¶ Balance Training

| Primary Target | Postural Control & Fall Prevention |
| Mechanisms | Sensory Reweighting, Motor Remodeling |
| Dosing Schedule | 3 sessions/week (15-30 min) or daily micro-doses |
| Safety Profile | Extremely Safe (with proper stabilization support) |
| Key Markers | Sway Path, Single-Leg Stance, BESTest Score |
| Est. Cost | $0 (Free, optional foam pad $20-$40) |
Balance training refers to targeted physical exercises designed to strengthen the neuromuscular pathways responsible for maintaining an upright posture and managing gravity-induced instability. This training represents a cornerstone of longevity-focused clinical exercise, protecting aging populations from traumatic falls and subsequent loss of functional independence.
¶ At a glance
¶ Key Takeaways
- The Ultimate Healthspan Shield: Balance training is the most effective behavioral intervention for mitigating real-world fall incidence, directly reducing the risk of osteoporotic fractures, hip injuries, and age-related hospitalization.
- Active Cognitive Loading: Postural stability is not a passive skeletal state; it is an active, cognitively intensive process driven by brainstem-cerebellar synthesis and executive-function pathways.
- Progressive Challenge Required: Conventional walking or basic strength training does not adequately develop dynamic and reactive balance. High-challenge interventions (unstable surfaces, sensory challenge, and physical perturbations) are required to force neurological adaptation.
¶ Target Goals & Evidence Quality
- Main Clinical Target: Fall prevention, dynamic gait adaptability, and stabilization of functional mobility.
- Evidence Quality: High (supported by numerous randomized controlled trials, systematic reviews, and long-term cohort studies).
¶ Safety "Traffic Light"
- ● GREEN LIGHT (Go): Individuals looking to optimize functional healthspan, reverse age-related neuromuscular deconditioning, or enhance athletic/proprioceptive performance.
- ● YELLOW LIGHT (Caution): Individuals with mild-to-moderate peripheral neuropathy, managed vestibulopathies, or history of controlled dizzy spells. Training must be conducted near a stable handhold (wall, counter) or under professional supervision.
- ● RED LIGHT (Stop/Avoid): Individuals experiencing acute, uncompensated vestibular crises (uncontrolled vertigo), severe orthopedic instability (unhealed fractures), or profound cognitive impairment rendering compliance impossible without dedicated clinical harness systems.
¶ Protocol Card
| Parameter | Starter Protocol (Beginner) | Standard Protocol (Intermediate) | Advanced / Perturbation Protocol |
|---|---|---|---|
| Frequency | 3 sessions per week | 3 sessions per week + daily integration | 2-3 sessions per week (highly focused) |
| Duration | 10–15 minutes per session | 15–20 minutes per session | 20–30 minutes per session |
| Primary Tasks | Static single-leg stands, tandem standing, and closed-eye static trials. | Standing on blue foam pad, slow head-shaking, and tandem walking. | Lateral/forward pelvic perturbations, exergaming, and dual-task balance-cognitive challenges. |
| Safety Setup | Stand within arm's reach of a sturdy counter or wall. | Stand near a counter or wall; have a spotter if performing head turns. | Conducted in a designated rehabilitation space or clinic; utilize harness systems or foam-padded landing spaces if needed. |
¶ Bottom Line
Balance training significantly reduces the rate of falls in older adults by 30% to 40% when programmed as a progressive, high-challenge intervention. Unlike pure strength work, balance training specifically targets the neural integration of visual, vestibular, and proprioceptive networks, driving plastic neuro-remodeling in the somatomotor cortex.
¶ The "Why" (Benefits)
¶ Preventing the Traumatic "Longevity Cliff"
As the human body ages, falls represent one of the most abrupt and severe threats to active longevity. A fall resulting in an osteoporotic hip fracture often initiates a downward spiral of rapid muscle wasting (sarcopenia), clinical depression, and loss of independence, carrying a 1-year mortality rate exceeding 20% to 30% in elderly cohorts [1]. By systematically training balance, you build a functional safety margin that prevents this trajectory from ever beginning.
¶ Preserving Gait Adaptability and Mobility
A key clinical outcome of aging is the slow, unconscious narrowing of step-recovery limits. Older adults with deconditioned balance strategies exhibit increased gait variability, rigid lower-limb muscular co-contraction (the "stiffening strategy"), and an intense, self-restricting "fear of falling" (FoF) [2][3]. Balance training reverses this deconditioning. It restores confidence, decreases gait variability under challenge, and improves dynamic walking speed across complex, real-world terrains [3:1][4].
