¶ Leaky Gut (Intestinal Permeability)
Increased intestinal permeability, colloquially referred to as "leaky gut," is a medically recognized pathophysiological state characterized by the compromise of the mucosal barrier's tight junction complexes. This structural defect allows the uncontrolled, paracellular translocation of luminal antigens—including dietary proteins, pathogenic microbes, and lipopolysaccharide (LPS) endotoxins—directly into the lamina propria and portal circulation. Once in the systemic environment, these molecules trigger localized and systemic immune activation, contributing to chronic low-grade inflammation, metabolic dysfunction, and autoimmune processes.
¶ At a Glance
¶ Key Points
- Physiological Entity: Clinical gastroenterology distinguishes between the pseudoscientific "leaky gut syndrome" (claimed to cause all chronic diseases) and "increased intestinal permeability" (a measurable, transient, or chronic structural impairment associated with specific inflammatory conditions) [1][2].
- Core Triggers: The primary triggers of tight junction disassembly are dietary gliadin (gluten), non-steroidal anti-inflammatory drugs (NSAIDs), ethanol (alcohol), and chronic psychophysiological stress.
- Biomarker Profile: Clinically monitored through serum lipopolysaccharide-binding protein (LBP), fecal calprotectin, the urinary lactulose/mannitol ratio, and selectively via fecal zonulin (though zonulin measurements remain subject to clinical debate regarding baseline variability).
- Therapeutic Core: Reversing barrier compromise requires removing dietary/chemical triggers, followed by targeted supplementation with enterocyte fuels (L-Glutamine), mucosal protectors (Zinc L-Carnosine), and metabolic regulators (butyrate, specific probiotics).
¶ What is Intestinal Permeability?
Under physiological conditions, the gut barrier utilizes a selectively permeable, single-cell epithelial layer to control nutrient absorption while excluding larger macromolecules. In a healthy state, molecules pass through the epithelial cells via transcellular pathways regulated by active transporters.
In contrast, increased intestinal permeability is a defect of the paracellular pathway—the microscopic gaps between adjacent epithelial cells. Think of the gut lining as a highly selective mesh sieve. Under normal circumstances, the mesh is tightly woven, allowing only water and dissolved micronutrients to slip through. When the barrier is compromised, the "threads" of the mesh are pulled apart, allowing larger, immunogenic particles to cross the epithelial monolayer unchecked.
¶ Pathophysiology & Triggers of Dysfunction
The compromise of the gut barrier occurs through distinct, well-documented molecular pathways triggered by external exposures.
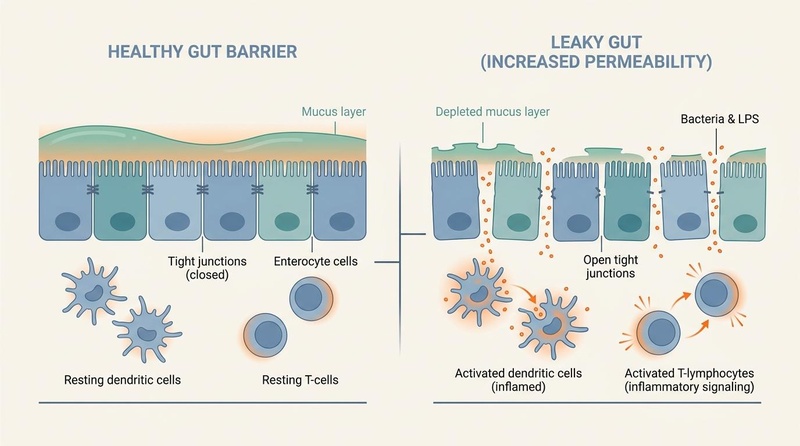
Figure 1: Healthy Intestinal Barrier vs. Increased Intestinal Permeability (Leaky Gut). On the left, tight junctions seal the paracellular space and a thick mucus layer repels pathogens. On the right, depleted mucus, gluten/gliadin, or dysbiosis breaks down tight junctions, allowing lipopolysaccharides (LPS) and food antigens to translocate and trigger immune activation.
