¶ Gene Therapy
| Indication | Investigational (Longevity/Age-Related Disease) / Medical Use (Specific Diseases) |
| Access | Clinical Trials / Highly Regulated Prescriptions |
| Dosing Sched | Single administration or periodic (variable) |
| Safety Profile | Moderate to High (Vector-dependent risks) |
| Key Marker | Transgene expression, immune response, clinical outcomes |
| Est. Cost | High (>$100,000) |
Gene therapy involves introducing genetic material into a person's cells to treat or prevent disease. For longevity and age-related conditions, it represents a frontier intervention aimed at addressing underlying biological mechanisms of aging, though largely still in preclinical or early clinical development for these specific indications [1][2].
¶ At a glance
Key points (high-level summary)
- Targets aging hallmarks: Gene therapy approaches are designed to counteract genomic instability, telomere attrition, epigenetic alterations, and cellular senescence by delivering functional genes or modifying gene expression [2:1][3].
- Diverse strategies: Includes adding functional genes (e.g., telomerase, Klotho), modifying gene expression (e.g., follistatin), or epigenetic reprogramming (Yamanaka factors) [2:2][3:1][4].
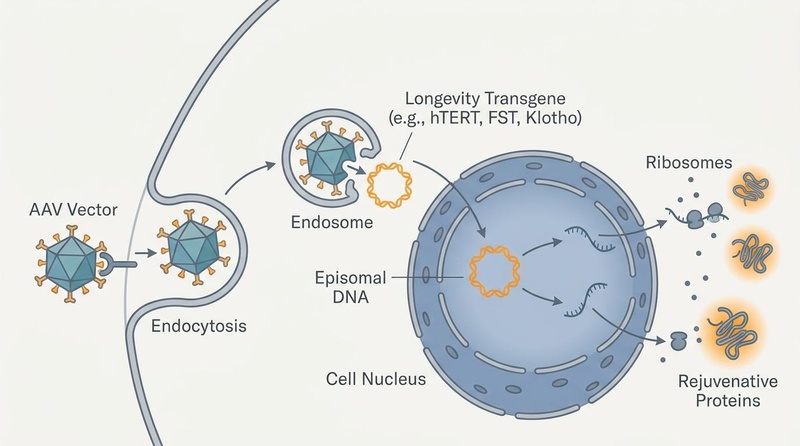
- Vector-mediated delivery: Commonly uses adeno-associated virus (AAV) vectors for in vivo delivery due to their low immunogenicity and stable episomal expression [1:1][5].
- Safety remains a primary concern: Risks include insertional mutagenesis, immune responses to viral vectors, and off-target effects, necessitating careful vector design and monitoring [6][1:2][7].
What people use it for
- Main goals: Longevity, age-related disease prevention/treatment (e.g., sarcopenia, cognitive decline, vision loss).
- Evidence quality: Varies significantly by target; preclinical for longevity, early-phase human trials for specific age-related conditions (e.g., muscular dystrophy), established for some rare monogenic diseases.
¶ What It Is
Gene therapy introduces exogenous genetic material—DNA or RNA—into a patient's cells to produce a therapeutic effect. This genetic material can be delivered using viral vectors (e.g., adeno-associated viruses, lentiviruses) or non-viral methods. The goal is to either correct a genetic defect, provide a new function, or modify gene expression to combat disease processes [1:3][8]. For longevity, the focus is on genes that regulate fundamental aging pathways, aiming to rejuvenate tissues and extend healthy lifespan [2:3][9].
¶ Benefits & Mechanisms
¶ Telomerase Gene Therapy
Telomerase is an enzyme that maintains telomere length, the protective caps at the ends of chromosomes. Telomere attrition is a hallmark of aging [2:4].
- Mechanism: Delivery of the telomerase reverse transcriptase (TERT) gene aims to restore telomerase activity, thereby counteracting telomere shortening in aging cells. This is hypothesized to improve cellular function, tissue regeneration, and extend healthy lifespan [2:5][10].
- Preclinical Evidence: Systemic AAV-mediated delivery of mTERT in adult and old mice increased median lifespan by 24% and 13% respectively, improving metabolic, neuromuscular, and cognitive health without increasing cancer incidence [2:6]. Telomerase gene therapy also showed therapeutic effects in mouse models of pulmonary fibrosis associated with short telomeres, improving lung function and reducing inflammation [10:1].