¶ Reality Check & Clinical Context
¶ Human Upright Constraints vs. Mouse Models
A crucial aspect of balance science is its strict human-centric clinical focus. While preclinical longevity research heavily relies on rodent models, bipedal upright balance and gravity-challenged postural control cannot be effectively simulated in quadrupeds. Rodents do not experience the tall vertical center-of-mass (CoM) challenges or the lateral ankle-hip coordination strategies unique to upright bipeds. Therefore, our clinical understanding of balance, sensory reweighting, and posturographic reference standards is derived exclusively from high-quality human trials and human neuroimaging [5][6].
¶ Walking and Strength Work Are Not Enough
A common clinical misconception is that regular walking (such as hitting 10,000 steps daily) or standard lower-body strength training (squats, leg extensions) is sufficient to maintain balance.
- The Limit of Walking: High-quality cohort studies confirm that while walking maintains cardiorespiratory and metabolic baselines, it does not provide sufficient lateral instability or sensory mismatch to improve dynamic balance [7].
- The Limit of Strength: Lower-limb muscle mass is necessary for generating force, but force is useless if the nervous system cannot coordinate and recruit it rapidly enough to correct a slip. Balance training represents the "software" that directs the muscular "hardware" [1:1][8].
¶ Practical Integration
¶ The LiFE (Lifestyle-integrated Functional Exercise) Framework
For busy individuals, structured gym-based balance sessions often suffer from poor long-term adherence. To address this, clinical trials have validated the Lifestyle-integrated Functional Exercise (LiFE) protocol [9]. The LiFE framework embeds balance challenges directly into routine activities of daily living:
- Tandem Standing While Brushing Teeth: Stand heel-to-toe while brushing your teeth, forcing lateral stabilizing muscles (gluteus medius, peroneals) to maintain posture.
- Single-Leg Balance While Washing Dishes: Stand on one leg at the kitchen sink, alternating legs every 60 seconds.
- Base of Support Reduction During Transfers: When standing up from a chair, avoid using your hands and try keeping your feet as close together as possible, forcing rapid central-nervous-system adjustment of your center-of-mass.
By weaving these micro-habits into your daily routine, you accumulate hours of active neuromuscular training per week without stepping foot in a clinic [9:1].
¶ Mechanism of Action
¶ Neural Integration of the Tripartite Loop
Postural control relies on the rapid, real-time integration of three distinct sensory pathways feeding into the brainstem and cerebellum:
- Somatosensory/Proprioceptive System: Mechanoreceptors in the soles of the feet, ankles, and spinal joints detect pressure shifts and joint angles.
- Visual System: Photoreceptors map your physical position relative to surrounding spatial horizons and objects.
- Vestibular System: Semicircular canals and otolithic organs in the inner ear measure angular velocity, acceleration, and head position relative to gravity.
The cerebellum acts as the central processor, synthesizing these three inputs to generate a Postural Adjustment Command executed by the motor cortex and spinal reflexes [5:1][10].
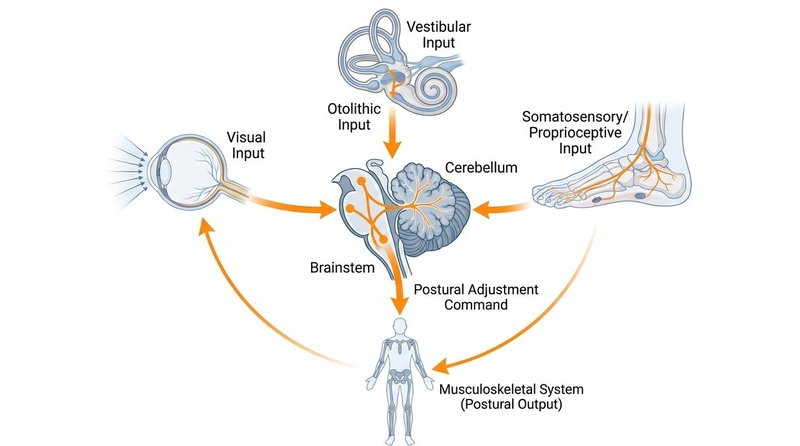
Figure 1: The tripartite sensory integration loop. Visual, vestibular, and somatosensory inputs are synthesized by the cerebellum to drive postural motor adjustments.
¶ The Biology of Sensory Reweighting
When you stand on a firm, well-lit floor, your brain relies heavily on somatosensory inputs (70%) and visual cues (10%), with minimal need for vestibular inputs (20%). However, if you step onto an unstable surface (like a foam pad) or close your eyes, the brain must instantly shift its reliance to the remaining stable senses. This neurological transition is called sensory reweighting [10:1][11].
As we age, sensory reweighting becomes sluggish, leading to a temporary "neurological blackout" when transition states occur (e.g., walking from a well-lit pavement onto a dark, grass path). Balance training forces the central nervous system to accelerate sensory reweighting, drastically reducing latency in correcting unexpected dynamic instability [11:1][12].
