¶ Atopic Dermatitis
| Indication | Chronic, relapsing, pruritic inflammatory skin disease (Atopic Eczema) [^16] |
| Access | OTC (barrier care) / Prescription (TCS, TCIs, PDE4i, biologics, oral JAKi) [^1][^2][^3] |
| Dosing Sched | Continuous daily barrier care; proactive or episodic reactive anti-inflammatory therapy [^2][^7][^11] |
| Safety Profile | Moderate (High for emollients/biologics; Moderate for chronic high-potency TCS and oral JAKi) [^2][^3][^18] |
| Key Marker | EASI, SCORAD (clinically rated severity indices) [^29][^37] |
| Est. Cost | Varies widely (OTC moisturizers to premium biologics/JAKi) |
Atopic dermatitis (AD) is a chronic, systemic inflammatory skin disorder that is highly prevalent globally [1]. It is driven by a complex interplay of epidermal barrier collapse (often involving FLG gene mutations) and type 2 helper T-cell-mediated (Th2) immune activation [2][3][4]. Effective management requires a dual approach that pairs daily mechanical skin barrier repair with targeted anti-inflammatory and immunomodulatory interventions to control both localized skin lesions and systemic inflammation [5][6][7].
¶ At a glance
¶ Key points
- Strongest Benefit: Core topicals (topical corticosteroids and topical calcineurin inhibitors) and systemic therapies (such as dupilumab) provide highly effective skin clearance and rapid pruritus reduction in mild-to-severe disease [5:1][8][9].
- Key Limitation or Risk: Improper long-term use of high-potency topical corticosteroids carries significant risk of skin atrophy and Topical Steroid Withdrawal (TSW) [10]. Systemic oral Janus kinase (JAK) inhibitors carry class-wide regulatory warnings for major adverse cardiovascular events (MACE), venous thromboembolism (VTE), and serious infections, though short-term clinical trials evaluated in systematic reviews did not demonstrate statistically significant increases in these events (while showing significant increases in Herpes Zoster, acne, headache, elevated blood creatinine phosphokinase, and nausea) [11].
- Verdict: Modern, evidence-based management of atopic dermatitis relies on a structured step-up and step-down treatment approach, using ceramide-dominant emollients as baseline therapy, transitioning to proactive topical anti-inflammatories, and escalating to targeted biologics or JAK inhibitors for moderate-to-severe disease [6:1][7:1][12].
¶ What people use it for
- Primary Goals: Restoring skin barrier integrity, reducing intense itch (pruritus), eliminating eczematous skin lesions, preventing flares, and improving overall health-related quality of life [5:2][6:2][7:2].
- Evidence Quality (Overall): High [5:3][6:3][7:3][8:1].
¶ Safety "Traffic Light"
CRITICAL CLINICAL ALERTS & CONTRAINDICATIONS
- RED (STOP): Do not use high-dose systemic oral corticosteroids (e.g., prednisone) for the routine management of chronic flares. Systemic steroids are associated with severe, rebound flares upon discontinuation, adrenal suppression, and long-term metabolic or bone toxicities [7:4][13]. Oral JAK inhibitors carry class-wide regulatory warnings and are generally avoided in patients with high baseline risk for major adverse cardiovascular events (MACE), venous thromboembolism (VTE), active serious infections, or malignancy [11:1]. Note that while these represent class-wide regulatory alerts, the short-term trials analyzed in [11:2] did not show statistically significant increases in VTE, MACE, or serious infections (other than Herpes Zoster).
- YELLOW (CAUTION): Limit continuous daily use of high-potency topical corticosteroids (TCS) to active lesions to prevent skin atrophy, striae, and Topical Steroid Withdrawal (TSW) [10:1]. Ensure patients are informed that topical calcineurin inhibitors (TCIs) can cause a transient, self-limiting localized burning sensation during the initial period of treatment as a matter of general clinical experience.
- GREEN (GO): Daily application of ceramide-dominant barrier repair emollients is highly safe, prolongs the interval between flares, and significantly decreases the cumulative need for prescription anti-inflammatory medications [6:4][14][15][16]. Monoclonal antibodies targeting interleukin-4 receptor alpha (IL-4Rα; dupilumab) or interleukin-13 (IL-13; lebrikizumab) are safe for long-term continuous use and do not require routine laboratory monitoring [7:5][12:1][9:1]. While dupilumab has demonstrated a favorable safety profile during pregnancy based on clinical registry data [17], lebrikizumab currently lacks similar published pregnancy registry data in the cited systematic review.
¶ What is it?
¶ Quick Answer
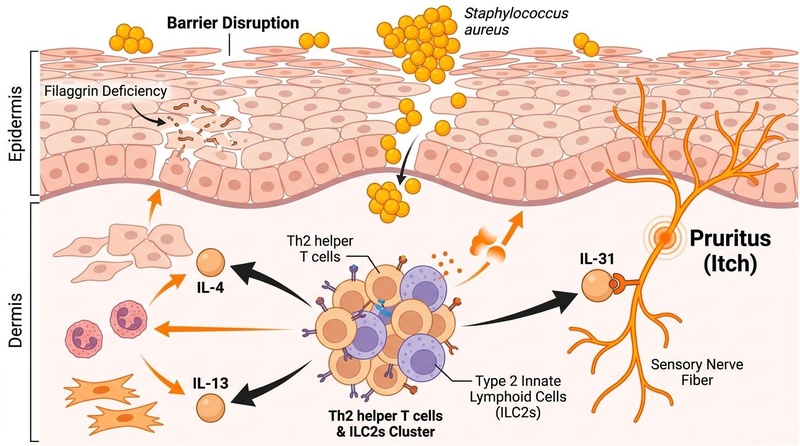
Atopic dermatitis is a chronic, relapsing, pruritic inflammatory dermatosis characterized by physical barrier disruption and immune dysregulation [18][15:1]. The condition is not simply dry skin; it is driven by a genetically or environmentally compromised epidermal barrier that allows environmental allergens and pathogens (specifically Staphylococcus aureus) to penetrate the epidermis [18:1][19]. This barrier breach activates an overactive Th2-skewed immune cascade, which releases cytokines such as IL-4, IL-13, and IL-31 [8:2]. These cytokines further damage the barrier and directly stimulate slow-conducting sensory nerve fibers, establishing a self-perpetuating itch-scratch cycle [15:2][20].
