¶ Stem Cell Therapy
| Indication | Established Medical Use (Orthopedics, Hematology) vs Investigational (Longevity, Frailty) |
| Access | Rx / Clinical Trials / Off-label Medical Tourism |
| Dosing Sched | Variable (Single or repeated cycles, typically 1–2 sessions annually) |
| Safety Profile | Moderate (Well-tolerated if high-purity MSCs; risks of ectopic growth if poorly characterized) |
| Key Marker | Inflammatory cytokines (TNF-α, IL-6), physical performance (6MWD), tissue-specific imaging |
| Est. Cost | High ($5,000 – $25,000+ per treatment cycle) |
Stem cell therapy is an advanced regenerative medicine intervention involving the clinical administration of self-renewing, multipotent, or pluripotent cellular populations to promote tissue repair, modulate systemic inflammation, and target the physiological hallmarks of aging [1]. While hematologic stem cell transplantations have been standard of care for leukemia and bone marrow disorders for decades, the modern frontier of stem cell therapy focuses on multipotent mesenchymal stem/stromal cells (MSCs) [2]. These cells are being actively evaluated in clinical trials for age-related conditions, skeletal disorders, heart failure, neurodegenerative diseases, and systemic frailty, although their application as an elective longevity therapy remains investigational and subject to rigorous ongoing clinical validation [3][4][5].
¶ At a glance
¶ Quick Overview
Stem cell therapy is an advanced clinical intervention involving the administration of self-renewing cellular populations to promote tissue repair, downregulate chronic systemic inflammation ("inflammaging"), and treat age-related degenerative conditions [1:1].
¶ Safety "Traffic Light"
CRITICAL CONTRAINDICATIONS & SAFETY LIMITS
- RED (STOP): Do NOT undergo stem cell therapy if you have any active malignancy, as MSCs can secrete potent angiogenic factors (such as VEGF) and suppress local immune cells, theoretically promoting tumor vascularization and allowing tumor cells to evade immune surveillance [1:2]. Do NOT undergo during pregnancy due to absent safety data.
- YELLOW (CAUTION): Avoid unapproved, direct-to-consumer "stem cell clinics" operating outside of regulated clinical trials. Ensure any allogeneic cell products are rigorously characterized, viability-tested, and manufactured under strict cGMP guidelines to prevent biological contamination or severe immune reactions [5:1][6].
- GREEN (GO): Intravenous infusion of characterized, young allogeneic MSCs (e.g., Wharton's Jelly or Lomecel-B) for aging frailty and intra-articular injection for knee osteoarthritis are highly tolerated and clinically validated in randomized controlled trials [3:1][7].
¶ Protocol Card
| Parameter | Clinical Protocol Summary | Key Details & Monitoring |
|---|---|---|
| Cell Dosage | 50M to 100M viable MSCs per treatment cycle [3:2][8] | Dosages above 100M do not show additional therapeutic benefit in frailty trials [3:3]. |
| Administration | Intravenous (IV) for systemic; Intra-articular (IA) for joints [3:4][8:1] | IV delivery undergoes "pulmonary trapping," acting via paracrine secretome release [5:2][1:3]. |
| Frequency | Single cycle, repeatable every 6 to 12 months if indicated [3:5][9] | Standard protocols rely on single sessions with long-term follow-up monitoring. |
| Monitoring | Systemic inflammation and physical functional markers [3:6][10] | Track CRP, circulating TNF-α/IL-6, and physical performance (6-Minute Walk Distance) [3:7][10:1]. |
¶ Bottom Line
Stem cell therapy, specifically utilizing characterized mesenchymal stem cells (MSCs), has demonstrated moderate-to-high human efficacy in mitigating age-related physical decline (frailty) and localized joint degradation, operating primarily through systemic immunomodulatory and paracrine signaling pathways rather than direct physical cell replacement [3:8][1:4][8:2].
¶ What is Stem Cell Therapy?
