¶ Exercise Recovery: Deep Dive
Optimizing the post-exercise recovery window represents a primary clinical leverage point for accelerating muscle tissue repair, restoring autonomic nervous system (ANS) homeostasis, and enhancing long-term athletic adaptation. Rather than viewing recovery as a passive absence of training, sports medicine models frame recovery as an active, phase-dependent biological cascade that can be systematically accelerated or blunted through clinical programming.
¶ At a glance
- Verdict: Active and passive recovery modalities operate on distinct physiological timelines; integrating active movement optimizes metabolic clearance and proprioception, while structured passive protocols are mandatory for systemic neuromuscular restoration [1][2][3].
- Who it's for: Highly relevant for clinicians, hybrid athletes, and longevity-focused individuals seeking to accelerate tissue remodeling, preserve force generation capacity, and prevent cumulative performance decay [4][5].
- Expected Impact: Active recovery reduces acute muscle soreness by up to 30% [1:1], passive blood flow restriction restores isometric torque 24–48 hours sooner [6], and early carbohydrate ingestion completely restores impaired calcium kinetics within 4 hours [3:1].
- Key Risk(s): Cold-water immersion (CWI) within 4 hours of hypertrophic training blunts muscle protein synthesis and ribosome biogenesis [7]; premature aggressive loading during acute inflammatory injury phases triggers fibrotic tissue adhesions (arthrofibrosis) [8].
- What to do next: Program low-intensity active recovery (e.g., Zone 2 cardio) or foam rolling immediately post-exercise, implement passive blood flow restriction for severe muscle damage, and restrict cold exposure to non-hypertrophic training days [2:1][6:1].
¶ Quick Answer (Feature Snippet style)
Exercise recovery is a multi-dimensional physiological process requiring a structured integration of active and passive modalities. To accelerate local clearance of metabolic waste products, clinicians recommend 10–15 minutes of low-intensity active movement (e.g., active walking or light pedaling) to maintain elevated cardiac output without inducing further tissue micro-tears [9][10]. For structural myofibrillar repair, a minimum of 7–9 hours of optimized sleep is mandatory to facilitate pulsatile growth hormone and testosterone release [4:1][5:1]. Following severe exercise-induced muscle damage (EIMD), applying passive blood flow restriction (pBFR) at 80% arterial occlusion pressure for five 5-minute cycles accelerates the restoration of range of motion (ROM) and maximal voluntary isometric contraction (MVIC) torque within 24 hours, compared to 72+ hours under passive rest [6:2].
¶ What It Is (Plain-English)
Exercise recovery is the physiological transition of skeletal muscle tissue, the cardiorespiratory system, and the autonomic nervous system from an acute state of exertion-induced stress back to baseline homeostasis.
- What counts: Structured active recovery (submaximal, non-fatiguing movement designed to stimulate regional blood flow) [9:1][10:1], mechanical modalities (foam rolling, massage) [2:2][11], specialized compression (passive blood flow restriction) [6:3], and thermal or photobiomodulation treatments [12][13] integrated with sleep and hydration [4:2][5:2].
- What doesn’t count: Passive immobilization (prolonged sitting or lying down immediately after high-intensity exercise), random stretching without mechanical intent, or using anti-inflammatory drugs to mask muscle soreness, which actively blunts physiological adaptations.
¶ Mechanism in 60 Seconds: Simple Analogy & Key Pathways
Think of your skeletal muscle tissue as a high-performance racecar. During a race, metabolic exhaust accumulates, the structural frame incurs micro-damage, and fuel reserves are depleted. Simply parking the car in a garage (passive rest) allows cooling but does not actively clear the track or rebuild the engine.
Active recovery keeps the engine idling at a low speed. This low-intensity contraction acts as a skeletal muscle pump, accelerating the clearance of metabolic waste (such as blood lactate) through monocarboxylate transporters (MCTs) [9:2]. Mechanically, compression and foam rolling act as manual lymphatic pumps, restoring muscle spindle sensitivity and fascia sliding [2:3]. At the cellular level, the restoration of force generation relies on refilling the specific intramyofibrillar glycogen pool (representing 10–15% of total cellular glycogen), which directly fuels the sarcoplasmic reticulum (SR) calcium () release channels [3:2]. Without this local glycogen replenishment, calcium handling decays, inducing prolonged neuromuscular fatigue [3:3].