¶ Pediatric vs. Adult Presentation
The clinical morphology and anatomical distribution of atopic dermatitis evolve characteristically across age brackets, dictating age-specific diagnostic and therapeutic approaches [21][16:1]:
- Infantile Bracket (Birth to 2 Years): Typically presents with erythematous papules, patches, or plaques on the face (especially the cheeks), scalp, trunk, and extensor surfaces of the limbs. The groin and axillary regions (diaper area) are characteristically spared [21:1][16:2].
- Childhood Bracket (2 to 12 Years): Typically presents with patches and plaques on the flexural surfaces, wrists, and ankles, where subacute or chronic lesions develop prominently [21:2][16:3].
- Adolescent & Adult Bracket (12 Years to Adulthood): Characterized by dry, scaly patches on the extremities, face, neck, and hands [21:3][16:4]. Chronic hand eczema is a highly prevalent and debilitating adult presentation [22].
¶ Skin of Color (SOC) Considerations
Clinical presentation can vary significantly across different skin tones, which can lead to diagnostic challenges or undertreatment [23].
- Erythema Presentation: Erythema (classic redness) can be masked by baseline melanin, presenting instead as darker brown, grey, violaceous, or hyperpigmented areas. Assessors are advised to evaluate secondary signs such as scaling, infiltration, induration, and cutaneous warmth to gauge disease severity [23:1].
- Atypical Morphological Patterns: Atypical clinical presentations can occur in patients with darker skin tones, including papular patterns and lichenified presentations [23:2], and perifollicular accentuation [21:4].
- Post-Inflammatory Pigmentary Changes: Post-inflammatory hyperpigmentation (PIH) and hypopigmentation are common sequelae of cutaneous inflammation, which may cause significant distress and require early, effective control of active eczema lesions [23:3].
¶ Diagnostic Differentiation
To ensure safe and effective therapy, clinicians must distinguish atopic dermatitis from other inflammatory dermatoses and infectious mimics:
| Condition | Primary Morphology & Features | Key Diagnostic Clues | Distinguishing Pathology |
|---|---|---|---|
| Atopic Dermatitis (AD) [18:2] | Pruritic, ill-defined erythematous plaques; age-dependent flexural distribution; lichenification. | Personal or family history of atopy (asthma, allergic rhinitis); highly chronic and relapsing. | Filaggrin deficiency, Th2 cytokine-driven (IL-4/IL-13) inflammation, high IgE [2:1][3:1]. It represents an advanced state of skin barrier dysfunction. |
| Allergic Contact Dermatitis (ACD) [21:5][24] | Acute, vesicular, highly localized pruritic lesions matching the shape/contact area of an allergen. | Direct exposure history; positive patch testing; sharp margins corresponding to external objects [25]. | T-cell-mediated delayed-type (Type IV) hypersensitivity reaction triggered by low-molecular-weight electrophilic chemicals or metals called haptens (e.g., nickel, fragrances, preservatives) binding to endogenous skin proteins to form immunogenic complexes [24:1]. |
| Irritant Contact Dermatitis (ICD) [26][27] | Dry, chapped, burning, painful erythema; localized primarily to hands or exposed areas. | Exposure to harsh soaps, solvents, or friction; immediate onset, limited to exposure area [26:1][27:1]. | Non-immunological physical or chemical epidermal barrier damage (no sensitization), causing cellular damage and release of pro-inflammatory cytokines [26:2][28]. |
| Seborrheic Dermatitis [18:3] | Greasy, yellowish, well-demarcated scales over pink-to-red patches. | Restricts to areas of high sebum density (scalp, eyebrows, nasolabial folds, chest). | Inflammatory response to commensal yeast Malassezia feeding on scalp sebum. For a complete clinical guide, see Scalp Health and Seborrheic Dermatitis. |
See also Redness, Rosacea, and Broken Capillaries for vascular components of chronic facial dermatoses.
¶ Diagnosis and Severity Assessment
Atopic dermatitis is diagnosed clinically; there are no diagnostic laboratory tests. Clinicians rely on standardized, validated diagnostic criteria and severity grading scales:
- Hanifin and Rajka Criteria: A comprehensive, traditional clinical diagnostic framework that relies on identifying major clinical features (such as pruritus, typical morphology and distribution, and personal/family history of atopy) alongside a variety of minor criteria [21:6][29].
- UK Working Party Diagnostic Criteria: A simplified, highly practical clinical tool that bases diagnosis on the presence of an itchy skin condition combined with a combination of supportive historical and physical findings [21:7][29:1].
- Severity Grading Scales:
- EASI (Eczema Area and Severity Index): An objective, clinician-rated instrument assessing the overall extent and severity of eczema signs across body regions [7:6][30].
- SCORAD (SCORing Atopic Dermatitis): An instrument that combines objective assessments of lesion extent and severity with subjective patient-reported symptoms like sleep loss and pruritus [7:7][30:1].
- POEM (Patient-Oriented Eczema Measure): A subjective patient questionnaire measuring the frequency of key symptoms over the past week [31][32].
- DLQI (Dermatology Life Quality Index): A questionnaire measuring the impact of skin disease on the patient's daily activities, relationships, and quality of life [31:1][32:1].
¶ Veterinary Medicine and Comparative Atopic Disease
Atopic dermatitis is also a highly prevalent and well-characterized condition in veterinary medicine, particularly in canine and feline populations [33][34]. Comparative clinical guidelines, such as those from the American Animal Hospital Association (AAHA) and the International Committee on Allergic Diseases of Animals (ICADA), emphasize that—similar to humans—veterinary management of chronic atopic skin disease requires a multimodal approach [33:1][34:1]. This includes maintaining skin barrier hygiene through mild therapeutic bathing, using essential fatty acids to support lipid barriers, and employing targeted immunomodulatory agents (such as glucocorticoids, ciclosporin, or oclacitinib) to control chronic pruritus and inflammatory skin lesions [33:2][34:2].
