¶ Shift Work & Jet Lag Harm Reduction Guide
This guide provides occupational health professionals, clinicians, and operators with an evidence-ranked, biologically driven roadmap to mitigate the cognitive, metabolic, and physiological degradation caused by exogenously imposed circadian mismatch.
¶ If you do only three things
- Schedule Clockwise Rotations: Ensure rotating shift rosters advance in a forward/clockwise direction (Day -> Evening -> Night) to utilize the human circadian pacemaker's natural tendency to delay.
- Implement Strategic Photic Resetting: Use bright white light (typically 3,000 to 5,000 lux) during the first half of a night shift to suppress melatonin, and shield the eyes with blue-blocking glasses during the morning post-shift commute.
- Deploy Precision Melatonin Chronotherapy: Administer low-dose exogenous melatonin (0.5 mg to 3.0 mg) 30 minutes before daytime sleep or target sleep windows to facilitate phase shifts and extend daytime sleep duration.
¶ What is actually going on
Exogenously imposed circadian mismatch occurs when there is a structural, operational, or geographic misalignment between the endogenous circadian timing system and the external environmental schedule (such as shift work hours or transmeridian travel destination times)[1]. This condition is distinct from endogenous circadian rhythm sleep-wake disorders, which are characterized by stable, intrinsic alterations in the functioning of the internal circadian timing system rather than exogenously imposed schedule shifts[1:1][2].
¶ Endogenous vs. Exogenous Circadian Disorders
Endogenous circadian rhythm sleep-wake disorders represent stable, intrinsic misalignments or dysfunction of the circadian pacemaker. Major endogenous disorders include:
- Delayed Sleep-Wake Phase Disorder (DSWPD): Characterized by an inability to fall asleep and wake up at standard societal times, with a stable phase delay of the endogenous circadian rhythm relative to desired sleep-wake times[1:2][2:1].
- Advanced Sleep-Wake Phase Disorder (ASWPD): Characterized by persistent, involuntary early-evening sleepiness and early-morning awakenings, representing a stable phase advance of the circadian pacemaker[1:3][2:2].
- Non-24-Hour Sleep-Wake Rhythm Disorder (Non-24): Also referred to as free-running disorder (FRD), this is an endogenous disorder characterized by a nonentrained circadian rhythm, which can occur in both sighted and unsighted individuals, and is managed using timed melatonin or evaluated with circadian phase markers and actigraphy[2:3]. Clinical management of Non-24, particularly in blind individuals, requires specialist clinical care to ensure proper synchronization and safety.
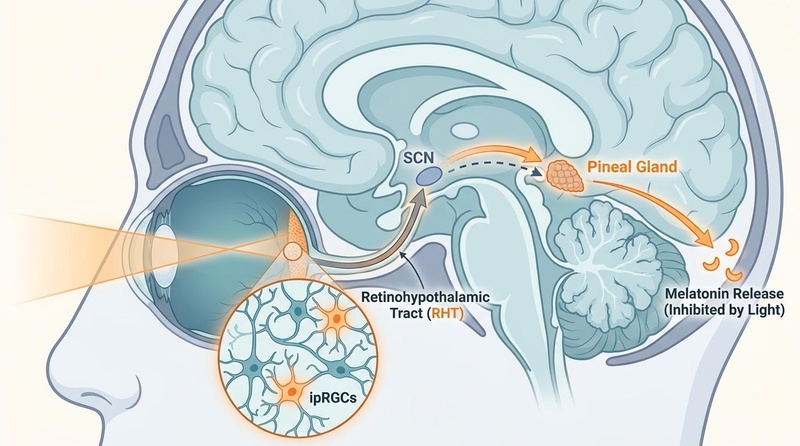
At the center of human chronobiology is the circadian pacemaker system, which regulates the timing of sleep and wakefulness[1:4]. Under natural conditions, the internal circadian timing system is synchronized (entrained) to the external 24-hour environmental light-dark cycle, with light being a key synchronizing agent[1:5][3].
Under a standard schedule, the human body exhibits endogenous circadian rhythms of melatonin secretion and core body temperature[4], as well as cortisol release[5].
Furthermore, the central pacemaker coordinates peripheral clocks located in peripheral tissues, such as peripheral blood mononuclear cells (PBMCs), which express clock genes including BMAL1, PER1, and PER2–3[6].
When an individual undergoes shift work or transmeridian travel, this hierarchical network is fractured. Working at night forces light exposure during a period when the SCN is programmed to signal melatonin synthesis and rest. Conversely, daytime sleep attempts force the body to rest when the SCN is driving cortisol release, elevated core body temperature, and sympathetic tone.