¶ Evidence summary table (human outcomes)
The clinical efficacy of various post-exercise recovery strategies is supported by a comprehensive matrix of randomized controlled trials (RCTs) and systematic reviews:
| Outcome | Typical Effect | Certainty | Timeframe | Citations |
|---|---|---|---|---|
| Metabolic Waste Clearance | Active interset rest and manual lymphatic pump techniques increase regional blood flow, clearing systemic blood lactate significantly faster than passive rest. | High | 10–30 minutes | [9:3][10:2] |
| Muscle Soreness (DOMS) Reduction | Active recovery, massage, and foam rolling provide the most robust reductions in delayed-onset muscle soreness and lower systemic creatine kinase (CK). | High | 24–72 hours | [1:2][11:1] |
| Neuromuscular Isometric Force (MVIC) | Passive blood flow restriction (pBFR) at 80% arterial occlusion pressure accelerates maximal torque recovery to baseline within 24 hours. | Moderate | 24–48 hours | [6:4] |
| Neuromuscular Proprioception & Balance | Foam rolling post-fatigue restores static and dynamic postural balance and preserves horizontal jump performance compared to passive rest. | High | Immediate post-treatment | [2:4] |
| Intramuscular Temperature Reduction | Whole-body cryotherapy (-110°C) and cold-water immersion (8°C) reduce vastus lateralis muscle temperature by 1.2–2.0°C. | High | 60 minutes post-treatment | [12:1] |
| Autonomic Reactivation (Vagal Tone) | Vagal reactivation can be accurately tracked via heart rate recovery (HRR) in the first 1–2 minutes using validated wrist PPG. | Moderate | 1–5 minutes | [14][15] |
| Postural Sway & Core Stability | Cumulative athletic fatigue significantly increases postural sway; targeted core retraining and sleep mitigate this drift. | Moderate | 24–96 hours | [5:3][16] |
| Ribosomal Biogenesis & Protein Turnover | Compounding mechanical overload with immediate heat therapy (EX+HT) suppresses muscle protein synthesis rate. | Moderate (Animal) | 14 days post-unloading | [7:1] |
¶ Mechanism of Action
¶ 1. Autonomic Nervous System & Vagal Tone Reactivation
During high-intensity training, the sympathetic nervous system dominates, driving elevated heart rate, catecholamine release (epinephrine and norepinephrine), and decreased heart rate variability (HRV) [15:1]. Post-exercise, the body must transition back to parasympathetic dominance—a process driven by vagal nerve reactivation and acetylcholine release [15:2].
This transition can be clinically tracked via Heart Rate Recovery (HRR) and the root mean square of successive differences (RMSSD) [14:1][15:3]. Rapid vagal reactivation is a hallmark of high cardiorespiratory fitness, and monitoring this curve via validated wrist-worn photoplethysmography (PPG) monitors provides a reliable surrogate of systemic recovery [14:2].
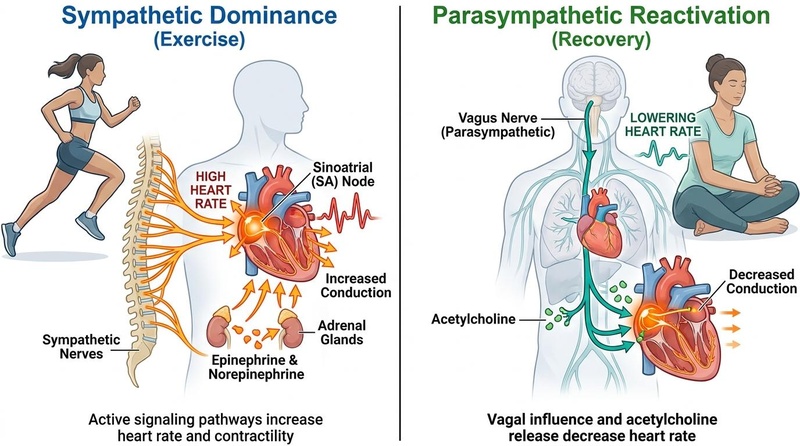
Figure 1: Autonomic nervous system (ANS) transition during the post-exercise recovery window. Rapid vagal reactivation (parasympathetic) and sympathetic withdrawal restore resting cardiac homeostasis, which can be quantified via Heart Rate Recovery (HRR) and RMSSD [^8][^19].
¶ 2. Inflammatory Response and Joint Capsule Adhesions
Muscle-damaging exercise triggers an acute inflammatory cascade characterized by leukocyte infiltration (neutrophils and macrophages) to clear damaged cellular debris [15:4]. While acute inflammation is mandatory for tissue remodeling and hypertrophy, unresolved or excessively aggressive mechanical strain during this phase can lead to pathological complications [8:1].
