¶ Frontier Longevity Contraindications
This guide provides a comprehensive, evidence-based overview of safety considerations, contraindications, and potential drug/supplement interactions for frontier longevity interventions. As these cutting-edge therapies advance, understanding their risk profiles is crucial for clinical education and professional reference.
| Type | Advanced Therapies, Supplements |
| Key Risks | Oncogenesis, Immunogenicity, Toxicity |
| Interaction Level | High (Pharmacokinetic & Pharmacodynamic) |
| Evidence Quality | Moderate (Emerging Clinical Data) |
¶ At a glance
Key points (high-level summary)
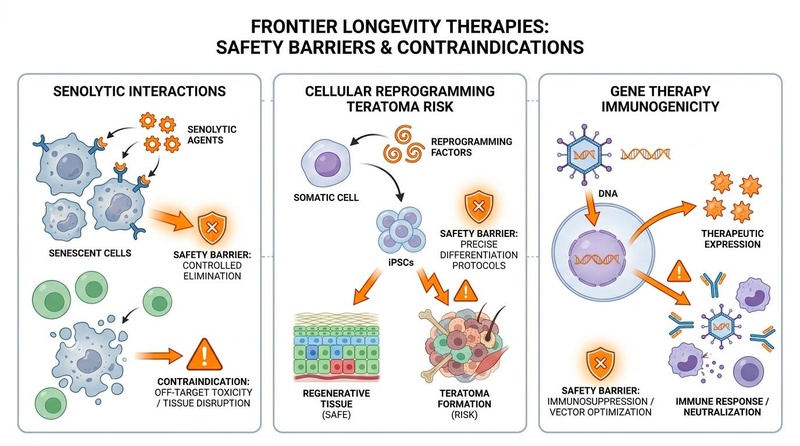
- Cellular Reprogramming: Potential for teratoma formation and oncogenic risk, necessitating strict control over Yamanaka factor expression[1][2].
- MicroRNA Therapies: Early clinical trials (e.g., MRX34) faced significant immune-mediated adverse events, including cytokine release syndrome, hepatotoxicity, and fatalities, highlighting delivery system (LNP) and off-target challenges[3].
- Gene Therapy: Risks include immunogenicity (neutralizing antibodies), hepatotoxicity, thrombotic microangiopathy (TMA), and insertional mutagenesis[4][5].
- Senolytics (Dasatinib, Quercetin, Fisetin): Generally well-tolerated in intermittent doses, but Dasatinib carries risks of myelosuppression, bleeding (antiplatelet effects), fluid retention (pleural effusion), and CYP3A4 interactions[6][7]. Fisetin shows a favorable safety profile with mild GI upset[8][9].
- Cryonics & Vitrification: Primary concerns are cryoprotectant toxicity, osmotic damage, blood-brain barrier disruption, and injury from post-mortem cold ischemia prior to vitrification[10][11].
What people use it for
- Main goals: Addressing fundamental aging mechanisms, disease reversal, healthspan extension.
- Evidence quality (overall): Moderate (based on a mix of preclinical, early human trials, and meta-analyses, with ongoing safety monitoring).
¶ What are the main safety concerns?
The safety landscape for frontier longevity interventions is complex, involving both known pharmacological risks and novel biological challenges.
¶ Cellular Reprogramming
The use of Yamanaka factors (Oct4, Sox2, Klf4, c-Myc, or OSKM) for partial cellular reprogramming carries inherent risks. The primary concern is the potential for teratoma formation (benign tumors with various tissue types) or inducing other neoplastic transformations due to the pro-oncogenic nature of these factors, particularly c-Myc[1:1][2:1][12]. Strategies to mitigate this include transient expression protocols and precise epigenetic control.
¶ MicroRNA (miRNA) Therapies
Early clinical experiences, such as with MRX34 (a liposomal miR-34a mimic), have highlighted significant safety hurdles. The Phase I trial for MRX34 was halted due to multiple fatal immune-mediated serious adverse events, including cytokine release syndrome, systemic inflammatory response syndrome, and hepatic failure[3:1]. These events underscore the challenges related to systemic delivery (e.g., lipid nanoparticle toxicity) and potential off-target effects of miRNAs.