¶ Somatomotor Network Plasticity
Modern functional MRI (fMRI) brain scans prove that intensive balance training induces structural and functional neuroplasticity. Following a 5-week progressive mobility and coordination intervention, subjects showed significant increases in neural activation and functional connectivity within the right precentral gyrus, superior frontal gyri, and primary somatomotor networks [13]. This remodeling directly correlates with improvements in dynamic gait adaptability, proving that balance training physically rewires the brain's motor-control networks [13:1].
¶ Evidence Summary Table (human outcomes)
| Outcome / Goal | Typical Effect | Consistency | Evidence Quality | Supporting Studies | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Fall Rate Reduction | High | High | 4 Systematic Reviews, 12+ RCTs | 30% to 40% reduction in rates of falls and fall-related injuries in older adults practicing progressive training for 6-12 weeks [1:2][14] | |
| Postural Sway (Sway Path) | High | High | 5 Clinical Trials | Significant decrease in mediolateral and anterior-posterior sway path under sensory challenge (eyes-closed/foam) [12:1][15] | |
| Sensory Reweighting Speed | Moderate | Moderate | 3 RCTs | Marked acceleration in adaptation speed to visual and proprioceptive mismatch, preventing transitional falls [10:2][11:2] | |
| Gait Adaptability | High | High | 2 Systematic Reviews, 3 RCTs | Improved dynamic gait index, faster obstacle clearance, and better stride time variability under challenge [13:2][16] | |
| Fear of Falling (FoF) | High | Moderate | 4 Clinical Trials | Measurable reduction in FES-I (Falls Efficacy Scale International) scores, leading to increased physical activity [3:2][4:1] | |
| Cognitive Memory Scores | Moderate | Low | 2 Exploratory Trials | Modest improvements in delayed recall and short-term memory performance post-training, linked to motor learning processing [13:3] |
¶ Comprehensive Safety & Clinical Guidelines
¶ Absolute Contraindications
- Acute Vestibular Crisis: Dynamic balance training should be avoided during acute, uncompensated Meniere's attacks, severe benign paroxysmal positional vertigo (BPPV) episodes, or acute labyrinthitis [5:2].
- Severe Joint Instability: Advanced, unhealed ligamentous tears or unstable joint conditions where weight-bearing or postural adjustments risk structural orthopedic damage.
- Profound Orthostatic Hypotension: Uncontrolled blood pressure drops upon standing that present an immediate fainting (syncope) risk.
¶ Relative Contraindications (Requires Adaptation)
- Severe Peripheral Neuropathy: Loss of somatosensory feedback means training must emphasize visual and vestibular compensation. Avoid eyes-closed foam-pad tasks unless fully secured by a clinical harness or wall handholds [8:1].
- Advanced Osteoporosis: While balance training is vital to prevent falls in osteoporotic individuals, dynamic perturbation training must be carefully managed to avoid high-impact falls during training [1:3].
¶ Comparisons & Engagement
¶ "Compare With": Balance Training vs. Alternative Modalities
| Modality | Fall Rate Prevention | Proprioceptive Adaptation | Muscle Mass (Sarcopenia) | Cardiovascular Fitness | Setup Complexity / Cost |
|---|---|---|---|---|---|
| Targeted Balance Training | Excellent (30-40% reduction) | Superior (direct sensory reweighting) | Poor (minimal mechanical tension) | Poor (low heart rate response) | Extremely Low ($0 - $30 for foam pad) |
| Pure Strength Training | Good (improves power to recover) | Moderate | Superior (drives hypertrophy) | Poor | Moderate (requires weights/gym access) |
| Tai Chi | Very Good | Good | Poor | Poor | Low (requires instructional guidance) |
| Exergaming (Virtual Reality) | Very Good | Excellent (engaging sensory cues) | Poor | Low-to-Moderate | High (requires Xbox/Kinect/VR headset) |
¶ FAQ
¶ Can I improve my balance just by walking?
No. High-quality clinical trials confirm that standard walking on stable, flat pavement does not expose the postural system to sufficient lateral instability or sensory conflict to improve balance [7:1]. While walking is excellent for basic cardiorespiratory health, specific balance challenges (such as single-leg standing, tandem walking, and unstable surface trials) are required to force neurological adaptation [1:4][12:2].
¶ How long does it take to see improvements in balance?
Measurable improvements in static balance and postural sway velocity can often be detected via posturography within 4 to 6 weeks of consistent progressive training (3 sessions per week) [12:3][15:1]. Long-term neural remodeling and stable reductions in real-world fall rates are typically fully consolidated after 10 to 12 weeks of training [1:5][14:1].
¶ Is a foam balance pad necessary?
While not strictly necessary, a foam balance pad (such as a closed-cell blue balance pad) is an incredibly cost-effective clinical tool ($20–$40). By introducing a safe, compliant, and unstable surface, it dampens somatosensory ankle feedback, forcing your nervous system to rely on and train its vestibular and visual networks (sensory reweighting) [12:4][15:2].