¶ 1. Gluten and Gliadin (CXCR3 Pathway)
In all humans—not just those with celiac disease—the ingestion of gluten-containing grains releases gliadin, a highly indigestible glycoprotein.
- Receptor Binding: Gliadin binds directly to the chemokine receptor CXCR3 on the apical membrane of enterocytes [3][4].
- MyD88 Activation: This binding initiates a MyD88-dependent intracellular signaling cascade that triggers the synthesis and apical exocytosis of zonulin [3:1][5].
- Tight Junction Disassembly: Secreted zonulin binds back to its receptors (EGFR and PAR2) on the enterocyte surface. This activates phospholipase C (PLC) and protein kinase C (PKC), which polymerize actin microfilaments. This cytoskeletal contraction pulls the scaffolding protein ZO-1 away from claudins and occludin, physically opening the tight junction pore [1:1][6].
¶ 2. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Common NSAIDs (e.g., indomethacin, ibuprofen, naproxen) disrupt the gut barrier via three distinct mechanisms:
- Prostaglandin Depletion: By inhibiting the cyclooxygenase (COX-1 and COX-2) enzymes, NSAIDs deplete mucosal prostaglandins ( and ), which are critical for stimulating bicarbonate and mucus secretion and maintaining mucosal blood flow.
- Direct Mitochondrial Injury: NSAIDs are weak organic acids that uncouple mitochondrial oxidative phosphorylation in enterocytes. This depletes cellular ATP, directly disabling the energy-dependent actomyosin cytoskeleton required to maintain tight junction tension [7].
- Topical Irritation: Direct contact of NSAID molecules with the mucosal lining leads to local cellular sloughing and micro-ulceration.
¶ 3. Ethanol & Acetaldehyde
Alcohol ingestion induces rapid, transient barrier disruption:
- Direct Cytotoxicity: Ethanol acts as a local solvent, solubilizing the lipid membranes of enterocytes and degrading the protective mucus bilayer.
- Acetaldehyde Metabolism: Intestinal alcohol dehydrogenase converts ethanol into acetaldehyde, which directly induces the phosphorylation of occludin and E-cadherin, causing them to internalize and dissolve from the junctional complex.
- Endotoxemic Cycle: Ethanol promotes the overgrowth of Gram-negative luminal bacteria, increasing the local concentration of lipopolysaccharides (LPS) that can translocate through the newly opened gaps.
¶ 4. Stress and Mast Cell Degranulation
Chronic psychophysiological stress drives barrier failure via the brain-gut axis:
- CRH Release: Stress triggers the hypothalamic-pituitary-adrenal (HPA) axis, releasing corticotropin-releasing hormone (CRH) both centrally and locally in the gut mucosa.
- Mast Cell Activation: Mucosal mast cells express high levels of CRH receptors ( and ). Activation of these receptors causes mast cells to degranulate, releasing pre-formed inflammatory mediators, including histamine, tumor necrosis factor-alpha (TNF-α), and tryptase.
- Junction Cleavage: Mast cell tryptase directly cleaves protease-activated receptors on enterocytes, triggering the internalization of ZO-1 and occludin, while TNF-α upregulates MLCK (myosin light-chain kinase), which physically contracts the perijunctional actomyosin ring, opening the barrier.
¶ Evidence Summary Table (Human Outcomes)
The clinical evidence for reversing increased intestinal permeability is highly compound-specific. The table below represents evaluated human outcomes for major barrier-targeted interventions.