This mismatch leads to immediate sleep fragmentation, profound daytime somnolence, and cognitive decline. Over time, eating during the biological night—when glucose tolerance is naturally reduced—leads to internal circadian misalignment between central and peripheral glycemic rhythms, driving a cascade of metabolic dysregulation[7][8].
¶ Interventions ranked by evidence
| Intervention | Evidence Level | What to do | Clinical Notes & References |
|---|---|---|---|
| Exogenous Melatonin Chronotherapy | High | Administer 0.5 mg to 3.0 mg approximately 30 minutes prior to daytime sleep or targeted night sleep. | Significantly promotes circadian adaptation to shifted schedules and daytime sleep compared to placebo[4:1]; timed melatonin administration is a clinically indicated treatment option for jet lag disorder and shift work disorder[2:4]. |
| Timed Bright Light Exposure | High | Expose the retina to bright white light (typically 3,000 to 5,000 lux) during the first half of night shifts or calculated times pre-travel. | Powerful photic resetting agent; suppresses melatonin and enhances night-shift alertness[3:1][9][10]. |
| Strategic Scheduled Naps | High | Implement brief 15–30 minute preventive or operational naps during work breaks, or complete 90-minute sleep cycles. | Minimizes homeostatic sleep pressure, reduces sleepiness during shifts, and improves sleep-related performance, although short periods of sleep inertia may occur immediately post-nap[11][12][13]. |
| Strategic Caffeine Administration | High | Consume standard dietary amounts (e.g., a standard cup of coffee containing approximately 100–200 mg) at the start of night shifts or prior to peak cognitive demands. | Blocks adenosine receptors to temporarily restore psychomotor speed and vigilance[14][15]. |
| Forward/Clockwise Shift Rotation | Moderate | Structure shift patterns to rotate in a clockwise direction (Day Evening Night). | Aligns with the human circadian system's natural tendency to phase-delay[16]. |
| Retinal Light Shielding (Blue-Blocking) | Moderate | Wear blue-blocking glasses during morning post-shift commutes and maintain darkened sleep spaces. | Shielding morning light prevents unwanted circadian phase shifts and facilitates daytime sleep consolidation[3:2][9:1]. |
¶ Chronobiotic and Behavioral Protocols
¶ Schedule Design: Roster Rotation Parameters
Occupational shift schedules must be designed to align with basic biological principles of the human pacemaker. The human circadian system has a natural tendency to delay rather than advance, making it easier to adjust to a later schedule than an earlier one[16:1]. Because of this natural tendency, the biological clock is more adaptable to a phase delay (shifting sleep-wake cycles later) than to a phase advance (shifting sleep-wake cycles earlier)[16:2].
Therefore, rotating rosters must always be structured to rotate in a forward (clockwise) direction:
Rotating rosters are commonly structured to rotate in a forward (clockwise) direction (Day Evening Night), based on the human circadian system's natural tendency to phase-delay[16:3]. However, systematic clinical evidence regarding the real-world impact of rotation direction is limited. A Cochrane review found very low-certainty evidence that forward rotation did not affect sleep quality or sleep duration off-shift compared with backward rotation, though it may reduce sleepiness during shifts[17].
Two main strategies exist for scheduling night shift rosters:
- Faster Rotation: Rapidly rotating rosters involve changing shifts quickly (e.g., faster rotation schedules). Clinical evidence indicates that faster shift rotation may decrease sleepiness during shifts, though it may also reduce off-shift sleep duration, with no significant difference in off-shift sleep quality compared to slower rotations[17:1].
- Slow/Non-Shifting Rotation: In slowly rotating night shift schedules, operators remain on a night shift pattern for consecutive days. Bright light interventions are most suitable during the first three night shifts to facilitate adaptation, or a non-shifting strategy can be utilized with lower light exposure at night and daytime daylight exposure[3:3].