¶ Clinical Benefits
Modern clinical management of atopic dermatitis aims to systematically restore the skin barrier, interrupt the Th2-mediated neuroimmune itch cascade, and clear inflammatory skin lesions [5:4][6:5][7:8]. Utilizing highly targeted biologics (such as dupilumab) or advanced topicals can achieve significant skin clearance (such as achieving a 75% or greater reduction in Eczema Area and Severity Index, or EASI-75, in a large majority of patients) while demonstrating safety profiles that allow for long-term maintenance [5:5][7:9][8:3][9:2].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence Quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Emollients (Ceramide-dominant) | High | High | Multi-center trials | Applied daily as baseline therapy across all age brackets [6:6][14:1][15:3]. | |
| Topical Corticosteroids (TCS) | High | High | RCTs | Standard first-line reactive therapy; potency matched to site; episodic use as directed [5:6][6:7][14:2]. | |
| Topical Calcineurin Inhibitors (TCI) | High | High | Multiple large RCTs | Gold standard for proactive maintenance and sensitive areas (tacrolimus/pimecrolimus) [5:7][6:8][15:4]. | |
| Topical PDE4 Inhibitors | High | Moderate | Phase III RCTs | Crisaborole 2% ointment; useful for mild-to-moderate AD in adults and pediatric patients [5:8][6:9]. | |
| Topical JAK Inhibitors | High | High | Large Phase III RCTs | Ruxolitinib 1.5% cream; provides rapid itch relief and superior clearance [5:9][6:10]. | |
| Biologics (IL-4Rα/IL-13 Inhibitors) | High | High | Multiple pivotal trials | Dupilumab, lebrikizumab, tralokinumab; safe long-term, achieves EASI-75 in a large majority of patients [7:10][8:4][32:2][9:3]. | |
| Oral JAK Inhibitors | High | High | Multiple head-to-head RCTs | Upadacitinib, abrocitinib; fastest skin clearance but requires baseline and periodic laboratory monitoring [7:11][8:5][11:3]. | |
| Phototherapy (Narrowband UVB) | Moderate | Moderate | Clinical cohorts | 2–3 sessions per week; effective adjunctive therapy for moderate-to-severe disease [7:12][13:1]. | |
| Vitamin D Supplementation | Moderate | Moderate | RCTs | Vitamin D supplementation significantly reduces atopic dermatitis severity scores (SCORAD/EASI) [35]. | |
| Dietary Elimination Diets | Moderate | Low | RCTs | May lead to slight, potentially unimportant improvements in mild-to-moderate disease, but lacks high-certainty evidence and is not routinely recommended [6:11][36]. |
*Effect magnitude: Arrow count (1-3) indicates magnitude. Direction: u (↑ increase), d (↓ decrease), e (= no effect), q (? unclear). Impact: p (positive), n (negative), x (neutral/unknown).
¶ Mechanisms
The pathogenesis of atopic dermatitis is characterized by three overlapping biological pathways:
+-----------------------------------+
| Physical Barrier Disruption |
| - Filaggrin (FLG) deficiency |
| - Elevated pH & lipid depletion |
+-----------------+-----------------+
|
| (Allergen & S. aureus entry)
v
+-----------------------------------+
| Innate Alarmin Release |
| - TSLP, IL-25, IL-33 |
+-----------------+-----------------+
|
| (Dendritic cell activation)
v
+-----------------------------------+
| Adaptive Th2 Immune Response |
| - Cytokines: IL-4, IL-13, IL-31 |
+-----------------+-----------------+
|
+-----------------+-----------------+
| |
v v
+---------------------------+ +---------------------------+
| Further Barrier Injury | | Sensory C-Nerve Itch |
| - Downregulates FLG | | - Direct IL-31 binding |
| - Inhibits antimicrobial | | - Triggers TRPV1 |
| host peptides | | - Drives "Itch-Scratch" |
+---------------------------+ +---------------------------+
¶ 1. Epidermal Barrier Dysfunction and the Filaggrin Pathway
The stratum corneum acts as the skin’s primary physical and chemical shield, constructed of keratinocytes ("bricks") embedded in a highly organized lipid matrix ("mortar") composed of ceramides, cholesterol, and free fatty acids.
- Filaggrin (FLG) Loss-of-Function: Filaggrin is a critical structural protein that aggregates keratin filaments to flatten and structurally reinforce keratinocytes. Atopic dermatitis is characterized by a genetically or environmentally compromised epidermal barrier and skin barrier defects [37].
- Natural Moisturizing Factors (NMF) Depletion: Filaggrin is proteolytically degraded into amino acids (including histidine and glutamic acid) that constitute NMF. NMF binds water within the cells, maintaining skin hydration and an acidic pH (~4.5–5.5). Reduced NMF leads to skin dryness (xerosis) and elevations in skin pH.
- Enzymatic Disruption: The elevated pH activates endogenous serine proteases (kallikreins) while inhibiting enzymes responsible for lipid synthesis. This leads to premature shedding of keratinocytes and a depleted, disorganized lipid mortar, creating physical micro-cracks in the skin barrier.
¶ 2. The Innate and Th2 Immune Cascades
When the physical barrier is breached, environmental allergens, irritants, and pathogens penetrate into the epidermal layer.
- Alarmin Release: Damaged keratinocytes release innate alarm signals (alarmins), including Thymic Stromal Lymphopoietin (TSLP), Interleukin-25 (IL-25), and Interleukin-33 (IL-33).
- Th2 Lymphocyte Recruitment: These alarmins activate dermal dendritic cells and Type 2 Innate Lymphoid Cells (ILC2), which migrate to regional lymph nodes to prime naive T-cells into Th2 helper T-cells.
- Th2 Cytokines (IL-4 & IL-13): Activated Th2 cells infiltrate the skin and secrete Th2 cytokines (such as IL-4 and IL-13). These cytokines act on keratinocytes to further impair the skin barrier, creating a continuous cycle of inflammation and barrier disruption [15:5].
¶ 3. Cutaneous Dysbiosis and Staphylococcus aureus Superantigens
Healthy skin is colonized by a diverse microbial community that secretes antimicrobial peptides to suppress pathogen colonization.
- Loss of Microbial Diversity: In AD, the dry, alkaline skin surface and the lack of host-derived antimicrobial peptides (suppressed by IL-4 and IL-13) cause a loss of microbial diversity.
- Staphylococcal Domination: Staphylococcus aureus aggressively colonizes atopic lesions at high rates [19:1]. Microbial colonization and superinfection by Staphylococcus aureus can cause disease exacerbation [19:2], contributing to massive T-cell activation and cytokine release that drive acute clinical flares [18:4].