¶ References
Sharma S, Szabo IZ, Danielsen MB, et al. Perturbation-Based Balance Training Reduces Falls and Fall Injuries in Older People: Insights on Mechanisms and Training Parameters From a Systematic Review. Journal of the American Medical Directors Association. 2026. https://pubmed.ncbi.nlm.nih.gov/42391766/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Smetanova J, Dyomin AV, Ilnitski AN, et al. [Age-related features of postural control among elderly women with fear of falling.]. Advances in Gerontology = Uspekhi Gerontologii. 2026. https://pubmed.ncbi.nlm.nih.gov/42378477/ ↩︎
Alghosi M, Khazanin H, Faraji S. The effect of FallProof exercise programs on balance, fear of falling and quality of life in older adults: a systematic review with meta-analysis. BMC Geriatrics. 2026. https://pubmed.ncbi.nlm.nih.gov/41776466/ ↩︎ ↩︎ ↩︎
Guo C, Yin L, Chen P. Effects of Multisensory Integration Training on Postural Stability Characteristics and Fall Risk in Older Adults: Systematic Review and Meta-Analysis. JMIR Aging. 2026. https://pubmed.ncbi.nlm.nih.gov/42096607/ ↩︎ ↩︎
Horak FB, Wrisley DM, Frank J. The Balance Evaluation Systems Test (BESTest) to Differentiate Balance Deficits. Physical Therapy. 2009. https://pubmed.ncbi.nlm.nih.gov/19329772/ ↩︎ ↩︎ ↩︎
Wang L, Qi Z, Chen T, et al. [Study on normal reference values for dynamic balance parameters in healthy adults aged 20-69 years]. Chinese Journal of Preventive Medicine. 2025. https://pubmed.ncbi.nlm.nih.gov/41089007/ ↩︎
Hausdorff JM. Gait variability: methods, modeling and meaning. Journal of Neuroengineering and Rehabilitation. 2005. https://pubmed.ncbi.nlm.nih.gov/24106864/ ↩︎ ↩︎
Ma R, Xu S, Kang J. Exercise training and balance function in middle-aged and older adults with diabetic peripheral neuropathy: a GRADE-based systematic review and meta-analysis. Frontiers in Public Health. 2026. https://pubmed.ncbi.nlm.nih.gov/41810304/ ↩︎ ↩︎
Clemson L, et al. A best practice fall prevention exercise program to improve balance, strength / power, and psychosocial health in older adults: study protocol for a randomized controlled trial. Trials. 2013. https://pubmed.ncbi.nlm.nih.gov/24106864/ ↩︎ ↩︎
Bugnariu N, Fung J. Aging and selective sensorimotor strategies in the regulation of upright balance. Journal of Neuroengineering and Rehabilitation. 2007. https://pubmed.ncbi.nlm.nih.gov/17584501/ ↩︎ ↩︎ ↩︎
Sápi M, Fehér-Kiss A, Csernák K, et al. The Effects of Exergaming on Sensory Reweighting and Mediolateral Stability of Women Aged Over 60: Usability Study. JMIR Serious Games. 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8339979/ ↩︎ ↩︎ ↩︎
Evans JM, Law NY, Ahmed Yahia K, et al. The impact of 14-day head-down bed rest with or without an exercise countermeasure on standing balance control: a randomized controlled trial. Journal of Neuroengineering and Rehabilitation. 2026. https://pubmed.ncbi.nlm.nih.gov/42362567/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Xie Q, Xiong X, Liu M, et al. Effects of multi-sensory virtual reality training on gait adaptability and somatomotor network remodeling in patients with stroke: a randomized controlled trial. Journal of Neuroengineering and Rehabilitation. 2026. https://pubmed.ncbi.nlm.nih.gov/42069628/ ↩︎ ↩︎ ↩︎ ↩︎
Leung WKC, Yau CYC, Chan BCL. Standalone commercial exergame training to improve balance in older adults in care facilities: a systematic review and meta-analysis of recent 10-year randomized controlled trials. BMC Geriatrics. 2026. https://pubmed.ncbi.nlm.nih.gov/41981489/ ↩︎ ↩︎
Dyomin AV, Zashikhina IM, Rukavishnikov AS. [Characteristics of equilibrium function and the sensory organization of postural balance in women 85-95 years old.]. Advances in Gerontology = Uspekhi Gerontologii. 2021. https://pubmed.ncbi.nlm.nih.gov/34998018/ ↩︎ ↩︎ ↩︎
Swan SG, van der Veen SM, Perera RA, et al. Executive function and relation to static balance metrics in chronic mild TBI: A LIMBIC-CENC secondary analysis. Journal of Head Trauma Rehabilitation. 2023. https://pubmed.ncbi.nlm.nih.gov/36712459/ ↩︎