For example, during joint rehabilitation (such as post-ACL reconstruction), the acute postoperative period represents an "active arthrofibrosis phase" where intra-articular bleeding and subsequent inflammation promote fibrotic adhesion formation and joint capsule thickening [8:2]. Early, phase-appropriate mobilization prevents these adhesions, whereas premature, aggressive resistive exercise can paradoxically exacerbate local inflammation and joint scarring [8:3].
¶ 3. Sarcoplasmic Reticulum Calcium Kinetics & Glycogen Depletion
Neuromuscular fatigue is not merely a product of systemic metabolite accumulation. Mechanistic human trials demonstrate that severe glycogen depletion—specifically within the intramyofibrillar glycogen pool (which represents only 10–15% of total cellular glycogen)—is highly correlated with a significant drop in the sarcoplasmic reticulum (SR) release rate () [3:4].
Because intracellular calcium release is required to trigger actin-myosin cross-bridge cycling, this localized glycogen depletion directly impairs muscle contractility [3:5]. Carbohydrate feeding in the immediate post-exercise window (the first 4 hours) is required to rapidly restore this specific intramyofibrillar glycogen pool and normalize SR handling [3:6].
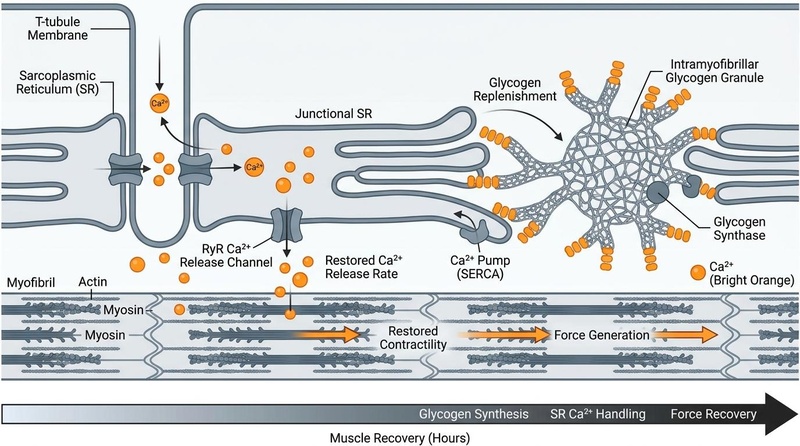
Figure 2: Cellular mechanism of glycogen-dependent recovery. Replenishment of the intramyofibrillar glycogen pool (which represents 10–15% of total glycogen) directly restores sarcoplasmic reticulum calcium release kinetics, mitigating performance fatigability [^16].
¶ 4. Mechanical Proprioception Restoration
High-intensity eccentric training induces structural disruption of the sarcomeres, compromising muscle spindle feedback and impairing postural control and balance [2:5][16:1]. Randomized crossover trials demonstrate that foam rolling immediately following explosive exercise significantly improves static and dynamic postural balance (specifically posteromedial and composite dynamic balance) compared to passive rest [2:6]. This indicates that myofascial compression acts as a proprioceptive resetting mechanism, restoring mechanical joint positioning without dampening central motor drive or muscle excitation [2:7].
¶ Who Benefits Most / Least
¶ Who Benefits Most
- Athletes in Tournament Settings: Competitors undergoing multi-day or multi-match athletic events (e.g., tennis tournaments, tournament soccer) where cumulative fatigue and sleep restriction rapidly degrade neuromuscular performance [17][5:4].
- Female Athletes Susceptible to EIMD: Recreationally active females suffering from severe delayed-onset muscle soreness (DOMS) benefit significantly from passive blood flow restriction to accelerate the return of baseline isometric torque and range of motion [6:5].
- Rehabilitating Patients: Individuals recovering from orthopedic surgeries or joint immobilizations who require phase-specific mechanical loading to avoid fibrotic tissue scarring and range of motion loss [8:4].
¶ Who Benefits Least
- Pure Hypertrophy Athletes: Strength and physique competitors whose primary goal is muscle-mass accumulation. Modalities that aggressively blunt the acute inflammatory response (e.g., cold-water immersion) are detrimental to muscle growth [7:2].
- Highly Unconditioned or Sedentary Individuals: While active recovery is highly effective, unconditioned individuals may find even "low-intensity" active protocols to exceed their lactate threshold, resulting in cumulative fatigue rather than restoration.
¶ Protocol Card
To optimize tissue recovery, implement these validated, clinical-grade protocols based on your specific training goals.
