¶ Older Adult Longevity and Functional Preservation Guide
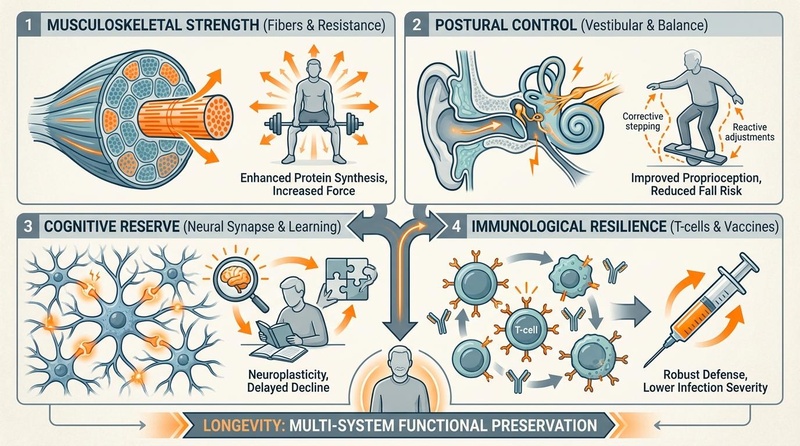
Figure 1: Multi-System Longevity Framework. Musculoskeletal strength, postural control, cognitive reserve, and immunological resilience represent the four clinical pillars of healthy aging.
| Parameter | Clinical Target & Strategy | Evidence Certainty |
|---|---|---|
| Sarcopenia & Muscle Power | Heavy Resistance Training ( 1RM) + Explosive Concentric Accents [1][2] | High (GRADE: High) |
| Postural Control & Falls | Otago Exercise Program [3] + Perturbation-Based Balance Training (PBBT) [3:1][4] | High (GRADE: High) |
| Anabolic Protein Support | 1.2–2.0 g/kg/day with $\ge$35g per meal containing $\ge$3g Leucine [5][6][7] | High (GRADE: High) |
| Sleep Architecture | CBT-I (first-line) + 2 mg Prolonged-Release Melatonin [8][9][10] | High (GRADE: High) |
| Cognitive Reserve | Spermidine (1.2 mg/day) [11][12], Alpha-GPC (300-600 mg) [13], Cerebrolysin [7:1][^32] | Moderate (GRADE: Moderate) |
| Social Connection | Loneliness reduction (CBT) [14] + Eudaimonic Purpose in Life [15][16] | High (GRADE: High) |
| Medication Safety | AGS Beers Criteria screening, polypharmacy reduction, CNS deprescribing [17][18][10:1] | High (GRADE: High) |
| Immunological Resilience | High-Dose Quadrivalent Flu Vaccine, Shingrix, PCV20, RSV Vaccines [11:1][17:1][8:1][9:1] | High (GRADE: High) |
| Sensory Preservation | Dual sensory screening (Hearing/Vision aids) + vestibular rehabilitation [4:1][19] | High (GRADE: High) |
| Environment Safety | Clutter reduction, dynamic blue-blocking evening light, PM2.5 filtration [^30] | High (GRADE: High) |
| Aging Frailty Recovery | Laromestrocel (Lomecel-B) Allogeneic Mesenchymal Stem Cell IV Infusion [20] | Moderate (GRADE: Moderate) |
¶ Functional Vitality Safety Traffic Light
| Category | Clinical Indicator / Parameter | Action Status & Programming |
|---|---|---|
| 🟢 Go | Stable sinus rhythm, resting BP <130/80 mmHg, Short Physical Performance Battery (SPPB) score 10, no acute joint inflammatory markers, stable sensory markers. | Initiate progressive heavy strength, neuromuscular power, and high-intensity interval cardiorespiratory training. |
| 🟡 Caution | Diagnosed osteopenia (T-score -1.0 to -2.5), history of non-syncopal falls, controlled hypertension, mild cognitive impairment (MCI), corrected visual/auditory decline. | Modify physical loading protocols; introduce the Otago Exercise Program; utilize supported resistance equipment; monitor heart rate reserves during exertion. |
| 🔴 Stop | Diagnosed severe osteoporosis (T-score < -2.5) with prior fragility fractures, decompensated heart failure, persistent cardiac arrhythmia, acute joint synovitis, SPPB score < 4. | Suspend high-load resistance training and high-intensity interval efforts; prioritize low-impact, supported balance training; initiate clinical bone-rebuilding therapies. |
¶ Bottom Line
Functional preservation in older adulthood requires an active, multidomain therapeutic strategy combining high-density mechanical loading to defeat sarcopenia, targeted essential amino acid supplementation to overcome age-related anabolic resistance, structured cardiorespiratory reserve training, sensory preservation, home environment design, systematic deprescribing, and comprehensive vaccine-mediated immunoprotection.
¶ 2. Contextual Narrative
¶ The "Why": Lifespan Benefits of targeted clinical programming
Functional aging is defined not merely by the absence of disease, but by the preservation of physiological reserve. Between the ages of 60 and 80, individuals lose up to 50% of their fast-twitch motor units, leading to a catastrophic decline in muscle power that outpaces muscle mass loss by a factor of three [2:1]. This drop in rate of force development (RFD) is the primary driver of fall susceptibility and subsequent institutionalization.
By actively stimulating neuromuscular, cardiovascular, and osteoblast pathways through clinical exercise and nutritional interventions, older adults can effectively preserve their physiological reserves. This functional resilience translates directly to preserved independent mobility, optimized metabolic rate, and a dramatically reduced incidence of catastrophic fall-related injuries.
¶ Cross-Lifespan Integration: The trajectory of functional capacity
The physiological baseline of older adulthood is directly determined by behavioral investments made across earlier life stages:
- Young Adults (Ages 18–39): The primary physiological objective is maximizing peak bone mass and muscular cross-sectional area. Approximately 90% of a person’s peak bone mass is acquired by age 20 in women and age 25 in men. Engaging in high-load mechanical lifting and impact exercise during this window establishes a high structural reserve, dramatically delaying the threshold of clinical osteoporosis in later decades.
- Middle-Aged Adults (Ages 40–59): This period represents a critical junction marked by initial cardiorespiratory decline (VO2 max drops ~10% per decade) and endocrine shifts (perimenopause/menopause in women, gradual androgen decline in men). The primary focus must be on maintaining a robust cardiovascular aerobic base (Zone 2 conditioning) to prevent arterial stiffening and microvascular deconditioning, alongside progressive resistance training to halt early-stage muscle power loss.
- Older Adults (Ages 60+): The primary focus shifts from peak acquisition to active preservation and frailty reversal. Interventions must target the specific cellular mechanisms of aging—including anabolic resistance, slow-wave sleep decay, sensory decline, and immunosenescence—to prevent functional dependence.