Stem cell therapy refers to the therapeutic delivery of viable stem cells to repair, replace, or regenerate damaged tissues and organs. Stem cells are distinguished by two fundamental properties: self-renewal (the capacity to undergo numerous cycles of cell division while maintaining their undifferentiated state) and potency (the capacity to differentiate into specialized cell types) [1:5].
Historically, stem cell therapy was synonymous with hematopoietic stem cell transplantation (HSCT) for bone marrow reconstitution [2:1]. However, the modern longevity and clinical landscape is dominated by the following cell populations:
¶ Mesenchymal Stem/Stromal Cells (MSCs)
MSCs are multipotent adult stem cells that can differentiate into lineages of the mesoderm, including osteoblasts (bone), chondrocytes (cartilage), and adipocytes (fat) [1:6]. They can be harvested from various tissues, most commonly bone marrow (BM-MSCs), adipose tissue (ADSCs), and umbilical cord tissue/Wharton's Jelly (UC-MSCs) [2:2]. Due to their low expression of Major Histocompatibility Complex (MHC) Class II molecules, MSCs are largely immunoprivileged, allowing for the widespread use of allogeneic (donor-derived) cells without human leukocyte antigen (HLA) matching or systemic immunosuppression [11].
¶ Induced Pluripotent Stem Cells (iPSCs)
iPSCs are somatic cells (such as skin or blood cells) that have been genetically reprogrammed back into an embryonic-like state by the forced expression of specific transcription factors (the Yamanaka factors: Oct3/4, Sox2, Klf4, and c-Myc) [12]. Unlike MSCs, iPSCs are truly pluripotent, meaning they can differentiate into any cell type of the three germ layers (ectoderm, mesoderm, and endoderm). While they hold extraordinary potential for personalized disease modeling and autologous cell-replacement therapies, they are not currently approved for clinical longevity use due to high genomic instability and the risk of teratoma formation [12:1].
¶ Multilineage-Differentiating Stress-Enduring (Muse) Cells
Muse cells are a subpopulation of endogenous, non-tumorigenic pluripotent stem cells found in connective tissues, bone marrow, and peripheral blood [13]. They are characterized by their ability to endure severe cellular stress and selectively home to damaged tissues, where they differentiate into tissue-appropriate cells to achieve functional regeneration without forming teratomas, representing a key alternative to traditional MSCs and iPSCs [13:1].
¶ Autologous vs. Allogeneic Therapies
| Characteristic | Autologous (Patient's Own Cells) | Allogeneic (Donor-Derived / Gestational) |
|---|---|---|
| Source Tissue | Patient's bone marrow, adipose tissue, or peripheral blood [2:3]. | Healthy young donors, umbilical cord, placenta, amnion [5:3][2:4][14]. |
| Cellular Vitality | Dependent on patient age and health; often characterized by cell senescence, somatic mutations, and reduced proliferation [12:2]. | Highly proliferative, pristine epigenetic state, high secretome potency, and zero donor age-related decay [5:4][1:7]. |