| Intervention | Typical Dose | Primary Target | Efficacy* | Evidence Quality | Key Trials & Context |
|---|---|---|---|---|---|
| L-Glutamine | 5–15 g / day | Enterocyte mitochondrial fuel; mTOR activation | Moderate | Demonstrated to significantly lower urinary lactulose/mannitol ratio and improve gastrointestinal symptoms in post-infectious IBS-D [8][9]. | |
| Zinc L-Carnosine | 75–150 mg / day | HSP72 induction; mucosal stabilization | Moderate | Truncates exercise-induced and NSAID-induced increases in intestinal permeability in controlled human crossover trials [7:1][10][11]. | |
| Butyrate / Tributyrin | 1–3 g / day | AMPK activation; hypoxia maintenance | Moderate | SCFA administration protects mucosal architecture, lowers systemic inflammation, and suppresses uremic toxin translocation [12][13]. | |
| Multi-strain Probiotics | 10–50 Billion CFU | Colonization resistance; TJ upregulation | Moderate | Custom Lactobacillus and Bifidobacterium formulations significantly reduce zonulin levels and lower systemic oxidative stress [14][15]. | |
| Slippery Elm (Ulmus rubra) | 500–1,500 mg / day | Demulcent coating; prebiotic substrate | Low | Primarily historical and clinical consensus; acts as a protective mucilage and fermentable substrate for SCFA production [2:1]. |
¶ Mechanistic Breakdown of Key Interventions
¶ 1. L-Glutamine: The Cellular Fuel
L-Glutamine is the most abundant free amino acid in the human body and the primary metabolic fuel for rapidly dividing enterocytes.
- Mitochondrial Respiration: Enterocytes utilize glutamine at a high rate to produce ATP via glutaminolysis, supporting the high-energy demands of constant cell division and active nutrient transport.
- mTOR Pathway Activation: Glutamine acts as a direct signaling molecule that activates the mTORC1 pathway. This upregulates the translation and assembly of tight junction proteins, specifically increasing the expression of ZO-1, Occludin, and Claudin-1 [8:1].
- Anti-apoptotic Effect: During states of heat, physical, or inflammatory stress, glutamine prevents cellular apoptosis by suppressing the activation of caspase-3 and upregulating protective heat shock proteins.
¶ 2. Zinc L-Carnosine (Polaprezinc): The Mucosal Stabilizer
Zinc L-Carnosine is a polymeric chelate compound of zinc and L-carnosine that dissociates in the gut at a slow, controlled rate, allowing it to adhere selectively to damaged mucosal tissues.
- HSP72 Induction: It strongly induces the expression of Heat Shock Protein 72 (HSP72), which folds damaged cellular proteins and protects enterocytes from thermal, chemical, and physical stressors [11:1][16].
- Antioxidant & Zinc Delivery: Delivers elemental zinc directly to the mucosa, where zinc acts as a mandatory cofactor for over 300 enzymes, including those involved in DNA repair and cellular migration (re-epithelialization) [17].
- Inhibition of MLCK: Prevents the upregulation of Myosin Light-Chain Kinase (MLCK), effectively blocking the cytoskeletal contraction that pulls tight junctions apart in response to inflammatory cytokines (like TNF-α) [7:2].
¶ 3. Butyrate & Tributyrin: The Metabolic Rheostat
Butyrate is a short-chain fatty acid produced by the microbial fermentation of dietary fibers. Tributyrin is a prodrug of butyrate consisting of three butyrate molecules bound to glycerol, offering superior bioavailability and delivery to both the small and large intestines.
- AMPK Activation: Butyrate activates AMP-activated protein kinase (AMPK), which coordinates the rapid assembly of tight junction proteins into the cell membrane.
- Oxygen Consumption & Hypoxia: Fermentation of butyrate by enterocytes consumes large amounts of oxygen via beta-oxidation. This maintains a state of physiological "physioxia" (near-anoxia) at the epithelial surface, which is critical for stabilizing the transcription factor Hypoxia-Inducible Factor-1 alpha (HIF-1α), a master upregulator of barrier protection genes.
¶ Clinical Protocols for Gut Barrier Repair
Reversing compromised gut permeability requires a structured, phase-based clinical protocol to eliminate destabilizing triggers before introducing restorative substrates.