¶ Timed Light and Darkness: Photic Resetting
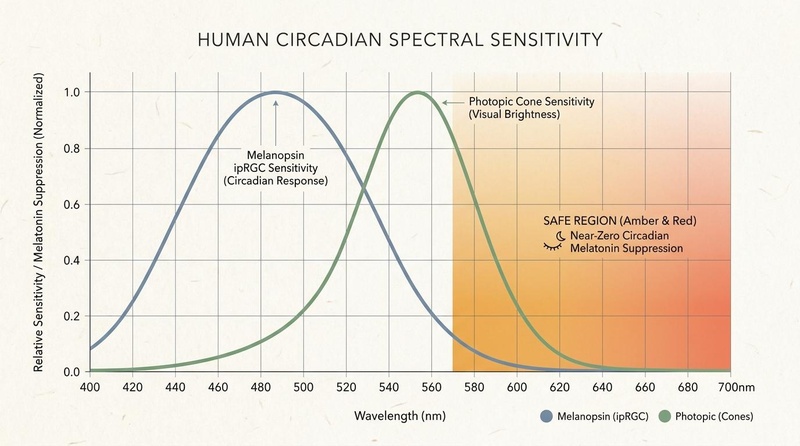
Photic resetting represents the primary non-pharmacological tool to shift circadian phase (photic entrainment). High-intensity, blue-enriched light hitting the retina stimulates melanopsin-expressing ipRGCs, sending a powerful synchronizing signal to the SCN[18].
- Shift-Work Adaptation Protocol: To shift the circadian pacemaker later (phase delay) and adapt to a permanent or semi-permanent night shift, operators should expose themselves to bright white light (typically 3,000 to 5,000 lux) during the first half of the night shift (such as between 22:00 and 02:00) as a photic resetting stimulus[3:4][9:2][10:1].
- The Morning Commute Shield: Conversely, to facilitate high-quality daytime sleep, shift workers must actively shield their eyes during the morning commute home[9:3]. Retinal exposure to bright morning sunlight stimulates ipRGCs, triggering an unwanted circadian phase advance and enhancing alertness, which can conflict with daytime sleep consolidation[3:5][9:4][18:1]. Operators can wear blue-blocking glasses during the commute to block short-wavelength light, and transition immediately to a darkened bedroom environment optimized with blackout curtains or an eye mask[3:6][9:5].
Wrong-Direction Light Risk: A critical parameter in light therapy is the timing of exposure relative to the baseline body temperature minimum, which serves as the crossover point on the light phase-response curve (PRC) between phase delays and phase advances[9:6][19]. Miscalculating the timing of light exposure can trigger a phase shift in the unintended direction, potentially worsening circadian desynchronization[9:7].
¶ Strategic Napping
Scheduled napping is a highly validated clinical and operational countermeasure to mitigate homeostatic sleep pressure during extended wakefulness or non-standard shifts[12:1].
- On-Shift/Scheduled Napping: During night shifts or work-shift hours, scheduled naps are used to restore psychomotor speed and reduce sleepiness/fatigue[11:1][12:2]. While brief naps are commonly used to mitigate alertness deficits, systematic reviews have found mixed evidence comparing brief (≤30 min), moderate (31-60 min), and long (61+ min) naps, with low overall quality of evidence for specific duration recommendations[13:1].
¶ Caffeine Timing and Pharmacokinetics
Caffeine is a powerful methylxanthine that promotes wakefulness primarily by acting as a competitive antagonist at central adenosine and receptors, thereby blocking the somnogenic effects of accumulated homeostatic sleep pressure[15:1][20].
- Dosing Parameters: For night-shift workers, caffeine may be administered in standard dietary amounts (e.g., a standard cup of coffee containing approximately 100–200 mg of caffeine) at the beginning of the shift or prior to periods requiring peak cognitive vigilance to temporarily restore psychomotor performance[14:1].
- The Sleep Interference Window: Because of caffeine's prolonged duration of action and significant pharmacokinetic variability in the human body, its consumption should be restricted prior to any planned sleep window to prevent sleep fragmentation[14:2][15:2]. Caffeine acts as a competitive antagonist at adenosine receptors, and its clearance rates are highly variable between individuals, influenced by factors such as individual metabolic rates and lifestyle habits[14:3][15:3]. Active caffeine levels during a sleep attempt can block the somnogenic effects of adenosine, preventing the consolidation of deep sleep stages and reducing overall sleep efficiency[14:4][15:4].
¶ Jet Lag Direction and Travel Planning
The physiological severity of jet lag is heavily dictated by the direction of travel, representing a distinct biological asymmetry:
- Westward Travel (Phase Delay): Traveling west requires a circadian phase delay (extending the day). Because the human circadian system has a natural tendency to delay rather than advance, phase-delaying is more easily accommodated by the SCN, making westward travel generally easier to adapt to than eastward travel[16:4].
- Eastward Travel (Phase Advance): Traveling east requires a circadian phase advance (shortening the day). Shifting sleep and wake schedules earlier runs counter to the biological clock's natural tendency to delay, making eastward travel more challenging and slower to resolve[16:5].