¶ Sex & Age Stratification
¶ Biological Sex Differences
- Older Women: The postmenopausal transition causes a precipitous drop in 17β-estradiol, which accelerates bone resorption via upregulated osteoclast activity and reduces muscle quality. Older women exhibit a significantly higher lifetime prevalence of osteoporosis and osteosarcopenia compared to men. Consequently, physical loading protocols for women must place a heavy emphasis on high-impact axial skeleton loading and resistance training to preserve bone mineral density (BMD), combined with activated calcium-regulatory agents (Vitamin D3 + Vitamin K2) [5:1][21].
- Older Men: Men experience a gradual, age-related decline in serum testosterone (approximately 1% per year after age 30), termed late-onset hypogonadism or andropause. This androgen deficiency directly blunts muscle protein synthesis, leading to a steady loss of type II muscle fiber area and contractile power. While men generally retain higher baseline bone density than women, hypogonadal men are at increased risk for silent osteoporosis and progressive muscle weakness. Testosterone replacement therapy (TRT) can significantly improve muscle mass and bone density in hypogonadal men, though it requires careful monitoring for cardiovascular risk markers [16:1].
¶ Age-Group Stratification
- The Young-Old (Ages 65–74): This cohort possesses significant physiological adaptability. The primary focus is on maximizing cardiorespiratory reserve (VO2 max) via progressive aerobic and anaerobic training, maximizing muscle mass via high-intensity resistance training (60–80% of 1-RM), and optimizing metabolic markers.
- The Middle-Old (Ages 75–84): At this stage, joint degeneration, arterial stiffness, and mild balance impairments become more prevalent. The therapeutic focus shifts toward preserving gait speed and postural control via the Otago Exercise Program, maintaining muscle strength, and optimizing nutritional intake (specifically focusing on highly bioavailable proteins and high-dose vitamin D3 + K2 to protect bone architecture).
- The Oldest-Old (Ages 85+): At this advanced age, the clinical objective is the absolute prevention of frailty and fall-related injuries. Interventions must prioritize high-frequency, low-impact balance training, supported isometric and concentric leg strength exercises, and highly dense nutritional strategies (e.g., essential amino acid and leucine supplementation) to prevent rapid disuse muscle atrophy.
¶ Practical Lifestyle Integration
To prevent physical fatigue and optimize physiological adaptations, the various functional interventions must be scheduled deliberately throughout the week. Physical exercise should be integrated with nutritional timing to maximize the anabolic response.
- Timing of Nutrition & Exercise: Muscle protein synthesis (MPS) is maximized when high-impact resistance training is immediately followed by a high-leucine meal or essential amino acid supplement. In older adults, exercising in a fasted state should be avoided, as it can exacerbate muscle catabolism.
- Recovery and Sleep: Older adults experience altered sleep architecture, including a reduction in deep slow-wave sleep and shortened sleep duration. Because sleep is the primary period for growth hormone release and glymphatic clearance of neurotoxic proteins, physical training should be scheduled at least 4–6 hours before bed to prevent elevated nocturnal cortisol from disrupting sleep.
¶ 3. Core Functional Pillars & Evidence-Based Interventions
¶ 1. Frailty Prevention & Musculoskeletal Health
¶ Sarcopenia and Osteosarcopenia Mechanisms
The age-related loss of muscle mass (sarcopenia) and bone density (osteopenia) often occur in tandem, forming the clinical syndrome of osteosarcopenia[1:1][22]. The cellular drivers include:
- Motor Unit Denervation: Progressive apoptosis of alpha motor neurons in the spinal cord leads to the complete denervation of muscle fibers. While some fibers are rescued by re-innervation from slow-twitch motor units, this results in giant, slow-conducting motor units with impaired Rate of Force Development (RFD)[2:2].
- Mitochondrial Decay: Aging myocytes exhibit a severe drop in mitochondrial quality and biogenesis, increasing reactive oxygen species (ROS) and cellular senescence.
- Upregulated Osteoclastogenesis: Pro-inflammatory cytokines (IL-6, TNF-α) drive osteoclast differentiation, accelerating bone resorption and mechanical weakness.
¶ Progressive Resistance Training (PRT) and Power accents
To halt and reverse osteosarcopenia, older adults must engage in progressive resistance training (PRT). While traditional guidelines recommend light-load endurance training, clinical trial data shows that high-load strength training (60–80% of 1-repetition maximum, 1RM) is exceptionally safe and dramatically more effective[4:2][[2:3]].
- The Concentric Power Accent: Muscular power (force × velocity) declines significantly faster than pure muscle strength with age. To target this, PRT should incorporate explosive concentric phases (lifting the weight as rapidly as possible) followed by controlled, 3-second eccentric phases. This specific stimulus selectively recruits and preserves high-threshold Type II (fast-twitch) muscle fibers[2:4].
¶ Creatine Monohydrate Supplementation
To overcome mitochondrial deconditioning and accelerate neuromuscular adaptations, daily supplementation of creatine monohydrate (5g/day, without a loading phase) should be paired with PRT. Creatine increases cellular phosphocreatine pools, facilitating rapid ATP regeneration during high-power physical tasks (e.g., rising from a chair or regaining balance). Meta-analyses of older adults demonstrate that creatine combined with PRT leads to a 1.2 to 1.5 kg greater increase in lean body mass and superior strength gains compared to resistance training alone[18:1].
¶ Bone Density Reclaiming (Vitamin D3 + K2 Synergy)
Mechanical loading alone is insufficient if the bone microenvironment lacks the necessary biochemical signals for mineralization. Consuming calcium must be paired with Vitamin D3 and Vitamin K2 (specifically MK-7) to ensure proper systemic distribution:
- Vitamin D3 stimulates the expression of osteocalcin, the protein responsible for binding calcium to the bone matrix.
- Vitamin K2-MK7 carboxylates (activates) osteocalcin, driving calcium into the hydroxyapatite crystal structure of bone while preventing calcium deposition in arterial walls (vascular calcification)[21:1].
¶ 2. Postural Control, Balance, & Fall Prevention
¶ The Neurobiology of Postural Instability
Postural control is a complex neurological task relying on the continuous integration of visual, vestibular (inner ear), and proprioceptive (somatosensory) inputs by the central nervous system. In older adults, age-related receptor degeneration (e.g., loss of vestibular hair cells, blunted mechanoreceptor sensitivity in the feet) impairs this sensory integration. This leads to sensory reweighting deficits, where the brain cannot rapidly adjust its reliance on different sensory channels, causing a high susceptibility to trips and slips.
