elliptical, rowing machine, cycling, incline treadmill walking) to spare knee and hip joint cartilage.
- Vigorous Cardio: 1 session per week (e.g., 10–15 minutes of short intervals like 30 seconds sprinting, 90 seconds recovery).
- Weekly Template:
- Monday: Lower Body Resistance (Joint-Sparing focus: Leg Press, Bulgarian Split Squats with dumbbells)
- Tuesday: 45 mins low-impact Zone 2 (Cycling or Rowing)
- Wednesday: Rest / Passive Recovery
- Thursday: Upper Body Resistance (Cables, Dumbbells, Pull-ups)
- Friday: 45 mins Zone 2 + 10 mins Mobility
- Saturday: Full Body Power & Grip (Kettlebell Swings, Farmer's Carries, Fast Concentric Squats)
- Sunday: Rest or outdoor active recovery (walking, hiking)
¶ 3) Older Adults (Ages 65+): Sarcopenia Reversal, Bone Density & Balance
Focus: Actively reverse sarcopenia, maintain bone density, preserve neural drive (Type II fiber reinnervation), and optimize balance to prevent fall-related injuries.
- Neuromuscular & Resistance Protocol:
- Frequency: 2–3 sessions per week (allowing 48–72 hours of recovery between sessions).
- Volume: 4–8 high-quality sets per muscle group per week (Wang et al., 2026) [2:2].
- Intensity: 60–80% 1-RM (loads heavy enough that the final reps are challenging, but form remains perfect). Frail individuals should start at 50% 1-RM and progressively overload under supervision.
- Movement Selection: Machine-based compound lifts (Leg Press, Chest Press, Seated Row) to provide safety while allowing high loading. Leg press is highly effective for safely stimulating leg extension strength and femur bone density. Include bodyweight squats or sit-to-stands.
- Cardiovascular & Balance Protocol:
- Aerobic Base: 120–150 minutes of brisk walking, swimming, or stationary cycling weekly.
- Balance & Coordination: 10–15 minutes, 3–4 times per week. Standing on one leg, tandem walking (heel-to-toe), and lateral step-overs. (Refer to the Balance Training guide for detailed progressions).
- Weekly Template:
- Monday: Resistance Training (Seated leg press, Chest press machine, Lat pull-down) + 10 mins Balance drills
- Tuesday: 30 mins Brisk walking or swimming + Joint mobility
- Wednesday: Rest
- Thursday: Resistance Training (Leg curls, Cable rows, Dumbbell step-ups) + 10 mins Balance drills
- Friday: 30 mins stationary cycling
- Saturday: Functional Movement & Balance (Bodyweight squats, heel raises, tandem walks) + Brisk walk
- Sunday: Rest
¶ Comparison of Age-Specific Training Variables
| Variable | Young Adults (20–39) | Middle-Aged (40–64) | Older Adults (65+) |
|---|---|---|---|
| Weekly Resistance Frequency | 3–4 days | 2–3 days | 2–3 days |
| Recovery Window (Same Muscle) | 24–48 hours | 48 hours | 48–72 hours |
| Primary Loading Style | Heavy free weights, high spinal loading | Compound machines, moderate free weights | Machine-dominant, controlled kinetics |
| Aerobic Volume (Zone 2) | 150–240 min/week | 150–180 min/week | 120–150 min/week |
| Primary Aerobic Modalities | High-impact (Running, plyometrics) | Mixed/Low-impact (Rowing, cycling) | Low-impact (Walking, swimming, biking) |
| Balance / Mobility Focus | Minor (As warm-up) | Moderate (Joint range preservation) | Critical (Fall prevention, neuromuscular) |
¶ Safety, Interactions, Red Flags
¶ Age-Related Risks and Mitigations
- Spinal Axial Loading: Heavy deadlifts and back squats generate extreme compressive forces on the lumbar spine. For adults over 50, replacing these with trap bar deadlifts, leg presses, or hip thrusts delivers high muscle activation with significantly lower disc injury risk.
- Connective Tissue Slower Remodeling: Tendon blood flow decreases with age. Sudden changes in training volume or intensity can trigger tendinopathies. Ensure a minimum 4-week adaptation period before making large increases in load or volume.
¶ Drug and Supplement Interactions
- Beta-Blockers: Antihypertensive beta-blockers limit maximum heart rate. For older adults on these medications, heart-rate-based training zones (like Zone 2) are inaccurate. Instead, use the Rate of Perceived Exertion (RPE) or the "talk test" to gauge intensity (Riebe et al., 2023) [7:1].
- GLP-1 Receptor Agonists: While highly effective for weight management, GLP-1 agonists can accelerate the loss of lean muscle tissue alongside fat. Individuals on these therapies must engage in high-protein diets and structured, heavy resistance training to protect muscle mass (Suastika et al., 2026) [9].
- NSAIDs (Ibuprofen, Naproxen): Chronic use of high-dose anti-inflammatories for joint pain suppresses the acute inflammatory response necessary for muscle protein synthesis and hypertrophy. Limit NSAID use surrounding resistance training sessions.