[ Westward Travel ] [ Eastward Travel ]
| |
v v
[ Phase Delay ] [ Phase Advance ]
| |
(Matches Natural Delay) (Opposes Natural Drift)
| |
v v
[ Faster Adaptation ] [ Slower Adaptation ]
(1.5-2.0 Zones / Day) (1.0 Zone / Day)
To minimize jet lag, travelers should deploy structured pre-travel, transit, and post-travel protocols based on their direction of travel:
¶ Eastward Travel Protocol (Phase Advance)
- Pre-travel (3 Days Prior): Gradually shift sleep and wake times 1 hour earlier each day to partially adapt the circadian phase[16:6]. This schedule shift can be paired with bright morning light exposure (continuous or intermittent bright light of >3,000 lux for 3.5 hours after waking, as studied in Burgess et al. 2003) to accelerate the endogenous phase advance[16:7]. To further facilitate the phase advance, a low dose of melatonin (0.5 mg to 3.0 mg) may be administered in the late afternoon or early evening (prior to the advanced sleep window), as supported by clinical and simulated night-work protocols[2:5][4:2].
- Transit: Avoid caffeine and heavy meals. If traveling overnight, use an eye mask, earplugs, and low-dose melatonin to maximize sleep opportunity during the flight's target sleep window.
- Post-travel (On Arrival): Seek bright natural sunlight or high-intensity artificial light in the local morning to drive the SCN phase advance. Avoid bright light in the local late afternoon and evening. Administer 1.0 to 3.0 mg of melatonin 30 minutes before the local target bedtime to promote sleep consolidation[2:6].
¶ Westward Travel Protocol (Phase Delay)
- Pre-travel (3 Days Prior): Gradually delay sleep and wake times by 1 hour per day.
- Transit: Remain awake during the local daytime hours of the destination. Seek light exposure where possible.
- Post-travel (On Arrival): Seek bright natural sunlight or high-intensity artificial light in the local evening for the first two days post-arrival to facilitate a circadian phase delay[21]. Avoid bright morning light on the first two days if waking up early. If waking up prematurely in the early morning hours, a micro-dose of melatonin (0.5 mg) can be taken to support sleep back to a local wake time.
¶ Occupational Fatigue Risk & Safety
Within professional, high-stakes environments, individual chronobiotic protocols must be integrated into systemic Fatigue Risk Management Systems (FRMS)[22]. FRMS frameworks, endorsed by organizations such as the International Civil Aviation Organization (ICAO)[22:1][23] and training programs developed by the National Institute for Occupational Safety and Health (NIOSH)[24], treat fatigue as a measurable, biological hazard that cannot be managed solely by traditional prescriptive hours-of-service regulations[22:2][23:1].
¶ Motor-Vehicle and Safety-Critical Work
Operating machinery, driving, or performing safety-critical tasks while under the influence of severe sleep deprivation poses extreme physical and operational hazards[1:6][10:2][25][26]. Sleep deprivation and circadian misalignment lead to complaints of excessive daytime sleepiness, insomnia, and profound impairment in daytime functioning, including cognitive performance, vigilance, and reaction time[1:7][3:7][10:3].
Empirical studies evaluating performance degradation demonstrate a stark equivalence between prolonged wakefulness and Blood Alcohol Content (BAC) metrics:
- 17 to 19 hours of continuous wakefulness produces cognitive and psychomotor deficits equivalent to a 0.05% BAC[25:1][26:1].
- 24 hours of continuous wakefulness produces deficits equivalent to a 0.10% BAC[25:2][26:2], which exceeds the legal limit for motor-vehicle operation in almost all developed jurisdictions.
Hours Awake Equivalent Blood Alcohol Content (BAC)
=========== ======================================
17-19 hours --> [======== 0.05% BAC ========]
24 hours --> [============ 0.10% BAC ============] (Legally Impaired)
To eliminate the extreme hazard of the morning post-shift commute, occupational safety guidelines recommend these operational alternatives:
- Mandatory Post-Shift Napping: Establish designated, quiet rest areas within industrial facilities where night-shift workers must take a scheduled 20-minute nap prior to commuting home.
- Rideshare and Shuttle Utilization: Implement company-sponsored transit, rideshare credits, or public transportation alternatives to prevent fatigued workers from operating personal motor vehicles.
- Strategic Shift Limitations: Cap continuous safety-critical work shifts at 12 hours, ensuring a minimum of 11 consecutive hours of rest between shifts to facilitate recovery.
¶ Off-Label Stimulant Use & Clinical Evidence
Prescription-only wakefulness-promoting agents (such as modafinil and armodafinil) are occasionally evaluated for the clinical management of diagnosed Shift Work Sleep Disorder (SWSD) with severe impairment[2:7].