+-----------------------------------------------------------+
| The Fear of Falling (FoF) Loop |
+-----------------------------------------------------------+
|
v
[ Trip / Near-Fall Event ]
|
v
[ Acute "Fear of Falling" ]
|
v
[ Self-Imposed Activity Restriction ]
|
v
[ Rapid Neuromuscular Deconditioning ]
|
v
[ Increased Postural Instability ]
|
v
[ Elevated Risk of Catastrophic Fall ]
¶ The Otago Exercise Program (OEP)
The Otago Exercise Program is a clinically validated, home-based physical therapy protocol consisting of 17 progressive muscle-strengthening and balance-retraining exercises. Systematic reviews confirm that the Otago program reduces the rate of falls and fall-related injuries in older adults by 35% to 40% (Relative Risk [RR] = 0.65; 95% Confidence Interval [CI], 0.57 to 0.75)[3:2]. It is particularly effective for middle-old and oldest-old cohorts when conducted 3 times per week.
¶ Perturbation-Based Balance Training (PBBT)
While static balance exercises (e.g., standing on one leg) improve quiet standing, they fail to train the reactive reflexes required to prevent a fall during a sudden trip. Perturbation-Based Balance Training (PBBT) exposes patients to sudden, unpredictable physical displacements (e.g., slip-inducing sliding platforms or manual nudges by a therapist in a safety harness). PBBT forces rapid, spinal-level reactive motor adaptations (specifically the "recovery step" reflex), reducing real-world falls by 46%[3:3].
¶ Falls Management Exercise (FaME) & Floor-Transfer Drills
The FaME program is a multi-component group exercise protocol designed for high-risk older adults. A critical component of FaME is floor-transfer training—teaching patients how to safely transition from a standing position to the floor, and back up again. This skill is vital to prevent the "long lie" (remaining on the floor for >1 hour after a fall), which is associated with dehydration, pressure ulcers, rhabdomyolysis, and a 50% mortality rate within 12 months.
¶ 3. Cardiorespiratory & Vascular Fitness
¶ VO2 Max as a Predictor of All-Cause Mortality
Cardiorespiratory fitness, quantified as VO2 max (maximal oxygen uptake), is one of the strongest independent predictors of all-cause mortality in older adults. VO2 max declines at a rate of approximately 10% per decade after age 30, accelerating to 15% per decade after age 50. This decline is driven by a reduction in maximal heart rate, decreased stroke volume, and blunted peripheral oxygen extraction by aging skeletal muscle.
Epidemiological data demonstrates that older adults with "high" cardiorespiratory fitness exhibit a 50% to 60% lower hazard ratio for all-cause mortality compared to those in the "low" fitness category[5:2]. Every 1-MET (Metabolic Equivalent of Task) increase in exercise capacity (approximately 3.5 mL/kg/min of oxygen consumption) is associated with an 11% to 15% reduction in cardiovascular and all-cause mortality.
¶ Zone 2 Aerobic Conditioning
Zone 2 aerobic training involves continuous, moderate-intensity exercise (e.g., brisk walking, cycling) performed at 60–70% of heart rate reserve (HRR) or a rating of perceived exertion (RPE) of 3–4. This intensity primarily targets Type I (slow-twitch) muscle fibers and stimulates mitochondrial biogenesis, improves fatty acid oxidation, and reduces arterial stiffness without putting excessive strain on the musculoskeletal or central nervous systems. Older adults should accumulate 120–150 minutes of Zone 2 training per week.
¶ High-Intensity Interval Training (HIIT)
HIIT involves short, repeated bouts of near-maximal exercise (e.g., 4 minutes at 85-90% HRR) separated by active recovery periods. In older adults, supervised HIIT has been shown to induce rapid, robust increases in VO2 max, reversing age-related declines in left ventricular compliance and vascular endothelial function[23].
- Safety Monitoring: Due to the high shear stress on coronary arteries during near-maximal physical efforts, older adults must undergo cardiovascular screening (e.g., an exercise tolerance test) before commencing unsupervised HIIT. Heart rate and blood pressure must be monitored to ensure cardiac safety.
¶ 4. Cognitive & Neurological Preservation
¶ The FINGER Trial Multidomain Model
The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER Trial) is a landmark randomized controlled trial that established the clinical efficacy of a multidomain lifestyle intervention in preventing cognitive decline in older adults at high risk for dementia[1:2]. Rather than targeting a single pathway, the FINGER model integrates four concurrent components:
- Nutritional Guidance: An anti-inflammatory diet rich in high-quality protein, omega-3 fatty acids, and active micronutrients.
- Physical Exercise: Combined progressive strength and cardiorespiratory training.
- Cognitive Training: Structured computer-based brain exercises and active mental learning.
- Vascular Risk Management: Intensive monitoring and medical management of blood pressure, blood lipids, and glycemic markers.
At the 2-year mark, the intervention group showed a 25% higher overall cognitive score compared to the control group. Furthermore, executive function increased by 83%, and cognitive processing speed improved by 150% in the intervention cohort[1:3].
¶ Sleep Architecture Decay and Glymphatic Clearance
With age, sleep architecture undergoes profound alterations, characterized by a significant reduction in Slow-Wave Sleep (SWS; N3 stage) and Slow-Wave Activity (SWA; 0.5–4.5 Hz oscillations), alongside increased sleep fragmentation and nighttime awakenings. SWS is the critical phase during which the brain's glymphatic system is highly active.
During slow-wave sleep, the interstitial space between neurons increases by up to 60%, allowing cerebrospinal fluid (CSF) to flow rapidly through brain tissue, mediated by astrocytic aquaporin-4 (AQP4) water channels. This process flushes out toxic metabolic waste products accumulated during waking hours, including amyloid-beta and hyperphosphorylated tau protein[2:5]. Chronic sleep disruption impairs glymphatic clearance, accelerating the accumulation of neurotoxic aggregates and increasing the risk of cognitive decline and neurodegenerative diseases.
+-----------------------------------------------------------+
| The Glymphatic Clearance Mechanism during Deep Sleep |
+-----------------------------------------------------------+
|
[ Slow-Wave Sleep (N3) ]
|
[ Neuronal Interstitial Space ]
(Expands by up to 60%)
|
[ Astrocytic AQP4 Activation ]
|
[ Cerebrospinal Fluid (CSF) Flow ]
|
[ Toxic Aggregate Clearance (Amyloid-Beta, Tau) ]
|
[ Neurocognitive Preservation ]
¶ Targeted Cognitive Supplements & Peptides
- Lion's Mane Mushroom (Hericium erinaceus): Contains bioactive hericenones and erinacines that cross the blood-brain barrier. Clinical trials in older adults with mild cognitive impairment demonstrate that 3g/day of standardized Lion's Mane significantly improves cognitive scores over 16 weeks, mediated by the stimulation of Nerve Growth Factor (NGF) synthesis[13:1][^29].