| Immunogenicity | Zero risk of immune rejection or host-versus-graft reaction [11:1]. | Minimal risk; cells are immunoprivileged but can occasionally induce HLA sensitization over repeated doses [15][11:2]. |
| Manufacturing | Custom, single-batch isolation; high cost and delay due to harvesting and expansion times [6:1]. | Off-the-shelf, mass-manufactured, highly standardized, and immediately available for clinical use [6:2]. |
| Harvest Procedure | Invasive surgical harvesting (liposuction or bone marrow aspiration) [2:5]. | Non-invasive collection of postpartum donor gestational tissues [5:5]. |
¶ Mechanisms of Action
The clinical efficacy of stem cells, particularly MSCs, is governed by four primary, overlapping biological mechanisms:
¶ 1. Paracrine Signaling and the Secretome
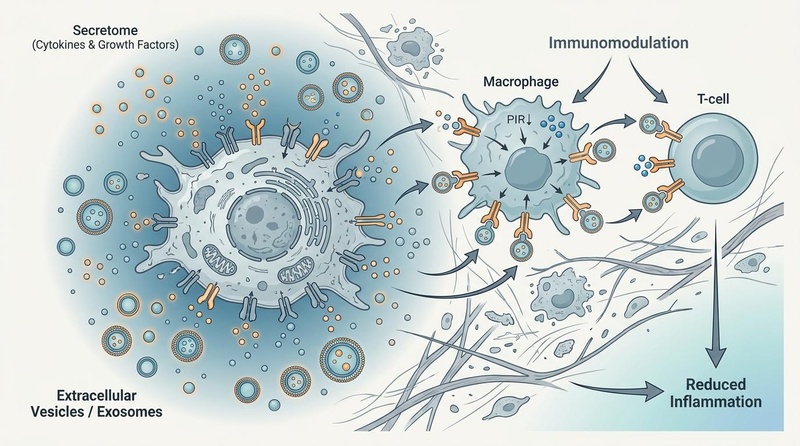
Rather than physically integrating and differentiating to replace host tissues, MSCs act primarily as "cellular orchestrators" [1:8]. Upon homing to sites of injury or systemic inflammation, MSCs secrete a dense cocktail of bioactive molecules known collectively as the secretome [12:3]. This includes growth factors (such as VEGF, FGF, and IGF-1) and extracellular vesicles (EVs / exosomes) containing regulatory microRNAs and proteins [12:4]. These paracrine signals act directly on host tissue-resident cells to inhibit apoptosis, stimulate endogenous stem cell niches, promote angiogenesis, and initiate tissue repair [1:9][12:5].
Schematic representation of Mesenchymal Stem Cell (MSC) mechanisms of action. Under the influence of an aged or injured microenvironment, MSCs release paracrine factors and secretome components (such as extracellular vesicles and cytokines) to modulate macrophages and T-cells, promoting M2 macrophage polarization and downregulating systemic inflammatory cascades.
¶ 2. Immunomodulation
MSCs possess profound immunomodulatory capabilities [1:10]. They interact dynamically with both the innate and adaptive immune systems:
- Macrophage Polarization: MSCs actively drive the polarization of macrophages from the pro-inflammatory M1 phenotype to the anti-inflammatory, tissue-rejuvenating M2 phenotype [1:11][12:6].
- T-Cell Suppression: By secreting indoleamine 2,3-dioxygenase (IDO), prostaglandin E2 (PGE2), and transforming growth factor-beta (TGF-β), MSCs suppress the proliferation and activation of cytotoxic T-cells and natural killer (NK) cells, while promoting the generation of regulatory T-cells (Tregs) [1:12].
¶ 3. Mitochondrial Transfer
MSCs can physically rescue energetically compromised, senescent, or damaged host cells by transferring healthy mitochondria [1:13][12:7]. This occurs via the formation of intercellular tunneling nanotubes (TNTs) or through the release of microvesicles containing functional mitochondria. The recipient cells internalize these mitochondria, leading to a restoration of oxidative phosphorylation, increased ATP production, and a reversal of cellular distress [12:8].