In clinical parameters, these agents have been shown to reduce sleepiness and improve alertness in patients with SWSD, but they are associated with notable adverse effects, including headache, nausea, and elevated blood pressure[27]. Crucially, there is a lack of randomized controlled trials evaluating the safety and efficacy of these substances in healthy shift workers who do not have a clinical diagnosis of SWSD (i.e., off-label self-medication)[27:1].
Due to the potential for adverse cardiovascular and neurological effects, along with the absence of safety data in non-clinical cohorts, off-label self-medication with these agents is not recommended as a standard harm-reduction strategy[27:2]. Additionally, operators and clinicians must note:
- No Replacement for Biological Sleep: Wakefulness-promoting agents do not clear homeostatic sleep debt or restore the essential restorative functions of biological sleep; they merely mask the perception of fatigue, leaving the brain vulnerable to sudden cognitive lapses when the drug's effects wane.
- Cardiovascular and Autonomic Stress: These compounds can lead to adverse effects including headache, nausea, and a rise in blood pressure[27:3].
- Overconfidence Bias: Stimulants can induce a false sense of cognitive competence, leading operators to overestimate their actual physical and psychomotor performance, thereby increasing operational risk in safety-critical roles.
- Dependency and Tolerance: Chronic, unmonitored use carries a risk of psychological dependence, tolerance, and subsequent withdrawal-induced hypersomnia.
Behavioral, environmental, and chronobiotic protocols (such as timed light, dark, strategic naps, and schedule design) must always serve as the primary, non-pharmacological foundation of circadian mismatch management[1:8][17:2].
¶ Cardiometabolic and Cancer Associations
When evaluating the long-term health consequences of chronic shift work and circadian disruption, it is clinically critical to maintain a rigorous distinction between statistical association and direct causation.
¶ Oncological Associations (IARC Group 2A)
In 2019, the International Agency for Research on Cancer (IARC) re-evaluated the scientific literature regarding night shift work and classified it as Group 2A: "probably carcinogenic to humans"[28].
- The Evidence Base: This classification is characterized by limited evidence of carcinogenicity in humans derived from epidemiological studies (including case-control and cohort designs observing a higher incidence of breast cancer in long-term night-shift workers)[28:1][29]. Conversely, there is sufficient evidence of carcinogenicity in experimental animal models and strong mechanistic evidence in experimental animals[28:2]. In controlled animal models, chronic, forced phase shifts and disrupted light-dark cycles have demonstrated sufficient evidence of carcinogenicity and strong mechanistic support, which forms the biological basis of the Group 2A classification[28:3].
- Causation vs. Association: The link in humans remains an association. Night shift work is inherently confounded by lifestyle factors that are difficult to isolate in epidemiological cohorts, including altered dietary patterns, elevated alcohol consumption, chronic physical inactivity, socioeconomic variables, and reduced systemic Vitamin D status from limited daylight exposure. Circadian disruption itself is a major physiological stressor, but it has not been proven to be an independent, direct carcinogen in humans.
¶ Cardiometabolic Pathways
Long-term circadian misalignment is strongly associated with an elevated incidence of metabolic syndrome, cardiovascular disease, type 2 diabetes, and visceral obesity[30], as well as alterations in blood pressure regulation[31]. However, this relationship is highly complex, multi-factorial, and bi-directional:
- Endocrine Mismatch: Eating during the biological night occurs when the body's glycemic control is naturally reduced[8:1]. This mismatch leads to impaired glucose tolerance, which is mediated by decreased pancreatic -cell function (decreased early-phase insulin) in the biological evening, and reduced insulin sensitivity during circadian misalignment[7:1][8:2]. These effects result in internal circadian misalignment between the central body temperature rhythm and peripheral glucose rhythms[7:2].
- Confounding Variables: The association with chronic cardiometabolic disease is heavily confounded by a cluster of secondary, lifestyle-mediated factors:
- Altered Eating Patterns: Eating during the nighttime shift instead of the daytime leads to circadian misalignment of glucose tolerance[7:3]. Restricting meals to the daytime has been shown to prevent this internal circadian misalignment and glucose intolerance in simulated night work[7:4].
- Sedentary Behavior: Working non-standard hours severely limits opportunities for structured physical training and Zone 2 cardiovascular exercise, compounding metabolic stasis.
- Blood Pressure and Cardiovascular Risk: Exposure to night shift work can alter normal circadian patterns of blood pressure (BP) and heart rate variability (HRV), which is hypothesized to contribute to cardiovascular disease risk[32]. Ambulatory blood pressure monitoring of night shift workers shows that the natural drop (dipping) of blood pressure during daytime sleep is frequently blunted, but taking a scheduled nap of 60 minutes or longer during the night shift is associated with a healthier blood pressure dipping pattern during sleep[33].