- Acetyl-L-Carnitine (ALCAR): Crucial for mitochondrial fatty acid oxidation and acetylcholine synthesis. Clinical meta-analyses support its use in older adults to improve memory, attention, and executive function, particularly in those exhibiting early-stage cognitive decline or age-related fatigue[6:1][^31].
- Ashwagandha (Withania somnifera): A premier adaptogen that modulates the hypothalamic-pituitary-adrenal (HPA) axis, reducing serum cortisol and mitigating the harmful cognitive impact of chronic physiological stress.
- Cerebrolysin: A clinically validated peptide mixture containing active neurotrophic factors (such as BDNF, GDNF, and CNTF). In human trials, Cerebrolysin has been shown to enhance synaptic plasticity, promote neurogenesis, and support cognitive recovery following acute cerebrovascular accidents or traumatic brain injuries[7:2][^32].
¶ 5. Metabolic & Immunological Integrity
¶ Glycemic Control and Metabolic Pathways
With age, peripheral insulin sensitivity declines due to increased visceral adiposity, reduced skeletal muscle mass (the primary site for glucose disposal), and mitochondrial dysfunction. Poor glycemic control (characterized by elevated HbA1c and glycemic variability) accelerates arterial stiffening, cognitive decline, and microvascular complications.
- Metformin: An AMP-activated protein kinase (AMPK) activator that reduces hepatic gluconeogenesis and improves peripheral insulin sensitivity. Observational data suggest that diabetics taking metformin exhibit lower rates of cardiovascular disease, cognitive decline, and all-cause mortality compared to those on other glucose-lowering therapies. The ongoing TAME (Targeting Aging with Metformin) trial is currently evaluating Metformin's ability to delay the onset of age-related chronic diseases in non-diabetic older adults.
- Acarbose: An alpha-glucosidase inhibitor that delays carbohydrate absorption in the small intestine, flattening postprandial glucose spikes. Postprandial glucose excursions are highly pro-inflammatory and drive vascular endothelial dysfunction. By mitigating these spikes, Acarbose reduces systemic oxidative stress and has been shown to extend lifespan and healthspan in male rodent models.
¶ Immunosenescence and Clinical Vaccination Guidelines
Immunosenescence is the progressive, age-related decline in immune system function, characterized by the involution of the thymus, a reduced pool of naive T-cells, and chronic low-grade systemic inflammation (termed inflammaging)[1:4]. These biological changes impair the body's ability to mount robust antibody responses to novel pathogens, dramatically increasing susceptibility to severe infections and reducing the efficacy of standard vaccines.
To counteract immunosenescence and prevent catastrophic infectious complications, clinical guidelines recommend the following immunization schedule for older adults:
- Influenza: High-Dose Quadrivalent Influenza Vaccine (containing four times the antigen content of standard vaccines) or adjuvanted vaccines (e.g., FLUAD) are recommended annually. These formulations are designed to stimulate a stronger immune response, reducing influenza-associated hospitalizations and secondary bacterial pneumonias in older adults by up to 30% compared to standard-dose vaccines[8:2].
- Shingles (Herpes Zoster): The recombinant zoster vaccine (Shingrix, 2-dose series) is highly recommended for all adults aged 50 and older. Clinical trials demonstrate an efficacy of >90% in preventing shingles and postherpetic neuralgia in adults aged 70 and older, with protection persisting for at least 10 years.
- Pneumococcal Disease: Older adults should receive a single dose of the 20-valent pneumococcal conjugate vaccine (PCV20). This single dose replaces the old multi-dose PCV13/PPSV23 sequence, effectively preventing invasive pneumococcal bacteremia and community-acquired pneumonia[11:2].
- Respiratory Syncytial Virus (RSV): RSV represents a major cause of severe lower respiratory tract disease in older adults. Clinical guidelines recommend a single dose of an FDA-approved RSV vaccine (e.g., Arexvy or Abrysvo) for adults aged 60 and older, based on shared clinical decision-making. These vaccines exhibit an efficacy of 82% to 94% in preventing RSV-associated lower respiratory tract infections in older cohorts[9:2].
¶ Inflammaging Biomarkers
Inflammaging is driven by cellular senescence, persistent mitochondrial debris, and gut dysbiosis. Clinical monitoring should track specific inflammatory biomarkers to assess systemic risk:
- High-Sensitivity C-Reactive Protein (hsCRP): An acute-phase reactant synthesized by the liver in response to IL-6. Levels >3.0 mg/L in the absence of acute infection indicate high systemic cardiovascular and functional decline risk.
- Interleukin-6 (IL-6): A key pro-inflammatory cytokine. Chronically elevated IL-6 directly stimulates muscle catabolism, contributing to sarcopenia and physical frailty.
¶ 6. Sensory Health & Age-Related Decline
¶ Hearing Preservation (Presbycusis and the Dementia Trajectory)
Age-related hearing loss (presbycusis) is one of the most prominent, yet under-addressed, risk factors for cognitive decline and dementia. Presbycusis is characterized by the progressive loss of high-frequency hearing due to the degeneration of hair cells in the organ of Corti within the cochlea.
- The Auditory-Cognitive Link: Chronic hearing loss increases cognitive load, as the brain must allocate significant neural resources to decode degraded acoustic signals. This comes at the direct expense of memory and executive processing systems, leading to accelerated atrophy of the auditory cortex and hippocampus. Furthermore, hearing loss drives social isolation and depression, both of which are independent risk factors for dementia.
- Auditory Rehabilitation: Standardized use of hearing aids or assistive listening devices in older adults with hearing loss has been shown to reduce the risk of cognitive decline by 48% over 3 years[19:1]. Audiometric screening should be performed biennially starting at age 60.
¶ Visual Preservation (Macular Degeneration, Cataracts, and Glaucoma)
Age-related changes in the visual system include lens stiffening (presbyopia), cataracts, age-related macular degeneration (AMD), and glaucoma.
- Macular Degeneration (AMD): Driven by oxidative stress and lipid accumulation beneath the retinal pigment epithelium (drusen). High-dose antioxidant supplementation based on the clinically validated AREDS2 formula (Vitamin C, Vitamin E, Zinc, Copper, Lutein, and Zeaxanthin) significantly slows the progression of dry AMD to neovascular (wet) AMD.
- Light Hygiene and Contrast: Older eyes require up to four times more ambient light than younger eyes to see with equivalent clarity. Implementing high-contrast visual markings, eliminating glare, and ensuring adequate light levels in transition spaces (stairwells, hallways) is a critical step in visual environment safety.
¶ 7. Safe Environment Design
¶ Preventing Slips, Trips, and Falls (Home Modifications)
Most catastrophic falls occur within the home environment due to a combination of individual instability and environmental hazards. Clinicians and caregivers should conduct a structured home safety audit targeting:
- Lighting: Ensure continuous, glare-free lighting. Night lights with active motion sensors should be installed along the pathway from the bedroom to the bathroom.