¶ 4. The Itch-Scratch Cycle and Neuroimmune Signaling
Pruritus in atopic dermatitis is not mediated by histamine; antihistamines are clinically ineffective at treating AD-induced itch [6:12][15:6]. Instead, it is driven by direct neuroimmune communication:
- The "Itch Cytokine" (IL-31): IL-31 is produced primarily by Th2 cells. The cytokine IL-31 is a key mediator of pruritus, and targeting this pathway (e.g., with nemolizumab) represents an important therapeutic approach for managing itch [12:2][18:5][38].
- Sensory Transmission: Activation of IL-31RA triggers downstream signaling (JAK1/2 pathways) in the sensory neuron, transmitting the itch signal through the spinal cord to the somatosensory cortex, inducing the urge to scratch.
- Physical Damage and Amplification: Scratching physically tears the epidermis, causing further alarmin release, cell damage, and pathogen penetration. This recruits more Th2 cells, releasing more IL-31, locking the patient into a chronic itch-scratch cycle [15:7].
¶ Dosage & Protocols
¶ Step-Up and Step-Down Treatment Protocol
Clinical management of atopic dermatitis utilizes a stepped care approach. Treatment intensity escalates (step-up) when disease is uncontrolled, and tapers (step-down) once stable remission is achieved [6:13][7:13][18:6].
+-----------------------------------------------------------------------------------+
| STEPPED TREATMENT PROTOCOL FLOW |
+-----------------------------------------------------------------------------------+
| |
| [STEP 1: Mild / Baseline (All Patients)] |
| - Daily ceramide-dominant emollients (twice daily, within 3 min of bathing). |
| - Diluted sodium hypochlorite baths for S. aureus colonization. |
| - Trigger identification & management. |
| - *DIETARY WARNING:* Focus on low certainty of elimination diet evidence. |
| |
| [STEP 2: Mild-to-Moderate (Episodic or Proactive)] |
| - Low-to-medium potency TCS (e.g., Hydrocortisone 2.5%, Triamcinolone 0.1%). |
| - Topical Calcineurin Inhibitors (TCIs; Tacrolimus 0.1%, Pimecrolimus 1%). |
| - Topical PDE4 Inhibitors (Crisaborole 2%) or topical JAKi (Ruxolitinib 1.5%). |
| |
| [STEP 3: Moderate-to-Severe (Refractory to Topicals)] |
| - Add Phototherapy: Narrowband UVB (NB-UVB), 311 nm wavelength. |
| - Frequency: 2 to 3 sessions per week; assess response at 12 weeks. |
| |
| [STEP 4: Severe / Refractory (Advanced Systemic Therapies)] |
| - Targeted Biologics: |
| * Dupilumab: Subcutaneous administration according to manufacturer labeling. |
| * Lebrikizumab: Subcutaneous administration according to manufacturer labeling.|
| - Oral JAK Inhibitors: |
| * Upadacitinib: Oral administration according to manufacturer labeling. |
| * Abrocitinib: Oral administration according to manufacturer labeling. |
| * Establish baseline screenings and periodic lab monitoring per labeling. |
+-----------------------------------------------------------------------------------+
¶ Step 1: Mild / Baseline Barrier Care and Trigger Management
- Emollient Therapy: Apply a ceramide-dominant, fragrance-free emollient (cream or ointment) at least twice daily and within 3 minutes of bathing to seal in moisture [6:14][14:3].
- Wet Wrap Therapy: For acute flares, wet wrap therapy can be used with emollients and topical corticosteroids to rapidly boost skin hydration and reduce disease severity [6:15][14:4][16:5].
- Diluted Bleach Baths: Diluted sodium hypochlorite baths (bleach baths) are sometimes suggested as an adjunctive clinical option; however, clinical trial evidence remains conflicting regarding their effectiveness in reducing S. aureus density or eczema severity [6:16][15:8].
- Trigger Management & Food Allergy Warnings: Identify and minimize exposure to physical, chemical, or emotional triggers [15:9].
- Dietary Elimination Warning: Do not initiate unselected or routine dietary elimination diets (such as dairy-free or gluten-free) in patients with atopic dermatitis. Systematic review evidence shows only low-certainty evidence that dietary elimination may lead to a slight, potentially clinically unimportant improvement in eczema severity, pruritus, and sleeplessness [36:1].
- There is a strong clinical consensus against routine, unselected dietary restriction in atopic dermatitis without a confirmed, clinically proven food allergy [6:17]. Unnecessary food restriction should be avoided because of the low certainty of benefit, potential nutritional deficiencies, and the risk of delaying more effective, standard-of-care treatments [6:18][36:2].
¶ Step 2: Mild-to-Moderate Topical Anti-inflammatory Therapy
- Topical Corticosteroids (TCS): Apply once or twice daily during active flares. Potency must match lesion location and patient age:
- Sensitive Areas (Face, Flexures, Genitals, Pediatric): Low-potency (Class 6 or 7, e.g., Hydrocortisone 2.5% or Desonide 0.05%) to minimize risk of atrophy [6:19][14:5].
- Trunk and Limbs: Mid-potency (Class 4 or 5, e.g., Triamcinolone acetonide 0.1% or Fluticasone propionate 0.05%) [6:20][14:6].
- Thickened/Lichenified Plaques (Palms, Soles): High-to-super-high potency (Class 1 or 2, e.g., Clobetasol propionate 0.05%) applied to active lesions for short periods under medical supervision to avoid adverse effects [6:21][14:7].
- Topical Calcineurin Inhibitors (TCI): Tacrolimus 0.1% ointment or Pimecrolimus 1% cream [5:10][6:22].
- Topical PDE4 Inhibitors: Crisaborole 2% ointment applied twice daily [6:24].
- Topical JAK Inhibitors: Ruxolitinib 1.5% cream applied twice daily to active lesions (restricted to body surface area) for rapid pruritus relief [5:11][6:25].
¶ Step 3: Moderate-to-Severe Phototherapy
- Indication: Patients with moderate-to-severe disease refractory to optimized topical therapies [7:14][13:2].
- Regimen: Narrowband UVB (NB-UVB; 311 nm wavelength) phototherapy can be administered as a safe and effective treatment option [15:11][39], typically administered in a clinical setting as a second-line treatment for moderate-to-severe disease [7:15][13:3][16:6].
- Mechanism & Safety: Suppresses cutaneous T-cell inflammation and reduces S. aureus colonization [7:16]. Ensure eyes and genitals are shielded during treatment.