- Chronic Psychosocial Stress: The chronic mismatch between an operator's schedule and the diurnal schedule of their social and family network increases psychological strain, further driving chronic hypothalamic-pituitary-adrenal (HPA) axis activation and elevated cortisol.
¶ What to do this week
To systematically implement a harm-reduction protocol for shift work or upcoming transmeridian travel, follow these actionable steps:
- Audit Your Circadian Schedule: Map out your upcoming shift roster or flight itinerary. Note the exact direction of shift rotation (ensure it is clockwise) or the number of time zones to be crossed.
- Optimize Your Sleep Sanctuary: Install heavy blackout curtains in your bedroom to achieve absolute, near-zero lux darkness. Ensure you have orange-tinted blue-blocking glasses available for the morning commute or late-evening pre-travel windows.
- Establish Your Chronobiotic Protocol: Source high-quality, third-party tested low-dose melatonin (0.5 mg to 1.0 mg). Calculate the exact timing of administration (30 minutes before your planned daytime sleep or target destination bedtime) and bright light exposure windows (during the first half of night shifts or calculated morning windows)[2:8][9:8].
¶ Safety and when to get help
¶ Clinical Contraindications and Pharmacological Interactions
While behavioral and chronobiotic interventions are highly effective, they carry critical physiological parameters and contraindications that must be clinically managed:
-
Exogenous Melatonin: Exogenous melatonin administration is a potent chronobiotic intervention, but its use requires careful clinical oversight. Although generally well-tolerated, individuals taking concomitant prescription medications (including anticoagulants, oral hypoglycemics, immunosuppressants, or anticonvulsants) should exercise caution due to potential drug-hormone interactions and individual variability in clearance and glycemic response. For a comprehensive, detailed review of specific clinical contraindications, safety profiles, and metabolic interactions, refer to Melatonin, Sleep, and Circadian/Light Contraindications.
-
Bright Light Therapy: While bright light phototherapy is a standard treatment, its use requires caution. Phototherapy is potentially contraindicated or dangerous if associated with tricyclic antidepressants, neuroleptics, or other medications containing a tricyclic, heterocyclic, or porphyrin ring system due to potential ocular phototoxicity concerns[34].
-
Clinical Screening and Referral: If an operator or traveler exhibits persistent, severe daytime somnolence, cognitive lapses, or sleep fragmentation that fails to resolve with structured environmental and chronobiotic optimization, they should undergo formal clinical screening. Persisting deficits may indicate an underlying primary sleep disorder, which may require polysomnography to rule out other diagnoses[2:9]. Clinical screening for persistent insomnia or sleep disturbances must actively screen out untreated obstructive sleep apnea (OSA), bipolar mania risk, dangerous daytime sleepiness/driving, and suicidality to ensure patient safety before initiating sleep interventions.
Formal clinical evaluation is recommended when sleep disturbances or daytime sleepiness persist, in order to rule out other primary sleep disorders and systematically guide therapy[2:10].
¶ Next step
To expand your understanding of sleep physiology and environmental optimization, explore these related resources:
- Review the foundational biology of sleep architecture in Sleep Optimization.
- Explore a complete analysis of light-induced endocrine pathways and safety parameters in Melatonin, Sleep, and Circadian/Light Contraindications.
- For an advanced deep dive into industrial shift-work chronobiology and adaptive lighting, read Shift Work Sleep Disorder & Chronobiotic Protocols.
¶ How we review this
Longevipedia pages are AI-updated and human-reviewed. We prioritize human evidence, cite claims, and update pages when the evidence changes.