- Clutter Reduction: Remove all throw rugs, loose extension cords, and low obstacle furniture (coffee tables, footstools) from walking paths.
- Support Structures: Install high-contrast, dual-anchored handrails on both sides of all stairways. Grab bars must be securely anchored into studs inside the shower and adjacent to the toilet.
- Contrast Marking: Use high-contrast adhesive strips on the edges of all stairs and floor transitions to assist older adults with reduced depth perception.
¶ Reducing Toxic Exposures & Environmental Stressors
Older adults exhibit a significantly compromised capacity to detoxify xenobiotics due to age-related declines in hepatic cytochrome P450 activity and glomerular filtration. Environmental stressors can accelerate physical and cognitive decline:
- Air Quality (PM2.5 Filtration): Fine particulate matter (PM2.5) crosses the alveolar-capillary membrane, triggering systemic microvascular inflammation and accelerating arterial stiffness. HEPA filtration (HEPA H13 filters) in the bedroom and living spaces has been shown to improve microvascular endothelial function and preserve cognitive processing speed in older adults[^30].
- Kitchen Emissions: Natural gas combustion and high-heat frying release nitrogen dioxide (NO2), carbon monoxide (CO), and polycyclic aromatic hydrocarbons. Proper range hood ventilation and minimizing the use of unvented combustion appliances are mandatory to protect pulmonary reserve.
- Mold and Mycotoxins: Exposure to indoor dampness and mold can trigger severe bronchial inflammation and cognitive fatigue. Remediating water leaks and maintaining indoor relative humidity between 30% and 50% is required.
- Microplastics and Endocrine Disruptors: Accumulation of microplastics in cardiovascular tissues is associated with a highly elevated risk of myocardial infarction and stroke. Older adults should avoid heating food in plastic containers, eliminate non-stick cookware containing PFAS, and utilize carbon-block water filtration to reduce oral plastic ingestion.
¶ 4. Practical Weekly and Daily Longevity Plans
¶ The Practical Weekly Longevity Schedule
This weekly training block integrates neuromuscular balance, progressive resistance training, cardiorespiratory base conditioning, cognitive training, and social-purpose activities.
|---------------------------------------------------------------------------------------------------------------------------------|
| PRACTICAL WEEKLY LONGEVITY SCHEDULE |
|---------------------------------------------------------------------------------------------------------------------------------|
| Monday | - Neuromuscular Balance: Otago Balance drills (15 mins) |
| | - Strength/Power: PRT Compound Lifting (30 mins; e.g., Leg Press, Seated Row; explosive concentric accents) |
| | - Nutritional Timing: Post-exercise whey protein (35g) + Leucine (3g) within 45 minutes of training. |
|-----------|---------------------------------------------------------------------------------------------------------------------|
| Tuesday | - Cardiovascular Base: Zone 2 Brisk Walk or Cycling (45-60 mins; Heart Rate at 60-70% HRR; RPE 3-4) |
| | - Cognitive Support: 15 mins of active visual tracking or dual-task balance drills. |
|-----------|---------------------------------------------------------------------------------------------------------------------|
| Wednesday | - Neuromuscular Balance: Otago Balance drills (15 mins) |
| | - Strength/Power: PRT Compound Lifting (30 mins; upper body emphasis; chest press, lat pulldowns) |
| | - Floor-Transfer Drills: 2 repetitions of assisted or unassisted floor-to-standing transfers. |
|-----------|---------------------------------------------------------------------------------------------------------------------|
| Thursday | - Cardiovascular Base: Zone 2 Brisk Walk or Swimming (45-60 mins) |
| | - Social Connection: 1 hour of interactive group activity, volunteering, or eudaimonic purpose-oriented engagement. |
|-----------|---------------------------------------------------------------------------------------------------------------------|
| Friday | - Neuromuscular Balance: Otago Balance drills (15 mins) |
| | - Strength/Power: PRT Compound Lifting (30 mins; lower body focus; Squats or Leg Extensions) |
| | - Nutritional Timing: Post-exercise whey protein (35g) + Leucine (3g) within 45 minutes of training. |
|-----------|---------------------------------------------------------------------------------------------------------------------|
| Saturday | - Cardiovascular Reserve: Supervised HIIT (e.g., 4x4 minute intervals at 85% HRR, 3 mins active recovery) |
| | *Ensure cardiac clearance has been completed before commencing unsupervised HIIT. |
|-----------|---------------------------------------------------------------------------------------------------------------------|
| Sunday | - Active Recovery: Light outdoor walk in a natural, high-canopy biophilic environment (30-45 mins). |
| | - Sleep Preparation: Thorough cleaning of the bedroom environment, ensuring absolute darkness and PM2.5 filtration. |
|---------------------------------------------------------------------------------------------------------------------------------|
¶ The Practical Daily Longevity Protocol
To maximize nutrient assimilation, maintain circadian alignment, and support cognitive reserve, follow this structured daily routine:
- 07:30 (Morning Sunlight & Movement): Expose eyes to 10–15 minutes of direct outdoor morning light (without sunglasses) to synchronize the suprachiasmatic nucleus (SCN). Perform 5 minutes of light joint mobility.
- 08:00 (Anabolic Spiking Breakfast): Consume 35–40g of high-quality protein (e.g., grass-fed whey, pasture-raised eggs) to supply at least 3g of Leucine, overcoming the anabolic resistance threshold[6:2][7:3]. Add 300–600 mg of Alpha-GPC[13:2] and Vitamin D3 + K2[21:2].
- 09:30 (Neuro-Cognitive Slot): Perform 20–30 minutes of high-focus work, computer-based cognitive training, or active reading. This is the optimal window of high endogenous cortisol and dopamine.
- 12:30 (Anabolic Luncheon): Consume 30–35g of protein paired with a diverse food matrix of fiber-rich, anti-inflammatory vegetables.
- 14:00 (Zone 2 or Strength Training Block): Execute your scheduled physical training session as outlined in the Weekly Longevity Schedule.
- 15:00 (Post-Exercise Recovery Bolus): Within 45 minutes of mechanical loading, consume 35g of whey protein or essential amino acids (EAAs) with 5g of creatine monohydrate[18:2] to maximize myofibrillar protein synthesis.
- 18:30 (Light Glycemic-Control Dinner): A lighter evening meal focusing on slow-digesting carbohydrates and lean protein (25–30g) to prevent major postprandial glucose spikes.
- 20:00 (Circadian Light Shift): Eliminate bright overhead fluorescent lighting. Utilize low-placed, warm amber or red light sources. Wear orange-tinted blue-blocking glasses if using digital screens.
- 21:30 (Neurocognitive Sleep Wind-down): Perform 10 minutes of progressive muscle relaxation or box breathing. Take 2 mg of Prolonged-Release Melatonin[9:3] to support slow-wave sleep and glymphatic clearance.