¶ Step 4: Severe / Refractory Advanced Systemic Therapies
- Systemic Biologics:
- Dupilumab (IL-4Rα Antagonist): Administered subcutaneously with dosing determined by a clinician according to patient-specific factors and manufacturer labeling [7:17][9:4]. No routine laboratory monitoring is required [7:18].
- Lebrikizumab (IL-13 Antagonist): Administered subcutaneously with dosing determined by a clinician according to patient-specific factors and manufacturer labeling [12:3].
- Tralokinumab (IL-13 Antagonist): Administered subcutaneously with dosing determined by a clinician according to patient-specific factors and manufacturer labeling [7:19].
- Oral Janus Kinase (JAK) Inhibitors:
- Oral JAK Inhibitors: Medications such as upadacitinib and abrocitinib are administered orally with dosing determined by a clinician according to patient-specific factors and manufacturer labeling [7:20][8:6]. These agents provide highly effective, rapid skin clearance and itch reduction, with high-dose upadacitinib being among the most effective systemic treatments for key clinical outcomes [8:7][31:2].
- Monitoring Requirements: Baseline screenings and periodic laboratory monitoring should be established in accordance with clinical guidelines and product-specific manufacturer labeling [7:21][11:4].
¶ Adjuvant and Complementary Therapies
- Allergen Immunotherapy (AIT): For patients with atopic dermatitis who are sensitized to aeroallergens, particularly house dust mites, allergen immunotherapy (both subcutaneous and sublingual routes) has been shown to produce clinically meaningful improvements in disease severity and quality of life [37:1].
- Complementary Modalities (Acupuncture and LED): Systematic reviews suggest that acupuncture may help reduce itch intensity (measured by visual analogue scale), improve general health-related quality of life (DLQI), and reduce overall disease severity scores (SCORAD) in patients with atopic dermatitis, though larger, high-quality clinical trials are needed to confirm these clinical effects [40]. Additionally, light-emitting diode (LED) phototherapy, such as yellow or near-infrared light devices, has been evaluated as an alternative non-UV phototherapeutic option with potential benefit, though clinical heterogeneity remains high [41].
¶ Pregnancy & Lactation Management
Atopic dermatitis is the most common skin disease among pregnant women, requiring a careful step-up therapeutic hierarchy to balance maternal relief with fetal safety [17:1]:
- First-Line (Low-to-Medium Potency TCS): Low-to-medium potency topical corticosteroids are generally considered safe during pregnancy based on systematic reviews of pregnancy outcomes [42][43]. During lactation, topical corticosteroids are safe when applied appropriately, avoiding prolonged use on large areas [39:1]. If applied to the breast or nipple, ensure any treated area is washed before nursing, and consult a clinician to select an appropriate water-miscible formulation over ointments to avoid paraffins. It is recommended to avoid potent or very potent topical corticosteroids over large body surface areas during pregnancy to minimize any potential systemic risk of reduced birth weight, whereas mild-to-moderate topical corticosteroids are considered safe for both mother and fetus [42:1][43:1].
- Second-Line (Phototherapy): Narrowband UVB (NB-UVB) phototherapy is the safest second-line choice for moderate-to-severe disease in pregnant patients, as it lacks systemic teratogenic potential [7:22][13:4].
- Systemic Biologic Considerations (Dupilumab): Systematic reviews and meta-analyses of pregnancy registries indicate that dupilumab is probably safe during pregnancy and preconception, displaying spontaneous abortion rates (18.9%) comparable to the general population and zero reports of congenital malformations [17:2]. However, its use should be reserved for cases where maternal disease is severe and refractory to phototherapy. Other biologics, such as lebrikizumab, currently lack similar published pregnancy registry data in the cited systematic review.
- Contraindicated Systemic Agents: Systemic JAK inhibitors (upadacitinib, abrocitinib) are generally avoided during pregnancy and lactation due to the lack of human safety data and recommendations in interdisciplinary expert consensus guidelines [44]. Systemic immunomodulatory therapies should only be initiated under strict specialist supervision and individual risk-benefit assessment [7:23].
¶ Safety
¶ Safety and Red Flags
EMERGENCY CLINICAL ALERT: ECZEMA HERPETICUM
- Definition & Emergency Status: Eczema herpeticum is a severe, disseminated cutaneous viral infection caused by the herpes simplex virus (HSV-1 or HSV-2) superinfecting skin barrier-disrupted atopic lesions. It is widely recognized in standard clinical consensus as a dermatological emergency requiring immediate attention.
- Clinical Presentation: Characterized by the sudden eruption of monomorphic, dome-shaped, painful, punched-out erosions with hemorrhagic crusts, often accompanied by high fever, malaise, and lymphadenopathy.
- Critical Risks: Rapid ocular involvement (herpetic keratoconjunctivitis) leading to permanent blindness, or systemic dissemination (viremia) leading to herpetic meningitis, encephalitis, or fatal multi-organ failure.
- Immediate Action Required: Initiate immediate systemic antiviral therapy and obtain emergency ophthalmology and dermatology evaluations [18:7].
¶ Unsafe Self-Prescribing & Misuse
- Topical Steroid Misuse: Continuous, unmonitored daily application of high-potency TCS, especially on thin-skin areas (face, neck, intertriginous folds), induces rapid tachyphylaxis, dermal thinning, irreversible striae, and increases the risk of developing Topical Steroid Withdrawal (TSW) [10:2].
- Prescription Sharing: Sharing systemic immunomodulators or JAK inhibitors is highly dangerous due to the strict requirement for baseline screening (e.g., tuberculosis, hepatitis B/C) and regular laboratory monitoring [7:24][11:5].
¶ Safe Self-Care Boundaries
- Home Care Limits: Self-care should be restricted to basic barrier preservation with ceramide-dominant emollients, wet wrap therapy, and trigger avoidance [6:26][14:8].
- Mandatory Clinician Evaluation: A comprehensive clinical evaluation is mandatory if:
- Skin symptoms are uncontrolled on basic Step 2 topical regimens [7:25].
- There are signs of secondary bacterial infection (yellow honey-colored crusting, purulent drainage) requiring topical or systemic antimicrobials [18:8][19:3].
- There is rapid, sudden worsening of pain or the appearance of vesicular/punched-out lesions suggesting eczema herpeticum [18:9].
- Erythroderma (diffuse, widespread redness covering the vast majority of the body surface area) develops, which carries high risks of high-output cardiac failure, hypothermia, and sepsis [18:10].