¶ References
Reid KJ, Zee PC. Circadian rhythm disorders. Seminars in neurology. 2004;24(3):213-225. https://pubmed.ncbi.nlm.nih.gov/15449224/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Morgenthaler TI, Lee-Chiong T, Alessi C. Practice parameters for the clinical evaluation and treatment of circadian rhythm sleep disorders. An American Academy of Sleep Medicine report. Sleep. 2007;30(11):1445-1459. https://pubmed.ncbi.nlm.nih.gov/18041479/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lowden A, Öztürk G, Reynolds A. Working Time Society consensus statements: Evidence based interventions using light to improve circadian adaptation to working hours. Industrial health. 2019;57(2):202-211. https://pubmed.ncbi.nlm.nih.gov/30700675/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sharkey KM, Eastman CI. Melatonin phase shifts human circadian rhythms in a placebo-controlled simulated night-work study. American journal of physiology. Regulatory, integrative and comparative physiology. 2002;282(2):R454-R463. https://pubmed.ncbi.nlm.nih.gov/11792655/ ↩︎ ↩︎ ↩︎
Facer-Childs ER, Middleton B, Skene DJ. Resetting the late timing of 'night owls' has a positive impact on mental health and performance. Sleep medicine. 2019;60:236-247. https://pubmed.ncbi.nlm.nih.gov/31202686/ ↩︎
Cuesta M, Cermakian N, Boivin DB. Glucocorticoids entrain molecular clock components in human peripheral cells. FASEB journal : official publication of the Federation of American Societies for Experimental Biology. 2015;29(4):1556-1564. https://pubmed.ncbi.nlm.nih.gov/25500935/ ↩︎
Chellappa SL, Qian J, Vujovic N. Daytime eating prevents internal circadian misalignment and glucose intolerance in night work. Science advances. 2021;7(49):eabg9910. https://pubmed.ncbi.nlm.nih.gov/34860550/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Morris CJ, Yang JN, Garcia JI. Endogenous circadian system and circadian misalignment impact glucose tolerance via separate mechanisms in humans. Proceedings of the National Academy of Sciences of the United States of America. 2015;112(17):E2225-E2234. https://pubmed.ncbi.nlm.nih.gov/25870289/ ↩︎ ↩︎ ↩︎
Eastman CI, Martin SK. How to use light and dark to produce circadian adaptation to night shift work. Annals of medicine. 1999;31(2):109-118. https://pubmed.ncbi.nlm.nih.gov/10344580/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kelly TL, Kripke DF, Hayduk R. Bright light and LEET effects on circadian rhythms, sleep and cognitive performance. Stress medicine. 1997;13(4):251-258. https://pubmed.ncbi.nlm.nih.gov/11542396/ ↩︎ ↩︎ ↩︎ ↩︎
Martin-Gill C, Barger LK, Moore CG. Effects of Napping During Shift Work on Sleepiness and Performance in Emergency Medical Services Personnel and Similar Shift Workers: A Systematic Review and Meta-Analysis. Prehospital emergency care. 2018;22(3):397-406. https://pubmed.ncbi.nlm.nih.gov/29324083/ ↩︎ ↩︎
Ruggiero JS, Redeker NS. Effects of napping on sleepiness and sleep-related performance deficits in night-shift workers: a systematic review. Biological research for nursing. 2014;16(2):137-149. https://pubmed.ncbi.nlm.nih.gov/23411360/ ↩︎ ↩︎ ↩︎
Patterson PD, Liszka MK, Mcilvaine QS. Does the evidence support brief (≤30-mins), moderate (31-60-mins), or long duration naps (61+ mins) on the night shift? A systematic review. Sleep medicine reviews. 2021;57:101436. https://pubmed.ncbi.nlm.nih.gov/34116386/ ↩︎ ↩︎
Temple JL, Hostler D, Martin-Gill C. Systematic Review and Meta-analysis of the Effects of Caffeine in Fatigued Shift Workers: Implications for Emergency Medical Services Personnel. Prehospital emergency care. 2018;22(3):387-396. https://pubmed.ncbi.nlm.nih.gov/29324066/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pohanka M. The perspective of caffeine and caffeine derived compounds in therapy. Bratislavske lekarske listy. 2015;116(8):487-493. https://pubmed.ncbi.nlm.nih.gov/26435014/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Burgess HJ, Crowley SJ, Gazda CJ. Preflight adjustment to eastward travel: 3 days of advancing sleep with and without morning bright light. Journal of biological rhythms. 2003;18(4):318-328. https://pubmed.ncbi.nlm.nih.gov/12932084/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hulsegge G, Coenen P, Gascon GM. Adapting shift work schedules for sleep quality, sleep duration, and sleepiness in shift workers. The Cochrane database of systematic reviews. 2023;9:CD010637. https://pubmed.ncbi.nlm.nih.gov/37694838/ ↩︎ ↩︎ ↩︎
