¶ Lung Cancer Screening
| Indication | Early detection of lung cancer in high-risk individuals |
| Access | Clinician referral; covered by insurance if eligibility met |
| Repeat testing | Annual screening while eligibility criteria are maintained |
| Safety Profile | Low-dose radiation, risk of diagnostic cascades |
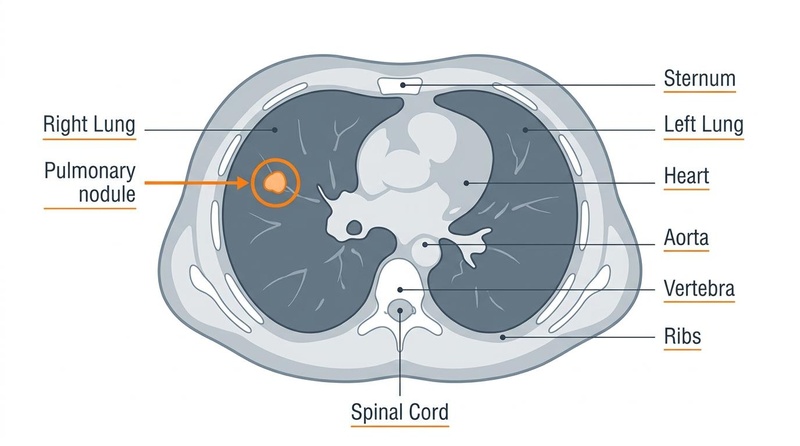
| Key Marker | Pulmonary Nodules (Lung-RADS categorization) |
| Est. Cost | Fully covered under the Affordable Care Act (ACA) in the US; $150–$400 self-pay |
Lung cancer screening is a secondary prevention strategy that utilizes annual low-dose computed tomography (LDCT) to detect early-stage lung malignancies in asymptomatic, high-risk individuals [1]. Because lung cancer is typically asymptomatic in its highly curable, localized stages, screening facilitates a significant clinical "stage shift," allowing for surgical resection or definitive therapy before the development of regional or distant metastasis [2][3]. Multiple large-scale, randomized controlled trials demonstrate that routine LDCT screening in properly stratified cohorts reduces lung cancer-specific mortality [4][5], with the landmark National Lung Screening Trial (NLST) also demonstrating a significant reduction in all-cause mortality [4:1].
¶ At a glance
- What people use it for: Early detection of primary epithelial lung malignancies (adenocarcinoma, squamous cell carcinoma, and small cell carcinoma) during the preclinical, asymptomatic phase, when tumors are highly amenable to curative treatment [6][3:1].
- Does it work? Yes, for high-risk cohorts. Landmark clinical trials demonstrate a 20% to 24% relative reduction in lung cancer mortality with annual LDCT screening [4:2][5:1], with a particularly pronounced reduction in lung cancer mortality observed in women [5:2].
- Key risks: Ionizing radiation exposure [7][8][9], high false-positive rates leading to diagnostic anxiety [4:3], overdiagnosis of indolent tumors [6:1], and invasive diagnostic cascades (biopsies or thoracic surgeries) for lesions that ultimately prove benign [10][2:1][6:2].
- Verdict: Recommended as an annual preventive scan for individuals meeting specific age and tobacco-exposure thresholds, or those with equivalent risk calculated via validated multivariable prediction engines [1:1][11][12]. Screening must be paired with structured smoking cessation support to optimize clinical benefit [13][12:1].
¶ Mechanism & Modalities
¶ Scan Technique & Low-Dose CT Parameters
Low-dose computed tomography (LDCT) of the chest is performed without intravenous contrast media during a single breath-hold [11:1][14][15]. Standard diagnostic chest CT scans typically deliver a higher radiation dose [14:1]. In contrast, LDCT protocols utilize a significantly lower radiation dose than standard diagnostic chest CT scans [16][7:1]. This reduced radiation exposure ensures a favorable safety profile for repeated annual administration in asymptomatic, high-risk cohorts [1:2][12:2].
Because LDCT is performed without intravenous contrast, it provides a non-invasive scanning method compared to contrast-enhanced diagnostic scans [14:2].
¶ Pathophysiology of Screening-Detected Lesions
The primary objective of LDCT is the identification of pulmonary nodules, which represent localized areas of increased lung density [17]. On high-resolution chest imaging, nodules are categorized based on their attenuation characteristics [17:1]:
- Solid Nodules: Homogeneous soft-tissue density that completely obscures the underlying lung parenchyma, bronchial structures, and vascular markings [17:2].
- Subsolid Nodules: Areas of hazy, increased attenuation that do not completely obscure the underlying lung tissue [17:3]. These are further subclassified:
- Pure Ground-Glass Nodules (GGNs): Lacking any solid soft-tissue component. Pure ground-glass nodules are frequently associated with noninvasive or pre-invasive lesions, but may also harbor invasive adenocarcinomas [18][19].
- Part-Solid Nodules: Contain both ground-glass and solid soft-tissue components. Part-solid nodules have the highest baseline probability of malignancy, as the solid portion typically represents active invasive epithelial components [20].