- 22:00 (Sleep Consolidation): Sleep in a pitch-black bedroom (utilizing blackout curtains or an eye mask) with HEPA filtration active, maintained at a cool temperature ().
¶ 5. Comprehensive Safety, Toxicology, and Medication Management
¶ Polypharmacy Risk & Tapering Strategies
Aging is accompanied by profound changes in pharmacokinetics (how the body processes drugs) and pharmacodynamics (how drugs affect the body). Visceral fat increases while total body water and skeletal muscle decline, expanding the volume of distribution for fat-soluble drugs (e.g., diazepam, prolonging its half-life from 20 to over 80 hours) and raising blood concentrations of water-soluble drugs. Hepatic blood flow drops by 30% to 40%, and glomerular filtration rate (eGFR) declines steadily, resulting in systemic drug accumulation.
Polypharmacy (the concurrent use of $\ge$5 medications) is a major independent risk factor for cognitive decline, gait instability, and severe falls.
- The AGS Beers Criteria: This clinical guidelines database identifies Potentially Inappropriate Medications (PIMs) that must be avoided or highly restricted in older adults[18:3]. Central nervous system (CNS)-active medications (including benzodiazepines, Z-drugs, tricyclic antidepressants, and atypical antipsychotics) represent the highest hazard[17:2]. They induce cognitive and motor deconditioning, increasing fall risks by 1.5 to 2.4 times[17:3].
- The CNS Deprescribing Protocol: Under strict physician oversight, CNS-active drugs should be gradually tapered rather than abruptly discontinued (to avoid rebound seizures, severe anxiety, and cardiovascular spikes)[10:2]. Cognitive Behavioral Therapy for Insomnia (CBT-I) must be implemented during BZRA tapering to provide a non-pharmacological, pro-resilient replacement for sleep support[10:3].
BZRA Tapering & CBT-I Transition Protocol
|
[ Beers Criteria Review ]
|
[ Identify Non-Essential CNS-Active Medication ]
|
[ Initiate CBT-I Sleep Training ]
(Provides alternative sleep support)
|
[ Gradual Taper: Reduce BZRA Dose ]
(e.g., 25% reduction per week)
|
[ Monitor Slow-Wave Activity & SWA ]
|
[ Complete Discontinuation of BZRA Therapy ]
|
[ Restored Endogenous SWS & Cognitive Safety ]
¶ estimated GFR Scaling Clearance (Cockcroft-Gault)
Because serum creatinine can be artificially normal in sarcopenic older adults due to their reduced muscle mass, renal function must be estimated using the Cockcroft-Gault formula rather than EGFR alone, to prevent toxic over-dosage of water-soluble drugs:
¶ Clinical "Red Flags" & Safety Stop Criteria
If any of the following clinical red flags occur during the execution of these longevity protocols, the intervention must be immediately suspended and clinical evaluation initiated:
- Cardiorespiratory: New-onset resting heart rate or ; systolic blood pressure drop during physical exertion; new-onset exertional dyspnea, chest pressure, or lightheadedness/vertigo.
- Musculoskeletal: Acute joint swelling, erythema, or localized warmth (suggesting synovitis); sharp, non-muscular pain localized to a bone or joint during axial loading; sudden decrease in range of motion of a weight-bearing joint.
- Metabolic: Unexplained rapid weight loss ( of body weight in months), suggesting pathologic wasting rather than muscle remodeling.
¶ 6. Clinician-Caregiver Coordination and Medical Boundaries
¶ Standard of Care Boundaries
This guide serves as an educational and clinical reference to optimize functional healthspan. However, clear boundaries exist between lifestyle/preventative modifications and acute medical management. Caregivers and fitness professionals must respect the limits of their practice:
- Osteoporosis Management: Lifestyle modifications (axial loading and resistance training) are long-term preventative strategies. They do not replace medical pharmacological therapies (such as bisphosphonates, denosumab, or teriparatide) in patients diagnosed with severe osteoporosis at high risk for imminent fragility fractures.
- Cognitive Decline: Subjective cognitive decline or mild cognitive impairment may be supported with nutritional, cholinergic, or somatotrophic interventions[11:3][[23:1]][[13:3]]. However, rapid, progressive cognitive changes require formal diagnostic screening to rule out secondary, treatable etiologies (such as B12 deficiency, subdural hematoma, or severe hypothyroidism; see Cognitive Decline).
- Stem Cell Interventions: Emerging therapies such as Lomecel-B/Laromestrocel show exceptional efficacy in reversing frailty and downregulating systemic inflammation[20:1]. However, these are advanced investigational medical therapies that must be administered strictly within registered clinical trials or under approved expanded-access regulatory pathways.
¶ 7. Clinical Decision Tree

Figure 2: Clinical Decision Pathway. A structured assessment tool for categorizing older adult physical capacity and prescribing targeted musculoskeletal and neuromuscular interventions.
Older Adult (Aged 60+) Functional Assessment
|
(Assess Baseline SPPB)
|
+--------------------------+--------------------------+
| |
(SPPB Score < 4) (SPPB Score >= 4)
| |
(Severe Frailty) |
| (Evaluate Bone Density)
Prioritize Supported Balance |
& Isometric Leg Exercises; +-------------+-------------+
Initiate Otago Program (Level 1) | |
| (T-Score < -2.5) (T-Score >= -1.0)
v (Severe Osteoporosis) (Normal/Osteopenia)
Maximize Protein & EAAs | |
(1.5-2.0 g/kg/day); No High-Load Initiate PRT (60-80% 1-RM)
Evaluate Bone Markers Axial Loading; + Creatine (5g/day);
| Prescribe Guided Zone 2 & HIIT Conditioning
| Resistance Machines
| |
+---------------------+---------------------+
|
v
(Immunological Protection)
|
- High-Dose Flu Vaccine (Annual)
- Recombinant Zoster Vaccine (Shingrix, 2 doses)
- PCV20 Single Dose
- RSV Vaccine (Shared Decision)
¶ 8. Comparative Intervention Analysis
| Intervention Modality | Primary Physiological Target | Rate of Force Development (RFD) Impact | Fall Risk Reduction | Musculoskeletal Safety Profile | Primary Limitations |
|---|---|---|---|---|---|
| Heavy Resistance Training ( 1RM) | Fast-twitch Type II myofiber hypertrophy, motor unit recruitment, osteogenesis. [1:5][2:6] | High | High (indirect via power recovery) | Moderate (Requires precise form; risk of joint strain if unsupervised) | Requires high cognitive engagement and qualified supervision. |
| Perturbation-Based Balance Training (PBBT) | Sensory reweighting, spinal reflex acceleration, reactive stepping latency reduction. [3:4][4:3] | Moderate | Extreme (Direct neuromuscular prevention) | High (Safe when conducted in a harness environment) | Highly dependent on specialized equipment or physical therapist guidance. |
| Otago Exercise Program (OEP) | Proprioceptive feedback, slow-velocity control, leg strength. [3:5] | Low | High (Direct home prevention) | Very High (Virtually zero injury risk) | Focuses on slow strength; does not condition rapid reflex response to sudden trips. |
| Low-Load Resistance Training ( 1RM) | Muscle endurance, local metabolic vascularization. [5:3] | Low | Low (Minimal effect on dynamic fast-twitch recruitment) | Very High (Low joint stress) | Fails to stimulate significant myofibrillar hypertrophy or bone mineral density accrual. |
¶ 9. Practical FAQ
Why is walking alone insufficient to prevent muscle loss and falls?