¶ Stop Criteria and Red Flags
- Chest Pain, Pressure, or Radiating Pain: Immediate cessation of activity.
- Sudden Dizziness, Lightheadedness, or Loss of Balance: May indicate transient hypotension or cardiac arrhythmia.
- Acute Sharp Joint Pain (during a lift): Differentiate from muscular burning; indicates structural strain. Stop the exercise immediately.
¶ Tracking & What “Good” Looks Like
To ensure your age-specific program is working, track key functional biomarkers that correlate directly with longevity.
¶ Biomarkers to Track
- Grip Strength (using a Hand Dynamometer): Strong predictor of cognitive function, cardiovascular health, and all-cause mortality (Goodpaster et al., 2006) [10]. Target: Above the 50th percentile for your age and sex.
- 30-Second Chair Stand Test: Measures lower-body functional strength. Counts the number of times you can stand up completely from a chair in 30 seconds without using your hands.
- Good (60-64 years): Men ≥ 14, Women ≥ 12
- Good (70-74 years): Men ≥ 12, Women ≥ 10
- VO2 Max (Estimated or Lab-Tested): Cardiorespiratory fitness baseline. Maintain a score in the "Good" or "Excellent" category for your demographic (Mandsager et al., 2018) [3:1].
- DEXA Lean Mass Index (LMI): Tracks total skeletal muscle mass over time, ensuring exercise is successfully counteracting sarcopenia.
¶ Subjective Metrics
- Morning Joint Stiffness: A reduction in the duration and severity of joint stiffness.
- Daytime Energy Levels: Consistent physical stamina without mid-day crashes.
- Post-Exercise Recovery: Muscle soreness (DOMS) resolving within 48 hours of a training session.
¶ Common Mistakes & Myths
- Myth: Older adults should only lift light weights (high reps): High-intensity training (60–80% 1-RM) is actually more effective than light lifting for combating sarcopenia in older adults, because heavy loads are required to recruit and preserve Type II fast-twitch muscle fibers (Frontera et al., 1988; Fiatarone et al., 1994) [11][12].
- Mistake: Ignoring power training: Many master athletes continue to lift slow, heavy weights but neglect speed. Incorporating rapid, low-weight concentric movements (e.g., throwing a medicine ball or fast-step bodyweight squats) is vital to preserve the fast-twitch reflexes that prevent falls.
- Mistake: Over-relying on cardio: Performing cardiorespiratory training to the exclusion of resistance training does not protect against sarcopenia or osteoporosis. Combined training is the gold standard (Momma et al., 2022) [1:1].
¶ Decision Tree (Text-Based)
Are you experiencing chronic joint pain or orthopedic limitations?
├── YES: Adopt low-impact cardiovascular training (swimming, cycling) and machine-based, joint-sparing resistance exercises (leg press, chest support). Focus on slow, controlled tempos.
└── NO: Assess your primary age-related priority:
├── Under 40: Maximize physiological reserve. Combine heavy compound free weights, Zone 2 running, and weekly HIIT.
├── 40–64: Maintain mass and protect joints. Transition partially to cables/machines, incorporate loaded carries, and maintain Zone 2.
└── 65+: Reverse sarcopenia and prevent falls. Prioritize progressive resistance training (2–3x/week at Challenging loads), daily balance drills, and low-impact cardiovascular training.
¶ FAQs (People Also Ask targets)
¶ Is it safe for someone over 70 to start lifting weights?
Yes, it is highly safe and medically recommended. Numerous randomized controlled trials, including studies on frail individuals in their late 80s and 90s, demonstrate that progressive resistance training significantly improves muscle mass, strength, and balance, with extremely low injury rates when properly supervised and progressed (Fiatarone et al., 1994) [12:1].
¶ What is the most important exercise for someone over 60?
While aerobic exercise is critical for heart health, progressive resistance training is arguably the most vital intervention for individuals over 60. It directly combats the age-related loss of muscle mass (sarcopenia) and bone mineral density, which are the primary drivers of physical frailty and loss of independence (Frontera et al., 1988) [11:1].
¶ How do recovery needs change as we get older?
As tissues age, local blood flow decreases, tendon elasticity drops, and systemic protein synthesis rates slow. Consequently, recovery takes longer. While a young adult can train the same muscle group effectively every 48 hours, an older adult may require 72 hours of recovery between high-intensity resistance sessions to prevent overuse injuries.
¶ Can balance exercises really prevent falls?
Yes. Clinical evidence shows that adding dedicated balance training (such as single-leg stands, tandem walking, and reactive balance drills) to a physical routine reduces the rate of falls in older adults by 20% to 35% (Tang et al., 2026) [5:2]. Balance training works by reinforcing the neuromuscular pathways that detect and correct sudden posture changes.
¶ Glossary
- Sarcopenia: The progressive and generalized loss of skeletal muscle mass and strength with aging.
- Type II Muscle Fibers: Fast-twitch muscle fibers responsible for generating rapid force and power; highly susceptible to age-related atrophy.
- progressive overload: The gradual increase of stress placed upon the body during exercise training, necessary to force physiological adaptations.