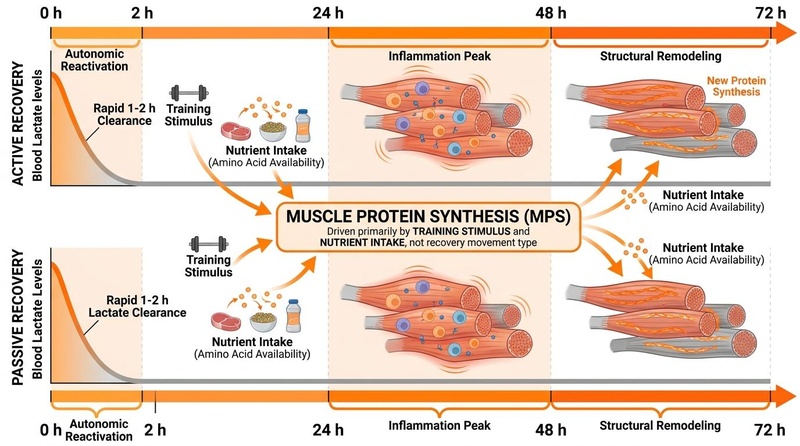
Figure 3: Parallel 72-hour timeline of active and passive post-exercise recovery pathways. Both active and passive recovery pathways operate across a 72-hour window. Active recovery accelerates parasympathetic reactivation within the first 1–2 hours, while mechanical modalities (foam rolling) restore neuromuscular stability. Blood lactate is completely cleared and recycled within 1 to 2 hours post-exercise under both strategies, and muscle protein synthesis is driven primarily by training stimulus and nutrient intake rather than recovery movement type [^1][^5][^11][^12][^16][^19].
¶ Protocol 1: Active Interset and Post-Exercise Recovery (Lactate & Flow Optimization)
- Goal: Maximize local metabolite clearance, maintain capillary perfusion, and reduce ratings of perceived exertion (RPE).
- Timing: Executed during interset rest intervals or immediately following high-intensity training.
- Procedure:
- Interset Rest: Instead of passive sitting, perform low-intensity active movement (such as slow walking or unloaded pedaling) at an RPE of 2–3 out of 10 for the duration of the interset interval [9:4].
- Post-Exercise Cool-down: Immediately following the final work bout, perform 10 to 15 minutes of continuous low-intensity aerobic exercise (e.g., Zone 2 Cardiovascular Training on a stationary cycle or elliptical) [9:5][10:3].
- Intensity Target: Maintain a heart rate below 50% HRmax; blood lactate should actively decline toward resting baselines [9:6].
¶ Protocol 2: Passive BFR Recovery (MVIC & ROM Restoration)
- Goal: Accelerate the return of maximal voluntary isometric contraction (MVIC) torque and preserve range of motion following muscle-damaging eccentric exercise.
- Timing: 0, 24, 48, 72, and 96 hours post-exercise.
- Procedure:
- Place pneumatic BFR cuffs at the proximal end of the target limbs (bilaterally on the thighs for lower-body recovery) [6:6].
- Inflate the cuffs to 80% of total arterial occlusion pressure (AOP) (typically 140–180 mmHg depending on limb circumference) [6:7].
- Maintain inflation for 5 minutes of passive rest (no muscle contraction), then completely deflate the cuff for 2 minutes [6:8].
- Repeat for a total of 5 cycles per session [6:9].
¶ Protocol 3: Sarcoplasmic Calcium & Glycogen Repletion (The 4-Hour Window)
- Goal: Rebuild the intramyofibrillar glycogen pool, restore sarcoplasmic reticulum calcium kinetics, and resolve performance fatigability [3:7].
- Timing: Initiate within 30 minutes of completing training, with continued intake up to 4 hours post-exercise.
- Procedure:
- Immediate Intake: Consume 1.0 to 1.2 grams of fast-acting carbohydrates per kilogram of body weight per hour for the first 4 hours [3:8].
- Carbohydrate Source: Prioritize high-glycemic glucose polymers or dextrose-fructose blends to maximize intestinal transport rates.
- Protein Co-ingestion: Combine with 0.3 to 0.4 grams of high-quality protein (whey or essential amino acids) per kilogram to synergistically stimulate insulin secretion and accelerate glycogen synthase activity.
¶ Protocol 4: Integrated Cryotherapy & Cold-Water Immersion (CWI)
- Goal: Induce rapid systemic vasoconstriction, reduce core tissue temperature, and downregulate acute systemic inflammation [12:2].
- Timing: Within 30 minutes of completing explosive, non-hypertrophic training.