A major pathophysiological challenge in lung cancer screening is distinguishing malignant epithelial neoplasms from benign nodules, which are highly prevalent in the general population [6:3]. Benign nodules are highly prevalent in the general population [6:4]. Distinguishing these non-cancerous screening-detected lesions from early-stage malignant neoplasms is a primary focus of screening and follow-up management protocols [13:1][6:5].
¶ Volumetric CT vs. Diameter-Based Assessment
Early screening programs, including the National Lung Screening Trial (NLST), relied on manual, two-dimensional diameter-based measurements (taking the average of the longest perpendicular diameters of a nodule on a single transverse slice) [3:2][4:4]. However, manual measurements suffer from significant inter-observer variability and fail to capture asymmetric or three-dimensional nodule growth [6:6][21].
Modern European screening models, pioneered by the Dutch-Belgian Nederlands-Leuvens Longkanker Screenings Onderzoek (NELSON) trial, utilize computerized volumetric-based assessment [5:3][6:7]. Automated segmentation software calculates the total volume of the nodule in cubic millimeters () and measures changes in volume over time [6:8]:
- Volume-Doubling Time (VDT): The number of days required for a nodule to double in volume [6:9]. Malignant nodules typically exhibit a characteristic range of volume doubling, whereas nodules that double extremely rapidly are usually infectious or inflammatory, and those that remain stable over long periods are considered highly indolent or benign [6:10].
- Clinical Efficacy: Volumetric assessment dramatically increases diagnostic specificity [5:4][6:11]. In the diameter-based NLST, the positive screening rate was 24.2% over all three screening rounds combined [4:5], whereas the baseline false-positive result rate under the original trial criteria was actually 26.6% [22]. In contrast, the volumetric-based NELSON protocol successfully distinguished highly benign from indeterminate or suspicious nodules: only 9.2% of screened participants had initially indeterminate nodules requiring at least one additional follow-up CT scan, and only 2.1% were directly referred to a specialist for suspicious nodules [5:5][23]. This approach prevents unnecessary diagnostic cascades by filtering out low-risk lesions before clinical referral [5:6][6:12][23:1].
¶ The Lung-RADS Classification System
To standardize reporting and clinical management, the American College of Radiology (ACR) developed the Lung Imaging Reporting and Data System (Lung-RADS) [11:2]. Lung-RADS categorizes screening findings from 1 (negative) to 4 (highly suspicious) based on nodule type, size, and growth [17:4][24]. Each category maps directly to a defined risk of malignancy and a recommended clinical action plan (ranging from routine annual screening to immediate tissue biopsy) [17:5][24:1]. While standard Lung-RADS protocols rely on longitudinal follow-up, research suggests that single-baseline scan evaluations still retain significant diagnostic utility (achieving a sensitivity of 72% and specificity of 90.7% for characterizing nodules as benign or malignant) in resource-limited settings where follow-up CT access is constrained [25].
¶ Eligibility & Screening Protocols
Clinical guidelines have evolved to expand screening access, optimize mortality benefits, and address historical eligibility disparities [26][27].
¶ Average-Risk Eligibility & Clinical Guideline Comparison
Lung cancer screening eligibility varies across major clinical organizations, reflecting ongoing clinical discussions regarding age limits, smoking history thresholds, and the duration of the tobacco-free quit window [1:3][11:3][12:3][28].
¶ Key Guideline Comparisons
- USPSTF 2021 Guidelines: The US Preventive Services Task Force (USPSTF) 2021 guidelines recommend annual screening with LDCT for individuals aged 50 to 80 years who have a ≥20 pack-year smoking history, and who currently smoke or have quit within the past 15 years [1:4]. Screening is recommended to be discontinued once a person has not smoked for 15 years, or if they develop a health problem that substantially limits life expectancy or the ability/willingness to undergo curative lung surgery [1:5]. This expansion in eligibility criteria significantly increases the screening-eligible population across various clinical registries and cohort studies, particularly among populations with lower smoking intensity who were previously excluded under more restrictive guidelines [29][30].
- ACS 2023 Guidelines: The American Cancer Society (ACS) updated its lung cancer screening guideline in 2023 [12:4]. Notably, ACS 2023 recommends removing the 15-year quit window limitation [12:5]. It recommends annual LDCT screening for individuals aged 50 to 80 years with a ≥20 pack-year history, regardless of how long ago they quit smoking (recommending lifelong annual screening for anyone meeting the pack-year threshold who is otherwise in good health) [12:6]. This change was driven by evidence that lung cancer risk remains elevated for decades after cessation [12:7][30:1].
- CMS Coverage Criteria: Historically, Medicare (CMS) covered annual lung screening for beneficiaries aged 55 to 77 years who had a ≥30 pack-year smoking history and currently smoked or had quit within the past 15 years [11:4]. Updated evaluations of Medicare coverage address eligibility criteria and screening patterns for older adults, noting that coverage transitions and clinical factors for beneficiaries exceeding Medicare's upper age criteria (77+ years) are active points of research [31].