¶ Gene Therapy (Adeno-Associated Virus - AAV Vectors)
While AAV vectors are a popular choice for in vivo gene delivery due to their low immunogenicity compared to other viral vectors, they are not without risks. Key safety concerns include:
- Immunogenicity: Host immune responses against the AAV capsid or transgene product can lead to neutralizing antibodies, limiting efficacy and potentially causing inflammatory reactions[4:1][5:1].
- Hepatotoxicity: Elevated liver enzymes (transaminasemia) is a common adverse event, sometimes leading to acute liver injury, especially with higher vector doses[4:2][13][14].
- Thrombotic Microangiopathy (TMA): A serious, albeit rare, complication involving microvascular injury and organ damage[4:3].
- Insertional Mutagenesis: Although rare with AAVs due to their generally non-integrating nature, there's a theoretical risk of viral DNA integrating into the host genome, potentially activating oncogenes or disrupting tumor suppressor genes[5:2][15].
¶ Senolytics (Dasatinib, Quercetin, Fisetin)
Senolytics are a class of drugs designed to selectively induce apoptosis in senescent cells.
- Dasatinib: A tyrosine kinase inhibitor, Dasatinib is associated with risks of myelosuppression (reduced blood cell production), fluid retention (e.g., pleural effusions), and gastrointestinal disturbances. It also inhibits platelet function, increasing bleeding risk, and is metabolized by CYP3A4, leading to numerous drug interactions[7:1][16].
- Quercetin: Generally considered safe, but high doses can cause gastrointestinal upset and may interact with CYP3A4 and P-glycoprotein, affecting drug metabolism[17].
- Fisetin: Human trials with Fisetin (up to 200 mg/day) have shown a favorable safety profile with mild and transient gastrointestinal side effects. It has mild anticoagulant and antiplatelet effects, requiring caution in those on blood thinners[8:1][9:1].
¶ Cryonics
Cryonics involves cryopreserving legally dead individuals with the hope of future reanimation. The primary safety concerns revolve around preventing cellular damage during vitrification:
- Cryoprotectant Toxicity: The high concentrations of cryoprotective agents (CPAs) required for vitrification are inherently toxic to cells, causing osmotic stress, dehydration, and direct chemical damage[10:1][11:1].
- Blood-Brain Barrier Disruption: The blood-brain barrier is susceptible to damage during cryopreservation, which can exacerbate osmotic injury and impair brain recovery[11:2].
- Ischemic Injury: Damage caused by lack of oxygen and blood flow (ischemia) that occurs between clinical death and the start of cryopreservation procedures significantly impacts tissue viability and complicates subsequent repair[10:2].
¶ Evidence summary table (key safety outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, intervention, key adverse events) |
|---|---|---|---|---|---|
| Teratoma Formation (Cellular Reprogramming) | High | Low | Preclinical/Case Rpts | Induced by uncontrolled Yamanaka factor expression in vivo[1:2][2:2] | |
| Immune-Mediated SAEs (miRNA Therapies) | High | Moderate | 1 Phase I | Fatal cytokine storm, hepatotoxicity with MRX34[3:2] | |
| Hepatotoxicity (AAV Gene Therapy) | High | Moderate | Meta-analysis 255 Trials | Transaminasemia, acute liver injury with high-dose AAV[4:4] | |
| Myelosuppression (Dasatinib) | High | High | Multiple RCTs | Thrombocytopenia, neutropenia; dose-dependent in cancer pts[7:2] | |
| Bleeding Risk (Dasatinib) | High | High | Multiple RCTs | Platelet dysfunction, synergistic with anticoagulants[7:3] | |
| Pleural Effusion (Dasatinib) | High | High | Multiple RCTs | Fluid retention, can be severe; dose-dependent[7:4][16:1] | |
| Cryoprotectant Toxicity (Cryonics) | High | Preclinical/Obs | Osmotic shock, chemical damage during vitrification[10:3][11:3] |
- *Effect: Compact renderer encoding:
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree).
- ***Trials: Number of RCTs or total trials informing this outcome.
¶ Drug and supplement interactions
Frontier longevity interventions, especially those involving pharmacological agents or genetic modifications, can have significant interactions.
¶ Pharmacokinetic Interactions (Drug Metabolism)
- CYP3A4 Inhibitors/Inducers: Many longevity compounds (e.g., Dasatinib, some senolytics) are metabolized by or inhibit cytochrome P450 enzymes, particularly CYP3A4. Concomitant use with strong inhibitors (e.g., ketoconazole, grapefruit juice) can increase drug levels and toxicity, while inducers (e.g., rifampin, St. John's wort) can decrease efficacy[7:5][17:1].