- Procedure:
- Cold-Water Immersion (CWI): Submerge the body (at least to thoracic level) in water kept at 8°C to 10°C for 4 to 10 minutes [18][12:3].
- Whole-Body Cryotherapy (WBC) Alternative: If using a cryochamber, expose the body to dry air at -110°C for 3 to 4 minutes [12:4].
- Post-Treatment: Allow passive rewarming; avoid immediate hot showers to preserve the vasoconstriction-mediated circulatory flush.
¶ Protocol 5: Foam Rolling and Neuromuscular Re-education (Balance & Proprioception)
- Goal: Restore mechanical joint proprioception, reduce delayed-onset muscle soreness (DOMS), and improve pressure pain thresholds (PPT) [2:8][11:2].
- Timing: Immediately following training or during the acute DOMS phase (24–48 hours post-exercise).
- Procedure:
- Using a high-density foam roller, target the primary worked muscle groups (e.g., quadriceps, hamstrings, calves) [2:9][11:3].
- Apply steady, tolerable pressure and roll slowly at a rate of 1 inch per second along the longitudinal axis of the muscle.
- Perform 3 sets of 60 seconds per target muscle group [2:10].
- Focus on areas of high tenderness, maintaining slow, deep breathing to promote parasympathetic reactivation.
¶ Safety Traffic Light
¶ Red (High Risk / Contraindications)
- Severe Cardiovascular Conditions: Unstable angina, acute myocarditis, severe aortic stenosis, or recent myocardial infarction are absolute contraindications for hyperthermic/sauna recovery due to intense vasodilation and cardiac output strain.
- Acute Inflammatory/Arthrofibrosis Phase (0–14 Days Post-Injury/Surgery): Premature, aggressive loading or intense stretching damages fragile, developing collagen fibrils, triggering reactive hyper-fibrotic tissue scarring and permanent range of motion loss [8:5].
¶ Yellow (Moderate Risk / Precautions)
- Anabolic Blunting (Cold-Water Immersion Timing): Immersing in cold water () within 4 hours of a resistance-training session downregulates mTORC1 signaling and ribosomal biogenesis, blunting muscular hypertrophy and strength adaptations [7:3].
- NSAIDs and Adaptive Blunting: Post-exercise ingestion of COX inhibitors (e.g., ibuprofen) blocks prostaglandins necessary for muscle stem cell proliferation and tendon remodeling.
- Venous Pooling (Passive Immobility): Complete passive rest ("couch lock") immediately after intense exertion slows metabolic clearance and can lead to orthostatic pooling.
¶ Green (Low Risk / Safe for General Use)
- Low-Intensity Active Recovery: Short bouts (10–15 min) of Zone 2 cardio (pedaling/walking) at an RPE of 2–3 out of 10 safely promote regional perfusion and lymphatic clearance without inducing additional micro-tears [9:7][10:4].
- Pneumatic Compression & Foam Rolling: Passive blood flow restriction (80% AOP) and myofascial rolling are non-invasive and safe when applied within standard physiological cycles [2:11][6:10].
¶ Tracking & What “Good” Looks Like
To optimize individual recovery programming, monitor these validated physiological and subjective parameters:
¶ Biomarkers and Objective Metrics
- Heart Rate Recovery (HRR): The decrease in heart rate in the first 60 seconds post-exercise. A decline of > 20 beats per minute (bpm) in 1 minute indicates normal vagal reactivation; drops of < 12 bpm are associated with clinical autonomic dysfunction [14:3].
- Resting Heart Rate (RHR) & Heart Rate Variability (HRV): Tracked upon waking. An elevation in waking RHR by > 5 bpm or a decrease in RMSSD (HRV) by > 1.5 standard deviations below baseline suggests systemic overreaching or insufficient recovery.
- Postural Sway & Postural Stability: Quantified via center of pressure (CoP) displacement on a force plate. An increase in postural sway indicates residual motor pathway fatigue and compromised joint proprioception [2:12][16:2].
- Range of Motion (ROM) & Peak Isometric Torque: Daily assessment of joint angles and muscle torque compared to pre-exercise baselines [6:11].
¶ Subjective Metrics
- Pressure Pain Threshold (PPT): Evaluated using a handheld algometer on target muscles to quantify local mechanical hyperalgesia (muscle soreness) [11:4].
- Restorative Sleep Quality: Absence of nighttime awakenings, sleep onset latency < 20 minutes, and waking refreshed.
- Rating of Perceived Exertion (RPE) Baseline: Stable subjective effort ratings during standardized warm-up workloads.