¶ 4. Homing and Chemotaxis
MSCs express specific chemokine receptors (such as CXCR4) that allow them to detect gradients of inflammatory signals (such as stromal cell-derived factor-1, or SDF-1) released by damaged or aging tissues [13:2]. This chemotactic homing mechanism directs intravenously or systemically administered cells to preferentially migrate to tissues experiencing acute or chronic biological stress [13:3].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Aging Frailty Reduction (Physical Function) | High | Moderate | 2 RCTs | Significant increase in 6-minute walk distance (6MWD) and physical performance at 6–12 months post-IV infusion of laromestrocel (Lomecel-B) [3:9][10:2]. | |
| Systemic Anti-Inflammation (TNF-α reduction) | Moderate | Moderate | 2 RCTs | Marked decrease in circulating TNF-α and other pro-inflammatory cytokines after IV MSC administration in elderly frail patients [3:10][10:3]. | |
| Knee Osteoarthritis (Pain and Joint Function) | High | High | Multiple RCTs | Intra-articular injection of ADMSCs or UC-MSCs (50–100M cells) significantly reduces pain and improves cartilage volume, sustained up to 60 months [7:1][8:3][16]. | |
| Ischemic Cardiomyopathy (LVEF Improvement) | Moderate | Moderate | Multiple RCTs | POSEIDON trials demonstrate improved left ventricular ejection fraction (LVEF), reduced scar size, and low major adverse cardiovascular events (MACE) [15:1][11:3][17]. | |
| Mild Alzheimer's Disease (Cognitive Stability) | Moderate | Moderate | 1 RCT | Phase 2a trial of laromestrocel demonstrated safety, neuroinflammatory biomarker stability, and slower brain volume loss compared to placebo [4:1]. | |
| Aging Kidney Function (eGFR Stability) | Moderate | Moderate | 1 RCT | Secondary analysis of a clinical trial showed that IV infusion of allogeneic bone marrow-derived MSCs preserved renal function (eGFR) and reduced markers of kidney aging over 12 months [18]. | |
| Aesthetic Rejuvenation (Wrinkles & Scarring) | High | Moderate | Systematic Review | Adipose-derived stem cell treatments improve facial volume, tissue elasticity, and significantly remodel hyperplastic dermal scars [19][14:1]. | |
| Biological/Epigenetic Age Reversal | Insufficient | Very Low | 0 RCTs | No high-quality randomized clinical trials have validated systemic epigenetic age reduction in humans [5:6][12:9]. |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- *Compact renderer encoding (preferred when using custom tags):
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ Dosage & Protocols
Stem cell protocols vary widely based on the delivery route, cell source, and target indication. Because MSCs are living biotherapeutics, standardized reporting is critical. The International Society for Cell & Gene Therapy (ISCT) has established strict reporting guidelines to monitor donor screening, viability, and population doubling levels [6:3].
¶ Routes of Administration
- Intravenous (IV) Infusion: The most common delivery route for systemic conditions, aging frailty, and autoimmune modulation [5:7]. Cells are suspended in saline-albumin and run over 30–60 minutes. Note that IV delivery results in the majority of cells being initially filtered and sequestered in the pulmonary capillary beds—a phenomenon known as pulmonary trapping—where they exert systemic effects primarily via paracrine signaling [5:8].
- Intra-articular (IA) Injection: Used exclusively for orthopedics and joint pathologies (e.g., knee osteoarthritis) [8:4]. Direct injection bypasses systemic circulation, retaining the MSCs within the synovial joint cavity to maximize local immunomodulation and interaction with host chondrocytes [7:2].
- Intranasal Delivery: An emerging, minimally invasive route evaluated in clinical trials for neurological and respiratory disorders [20]. Intranasally administered stem cells bypass the blood-brain barrier via olfactory and trigeminal nerve pathways to target cerebral neuroinflammation [20:1].
- Intrathecal (IT) Injection: Direct delivery into the cerebrospinal fluid (CSF) via lumbar puncture, utilized for advanced neurological diseases to bypass the blood-brain barrier [20:2].
¶ Typical Dosage Levels
| Indication | Cell Dosage Range | Delivery Route | Protocol details |
|---|---|---|---|
| Aging Frailty (Clinical trials) | 50M, 100M, or 200M cells [3:11] | Intravenous (IV) | Single IV infusion of allogeneic bone marrow-derived MSCs (laromestrocel); 100M dose identified as clinically optimal [3:12][10:4]. |
| Knee Osteoarthritis | 50M to 100M cells [8:5] | Intra-articular (IA) | Direct joint injection. Single dose or series of 3 injections spaced over several weeks [7:3][9:1]. |
| Ischemic Cardiomyopathy | 20M to 100M cells [11:4] | Transendocardial | Direct injection into viable myocardial tissue guided by electromechanical mapping during catheterization [15:2][11:5]. |
| Aesthetic Skin Rejuvenation | 10M to 50M cells [19:1] | Localized Intradermal | Micro-injections or combined with fat grafting (cell-assisted lipotransfer) [19:2]. |
¶ Safety and Contraindications
While stem cell therapy is characterized by a favorable safety profile when high-quality cellular products are used, it remains an invasive, biologically active treatment that carries distinct clinical risks.