- P-glycoprotein (P-gp) Modulators: P-gp is an efflux pump that affects the absorption and elimination of many drugs. Some senolytics (e.g., Quercetin, Fisetin) can modulate P-gp, potentially altering the pharmacokinetics of co-administered medications[17:2].
¶ Pharmacodynamic Interactions (Additive Effects)
- Anticoagulants/Antiplatelets: Senolytics like Dasatinib and Fisetin possess antiplatelet properties. Combining them with prescription anticoagulants (e.g., warfarin, clopidogrel) can increase the risk of bleeding[7:6].
- Immunosuppressants: Gene therapies or cellular reprogramming strategies might involve immunosuppression to mitigate immune responses. Co-administration of other immunosuppressants requires careful monitoring to prevent excessive immune suppression and infection risk[5:3].
- Hypoglycemic Agents: Some longevity compounds (e.g., Metformin, certain senolytics) can affect glucose metabolism. Combining them with insulin or oral hypoglycemics may potentiate their effects, increasing the risk of hypoglycemia.
¶ Who should be especially cautious or avoid these interventions?
- Pregnancy & Breastfeeding: Due to a lack of safety data and potential developmental risks, these interventions are generally contraindicated.
- Active Malignancy: Cellular reprogramming, with its oncogenic potential, and some gene therapies are contraindicated in patients with active cancers or a high risk of malignancy[1:3].
- Severe Organ Impairment: Individuals with significant cardiac, renal, or hepatic impairment are at higher risk for adverse events from interventions that affect fluid balance (Dasatinib), drug metabolism (senolytics, gene therapy), or immune function (miRNA, gene therapy)[4:5][7:7].
- Autoimmune Disorders: Interventions that modulate the immune system (e.g., some gene therapies, miRNA therapies) require extreme caution in patients with autoimmune conditions due to the risk of exacerbating the disease or triggering immune-related adverse events.
- Pre-existing Neutralizing Antibodies: Patients with pre-existing neutralizing antibodies to AAV vectors may not be candidates for AAV-based gene therapies due to reduced efficacy and increased risk of immune reactions[5:4].
- Coagulopathies: Individuals with bleeding disorders or those on anticoagulant therapy should exercise extreme caution or avoid interventions with antiplatelet effects (e.g., Dasatinib, Fisetin)[7:8].
¶ Practical questions (FAQ)
What is the primary safety concern for cellular reprogramming?
Why was the MRX34 microRNA trial halted?
The MRX34 (miR-34a mimic) Phase I clinical trial was halted due to multiple fatal immune-mediated serious adverse events, including cytokine release syndrome, systemic inflammatory response syndrome, and hepatic failure, indicating significant toxicity issues with the liposomal delivery system and/or the miRNA itself[3:3].
What are the biggest risks with AAV gene therapy?
Are senolytics always safe?
While many senolytics like Fisetin have favorable safety profiles, the combination of Dasatinib and Quercetin (D+Q) involves Dasatinib, which has a more significant risk profile, including myelosuppression, bleeding risk, fluid retention, and numerous drug interactions, even in intermittent senolytic dosing regimens[6:1][7:9].
What are the main challenges for cryonics safety?
¶ How we evaluated the evidence
- Study types prioritized: Randomized controlled trials (RCTs) and systematic reviews for senolytics; Phase I/II clinical trial reports and meta-analyses for gene and miRNA therapies; preclinical and theoretical analyses for cellular reprogramming and cryonics.
- How we graded evidence quality:
- High: Multiple high-quality RCTs or meta-analyses with consistent results.
- Moderate: Single high-quality RCT, multiple smaller RCTs with consistent signals, or comprehensive meta-analyses of preclinical safety data.
- Low: Phase I trials with significant adverse events, observational data, case reports, or primarily preclinical mechanistic studies.
- Very low: Primarily theoretical risks, in vitro data, or very early animal studies.
- Focus: Emphasis on human clinical trial data for safety outcomes where available, supplemented by robust preclinical evidence for emerging modalities where human data are sparse.