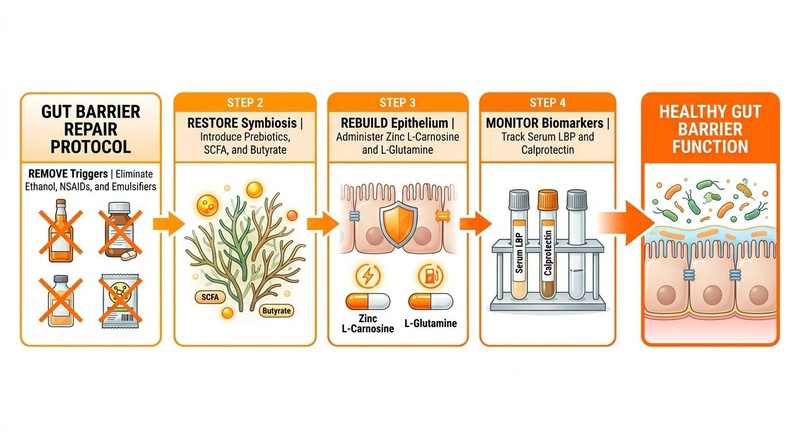
Figure 2: The Four-Phase Clinical Pathway for Gut Barrier Repair. This structured framework covers removing barrier-disrupting triggers, restoring metabolic and microbial inputs, rebuilding structural junction integrity, and monitoring progression via validated biomarkers.
¶ Phase 1: Remove (Weeks 1–4)
The absolute prerequisite for barrier repair is the strict elimination of known tight junction disruptors.
- Chemical Triggers: Stop all unnecessary over-the-counter NSAIDs (substitute with acetaminophen or alternative pain management strategies as clinically appropriate). Eliminate all ethanol (alcohol) intake.
- Dietary Triggers: Eliminate ultra-processed foods containing emulsifiers (such as polysorbate-80 and carboxymethylcellulose) which directly degrade the mucus layer. Temporary gluten/gliadin restriction may be clinically indicated for sensitive individuals or those with suspected non-celiac gluten sensitivity (NCGS) to downregulate CXCR3-mediated zonulin release [3:2][4:1], but is not universally required for all patients.
¶ Phase 2: Rebuild & Support (Weeks 1–8)
Simultaneously introduce structural support compounds to fuel enterocytes and stabilize junctional complexes.
- L-Glutamine: Take 5 grams of pure L-glutamine powder dissolved in room-temperature water, 2 to 3 times daily, on an empty stomach (30 minutes before meals) [9:1].
- Zinc L-Carnosine: Take 75 mg (providing approximately 16 mg of elemental zinc) twice daily, immediately after breakfast and before bed [7:3][11:2].
¶ Phase 3: Restore & Ferment (Weeks 5–12)
Once the acute structural repair phase is established, introduce microbial and metabolic inputs to restore the outer barrier layers.
- Tributyrin: Take 1,000 mg once daily with meals to provide a steady supply of butyrate to the enterocytes.
- Targeted Probiotics: Supplement with a high-potency, multi-strain probiotic containing clinically validated strains of Lactobacillus rhamnosus GG, Lactobacillus acidophilus, and Bifidobacterium lactis (10 to 50 Billion CFU daily with breakfast) [14:1][15:1].
- Demulcents: Take 500 to 1,000 mg of Slippery Elm bark powder mixed into warm water before meals to provide a soothing mucilage layer and prebiotic substrate [2:2].
¶ Phase 4: Monitor & Validate (Ongoing)
Establish baseline markers before starting Phase 1, and re-test at Week 12 to confirm barrier restoration.
- Serum LBP & Calprotectin: Monitor for a downward trend, confirming a reduction in systemic bacterial translocation and mucosal inflammation [18].
- Fecal Zonulin: Optionally monitor for a reduction back to reference ranges (), noting its clinical controversy and baseline variability compared to more stable biomarkers.
¶ Safety, Interactions, & Red Flags
¶ Dosage Safety & Contraindications
- High-Dose L-Glutamine: While highly tolerated, chronic daily doses exceeding 20–30g should be avoided. Glutamine is metabolized into glutamate and ammonia. Individuals with severe liver disease, renal impairment, or urea cycle disorders must avoid high-dose glutamine due to the risk of hyperammonemia. Patients with bipolar disorder should exercise caution, as glutamine may trigger manic episodes.