¶ Detailed Adverse Event Profiles
¶ 1. Topical Steroid Withdrawal (TSW) and Skin Atrophy
- Atrophy Pathophysiology: Corticosteroids inhibit dermal fibroblasts, leading to decreased synthesis of collagen, elastin, and glycosaminoglycans. This structurally weakens the dermis, presenting clinically as thin, translucent skin, striae, prominent telangiectasias, and purpura [45][46].
- TSW Presentation: Abrupt cessation of long-term, inappropriate, high-potency TCS can lead to significant rebound flares, burning erythema, and skin sensitivity [10:3].
- Tapering Protocols & Mitigation: To minimize withdrawal risks, a gradual reduction in application frequency or transition to non-steroidal topical agents (such as TCIs) under clinical supervision is generally recommended [10:4].
¶ 2. Oral Janus Kinase (JAK) Inhibitor Class Safety Metrics
Systemic oral JAK inhibitors (upadacitinib, abrocitinib) block downstream signaling of multiple inflammatory cytokines. Their safety profile involves a distinction between class-wide regulatory warnings and clinical trial findings:
- Class-Wide Regulatory Boxed Warnings: Oral JAK inhibitors carry regulatory boxed warnings (FDA warnings) for increased risk of venous thromboembolism (VTE), major adverse cardiovascular events (MACE), malignancies, and serious infections [11:6]. These are based on safety studies in other inflammatory diseases (such as rheumatoid arthritis).
- Clinical Trial Evidence (Short-Term): In systematic reviews of randomized controlled trials for atopic dermatitis, there was no statistically significant increase in the risks of VTE, MACE, malignancies, or serious infections (other than Herpes Zoster) during short-term follow-up [11:7].
- Proven Short-Term Adverse Events: The short-term trials did demonstrate a statistically significant increase in the risk of Herpes Zoster (shingles) reactivation, headache, acne, elevated blood creatinine phosphokinase (CPK), and nausea [11:8].
- Laboratory Monitoring Protocol: Baseline screenings and periodic laboratory monitoring should be established in accordance with clinical guidelines and product-specific manufacturer labeling [7:26][11:9].
¶ 3. Ocular Adverse Events of Biologics (IL-4Rα/IL-13 Inhibitors)
- Biologic-Associated Conjunctivitis: Conjunctivitis and other minor ocular issues (such as blepharitis or dry eye) represent potential side effects of IL-4Rα inhibitors when used for atopic dermatitis, though clinical trials demonstrate high overall tolerability with safety profiles comparable to placebo [9:5].
- Mitigation: Mild cases can typically be managed with artificial tears and warm compresses. More persistent or severe ocular symptoms require formal ophthalmological evaluation and co-management to determine appropriate prescription treatments while safely continuing the systemic biologic [7:27][12:4].
¶ Tracking and Referral Plan
¶ Subjective & Objective Biomarker Tracking
To optimize therapy and guide step-up or step-down adjustments, clinicians and patients should track disease activity using validated, standardized tools:
- EASI (Eczema Area and Severity Index): Clinicians should document EASI at every visit. A 75% or greater reduction from baseline (EASI-75) is the standard benchmark for successful clinical response in systemic therapy trials [7:28][8:8][9:6].
- POEM (Patient-Oriented Eczema Measure): Patients should complete the POEM questionnaire weekly to track subjective symptom burden. Reductions in the total score represent clinically meaningful improvements in patient-reported severity [31:3][32:3].
- Pruritus NRS (Numeric Rating Scale): Track peak daily itch on a 0 to 10 scale. A significant reduction in the pruritus score is a standard clinical endpoint representing meaningful itch relief [7:29][8:9][32:4].
¶ PCP to Dermatologist Referral Guidelines
Primary care providers should initiate a timely referral to a dermatologist under the following clinical circumstances:
- Treatment Failure: Symptoms remain uncontrolled (persistent intense pruritus, recurrent flares) despite 4 to 6 weeks of optimized, compliant Step 2 topical therapy [7:30].
- Diagnostic Ambiguity: Atypical lesion morphology, atypical distribution, or lack of response to topicals, raising suspicion for cutaneous T-cell lymphoma, atypical contact dermatitis, or unusual infectious mimics [21:8].
- Systemic Candidate: Patient is a potential candidate for Step 4 systemic biologics or oral JAK inhibitors, requiring advanced screening, prescription access, and specialized safety monitoring [7:31][11:10].
- Complications: Recurrent severe bacterial infections, suspected eczema herpeticum, or development of erythroderma [18:11][19:4].
¶ FAQ
¶ Why do antihistamines fail to relieve itching in atopic dermatitis?
Classic H1 antihistamines (such as cetirizine, fexofenadine, or diphenhydramine) fail because the pruritus in atopic dermatitis is non-histaminergic [6:27][15:12]. The intense itch is mediated directly by Th2 cytokines—specifically Interleukin-31 (IL-31)—binding to IL-31RA receptors on unmyelinated sensory C-fibers, as well as proteases and TSLP triggering neuroimmune pathway activation [15:13]. First-generation sedating antihistamines may assist with nighttime sleep solely due to their central sedative effects, but they do not resolve the underlying physiological itch signaling [6:28][15:14].
¶ Is there a link between atopic dermatitis and food allergies?
There is an epidemiological association between atopic dermatitis and food allergies, but routine, unselected elimination diets are not recommended [36:3]. Systematic reviews show only low-certainty evidence of slight, potentially clinically unimportant improvements in eczema symptoms with dietary elimination, which must be carefully weighed against the risks of indiscriminate restriction [36:4]. Clinical consensus parameters strongly recommend against routine dietary restriction, advising that elimination diets should be limited to individuals with a confirmed, IgE-mediated food allergy diagnosed by a specialist [6:29][36:5].
¶ What is the difference between eczema and atopic dermatitis?
"Eczema" is a broad umbrella term for several distinct types of inflammatory skin conditions, including allergic and irritant contact dermatitis, seborrheic dermatitis, nummular eczema, and dyshidrotic eczema. Atopic dermatitis is a specific, chronic, systemic, genetically linked type of eczema characterized by dry skin, a damaged barrier, Th2-mediated immune dysregulation, and a strong personal or family association with other atopic diseases like asthma and seasonal allergic rhinitis [18:12][21:9][30:2].
¶ Can bleach baths improve atopic dermatitis?