¶ References
Paine MJ, et al. Partial cellular reprogramming: A deep dive into an emerging rejuvenation technology. Aging Cell. 2024;23(2):e14039. https://pmc.ncbi.nlm.nih.gov/articles/PMC10861195/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Jo K, et al. Organ‐Specific Dedifferentiation and Epigenetic Remodeling in In Vivo Reprogramming. Aging Cell. 2025;24(1):e14168. https://pmc.ncbi.nlm.nih.gov/articles/PMC12610414/ ↩︎ ↩︎ ↩︎ ↩︎
Hong DS, et al. Phase 1 study of MRX34, a liposomal miR-34a mimic, in patients with advanced solid tumours. British Journal of Cancer. 2020;122(7):979-986. https://pmc.ncbi.nlm.nih.gov/articles/PMC7251107/ ↩︎ ↩︎ ↩︎ ↩︎
Sverdlov V, et al. rAAV immunogenicity, toxicity, and durability in 255 clinical trials: A meta-analysis. Frontiers in Immunology. 2022;13:1001263. https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2022.1001263/full ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Colella P, et al. Emerging Issues in AAV-Mediated In Vivo Gene Therapy. Gene Therapy. 2018;25(5):299-305. https://pmc.ncbi.nlm.nih.gov/articles/PMC5758940/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Nambiar AM, et al. Senolytics dasatinib and quercetin in idiopathic pulmonary fibrosis: results from a phase I, single-blind, single-center, randomized, placebo-controlled pilot trial on feasibility and tolerability. eBioMedicine. 2023;90:104523. https://www.thelancet.com/journals/ebiom/article/PIIS2352-3964(23)00046-4/fulltext ↩︎ ↩︎
Dasatinib Prescribing Information. FDA. 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/216099s004lbl.pdf ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Alipour M, et al. 12‑weeks fisetin supplementation and interval resistance with aerobic training: changes in Maresin‑1 and inflammatory markers in men with obesity: a randomized controlled trial. Journal of the International Society of Sports Nutrition. 2026;23(1):2679718. https://doi.org/10.1080/15502783.2026.2679718 ↩︎ ↩︎
Wang L, et al. Fisetin Prolongs Therapy Window of Brain Ischemic Stroke Using Tissue Plasminogen Activator: A Double-Blind Randomized Placebo-Controlled Clinical Trial. Clinical and Applied Thrombosis/Hemostasis. 2019;25:1076029619871359. https://doi.org/10.1177/1076029619871359 ↩︎ ↩︎
Best BP. Scientific Justification of Cryonics Practice. Rejuvenation Research. 2016;19(6):533-537. https://pmc.ncbi.nlm.nih.gov/articles/PMC4733321/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
McIntyre RL, et al. Aldehyde-stabilized cryopreservation. Cryobiology. 2015;71(2):292-298. https://www.sciencedirect.com/science/article/pii/S001122401500245X ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Yamada H, et al. In Vivo Reprogramming Highlights Epigenetic Regulation That Shapes Cancer Hallmarks. Cancer Science. 2025;116(1):17-27. https://onlinelibrary.wiley.com/doi/10.1111/cas.70067 ↩︎
Nathwani AC, et al. Sustained Factor IX expression after gene therapy for hemophilia B. New England Journal of Medicine. 2011;365(10):875-885. https://www.nejm.org/doi/full/10.1056/NEJMoa1103205 ↩︎
Piening BD, et al. Liver-directed gene therapy with an adeno-associated virus vector in a patient with ornithine transcarbamylase deficiency. Gene Therapy. 2014;21(7):643-646. https://pubmed.ncbi.nlm.nih.gov/24806877/ ↩︎
Vandenberghe LH, et al. AAV vector-mediated gene therapy for the central nervous system. Annual Review of Neuroscience. 2010;33:107-128. https://pubmed.ncbi.nlm.nih.gov/20350170/ ↩︎
Cortes JE, et al. Dasatinib in patients with chronic myeloid leukemia in accelerated phase after imatinib failure. Journal of Clinical Oncology. 2007;25(16):2263-2270. https://ascopubs.org/doi/10.1200/JCO.2006.09.4057 ↩︎ ↩︎
Chen X, et al. Effects of quercetin on the pharmacokinetics of drugs. Molecules. 2019;24(16):2912. https://pmc.ncbi.nlm.nih.gov/articles/PMC6720277/ ↩︎ ↩︎ ↩︎