¶ Adverse Events & Complications
| Adverse Event | Frequency / Clinical Context | Pathophysiological Mechanism | Evidence |
|---|---|---|---|
| Post-Infusion Fever | Common (up to 10–15% of IV cases); transient (resolves within 24–48 hours). | Acute immunological response to cellular debris or mild host response to allogeneic cell exposure [5:9]. | High [5:10] |
| Infusion Site Reactions | Occasional; mild local pain, swelling, or bruising. | Localized mechanical trauma from catheter insertion. | High [5:11][2:6] |
| Pulmonary Micro-embolism | Rare; associated with massive doses (>5-10M cells/kg) or poor cell suspension quality. | Mechanical lodging of clumped MSCs in the pulmonary capillaries due to their size (pulmonary trapping) [5:12]. | Moderate [5:13] |
| Tumorigenesis / Teratoma | Negligible for MSCs; High risk for pluripotent stem cells (iPSCs) if undifferentiated cells are present. | Pluripotent cells can proliferate indefinitely and form teratomas if not fully differentiated before implantation [12:10]. | High [12:11] |
| Ectopic Tissue Formation | Very rare; occurred historically with unvetted bone marrow aspirates injected into non-skeletal tissues. | Mal-differentiation of multipotent cells in response to local microenvironmental signaling cascades. | Low [2:7] |
¶ Regulatory Warnings
The clinical use of stem cells is heavily regulated. The U.S. Food and Drug Administration (FDA) and other major health authorities have repeatedly issued safety warnings against unapproved, unvetted stem cell clinics operating outside of clinical trials [5:14]. Many commercial "stem cell" treatments offered in medical tourism hubs utilize poorly characterized products with low cell viability, raising the risks of severe bacterial contamination, deep tissue infections, and severe inflammatory immune reactions.
¶ Contraindications
| Population / Condition | Clinical Precaution | Monitoring / Alternative Strategy |
|---|---|---|
| Active Malignancy | Absolute contraindication. MSCs secrete potent angiogenic factors (VEGF) and suppress local immune cells, which can theoretically promote tumor angiogenesis and allow tumor cells to evade immune surveillance [1:14]. | Mandatory pre-treatment oncological screening (e.g., PSA, mammography, colonoscopy). |
| Uncontrolled Systemic Infection | Relative contraindication. MSC-mediated immunosuppression may compromise the host's ability to clear bacterial or viral pathogens. | Full resolution of infection and normalization of C-reactive protein (CRP) and white blood cell (WBC) counts prior to therapy. |
| Hypercoagulable State | Precaution. Systemic IV administration of large cell volumes can transiently increase blood viscosity and activate coagulation cascades [5:15]. | Evaluation of D-dimer and coagulation panels; prophylactic administration of low-molecular-weight heparin (LMWH). |
| Pregnancy | Absolute contraindication. Lack of safety data regarding the impact of exogenous MSC administration on fetal development and maternal-fetal immunotolerance. | Negative pregnancy test required for females of childbearing potential before initiation. |
¶ FAQs
-
Is stem cell therapy FDA-approved?
- Stem cell therapy is only FDA-approved for specific hematologic and immunological indications, primarily hematopoietic stem cell transplants for blood-forming disorders and leukemia [2:8]. Other applications, such as IV MSC infusions for aging frailty, lung disease, or neurodegeneration, are not FDA-approved and are classified as investigational, currently restricted to regulated clinical trials [3:13][5:16].
-
What is the difference between autologous and allogeneic MSCs?
- Autologous stem cells are harvested from your own body, meaning there is zero risk of immune rejection, but the cells share your biological age, potential cellular senescence, and reduced regenerative capacity [11:6][12:12]. Allogeneic stem cells are harvested from healthy young donors or gestational tissues; they are younger, highly proliferative, and immunoprivileged, meaning they do not require tissue matching [15:3][11:7].
-
Can stem cells reverse systemic aging?