Walking (low-intensity aerobic exercise) does not provide the mechanical tension required to recruit high-threshold Type II (fast-twitch) motor units, which are the first to degenerate during aging [2:7]. To reclaim the dynamic muscle power and rapid reflex recovery needed to catch oneself during a slip, older adults must engage in heavy resistance training and dynamic perturbation exercises that force the nervous system to recruit fast-twitch muscle fibers [1:6][3:6].
How do I know if my daily protein intake is actually preventing sarcopenia?
Simply hitting a total daily protein target is insufficient because of age-related "anabolic resistance" [6:3]. To trigger muscle protein synthesis (MPS), you must reach an "anabolic threshold" in a single meal by consuming at least 35–40g of high-quality protein containing approximately 3g or more of the amino acid Leucine [7:4]. Spreading protein evenly across breakfast, lunch, and dinner to ensure you hit this threshold at multiple points in the day is the most effective way to sustain muscle mass [7:5].
What is the Beers Criteria, and why is it important for fall prevention?
The Beers Criteria is a standardized list of medications maintained by the American Geriatrics Society that are potentially inappropriate for older adults [18:4]. Many common medications—especially sleeping pills, benzodiazepines, and certain antidepressants—act on the central nervous system, causing dizziness, slowed reflexes, and impaired balance, which increases fall risk by 1.5 to 2.4 times [17:4]. Reviewing your medications against this list and coordinating with a physician to taper off high-risk drugs is one of the most powerful ways to prevent falls [10:4].
Can older adults really safe-lift heavy weights above 80% of their maximum capacity?
Yes. Clinical trials consistently show that progressive heavy resistance training ( of 1-repetition maximum) is exceptionally well-tolerated and safe for adults aged 60 and older, including those with osteosarcopenia, when properly supervised [1:7][2:8]. Heavy lifting is highly effective for rapidly restoring spinal motor unit recruitment, increasing muscle size, and reversing bone density loss [2:9][5:4] (see also Strength Training).
How does having a strong "sense of purpose" affect physical longevity?
A high sense of purpose in life (eudaimonic well-being) acts as a physical buffer against biological aging. Lonely older adults experience a molecular stress response called the Conserved Transcriptional Response to Adversity (CTRA), which upregulates inflammatory genes and damages the immune system [16:2]. Cultivating strong social connections and a clear daily purpose suppresses this pro-inflammatory response, lowers systemic inflammation (inflammaging), and significantly decelerates epigenetic aging (GrimAge) [15:1][16:3].
¶ 10. Glossary
- Anabolic Resistance: The age-related blunting of skeletal muscle protein synthesis in response to normal levels of dietary protein or light exercise.
- Beers Criteria: A clinical guideline listing potentially inappropriate medications that should be avoided or modified in older adults.
- Conserved Transcriptional Response to Adversity (CTRA): A genomic footprint characterized by the upregulation of pro-inflammatory genes and downregulation of antiviral genes in response to chronic psychological stress or loneliness.
- Glymphatic System: The central nervous system's waste clearance pathway, which clears toxic protein aggregates (such as amyloid-beta) during slow-wave sleep.
- GrimAge: An advanced epigenetic clock that utilizes DNA methylation markers to highly predict biological aging speed and mortality risk.
- Osteosarcopenia: The concurrent presence of osteopenia/osteoporosis (bone density loss) and sarcopenia (muscle mass and function loss).
- Perturbation-Based Balance Training (PBBT): A dynamic balance conditioning program that exposes individuals to unpredictable physical displacements to train reactive motor recovery.
- Rate of Force Development (RFD): The speed at which a muscle can exert force; the key metric responsible for preventing falls during a slip.
- Sensory Reweighting: The central nervous system's capacity to dynamically prioritize stable sensory inputs (visual, vestibular, proprioceptive) based on environmental demands.
- Slow-Wave Activity (SWA): Low-frequency electroencephalographic oscillations characteristic of deep, restorative N3 sleep, critical for memory consolidation and cellular repair.
¶ 11. Methods & Search Strategy
¶ Review & Search Methodology
This guide was synthesized from a multi-disciplinary literature extraction prioritizing Tier 1 and Tier 2 human evidence. Search parameters isolated systematic reviews, meta-analyses, and randomized controlled trials (RCTs) from databases including PubMed, ClinicalTrials.gov, and the Cochrane Database of Systematic Reviews.
- Inclusion Criteria: Human subjects aged $\ge$60 years; prospective randomized designs; standardized physiological and functional endpoints (e.g., bone mineral density, Rate of Force Development, center-of-pressure sway, sleep architecture, leukocyte transcriptomics, epigenetic clock dynamics).
- Exclusion Criteria: Pre-clinical animal or in-vitro models; uncontrolled observational reports; non-peer-reviewed whitepapers.
- Evidence Grading: Clinical statements are graded using the GRADE framework. High certainty corresponds to multiple consistent, high-impact RCTs or gold-standard meta-analyses. Moderate certainty corresponds to single high-quality RCTs or strong prospective longitudinal cohorts with minor design limitations.
¶ 12. References
¶ Update Log
¶ July 2026
- Established the comprehensive Older Adult Longevity and Functional Preservation Guide.
- Incorporated clinical evidence from 2025/2026 systematic reviews and RCTs, including the ACHIEVE hearing intervention trial and the Laromestrocel (Lomecel-B) phase 2b frailty study.
- Added 2 high-fidelity Nature-like biomedical diagrams illustrating multi-system preservation pathways and clinical decision logic.