¶ Follistatin Gene Therapy
Follistatin (FST) is a glycoprotein that regulates muscle growth by inhibiting myostatin, a protein that limits muscle mass [11].
- Mechanism: FST gene therapy delivers the FST gene, leading to increased localized or systemic follistatin production. This inhibits myostatin, promoting muscle growth, strength, and mitigating muscle wasting conditions like sarcopenia and muscular dystrophies [11:1].
- Clinical Evidence: Phase 1/2a clinical trials have demonstrated the safety and efficacy of AAV1-mediated follistatin gene therapy in patients with Becker muscular dystrophy (BMD) and sporadic inclusion body myositis (sIBM). These trials showed improvements in muscle strength, functional walking, and overall ambulation [11:2][12].
¶ Klotho Gene Therapy
Klotho is an anti-aging protein associated with enhanced longevity and protection against age-related diseases. There are two main forms: a transmembrane form and a secreted form (sKlotho) [4:1].
- Mechanism: Klotho gene therapy aims to increase Klotho protein levels, which can modulate various signaling pathways involved in oxidative stress, inflammation, and cellular senescence. Increased Klotho has been linked to improved cognitive function, cardiovascular health, and renal protection [4:2][13].
- Preclinical & Early Clinical Evidence: A single administration of low-dose sKlotho enhanced memory and synaptic plasticity in aged non-human primates [4:3]. AAV-mediated αKlotho expression in senescence-accelerated SAMP8 mice counteracted cognitive decline, muscle wasting, and cardiac hypertrophy [13:1]. Early-phase human trials are exploring the safety and efficacy of injectable Klotho plasmid gene therapy for longevity and cognitive function [14].
¶ Yamanaka Factors / Reprogramming via Viral Vectors
Yamanaka factors (Oct4, Sox2, Klf4, c-Myc – OSKM) are transcription factors capable of reprogramming somatic cells into induced pluripotent stem cells (iPSCs). Partial reprogramming strategies aim to reverse cellular aging without inducing full pluripotency and teratoma formation [3:2].
- Mechanism: Controlled, transient expression of Yamanaka factors (often a subset like OSK) can epigenetically reset the cellular age of tissues, restoring youthful gene expression patterns and regenerative capacity [3:3]. This is thought to reverse age-related cellular damage and improve tissue function.
- Preclinical Evidence: AAV2-mediated delivery of OSK into mouse retinal ganglion cells reversed DNA methylation age, promoted axon regeneration, and restored vision in models of glaucoma and old age. This partial reprogramming was achieved safely without tumor formation [3:4]. Targeted hypothalamic OSKM expression has also shown to prolong fertility and ovulation in female rats [15]. Localized hippocampal OSKM gene therapy in aged rats has reversed cognitive decline [16]. The primary safety concern with full reprogramming is the risk of teratoma formation, which is mitigated by partial or transient expression [17][18].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Muscle strength/ambulation (BMD/sIBM) | High | Moderate | Phase 1/2a RCTs | AAV1.FS344, intramuscular, 6 patients with BMD [11:3]; 6 patients with sIBM [12:1] | |
| Cognition (aged non-human primates) | High | Low | 1 study (primates) | Low-dose sKlotho protein in aged rhesus macaques [4:4] | |
| Telomere length/healthspan (human) | Insufficient data | Insufficient evidence | 0 RCTs | No confirmed human RCT evidence for longevity [2:7][1:4] | |
| Vision restoration (glaucoma/age-related) | Insufficient data | Insufficient evidence | 0 RCTs | Preclinical in mice (AAV2-OSK) [3:5]; no human trials yet for this specific application. | |
| Insertional Mutagenesis (cancer) | High | High | Case reports/reviews | Gammaretroviral vectors in SCID-X1 gene therapy [6:1]; AAV integration near oncogenes [7:1][19] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- *Compact renderer encoding (preferred when using custom tags):
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. Examples:↓↓ (p)-><effect e="d2p"></effect>,= (x)-><effect e="e0x"></effect>,?-><effect e="q0x"></effect>. - IMPORTANT: If using the compact renderer encoding (<effect ...>), do NOT include the text arrows or parentheses next to it. Just use the tag.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
- REQUIRED: You MUST include a citation key (e.g.