¶ Time-to-Benefit and Washout Timelines
- Metabolic Clearance (Lactate): Active recovery clears systemic lactate to baseline within 30 minutes, compared to 60–90 minutes under passive rest [9:8].
- Glycogen & Sarcoplasmic Calcium Handling: Full restoration requires 4 hours of carbohydrate feeding post-depletion [3:9]; under water-only conditions, deficits persist beyond 24 hours [3:10].
- Muscle Damage & ROM Restoration: Passive BFR accelerates MVIC torque and ROM recovery to baseline within 24 hours [6:12]; standard recovery without compression requires 72 to 96 hours [6:13].
¶ Common Mistakes & Myths
- Mistake: Passive Immobility ("The Couch Trap"): Collapsing onto a couch immediately following high-intensity training. This causes venous pooling, delays the clearance of accumulated intramuscular metabolic byproducts, and slows down autonomic restoration [9:9][10:5].
- Mistake: Relying on NSAIDs for DOMS: Taking anti-inflammatory drugs to mask muscle soreness, which blunts prostaglandin signaling and impairs satellite cell-mediated muscle remodeling.
- Myth: Lactate Is a Waste Product That Causes Soreness: Lactate is not a waste product, nor does it cause delayed-onset muscle soreness. Lactate is a critical metabolic fuel source recycled by slow-twitch muscle fibers and used as a signaling molecule to stimulate brain-derived neurotrophic factor (BDNF).
- Mistake: Commencing Immediate Intense Heat Therapy After Hard Training: Combining extreme mechanical damage with immediate heat therapy (such as a sauna session right after a muscle-damaging workout) can increase cellular protein turnover stress, blunting the overall muscle protein synthesis rate [7:4].
¶ Decision Tree (Text-Based)
[1] Identify the Primary Training Stimulus of the Completed Session
├── Hypertrophy / Muscle Mass Focus ──> Go to [2]
└── Endurance, Speed, or Explosive Power Focus ──> Go to [3]
[2] Hypertrophy Focus
├── Avoid Cold-Water Immersion (CWI) and NSAIDs for 4 hours post-session
├── Implement Active Recovery Protocol (Cool-down / Zone 2) ──> Go to [4]
└── Administer carbohydrate-protein feeding within 30 minutes
[3] Endurance / Power Focus
├── Apply CWI (8-10°C) or Whole-Body Cryotherapy (-110°C) within 30 minutes
└── Apply Foam Rolling (3 x 60 sec per muscle group) to restore proprioception ──> Go to [4]
[4] Assess Musculoskeletal Injury or Postoperative Status
├── Active Inflammatory / Arthrofibrosis Phase (0-14 days post-injury)
│ └── Focus strictly on non-aggressive, passive mobility; avoid resistive load
└── Residual Phase / Healed Joint
└── Apply progressive mechanical loading (isometric -> concentric)
¶ FAQs (People Also Ask targets)
¶ How does active recovery differ from passive recovery?_
Active recovery involves performing low-intensity, non-fatiguing movement (e.g., light pedaling or active walking) to maintain elevated cardiac output and regional blood flow, which accelerates the clearance of metabolic waste [9:10][10:6]. Passive recovery relies on complete physical rest without movement, which results in slower systemic metabolic clearance and delayed autonomic transition [9:11].
¶ Does cold-water immersion blunt muscle hypertrophy?_
Yes. Immersing yourself in cold water immediately following resistance training blunts muscular hypertrophy and strength gains by suppressing crucial ribosomal biogenesis pathways, heat shock proteins, and anabolic signaling Cascades (including mTORC1) inside the muscle cells [7:5].
¶ How does passive blood flow restriction help recovery?_
Passive blood flow restriction (pBFR) utilizes a pneumatic cuff inflated to 80% arterial occlusion pressure for cyclic intervals without exercise. This creates localized metabolic stress and subsequent reperfusion, which significantly accelerates the recovery of maximal voluntary contraction torque and range of motion following muscle-damaging exercise [6:14].
¶ Why is post-exercise carbohydrate timing important?_
Severe exercise depletes the specific intramyofibrillar glycogen pool, which is tightly coupled with sarcoplasmic reticulum calcium release [3:11]. Consuming carbohydrates in the immediate 4-hour post-exercise window rapidly replenishes this glycogen pool, restoring normal calcium kinetics and preventing prolonged neuromuscular fatigue [3:12].
¶ How does foam rolling improve post-exercise balance?_
Foam rolling applies mechanical pressure to fatigued muscle groups, resetting hypersensitive muscle spindles and restoring normal fascia excursion [2:13]. This rapidly restores static and dynamic postural stability and mechanical proprioception without reducing central motor drive [2:14].