Diluted sodium hypochlorite baths (bleach baths) are sometimes used as adjunctive therapies for patients with frequent flares or suspected high bacterial colonization [15:15]. While they possess antimicrobial properties in vitro, clinical evidence is conflicting regarding whether they consistently reduce S. aureus density or eczema severity in vivo [15:16].
¶ Are there any natural supplements that are clinically effective for atopic dermatitis?
Systematic reviews and meta-analyses support a clinical benefit for Vitamin D supplementation, which significantly reduces atopic dermatitis severity scores (such as SCORAD and EASI) [35:1]. For other interventions, clinical trials of probiotics, prebiotics, and hydrolyzed formulas in children without food allergies suggest a trend in reducing severity scores, but evidence remains limited [47]. Systematic reviews of dietary elimination diets show only a slight, potentially clinically unimportant improvement in symptoms [36:6].
¶ References
Migliavaca CB, Lazzarini R, Stein C. Prevalence of Atopic Dermatitis: A Systematic Review and Meta-Analysis. Dermatitis. 2025. https://pubmed.ncbi.nlm.nih.gov/39134072/ ↩︎
Brown SJ, Irvine AD. Atopic eczema and the filaggrin story. Seminars in Cutaneous Medicine and Surgery. 2008. https://pubmed.ncbi.nlm.nih.gov/18620134/ ↩︎ ↩︎
Rodríguez E, Baurecht H, Herberich E, et al. Meta-analysis of filaggrin polymorphisms in eczema and asthma: robust risk factors in atopic disease. The Journal of Allergy and Clinical Immunology. 2009. https://pubmed.ncbi.nlm.nih.gov/19501237/ ↩︎ ↩︎
Kawasaki H, Kubo A, Sasaki T. Loss-of-function mutations within the filaggrin gene and atopic dermatitis. Current Problems in Dermatology. 2011. https://pubmed.ncbi.nlm.nih.gov/21576945/ ↩︎
Chu DK, Chu AWL, Rayner DG, et al. Topical treatments for atopic dermatitis (eczema): Systematic review and network meta-analysis of randomized trials. The Journal of Allergy and Clinical Immunology. 2023. https://pubmed.ncbi.nlm.nih.gov/37678572/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sidbury R, Alikhan A, Bercovitch L, et al. Guidelines of care for the management of atopic dermatitis in adults with topical therapies. Journal of the American Academy of Dermatology. 2023. https://pubmed.ncbi.nlm.nih.gov/36641009/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Davis DMR, Drucker AM, Alikhan A, et al. Guidelines of care for the management of atopic dermatitis in adults with phototherapy and systemic therapies. Journal of the American Academy of Dermatology. 2024. https://pubmed.ncbi.nlm.nih.gov/37943240/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chu AWL, Wong MM, Rayner DG, et al. Systemic treatments for atopic dermatitis (eczema): Systematic review and network meta-analysis of randomized trials. The Journal of Allergy and Clinical Immunology. 2023. https://pubmed.ncbi.nlm.nih.gov/37678577/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Koskeridis F, Evangelou E, Ntzani EE. Treatment With Dupilumab in Patients With Atopic Dermatitis: Systematic Review and Meta-Analysis. Journal of Cutaneous Medicine and Surgery. 2022. https://pubmed.ncbi.nlm.nih.gov/36214355/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
H Hajar, YA Leshem, JM Hanifin, et al. A systematic review of topical corticosteroid withdrawal ("steroid addiction") in patients with atopic dermatitis and other dermatoses. Journal of the American Academy of Dermatology. 2015. https://pubmed.ncbi.nlm.nih.gov/25592622/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yoon S, Kim K, Shin K. The safety of systemic Janus kinase inhibitors in atopic dermatitis: A systematic review and meta-analysis of randomized controlled trials. Journal of the European Academy of Dermatology and Venereology. 2024. https://pubmed.ncbi.nlm.nih.gov/37597261/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Davis DMR, Frazer-Green L, Alikhan A, et al. Focused update: Guidelines of care for the management of atopic dermatitis in adults. Journal of the American Academy of Dermatology. 2025. https://pubmed.ncbi.nlm.nih.gov/40531067/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Sidbury R, Davis DM, Cohen DE, et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. Journal of the American Academy of Dermatology. 2014. https://pubmed.ncbi.nlm.nih.gov/24813298/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Eichenfield LF, Tom WL, Berger TG, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. Journal of the American Academy of Dermatology. 2014. https://pubmed.ncbi.nlm.nih.gov/24813302/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. Journal of the European Academy of Dermatology and Venereology. 2018. https://pubmed.ncbi.nlm.nih.gov/29676534/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
W Frazier, N Bhardwaj. Atopic Dermatitis: Diagnosis and Treatment. American Family Physician. 2020. https://pubmed.ncbi.nlm.nih.gov/32412211/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Safety of Dupilumab Therapy for Atopic Dermatitis during Pregnancy: A Systematic Review and Meta-analysis. Acta Dermato-Venereologica. 2025. https://pubmed.ncbi.nlm.nih.gov/39936607/ ↩︎ ↩︎ ↩︎
Saeki H, Ohya Y, Arakawa H, et al. English version of clinical practice guidelines for the management of atopic dermatitis 2024. The Journal of Dermatology. 2025. https://pubmed.ncbi.nlm.nih.gov/39707640/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part II. Journal of the European Academy of Dermatology and Venereology. 2018. https://pubmed.ncbi.nlm.nih.gov/29878606/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Katoh N, Ohya Y, Ikeda M, et al. Clinical practice guidelines for the management of atopic dermatitis 2018. The Journal of Dermatology. 2019. https://pubmed.ncbi.nlm.nih.gov/31599013/ ↩︎