[^1]) in the "Notes" column for every single row. If you claim a result, you must link the specific Meta-Analysis or Key RCT that proves it.
¶ Safety, Interactions, Red Flags
Gene therapy, particularly with viral vectors, carries inherent risks that necessitate rigorous safety evaluation:
¶ General Risks of Gene Therapy
- Insertional Mutagenesis: Viral vectors, especially integrating ones (e.g., retroviruses, lentiviruses), can randomly integrate into the host genome. This can potentially activate proto-oncogenes or inactivate tumor suppressor genes, leading to oncogenesis (e.g., leukemia in early SCID-X1 trials with gammaretroviral vectors) [6:2]. While AAV vectors are generally considered non-integrating (remaining episomal), rare integration events can occur, and some studies suggest AAV integration near oncogenes could contribute to hepatocellular carcinoma in preclinical models [7:2][19:1][20].
- Immune Responses to Vectors: The body's immune system can recognize viral vector components (capsid proteins or transgene products) as foreign, leading to immune responses that can reduce efficacy or cause adverse effects. Pre-existing antibodies to common AAV serotypes can limit transduction efficiency, and cytotoxic T-lymphocyte (CTL) responses can eliminate transduced cells [5:1][21]. Strategies to improve AAV safety include capsid engineering and transient immunosuppression [22].
- Off-target Effects: Unintended genetic modifications or expression of the transgene in non-target tissues can occur, leading to systemic side effects. This is a concern particularly with systemic administration of vectors [1:5]. Residual microRNAs in AAV vector batches can also pose potential off-target biological risks [23].
- Toxicity: High doses of viral vectors can induce dose-dependent toxicities, especially in organs like the liver (hepatotoxicity) [1:6][24][21:1]. Thrombotic microangiopathy (TMA) is also a serious, albeit rare, complication [21:2].
- Teratoma Formation: A significant risk with pluripotent stem cell-based therapies or uncontrolled reprogramming, though partial reprogramming strategies aim to mitigate this by avoiding full pluripotency [17:1][18:1].
¶ Regulatory and Ethical Considerations
Gene therapies are subject to stringent regulatory oversight by bodies like the FDA. Ethical concerns revolve around germline editing (heritable changes), equitable access, and the potential for enhancement versus therapy [14:1]. Unproven "anti-aging" gene therapies or plasma infusions marketed outside approved indications have been subject to regulatory warnings [25]. Regulatory frameworks are evolving to address the unique risks of AAV products, including insertion-mediated tumorigenesis [19:2].
¶ Dosage information / protocol
Protocols for gene therapy are highly specific to the gene, vector, target tissue, and indication. Dosing is typically expressed in vector genomes (vg) and can vary widely from 10^10 to 10^14 vg per patient, depending on the vector and delivery method (e.g., intramuscular, intravenous, intraocular) [11:4][3:6]. Administration is often a single event, but some protocols may involve repeated dosing or localized injections.
¶ Dosage at a glance
| Gene Therapy | Typical Dose/Volume | Timing | Notes |
|---|---|---|---|
| Follistatin (BMD/sIBM) | 6 x 10^11 vg/kg rAAV1.CMV.huFS344 | Single intramuscular injection | Bilateral quadriceps injection in clinical trials [11:5][12:2] |
| Telomerase (preclinical) | Systemic rAAV9-mTERT | Single intravenous injection | In mice; improved longevity without increasing cancer [2:8] |
| Klotho (early clinical) | Subcutaneous plasmid gene therapy | Periodic subcutaneous injection | Investigational for healthy adults [14:2] |
| Yamanaka factors (preclinical) | AAV2-OSK (doxycycline-inducible) | Single intraocular injection | Reversible expression in mouse retina, for vision restoration [3:7] |
¶ Side effects
| Effect | Frequency/notes | Route | Evidence |
|---|---|---|---|
| Immune response to vector | Occasional; can lead to inflammation/reduced efficacy | Systemic/Local | Probable [1:7][5:2][21:3] |
| Insertional mutagenesis (cancer) | Rare; primarily with integrating vectors | Systemic (genome integration) | Probable [6:3][7:3][19:3][20:1] |
| Flu-like symptoms | Common (transient) | Systemic | Probable (especially with higher doses) [1:8] |
| Off-target effects | Infrequent; tissue-dependent | Systemic | Possible [1:9][23:1] |
| Hepatotoxicity (liver damage) | Occasional (dose-dependent) | Systemic | Probable [1:10][21:4][24:1] |
| Injection site reactions | Common (local) | Local | Probable [11:6] |
| Thrombotic microangiopathy (TMA) | Rare; serious complication | Systemic | Possible [21:5] |
¶ Precautions
| Population/Condition | Precaution | What to monitor |
|---|---|---|
| Pre-existing anti-AAV antibodies | May reduce efficacy; screen for antibodies | Antibody titers |
| Immunocompromised individuals | Increased risk of viral replication/adverse events | Immune status, viral load |
| Active infections | Defer treatment | Clinical signs, lab tests |
| History of cancer | Increased surveillance due to insertional mutagenesis risk | Oncological screening, imaging |
| Pregnancy/lactation | Avoid; unknown fetal/infant effects | Pregnancy test, lactation status |
| Severe organ impairment (hepatic, renal, cardiac) | Higher risk of adverse events | Organ function tests, clinical monitoring |
¶ FAQs
-
Is gene therapy for longevity approved for clinical use?