David J. Ramsey, Kathryn Moynihan Ramsey, Demetrios G. Vavvas. Genetic Advances in Ophthalmology: The Role of Melanopsin-Expressing, Intrinsically Photosensitive Retinal Ganglion Cells in the Circadian Organization of the Visual System. Seminars in Ophthalmology. 2013;28(5-6):406-421. https://pubmed.ncbi.nlm.nih.gov/24010846/ ↩︎ ↩︎
Mitchell PJ, Hoese EK, Liu L. Conflicting bright light exposure during night shifts impedes circadian adaptation. Journal of biological rhythms. 1997;12(1):5-15. https://pubmed.ncbi.nlm.nih.gov/9104686/ ↩︎
Anas Sohail A, Ortiz F, Varghese T. The Cognitive-Enhancing Outcomes of Caffeine and L-theanine: A Systematic Review. Cureus. 2021;13(12):e20804. https://pubmed.ncbi.nlm.nih.gov/35111479/ ↩︎
Boulos Z, Macchi MM, Stürchler MP. Light visor treatment for jet lag after westward travel across six time zones. Aviation, space, and environmental medicine. 2002;73(10):953-961. https://pubmed.ncbi.nlm.nih.gov/12398256/ ↩︎
Gander P, Hartley L, Powell D. Fatigue risk management: Organizational factors at the regulatory and industry/company level. Accident; analysis and prevention. 2011;43(2):498-506. https://pubmed.ncbi.nlm.nih.gov/21130218/ ↩︎ ↩︎ ↩︎
Li WC, Kearney P, Zhang J. The Analysis of Occurrences Associated with Air Traffic Volume and Air Traffic Controllers' Alertness for Fatigue Risk Management. Risk analysis : an official publication of the Society for Risk Analysis. 2021;41(6):962-972. https://pubmed.ncbi.nlm.nih.gov/32920882/ ↩︎ ↩︎
James L, Caruso CC, James S. Pilot Test of "NIOSH Training for Law Enforcement on Shift Work and Long Work Hours". Journal of occupational and environmental medicine. 2022;64(6):455-462. https://pubmed.ncbi.nlm.nih.gov/35543640/ ↩︎
Dawson D, Reid K. Fatigue, alcohol and performance impairment. Nature. 1997;388(6639):235. https://pubmed.ncbi.nlm.nih.gov/9230429/ ↩︎ ↩︎ ↩︎
Williamson AM, Feyer AM. Moderate sleep deprivation produces impairments in cognitive and motor performance equivalent to legally prescribed levels of alcohol intoxication. Occupational and environmental medicine. 2000;57(10):649-655. https://pubmed.ncbi.nlm.nih.gov/10984335/ ↩︎ ↩︎ ↩︎
Liira J, Verbeek JH, Costa G. Pharmacological interventions for sleepiness and sleep disturbances caused by shift work. The Cochrane database of systematic reviews. 2014;8:CD009796. https://pubmed.ncbi.nlm.nih.gov/25113164/ ↩︎ ↩︎ ↩︎ ↩︎
Erren TC, Morfeld P, Groß JV. IARC 2019: "Night shift work" is probably carcinogenic: What about disturbed chronobiology in all walks of life? Journal of occupational medicine and toxicology. 2019;14:29. https://pubmed.ncbi.nlm.nih.gov/31798667/ ↩︎ ↩︎ ↩︎ ↩︎
Szkiela M, Kusideł E, Makowiec-Dąbrowska T. How the Intensity of Night Shift Work Affects Breast Cancer Risk. International journal of environmental research and public health. 2021;18(9):4812. https://pubmed.ncbi.nlm.nih.gov/33925799/ ↩︎
Moreno CRC, Marqueze EC, Sargent C. Working Time Society consensus statements: Evidence-based effects of shift work on physical and mental health. Industrial health. 2019;57(2):139-157. https://pubmed.ncbi.nlm.nih.gov/30700667/ ↩︎
Patterson PD, Mountz KA, Budd CT. Impact of shift work on blood pressure among emergency medical services clinicians and related shift workers: A systematic review and meta-analysis. Sleep health. 2020;6(3):387-398. https://pubmed.ncbi.nlm.nih.gov/32354630/ ↩︎
Patterson PD, Weiss LS, Weaver MD. Napping on the night shift and its impact on blood pressure and heart rate variability among emergency medical services workers: study protocol for a randomized crossover trial. Trials. 2021;22(1):210. https://pubmed.ncbi.nlm.nih.gov/33726840/ ↩︎
Patterson PD, Mountz KA, Agostinelli MG. Ambulatory blood pressure monitoring among emergency medical services night shift workers. Occupational and environmental medicine. 2021;78(1):51-57. https://pubmed.ncbi.nlm.nih.gov/32847989/ ↩︎
Sartori S, Poirrier R. [Seasonal affective syndrome and phototherapy: theoretical concepts and clinical applications]. L'Encephale. 1996;22(1):33-38. https://pubmed.ncbi.nlm.nih.gov/8681879/ ↩︎