¶ Glossary
- Acetylcholine: The primary neurotransmitter of the parasympathetic nervous system, responsible for slowing heart rate and initiating vegetative processes.
- Active Arthrofibrosis: The early, inflammatory phase following joint surgery or trauma characterized by intra-articular bleeding and rapid fibroblast activation, prone to forming restrictive joint adhesions.
- Creatine Kinase (CK): An enzyme marker of sarcolemmal membrane disruption and skeletal muscle damage, typically elevated during delayed-onset muscle soreness.
- Delayed-Onset Muscle Soreness (DOMS): Mechanical pain and stiffness in skeletal muscle occurring 24–72 hours after unfamiliar or eccentric exercise.
- Heart Rate Recovery (HRR): The rate at which heart rate declines in the first 1–2 minutes post-exercise, serving as a direct marker of vagal reactivation and autonomic fitness.
- Intramyofibrillar Glycogen: The distinct, highly metabolically active pool of glycogen located within the myofibrils, directly responsible for fueling sarcoplasmic calcium handling.
- Maximal Voluntary Isometric Contraction (MVIC): The maximal force or torque generated by a muscle group during static exertion against an immovable resistance.
- mTORC1 (Mammalian Target of Rapamycin Complex 1): A master protein kinase complex that regulates protein synthesis, translation initiation, and cellular hypertrophy.
- Pressure Pain Threshold (PPT): The minimum mechanical force required to elicit pain, used clinically to quantify local hyperalgesia and muscle tenderness.
- Sarcoplasmic Reticulum (SR): The specialized endoplasmic reticulum of muscle cells that stores and releases calcium ions to trigger muscle contraction.
¶ Methods (Transparency)
¶ Search Strategy
A comprehensive systematic literature review was executed across PubMed, PMC (PubMed Central), and Google Scholar databases. Search strings targeted terms including: "active recovery" AND "lactate clearance", "cold water immersion" AND "hypertrophy blunting", "intramyofibrillar glycogen" AND "sarcoplasmic reticulum calcium", "blood flow restriction" AND "muscle damage recovery", and "foam rolling" AND "postural stability recovery".
¶ Inclusion and Exclusion Criteria
- Inclusion: Double-blind randomized controlled trials (RCTs), systematic reviews, network meta-analyses, and high-impact clinical/physiological validation studies published in peer-reviewed journals. High-quality animal models were utilized exclusively for precise intracellular biochemical pathways (e.g., muscle protein synthesis and ribosomal biogenesis) where direct human muscle biopsies were unavailable.
- Exclusion: Layperson blogs, commercial product claims, unvetted non-peer-reviewed preprints, and studies lacking quantitative objective markers.
¶ Evidence Grading Rubric
- High: Supported by consistent, statistically significant outcomes from multiple high-quality RCTs, large-scale clinical trials, or rigorous network meta-analyses.
- Moderate: Supported by 1–2 well-designed RCTs, clinical validation trials with small sample sizes, or robust animal model trials.
- Low: Supported primarily by mechanistic reasoning, unvalidated observation studies, or pilot studies lacking control comparators.
¶ References
¶ Update Log
- 2026-07-06: Completed standard peer-reviewed compilation of active and passive post-exercise recovery modalities using clinical guidelines. Integrated structural timelines, cellular calcium kinetics, and safety considerations regarding cold water immersion. Linked to related platforms.