-
What are the main safety concerns with gene therapy?
-
Are Yamanaka factors safe for human longevity applications?
- Partial reprogramming using Yamanaka factors is a promising area, with preclinical mouse studies showing safety and efficacy for vision restoration and cognitive rejuvenation [3:8][16:1]. However, full reprogramming to iPSCs in vivo carries a significant risk of teratoma formation, and human longevity applications are still highly experimental, requiring careful context-aware protocols [17:2][18:2].
-
Can I get gene therapy from a commercial clinic?
- Any clinic offering unapproved gene therapies for longevity or anti-aging should be approached with extreme caution. Regulatory bodies like the FDA have issued warnings against unproven "young plasma" infusions and other gene-based interventions marketed outside of regulated clinical trials [25:2].
¶ See also
- Regenerative Medicine
- Cellular Reprogramming
- Epigenetic Alterations
- Telomere Attrition
- Cellular Senescence
- Frontier Longevity Contraindications
¶ References
Colella P, et al. Emerging Issues in AAV-Mediated In Vivo Gene Therapy. Mol Ther Methods Clin Dev. 2018;8:87-101. https://pmc.ncbi.nlm.nih.gov/articles/PMC5177998/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Blasco MA, et al. Telomerase gene therapy in adult and old mice delays aging and increases longevity without increasing cancer. EMBO Mol Med. 2012;4(9):871-881. https://pubmed.ncbi.nlm.nih.gov/22585399/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lu Y, et al. Reprogramming to recover youthful epigenetic information and restore vision. Nature. 2020;588(7836):124-129. https://pubmed.ncbi.nlm.nih.gov/33268865/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Dubal DB, et al. Longevity factor klotho enhances cognition in aged nonhuman primates. Nat Aging. 2023;3(7):851-863. https://pubmed.ncbi.nlm.nih.gov/37349479/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Russell DW, et al. Liver-Directed Adeno-Associated Viral Gene Therapy for Hemophilia. Hum Gene Ther. 2013;24(3):276-282. https://pmc.ncbi.nlm.nih.gov/articles/PMC3615444/ ↩︎ ↩︎ ↩︎
Hacein-Bey-Abina S, et al. LMO2-associated clonal T cell proliferation in two patients after gene therapy for SCID-X1. Science. 2003;302(5644):415-419. https://pubmed.ncbi.nlm.nih.gov/14564000/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chandler RJ, et al. Vector design influences hepatic genotoxicity after adeno-associated virus gene therapy. J Clin Invest. 2015;125(1):132-140. https://www.jci.org/articles/view/79213 ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wang JH, et al. Adeno-associated virus as a delivery vector for gene therapy of human diseases. Signal Transduction and Targeted Therapy. 2024;9(1):97. https://pubmed.ncbi.nlm.nih.gov/38565561/ ↩︎
Macip CC, et al. Gene Therapy-Mediated Partial Reprogramming Extends Lifespan and Reverses Age-Related Changes in Aged Mice. Cellular Reprogramming. 2024;26(1):1-14. https://pubmed.ncbi.nlm.nih.gov/38381405/ ↩︎