- There is currently no robust human clinical trial evidence proving that stem cell therapy can systematically reverse biological or epigenetic age [5:17][12:13]. Preclinical rodent models have shown tissue rejuvenation and lifespan extension, but human trials are restricted to targeted disease endpoints and physical frailty mitigation [3:14][4:2][12:14].
-
What is "pulmonary trapping" and is it dangerous?
- Pulmonary trapping refers to the phenomenon where the majority of intravenously administered stem cells lodge in the microvasculature of the lungs during their first circulatory pass, due to the cells' physical size [5:18]. While not typically dangerous in standardized clinical doses, it does drastically reduce the number of cells that directly reach peripheral tissues. As a result, IV stem cell therapies exert their effects primarily through systemic paracrine signaling rather than direct local tissue integration [5:19][1:15].
-
How do exosomes compare to live stem cell therapies?
- Exosomes (extracellular vesicles) are cell-free derivatives containing the active signaling components (microRNAs, proteins) of the stem cell secretome [12:15]. Because they are not living cells, they carry zero risk of tumorigenesis, do not trigger pulmonary trapping, can easily cross the blood-brain barrier, and are far easier to standardize and store. However, they lack the dynamic, feedback-controlled responsiveness of live stem cells, which can actively sense and respond to tissue-specific inflammatory environments [1:16][12:16].
¶ See also
- Cellular Reprogramming for Longevity
- Regenerative Medicine and Tissue Repair
- Exosomes and Extracellular Vesicles
- Therapeutic Plasma Exchange
¶ References
Pittenger MF, Discher DE, Péault BM, et al. Mesenchymal stem cell perspective: cell biology to clinical progress. NPJ Regen Med. 2019; PMID: 31815151. https://www.nature.com/articles/s41536-019-0083-6 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Squillaro T, Peluso G, Galderisi U. Clinical trials with mesenchymal stem cells: an update. Cell Transplant. 2016; PMID: 26214322. https://journals.sagepub.com/doi/10.3727/096368915X689622 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ruiz JG, Oliva AA Jr, Ramdas KN, et al. Randomized phase 2b dose-escalation trial of stem cell therapy with laromestrocel for aging frailty. Cell Stem Cell. 2026; PMID: 41747733. https://pubmed.ncbi.nlm.nih.gov/41747733/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Rash BG, Ramdas KN, Agafonova N, et al. Allogeneic mesenchymal stem cell therapy with laromestrocel in mild Alzheimer's disease: a randomized controlled phase 2a trial. Nature Medicine. 2025; PMID: 40065171. https://pubmed.ncbi.nlm.nih.gov/40065171/ ↩︎ ↩︎ ↩︎
Hum C, Poliwoda J, Lalu M, et al. Safety of intravascular administration of umbilical-cord-derived mesenchymal stromal cells: an updated systematic review and meta-analysis. Stem Cells Transl Med. 2026; PMID: 42246109. https://pubmed.ncbi.nlm.nih.gov/42246109/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Davies LC, Biard L, García-Olmo D, et al. Defining minimal criteria for peer-reviewed reporting of mesenchymal stromal cell clinical trials for autoimmune diseases. Cytotherapy. 2025; PMID: 40828119. https://pubmed.ncbi.nlm.nih.gov/40828119/ ↩︎ ↩︎ ↩︎ ↩︎
Jafar H, Samara O, Shahin D, et al. Intra-articular allogeneic adipose-derived mesenchymal stromal cell injections for stage III knee osteoarthritis: a double-blind placebo-controlled trial with 60-month follow-up. Stem Cells Transl Med. 2026; PMID: 42049633. https://pubmed.ncbi.nlm.nih.gov/42049633/ ↩︎ ↩︎ ↩︎ ↩︎