- Zinc Toxicity: Prolonged intake of Zinc L-Carnosine at high doses (exceeding 150 mg of the chelate, or ~32 mg of elemental zinc daily) for more than 12 weeks must be balanced with low-dose copper supplementation (1–2 mg daily) to prevent zinc-induced copper deficiency, which can manifest as microcytic anemia or myeloneuropathy [17:1].
¶ Potential Interactions
- Antibiotics: Zinc L-Carnosine may chelate with certain antibiotics (such as quinolones and tetracyclines), reducing their absorption. Space administration by at least 2 hours.
¶ Practical FAQ
How long does it take for the gut barrier to repair?
Because intestinal epithelial cells have an exceptionally rapid turnover rate (completely replacing themselves every 3 to 5 days), acute structural repair can begin within weeks of removing triggers. However, resolving chronic mucosal inflammation, restoring the mucus layer, and re-establishing microbial symbiosis typically requires 8 to 12 weeks of continuous compliance with a structured protocol.
Is gut barrier repair useful if I am otherwise healthy?
Yes, particularly for endurance athletes and individuals exposed to high heat or physiological stress. Strenuous exercise shifts blood flow away from the GI tract (splanchnic hypoperfusion), causing local hypoxia and rapid barrier compromise (exercise-induced leaky gut) [19]. Human trials show that supplementing with Zinc L-Carnosine prevents this exercise-induced increase in gut permeability, protecting against post-workout systemic inflammation and gastrointestinal distress [10:1].
Can I use collagen peptides instead of L-glutamine?
While collagen is rich in glycine and proline—which support connective tissues—it does not serve as a direct energy source for enterocytes like L-glutamine does. For targeted, high-energy repair of the epithelial monolayer and activation of the mTOR pathway, L-glutamine remains the primary clinically validated choice [8:2][9:2]. Collagen can be used as a secondary, supporting protein source.
¶ References
Fasano, A. (2020). "All disease begins in the (leaky) gut: role of zonulin-mediated gut permeability in the pathogenesis of some chronic inflammatory diseases." F1000Research, 9, F1000 Faculty Rev-98. https://pubmed.ncbi.nlm.nih.gov/32051759/ ↩︎ ↩︎
Camilleri, M. (2021). "Human Intestinal Barrier: Effects of Stressors, Diet, Prebiotics, and Probiotics." Clinical and Translational Gastroenterology, 12(1), e00308. https://pubmed.ncbi.nlm.nih.gov/33492118/ ↩︎ ↩︎ ↩︎
Lammers, K. M., et al. (2008). "Gliadin induces an increase in intestinal permeability and zonulin release by binding to the chemokine receptor CXCR3." Gastroenterology, 135(1), 194-204. https://pubmed.ncbi.nlm.nih.gov/18485912/ ↩︎ ↩︎ ↩︎
Lauxmann, M. A., et al. (2021). "From celiac disease to coccidia infection and vice-versa: The polyQ peptide CXCR3-interaction axis." BioEssays, 43(12), e2100140. https://pubmed.ncbi.nlm.nih.gov/34705290/ ↩︎ ↩︎
Troisi, J., et al. (2021). "The Therapeutic use of the Zonulin Inhibitor AT-1001 (Larazotide) for a Variety of Acute and Chronic Inflammatory Diseases." Current Medicinal Chemistry, 28(15), 2950-2962. https://pubmed.ncbi.nlm.nih.gov/33397225/ ↩︎
Menegotte, P. C. D. S., et al. (2026). "Effects of different intensities of aerobic exercise on intestinal permeability and inflammatory response in older adults: Randomized clinical trial." Experimental Gerontology, 178, 112230. https://pubmed.ncbi.nlm.nih.gov/42372927/ ↩︎