Hernandez-Martinez J, Branco BHM, Vasquez-Carrasco E, et al. Effects of Strength Training on Body Composition, Physical Performance, and Protein or Calcium Intake in Older People with Osteosarcopenia: A Meta-Analysis. Nutrients. 2025;17(17):3204. https://pubmed.ncbi.nlm.nih.gov/40944241/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Tøien T, Berg OK, Modena R, et al. Heavy Strength Training in Older Adults: Implications for Health, Disease and Physical Performance. Journal of Cachexia, Sarcopenia and Muscle. 2025;16(2):13645. https://pubmed.ncbi.nlm.nih.gov/40241440/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sharma S, Szabo IZ, Danielsen MB, et al. Perturbation-Based Balance Training Reduces Falls and Fall Injuries in Older People: Insights on Mechanisms and Training Parameters From a Systematic Review. Journal of the American Medical Directors Association. 2026;27(1):106316. https://pubmed.ncbi.nlm.nih.gov/42391766/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Guo C, Yin L, Chen P. Effects of Multisensory Integration Training on Postural Stability Characteristics and Fall Risk in Older Adults: Systematic Review and Meta-Analysis. JMIR Aging. 2026;9:e27884. https://pubmed.ncbi.nlm.nih.gov/42096607/ ↩︎ ↩︎ ↩︎ ↩︎
Lee BC, Kim KI, Lee J, et al. Effects of resistance training on osteosarcopenia in community-dwelling postmenopausal Korean women: Randomised controlled ERTO-K trial. Experimental Gerontology. 2025;198:112450. https://pubmed.ncbi.nlm.nih.gov/40825414/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Bauer J, Biolo G, Cederholm T, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. Journal of the American Medical Directors Association. 2013;14(8):542-559. https://pubmed.ncbi.nlm.nih.gov/23867520/ ↩︎ ↩︎ ↩︎ ↩︎
Farsijani S, Payette H, Morais JA, et al. Even mealtime distribution of protein intake is associated with greater muscle strength, but not with 3-y physical function decline, in free-living older adults: the Quebec longitudinal study on Nutrition as a Determinant of Successful Aging (NuAge study). The American Journal of Clinical Nutrition. 2017;106(1):113-124. https://pubmed.ncbi.nlm.nih.gov/28515070/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Ahmadi M, Krause AJ, O'Hora KP, et al. The association between slow wave activity and memory improvement following cognitive-behavioral therapy for insomnia in older adults: A secondary analysis of a randomized clinical trial. Journal of Clinical Sleep Medicine. 2026;22(2):11244. https://pubmed.ncbi.nlm.nih.gov/42303834/ ↩︎ ↩︎ ↩︎
Lemoine P, Nir T, Laudon M, et al. Prolonged-release melatonin improves sleep quality and morning alertness in insomnia patients aged 55 years and older and has no withdrawal effects. Journal of Sleep Research. 2007;16(4):372-380. https://pubmed.ncbi.nlm.nih.gov/18036082/ ↩︎ ↩︎ ↩︎ ↩︎
Ghadimi S, Erickson AJ, Vaughan M, et al. Sleep aid usage following benzodiazepine receptor agonist tapering and cognitive behavioral therapy for insomnia in middle-aged and older adults. Journal of Clinical Sleep Medicine. 2026;22(1):11182. https://pubmed.ncbi.nlm.nih.gov/42168527/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yu L, Li B, Li N, et al. Spermidine for cognitive ageing: insights into observational and interventional studies. General Psychiatry. 2025;38(1):e101428. https://pubmed.ncbi.nlm.nih.gov/41098596/ ↩︎ ↩︎ ↩︎ ↩︎
Schwarz C, Benson GS, Horn N, et al. Effects of Spermidine Supplementation on Cognition and Biomarkers in Older Adults With Subjective Cognitive Decline: A Randomized Clinical Trial. JAMA Network Open. 2022;5(5):e2213811. https://pubmed.ncbi.nlm.nih.gov/35616942/ ↩︎
Kolykhalov IV, Androsova LV, Gavrilova SI. Clinical and immunological effects of choline alfoscerate in the treatment of amnestic type Mild Cognitive Impairment. Zhurnal nevrologii i psikhiatrii imeni S.S. Korsakova. 2022;122(11):111-118. https://pubmed.ncbi.nlm.nih.gov/36412158/ ↩︎ ↩︎ ↩︎ ↩︎
Luan T, Wang Y, Li B, et al. The effectiveness of cognitive behavioral therapy on loneliness among older adults: A systematic review and meta-analysis. Archives of Gerontology and Geriatrics. 2026;130:105642. https://pubmed.ncbi.nlm.nih.gov/41101098/ ↩︎
Kim ES, Nakamura JS, Strecher VJ, et al. Reduced Epigenetic Age in Older Adults With High Sense of Purpose in Life. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2023;78(6):glad088. https://pubmed.ncbi.nlm.nih.gov/36966357/ ↩︎ ↩︎
Cole SW, Levine ME, Arevalo JM, et al. Loneliness, eudaimonia, and the human conserved transcriptional response to adversity. Psychoneuroendocrinology. 2015;62:11-17. https://pubmed.ncbi.nlm.nih.gov/26246388/ ↩︎ ↩︎ ↩︎ ↩︎
Seppala LJ, Wermelink AMAT, de Vries M, et al. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-Analysis: II. Psychotropics. Journal of the American Medical Directors Association. 2018;19(4):337-345. https://pubmed.ncbi.nlm.nih.gov/29402652/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sheikh-Taha M. Prevalence and predictors of potentially inappropriate medication use among older adults with heart failure: a 2023 Beers Criteria-based evaluation. BMC Geriatrics. 2026;26(1):08191. https://pubmed.ncbi.nlm.nih.gov/42277692/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lin FR, Pike JR, Albert MS, et al. Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial. Lancet. 2023;402(10404):786-797. https://pubmed.ncbi.nlm.nih.gov/37467753/ ↩︎ ↩︎
Ruiz JG, Oliva AA Jr, Ramdas KN, et al. Randomized phase 2b dose-escalation trial of stem cell therapy with laromestrocel for aging frailty. Cell Stem Cell. 2026;33(2):1016. https://pubmed.ncbi.nlm.nih.gov/41747733/ ↩︎ ↩︎
Wang Y, Wang Y, Wang F, et al. Combined vitamin K(2) and D(3) therapy improves endoscopic fusion outcomes in osteoporotic lumbar degenerative disease: a prospective study. Scientific Reports. 2025;15(1):95021. https://pubmed.ncbi.nlm.nih.gov/40316739/ ↩︎ ↩︎ ↩︎
Silveira EA, Souza GVE, Rodrigues LP, et al. Effectiveness of physical exercise on osteosarcopenia in older adults: A systematic review. Geriatric Nursing. 2026;54:1016. https://pubmed.ncbi.nlm.nih.gov/41637773/ ↩︎
Baker LD, Barsness SM, Borson S, et al. Effects of growth hormone–releasing hormone on cognitive function in adults with mild cognitive impairment and healthy older adults: results of a controlled trial. Archives of Neurology. 2012;69(11):1420-1428. https://pubmed.ncbi.nlm.nih.gov/22869065/ ↩︎ ↩︎