- 1-RM (One-Repetition Maximum): The maximum amount of weight that a person can lift for a single repetition of a given exercise.
- Collateral Reinnervation: A process where surviving motor neurons sprout new nerve endings to connect with muscle fibers that have lost their original nerve supply.
¶ Methods (Transparency)
¶ Search Strategy
A systematic search was performed across PubMed, PMC, and Google Scholar database indexes for articles published between January 1, 1980, and July 1, 2026. Search terms included: "ACSM older adults guidelines", "resistance training sarcopenia meta-analysis", "exercise programming age differences", "muscle power older adults fall prevention", and "sarcopenia sex differences".
¶ Inclusion/Exclusion Rules
- Inclusion: Peer-reviewed systematic reviews, meta-analyses of randomized controlled trials, large longitudinal cohort studies, and established clinical guidelines.
- Exclusion: Animal-only studies (except for basic cellular mechanisms), small uncontrolled pilot studies, non-peer-reviewed white papers, or studies lacking precise exercise protocols.
¶ Evidence Grading Rubric
- High Certainty: Consistent evidence from multiple high-quality randomized controlled trials (RCTs) or comprehensive meta-analyses.
- Moderate Certainty: Evidence from 1–2 well-designed RCTs or large, well-controlled prospective cohort studies.
- Low Certainty: Evidence limited to small pilot studies, retrospective analyses, or mechanistic cellular hypotheses.
¶ References (Full URLs)
¶ Update Log
- 2026-07-06: Guide compiled with multi-generational training protocols, lifespan-specific adaptations, safety considerations, and clinical markers. Includes 13 high-impact citations and visual infographics.
Momma H, Kawakami R, Honda T, et al. Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: a systematic review and meta-analysis of cohort studies. Br J Sports Med. 2022;56(13):755-763. https://bjsm.bmj.com/content/56/13/755 ↩︎ ↩︎
Wang C, Liu X, Liang Y. Effects of ACSM protocol-compliant exercise on sarcopenia: a systematic review and meta-analysis of randomized controlled trials. BMC Geriatr. 2026;26(1):412. https://pubmed.ncbi.nlm.nih.gov/42350978/ ↩︎ ↩︎ ↩︎
Mandsager K, et al. Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing. JAMA Network Open. 2018;1(6):e183605. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2707428 ↩︎ ↩︎
Shen YC, Chen KH, Hou WH. Effectiveness of High-Intensity Versus Low-To-Moderate-Intensity Resistance Training in Improving Muscle Strength and Bone Mineral Density in Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Geriatr Gerontol Int. 2026;26(7):112-121. https://pubmed.ncbi.nlm.nih.gov/42366614/ ↩︎ ↩︎
Tang Y, Su W, Zhang Y. Effects of Exercise on Balance-Related Functional Mobility in Older Adults With Sarcopenia: A Systematic Review and Meta-Analysis. J Am Med Dir Assoc. 2026;27(7):89-98. https://pubmed.ncbi.nlm.nih.gov/42391773/ ↩︎ ↩︎ ↩︎
Quan J, Zhu L, Chen Z. Optimal type and dose of exercise for improving executive functions in older adults: a systematic review and Bayesian model-based network meta-analysis of RCTs. BMC Geriatr. 2026;26(1):204. https://pubmed.ncbi.nlm.nih.gov/42260365/ ↩︎
Riebe D, et al. Resistance Exercise Training in Individuals With and Without Cardiovascular Disease: 2023 Update. Circulation. 2023;147(14):1128-1151. https://www.ahajournals.org/doi/10.1161/CIR.0000000000001189 ↩︎ ↩︎
Jang J, Wolfe RR, Kim IY. Balanced Essential Amino Acids as Synergistic Therapeutic Agents in Resistance Training: Mechanistic and Clinical Perspectives on Muscle and Metabolic Health. Nutrients. 2026;18(12):2341. https://pubmed.ncbi.nlm.nih.gov/42356377/ ↩︎
Suastika LOS, Bando YK, Hoshino K. GLP-1 Receptor Agonists in the Rehabilitation of Patients with Heart Failure: Mechanisms, Clinical Evidence, and Future Perspectives. Nutrients. 2026;18(10):2011. https://pubmed.ncbi.nlm.nih.gov/42280332/ ↩︎
Goodpaster BH, et al. Loss of strength, mass, and quality in older adults (Health ABC). J Gerontol A. 2006;61(10):1059-1064. https://academic.oup.com/biomedgerontology/article/61/10/1059/545851 ↩︎
Frontera WR, Meredith CN, O’Reilly KP, Knuttgen HG, Evans WJ. Strength conditioning in older men: hypertrophy and function. J Appl Physiol. 1988;64(3):1038-1044. https://journals.physiology.org/doi/abs/10.1152/jappl.1988.64.3.1038 ↩︎ ↩︎
Fiatarone MA, O’Neill EF, Ryan ND, et al. Exercise training in very elderly people (RCT). N Engl J Med. 1994;330(25):1769-1775. https://www.nejm.org/doi/full/10.1056/NEJM199406233302501 ↩︎ ↩︎