Mahmood, A., et al. (2007). "Zinc carnosine, a health food supplement that stabilises small bowel integrity and stimulates gut repair processes." Gut, 56(2), 168-175. https://pubmed.ncbi.nlm.nih.gov/16777920/ ↩︎ ↩︎ ↩︎ ↩︎
Abbasi, F., et al. (2024). "A systematic review and meta-analysis of clinical trials on the effects of glutamine supplementation on gut permeability in adults." Amino Acids, 56(1), 78. https://pubmed.ncbi.nlm.nih.gov/39397201/ ↩︎ ↩︎ ↩︎
Zhou, Q., et al. (2019). "Randomised placebo-controlled trial of dietary glutamine supplements for postinfectious irritable bowel syndrome." Gut, 68(6), 996-1002. https://pubmed.ncbi.nlm.nih.gov/30108163/ ↩︎ ↩︎ ↩︎
Davison, G., et al. (2016). "Zinc carnosine works with bovine colostrum in truncating heavy exercise-induced increase in gut permeability in healthy volunteers." The American Journal of Clinical Nutrition, 104(2), 526-536. https://pubmed.ncbi.nlm.nih.gov/27357095/ ↩︎ ↩︎
Efthymakis, K., & Neri, M. (2022). "The role of Zinc L-Carnosine in the prevention and treatment of gastrointestinal mucosal disease in humans: a review." Clinics and Research in Hepatology and Gastroenterology, 46(7), 101951. https://pubmed.ncbi.nlm.nih.gov/35659631/ ↩︎ ↩︎ ↩︎
Wang, M., et al. (2026). "Short-chain fatty acids of intestinal origin attenuate protein-bound uremic toxins in patients with chronic kidney disease by protecting the intestinal barrier: a pooled analysis." BMC Gastroenterology, 26(1), 112. https://pubmed.ncbi.nlm.nih.gov/42289655/ ↩︎
Li, W., et al. (2026). "Multidimensional intestinal barrier repair strategies for alleviating inflammatory bowel disease and gut-liver axis-associated metabolic liver disease." Biomaterials, 312, 122700. https://pubmed.ncbi.nlm.nih.gov/42385493/ ↩︎
Ahmadi-Khorram, M., et al. (2026). "A Novel Combination of Probiotic Supplements Reduces Gut Permeability, Oxidative Stress, and Inflammation in Undernourished Adults: A Randomized Controlled Trial." Food Science & Nutrition, 14(6), 2045-2057. https://pubmed.ncbi.nlm.nih.gov/42255712/ ↩︎ ↩︎
Hatami, A., et al. (2026). "The effects of a novel combination of a probiotic supplement with a weight gain intervention on body composition, appetite, gut permeability, oxidative stress, and inflammation in underweight adults." BMC Nutrition, 12(1), 89. https://pubmed.ncbi.nlm.nih.gov/42393816/ ↩︎ ↩︎
De Bastiani, R., et al. (2025). "Improveing Chronic Atrophic Gastritis After Treatment with Zinc L-Carnosine." The American Journal of Case Reports, 26, e942851. https://pubmed.ncbi.nlm.nih.gov/41264559/ ↩︎
Abiru, S., et al. (2024). "Zinc supplementation with polaprezinc was associated with improvements in albumin, prothrombin time activity, and hemoglobin in chronic liver disease." Journal of Clinical Biochemistry and Nutrition, 74(2), 120-127. https://pubmed.ncbi.nlm.nih.gov/38510683/ ↩︎ ↩︎
Piccirillo, M., et al. (2026). "Zinc-L-Carnosine (Polaprezinc) in managing infant regurgitation: a two-center randomized controlled trial." Frontiers in Pediatrics, 14, 895012. https://pubmed.ncbi.nlm.nih.gov/42093671/ ↩︎
Del Colle, A., et al. (2026). "Exercise-induced intestinal barrier dysfunction: a potential contributor to athlete mental health." BMJ Open Sport & Exercise Medicine, 12(1), e001850. https://pubmed.ncbi.nlm.nih.gov/42404979/ ↩︎
See also: Gut Barrier, Dysbiosis