Awad G, Saad JP, Hamyeh A, et al. Efficacy and safety of intra-articular mesenchymal stem cell-based therapies in knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Clin Rheumatol. 2026; PMID: 41863718. https://pubmed.ncbi.nlm.nih.gov/41863718/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Khodadoust E, Zarrabi M, Afzal E, et al. Three intra-articular injections of allogeneic umbilical cord-derived mesenchymal stromal cells in knee osteoarthritis: a phase-I clinical trial. Regenerative Medicine. 2026; PMID: 41757831. https://pubmed.ncbi.nlm.nih.gov/41757831/ ↩︎ ↩︎
Yousefi K, Ramdas KN, Ruiz JG, et al. The Design and Rationale of a Phase 2b, Randomized, Double-Blinded, and Placebo-Controlled Trial to Evaluate the Safety and Efficacy of Lomecel-B in Older Adults with Frailty. J Frailty Aging. 2022; PMID: 35441200. https://pubmed.ncbi.nlm.nih.gov/35441200/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hare JM, Fishman JE, Gerstenblith G, et al. Comparison of allogeneic vs autologous bone marrow–derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: the POSEIDON randomized trial. JAMA. 2012; PMID: 23117550. https://pubmed.ncbi.nlm.nih.gov/23117550/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Rudnitsky E, Braiman A, Wolfson M. Mesenchymal stem cells and their derivatives as potential longevity-promoting tools. Biogerontology. 2025; PMID: 40259142. https://pubmed.ncbi.nlm.nih.gov/40259142/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dezawa M. Comparison of MSCs and Muse cells: the possible use for healthspan optimization. Biogerontology. 2025; PMID: 40601066. https://pubmed.ncbi.nlm.nih.gov/40601066/ ↩︎ ↩︎ ↩︎ ↩︎
Chernoff G. Human Placental Mesenchymal Stem Cell-Derived Exosomes in Wound Healing and Scar Therapy: A Systematic Review and Meta-analysis. Aesthetic Surg J. 2026; PMID: 41800724. https://pubmed.ncbi.nlm.nih.gov/41800724/ ↩︎ ↩︎
Hare JM, DiFede DL, Rieger AC, et al. Randomized Comparison of Allogeneic Versus Autologous Mesenchymal Stem Cells for Nonischemic Dilated Cardiomyopathy: POSEIDON-DCM Trial. J Am Coll Cardiol. 2017; PMID: 27856208. https://pubmed.ncbi.nlm.nih.gov/27856208/ ↩︎ ↩︎ ↩︎ ↩︎
Xie R, Yu J, Feng Y, et al. Comparative efficacy of different doses of mesenchymal stem cells derived from different tissue sources for knee osteoarthritis: a systematic review and network meta-analysis of randomized controlled trials. PeerJ. 2026; PMID: 41836166. https://pubmed.ncbi.nlm.nih.gov/41836166/ ↩︎
Kavousi S, Hosseinpour A, Bahmanzadegan Jahromi F, et al. Efficacy of mesenchymal stem cell transplantation on major adverse cardiovascular events and cardiac function indices in patients with chronic heart failure: a meta-analysis of randomized controlled trials. J Transl Med. 2024; PMID: 39174960. https://pubmed.ncbi.nlm.nih.gov/39174960/ ↩︎
Martinez-Lemus JD, Molony DA, Suescun J, et al. Allogeneic bone marrow-derived mesenchymal stem cells in the aging kidney: secondary results of a Parkinson's disease clinical trial. Stem Cell Res Ther. 2025; PMID: 40993774. https://pubmed.ncbi.nlm.nih.gov/40993774/ ↩︎
Napoleon H, Djohan PB, Evelyn E. Systematic Review of Stem Cells in Plastic, Reconstructive, and Aesthetic Surgery: Clinical Application in Anti-Aging Medicine. Indian J Plast Surg. 2026; PMID: 42344566. https://pubmed.ncbi.nlm.nih.gov/42344566/ ↩︎ ↩︎ ↩︎
Habiba UE, Sathyanarayanan R, Shamim S, et al. Intranasal administration of stem cells and their derivatives for neurological and respiratory disorders: a systematic review of human clinical trials. Front Aging Neurosci. 2026; PMID: 42182566. https://pubmed.ncbi.nlm.nih.gov/42182566/ ↩︎ ↩︎ ↩︎