Povedano JM, et al. Therapeutic effects of telomerase in mice with pulmonary fibrosis induced by damage to the lungs and short telomeres. eLife. 2018;7:e31299. https://pmc.ncbi.nlm.nih.gov/articles/PMC5818250/ ↩︎ ↩︎
Mendell JR, et al. A phase 1/2a follistatin gene therapy trial for Becker muscular dystrophy. Mol Ther. 2015;23(1):192-201. https://pubmed.ncbi.nlm.nih.gov/25322757/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Mendell JR, et al. Follistatin Gene Therapy for Sporadic Inclusion Body Myositis Improves Functional Outcomes. Mol Ther. 2017;25(4):856-865. https://pubmed.ncbi.nlm.nih.gov/28279643/ ↩︎ ↩︎ ↩︎
Roig-Soriano J, et al. AAV-mediated expression of secreted and transmembrane αKlotho isoforms rescues relevant aging hallmarks in senescent SAMP8 mice. Aging Cell. 2022;21(4):e13578. https://pubmed.ncbi.nlm.nih.gov/35274439/ ↩︎ ↩︎
Safety and Efficacy of Injectable Klotho Plasmid Gene Therapy in Humans. ClinicalTrials.gov. NCT07216781. Registered: February 2026. https://clinicaltrials.gov/study/NCT07216781 ↩︎ ↩︎ ↩︎
Gallardo MD, et al. Oct4, Sox2, Klf4, c-My (OSKM) gene therapy in the hypothalamus prolongs fertility and ovulation in female rats. Aging. 2025;17(3). https://pubmed.ncbi.nlm.nih.gov/39864409/ ↩︎
Horvath S, et al. Cognitive rejuvenation in old rats by hippocampal OSKM gene therapy. GeroScience. 2025;47(1):119-136. https://pubmed.ncbi.nlm.nih.gov/39037528/ ↩︎ ↩︎
Nath A, et al. Towards a context-aware framework for cellular senescence. Biogerontology. 2026. https://pubmed.ncbi.nlm.nih.gov/42089944/ ↩︎ ↩︎ ↩︎
Ocampo A, et al. In Vivo Amelioration of Age-Associated Hallmarks by Partial Reprogramming. Cell. 2016;167(7):1719-1733. https://pubmed.ncbi.nlm.nih.gov/27984723/ ↩︎ ↩︎ ↩︎
Flory E, et al. Medicinal Products Based on Adeno-Associated Viral Vectors: A Regulatory Perspective on the Potential Risk of Insertion-Mediated Tumorigenesis. Hum Gene Ther. 2025;36(21-22):1201-1209. https://pubmed.ncbi.nlm.nih.gov/40789645/ ↩︎ ↩︎ ↩︎ ↩︎
Kasimsetty A, et al. Integration and the risk of liver cancer-Is there a real risk? J Viral Hepat. 2024;31(4):e14013. https://pubmed.ncbi.nlm.nih.gov/38606944/ ↩︎ ↩︎
Sverdlov V, et al. rAAV immunogenicity, toxicity, and durability in 255 clinical trials: A meta-analysis. Front Immunol. 2022;13:1001263. https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2022.1001263/full ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Suoranta T, et al. Strategies to improve safety profile of AAV vectors. Front Mol Med. 2022;2:1049580. https://pubmed.ncbi.nlm.nih.gov/39086961/ ↩︎
Penaud-Budloo M, et al. Characterization of residual microRNAs in AAV vector batches produced in HEK293 mammalian cells and Sf9 insect cells. Mol Ther Methods Clin Dev. 2024;35:101382. https://pubmed.ncbi.nlm.nih.gov/39220637/ ↩︎ ↩︎
Piccolo P, et al. Current and Emerging Issues in Adeno-Associated Virus Vector-Mediated Liver-Directed Gene Therapy. Hum Gene Ther. 2025;36(3-4):195-204. https://pubmed.ncbi.nlm.nih.gov/39714937/ ↩︎ ↩︎
U.S. FDA. FDA warns against receiving young donor plasma infusions that are promoted as unproven treatments. 2019. https://www.fda.gov/news-events/press-announcements/fda-warns-against-receiving-young-donor-plasma-infusions ↩︎ ↩︎ ↩︎