Lawrence F Eichenfield, Wynnis L Tom, Sarah L Chamlin, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. Journal of the American Academy of Dermatology. 2014. https://pubmed.ncbi.nlm.nih.gov/24290431/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Thyssen JP, Schuttelaar MLA, Alfonso JH, et al. Guidelines for diagnosis, prevention, and treatment of hand eczema. Contact Dermatitis. 2022. https://pubmed.ncbi.nlm.nih.gov/34971008/ ↩︎
Waleed Adawi, Hannah Cornman, Anusha Kambala, et al. Diagnosing Atopic Dermatitis in Skin of Color. Dermatologic Clinics. 2023. https://pubmed.ncbi.nlm.nih.gov/37236711/ ↩︎ ↩︎ ↩︎ ↩︎
Allergic contact dermatitis: epidemiology, molecular mechanisms, in vitro methods and regulatory aspects. Archives of Toxicology. 2012. https://pubmed.ncbi.nlm.nih.gov/21997384/ ↩︎ ↩︎
Patch Testing in an Allergy Clinic: Real-world Experience. Dermatology Research and Practice. 2022. https://pubmed.ncbi.nlm.nih.gov/36309860/ ↩︎
Esser PR, Martin SF. Pathomechanisms of Contact Sensitization. Current Allergy and Asthma Reports. 2017. https://pubmed.ncbi.nlm.nih.gov/29129023/ ↩︎ ↩︎ ↩︎
Schürer NY, Dickel H. Protection from physical noxae. Current Problems in Dermatology. 2007. https://pubmed.ncbi.nlm.nih.gov/17312360/ ↩︎ ↩︎
Effendy I, Löffler H, Maibach HI. Epidermal cytokines in murine cutaneous irritant responses. Journal of Applied Toxicology. 2000. https://pubmed.ncbi.nlm.nih.gov/10942909/ ↩︎
PP Vakharia, R Chopra, JI Silverberg, et al. Systematic Review of Diagnostic Criteria Used in Atopic Dermatitis Randomized Controlled Trials. American Journal of Clinical Dermatology. 2018. https://pubmed.ncbi.nlm.nih.gov/28624959/ ↩︎ ↩︎
Severity assessments used for inclusion criteria and baseline severity evaluation in atopic dermatitis clinical trials: a systematic review. The British Journal of Dermatology. 2017. https://pubmed.ncbi.nlm.nih.gov/28750145/ ↩︎ ↩︎ ↩︎
Drucker AM, Morra DE, Prieto-Merino D, et al. Systemic Immunomodulatory Treatments for Atopic Dermatitis: Update of a Living Systematic Review and Network Meta-analysis. JAMA Dermatology. 2022. https://pubmed.ncbi.nlm.nih.gov/35293977/ ↩︎ ↩︎ ↩︎ ↩︎
Drucker AM, Lam M, Prieto-Merino D, et al. Systemic Immunomodulatory Treatments for Atopic Dermatitis: Living Systematic Review and Network Meta-Analysis Update. JAMA Dermatology. 2024. https://pubmed.ncbi.nlm.nih.gov/39018058/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Miller J, Simpson A, Bloom P, et al. 2023 AAHA Management of Allergic Skin Diseases in Dogs and Cats Guidelines. Journal of the American Animal Hospital Association. 2023. https://pubmed.ncbi.nlm.nih.gov/37883677/ ↩︎ ↩︎ ↩︎
Treatment of canine atopic dermatitis: 2015 updated guidelines from the International Committee on Allergic Diseases of Animals (ICADA). BMC Veterinary Research. 2015. https://pubmed.ncbi.nlm.nih.gov/26276051/ ↩︎ ↩︎ ↩︎
Nielsen AY, Høj S, Thomsen SF. Vitamin D Supplementation for Treating Atopic Dermatitis in Children and Adults: A Systematic Review and Meta-Analysis. Nutrients. 2024. https://pubmed.ncbi.nlm.nih.gov/39683522/ ↩︎ ↩︎
Dietary Elimination for the Treatment of Atopic Dermatitis: A Systematic Review and Meta-Analysis. The Journal of Allergy and Clinical Immunology: In Practice. 2022. https://pubmed.ncbi.nlm.nih.gov/35987995/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Allergen immunotherapy for atopic dermatitis: Systematic review and meta-analysis of benefits and harms. The Journal of Allergy and Clinical Immunology. 2023. https://pubmed.ncbi.nlm.nih.gov/36191689/ ↩︎ ↩︎
Nemolizumab (Nemluvio) for atopic dermatitis. The Medical Letter on Drugs and Therapeutics. 2025. https://pubmed.ncbi.nlm.nih.gov/39946696/ ↩︎
Vestergaard C, Wollenberg A, Barbarot S, et al. European task force on atopic dermatitis position paper: treatment of parental atopic dermatitis during preconception, pregnancy and lactation period. Journal of the European Academy of Dermatology and Venereology. 2019. https://pubmed.ncbi.nlm.nih.gov/31231864/ ↩︎ ↩︎
Acupuncture for atopic dermatitis: a systematic review and meta-analysis. BMJ Open. 2024. https://pubmed.ncbi.nlm.nih.gov/39638592/ ↩︎
Utilization of light-emitting diodes for skin therapy: Systematic review and meta-analysis. Photodermatology, Photoimmunology & Photomedicine. 2023. https://pubmed.ncbi.nlm.nih.gov/36310510/ ↩︎
CC Chi, SH Wang, F Wojnarowska, et al. Safety of topical corticosteroids in pregnancy. The Cochrane Database of Systematic Reviews. 2015. https://pubmed.ncbi.nlm.nih.gov/26497573/ ↩︎ ↩︎
CC Chi, SH Wang, G Kirtschig, et al. Systematic review of the safety of topical corticosteroids in pregnancy. Journal of the American Academy of Dermatology. 2010. https://pubmed.ncbi.nlm.nih.gov/20117858/ ↩︎ ↩︎
Deleuran M, Dézfoulian B, Elberling J, et al. Systemic anti-inflammatory treatment of atopic dermatitis during conception, pregnancy and breastfeeding: Interdisciplinary expert consensus in Northern Europe. Journal of the European Academy of Dermatology and Venereology. 2024. https://pubmed.ncbi.nlm.nih.gov/37818828/ ↩︎
Lehmann P, Zheng P, Lavker RM, et al. Corticosteroid atrophy in human skin. A study by light, scanning, and transmission electron microscopy. The Journal of Investigative Dermatology. 1983. https://pubmed.ncbi.nlm.nih.gov/6875302/ ↩︎
Nuutinen P, Riekki R, Parikka M, et al. Modulation of collagen synthesis and mRNA by continuous and intermittent use of topical hydrocortisone in human skin. The British Journal of Dermatology. 2003. https://pubmed.ncbi.nlm.nih.gov/12534592/ ↩︎
A systematic review and meta-analysis of nutritional and dietary interventions in randomized controlled trials for skin symptoms in children with atopic dermatitis and without food allergy: An EAACI task force report. Allergy. 2024. https://pubmed.ncbi.nlm.nih.gov/38783644/ ↩︎