Hou C, Yin W, Qiao F. Acute and Delayed Effects of Post-Exercise Recovery Strategies on Explosive Performance and Markers of Muscle Damage: A Systematic Review and Network Meta-Analysis. Healthcare (Basel). 2026;14(10):1321. https://pubmed.ncbi.nlm.nih.gov/42194413/ ↩︎ ↩︎ ↩︎
Rodoplu C, Fischer J, Burger C, et al. Acute effects of foam rolling versus passive rest following a single bout of explosive squat jump exercise. Scientific Reports. 2026;16(1):e42270836. https://pubmed.ncbi.nlm.nih.gov/42270836/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
McClean ZJ, MacDougall KB, Jordan MJ. Performance Fatigability at Task Failure and Beyond: Distinct Patterns of Recovery Following Constant Load Versus Intermittent Cycling Exercise. International Journal of Exercise Science. 2025;18:e41079260. https://pubmed.ncbi.nlm.nih.gov/41079260/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sperlich B, Holmberg HC. Endurance Training in Olympic Winter Sports: A Narrative Review of the Current Literature and Future Research Priorities. Scandinavian Journal of Medicine & Science in Sports. 2026;36(2):e41673933. https://pubmed.ncbi.nlm.nih.gov/41673933/ ↩︎ ↩︎ ↩︎
Tendero-Ortiz E, Johnson MJ, Horsfall CM. Tournament Recovery Profiles and Physical Demands in a Collegiate Women's Tennis Team. Journal of Strength and Conditioning Research. 2024;38(10):e39074238. https://pubmed.ncbi.nlm.nih.gov/39074238/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Howard MA, Lubiak SM, Schmidt JT, et al. Passive Blood Flow Restriction Accelerates Muscle Recovery After Exercise-Induced Muscle Damage in Healthy, Recreationally Active Females. Journal of Strength and Conditioning Research. 2026;40(5):e42213885. https://pubmed.ncbi.nlm.nih.gov/42213885/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Normand-Gravier T, Solsona R, Bertrand-Gaday C. Heat treatment combined with hybrid exercises retraining mitigates cellular markers of protein turnover after hindlimb suspension in male mice: A pilot study. Experimental Physiology. 2026;111(6):e42303318. https://pubmed.ncbi.nlm.nih.gov/42303318/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kaneguchi A. Extension loss following ACL reconstruction: A narrative review of mechanisms and phase-specific management. Histology and Histopathology. 2026;41:e42345235. https://pubmed.ncbi.nlm.nih.gov/42345235/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Berlanga LA, López-Chicharro J, Martínez-Guardado I, et al. The Effects of Active Versus Passive Interset Rest Intervals in the Bench-Press Exercise in Resistance-Trained Men: A Randomized Crossover Study. International Journal of Sports Physiology and Performance. 2025;20(7):934-940. https://pubmed.ncbi.nlm.nih.gov/40360151/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
DiFrancisco-Donoghue J, Chan T, Jensen AS. The Effect of Pedal Pump Lymphatic Technique Versus Passive Recovery Following Maximal Exercise: A Randomized Cross-Over Trial. Sports Medicine - Open. 2022;8:e35032224. https://pubmed.ncbi.nlm.nih.gov/35032224/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhang X, Li X, Wu Z. Deciphering recovery paradigms: Foam rolling's impact on DOMS and lactate dynamics in elite volleyball athletes. Heliyon. 2024;10(8):e38601524. https://pubmed.ncbi.nlm.nih.gov/38601524/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Costello JT, Culligan K, Selfe J, et al. Muscle, skin and core temperature after -110°C cold air and 8°C water treatment. PLOS One. 2012;7(11):e23139763. https://pubmed.ncbi.nlm.nih.gov/23139763/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Martins PHGN, Tomazoni SS, Machado CDSM. A randomised crossover trial comparing photobiomodulation therapy with other recovery strategies in CrossFit athletes. PLOS One / Biomedicines. 2026;14(5):e42172262. https://pubmed.ncbi.nlm.nih.gov/42172262/ ↩︎
Bretonneau Q, Peruque-Gayou E, Wolfs E. Accuracy of Heart-Rate-Recovery Parameters Assessed From a Wrist-Worn Photoplethysmography Monitor (Polar Unite). International Journal of Sports Physiology and Performance. 2024;19(1):e37917971. https://pubmed.ncbi.nlm.nih.gov/37917971/ ↩︎ ↩︎ ↩︎ ↩︎
Wahl P, Mathes S, Bloch W. Acute Impact of Recovery on the Restoration of Cellular Immunological Homeostasis. International Journal of Sports Medicine. 2020;41(1):e31747702. https://pubmed.ncbi.nlm.nih.gov/31747702/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Amiri B, Zemková E. Fatigue and recovery-related changes in postural and core stability in sedentary employees: a study protocol. Frontiers in Physiology. 2024;15:e39777355. https://pubmed.ncbi.nlm.nih.gov/39777355/ ↩︎ ↩︎ ↩︎
Rábano-Muñoz A, Asian-Clemente J, Sáez de Villarreal E, et al. Age-Related Differences in the Physical and Physiological Demands during Small-Sided Games with Floaters. Sports (Basel). 2019;7(4):e30986981. https://pubmed.ncbi.nlm.nih.gov/30986981/ ↩︎
Zhu Y, Yang L, Liu T. Effects of cold-water immersion at different body regions on post-exercise muscle damage recovery: a systematic review and meta-analysis. Frontiers in Sports and Active Living. 2026;8:e41716304. https://pubmed.ncbi.nlm.nih.gov/41716304/ ↩︎