- NCCN Guidelines: The National Comprehensive Cancer Network (NCCN) publishes clinical practice guidelines that recommend standardized criteria for selecting individuals for lung cancer screening and offer detailed pathways for the evaluation, management, and follow-up of pulmonary nodules detected during initial and subsequent annual screening rounds [28:1].
| Guideline / Issuing Body | Eligible Age Range | Smoking History Criteria | Smoking Status / Quit Window | Key Clinical Distinctions & Coverage |
|---|---|---|---|---|
| USPSTF (2021) [1:6] | 50 to 80 years | ≥20 pack-years | Current smoker or quit within 15 years | National clinical standard; mandatory commercial insurance coverage [1:7]. |
| ACS (2023) [12:8] | 50 to 80 years | ≥20 pack-years | Current or former smoker (No quit window limit) | Removes the 15-year cessation cap; recommends screening former smokers indefinitely if in good health [12:9]. |
| CMS Coverage [11:5][31:1] | 55 to 77 years (historical standard) | ≥30 pack-years (historical standard) | Current smoker or quit within 15 years | Coverage standard for Medicare; caps screening 3 years earlier (at age 77) than USPSTF/ACS [11:6]; older adult coverage remains an active area of clinical study [31:2]. |
| NCCN Guidelines [28:2] | Standard clinical age limits | Standardized screening criteria | Standardized screening status | Focuses on structured nodule tracking and clinical workup algorithms across screening rounds [28:3]. |
¶ The Rationale for Guideline Expansion
The 2021 USPSTF guideline update lowered the screening age from 55 to 50 years and reduced the tobacco exposure requirement from 30 to 20 pack-years [1:8]. This expansion was driven by collaborative micro-simulation modeling showing that earlier and broader screening nearly doubled the eligible cohort, potentially saving additional lives [26:1][27:1].
Furthermore, the expansion directly addressed critical racial and sex disparities inherent in older criteria [27:2][29:1]:
- Disparities in Black Populations: Under older criteria, a lower proportion of high-risk Black individuals met eligibility thresholds, primarily because smoking patterns vary by race, and Black smokers often smoke fewer pack-years [29:2]. Lowering the thresholds to age 50 and 20 pack-years, or adopting risk-prediction models, significantly increased eligibility and sensitivity among Black smokers, thereby promoting clinical equity [29:3][32][33].
- Disparities in Female Populations: Women are more likely to have lower smoking intensities (fewer pack-years) compared to men [29:4]. The 2021 USPSTF criteria improved screening sensitivity for women, though some sex-based eligibility and screening uptake disparities still persist [34][30:2].
¶ Risk-Based Screening & The PLCOm2012 Model
While age and pack-year thresholds are simple to implement, they do not account for individual risk variations [10:1][32:1][35]. Clinical research increasingly supports risk-based screening, which utilizes multivariable risk prediction engines to calculate an individual's 6-year probability of developing lung cancer [10:2][32:2][35:1].
The PLCOm2012 model is the most widely validated and clinically integrated risk prediction tool [10:3][32:3][35:2]. It calculates risk using 11 distinct clinical variables:
- Age
- Race and ethnicity
- Education level
- Body mass index (BMI)
- Personal history of cancer
- Family history of lung cancer
- History of Chronic Obstructive Pulmonary Disease (COPD)
- Smoking status (current vs. former)
- Smoking intensity (cigarettes smoked per day)
- Smoking duration (years smoked)
- Smoking quit-time (years since quitting)
¶ Clinical Outcomes of Risk-Based Screening
Multiple prospective cohorts demonstrate that using a PLCOm2012 6-year risk threshold to determine screening eligibility is clinically superior to standard USPSTF age/pack-year criteria [10:4][35:3][33:1]:
- Improved Sensitivity: In prospective cohorts, risk-based selection identified significantly more lung cancer cases that would have been missed by standard guideline thresholds [35:4][33:2].
- Mitigation of Sex Disparities: Applying the PLCOm2012 model helps correct statistical sex disparities, achieving highly equitable sensitivities between women and men compared to pack-year standards [36].
- Reduced Benign Resections: By targeting screening to those with the highest absolute risk, risk-prediction models improve the positive predictive value of nodule detection, reducing the number of invasive procedures performed on benign lesions [10:5].
¶ Benefits of Screening: Clinical Trial Evidence
The clinical efficacy of LDCT screening is established by high-quality, randomized controlled trials involving tens of thousands of participants [2:2][3:3].
¶ Landmark Randomized Controlled Trials
LUNG CANCER MORTALITY REDUCTION
┌────────────────────────────────────────────────────────────────────────┐
│ NLST Trial (2011) │
│ [53,454 participants] ──► 20.0% Reduction (vs. Chest X-ray) │
├────────────────────────────────────────────────────────────────────────┤
│ NELSON Trial (2020) │
│ [15,789 participants] ──► 24.0% Reduction in Men (vs. No Screening) │
│ ──► Pronounced Reduction in Women │
├────────────────────────────────────────────────────────────────────────┤
│ UKLS Trial & Pooled Meta-Analysis (2021) │
│ [9 RCTs, Pooled] ──► Significant Pooled Mortality Reduction │
└────────────────────────────────────────────────────────────────────────┘
¶ 1. The National Lung Screening Trial (NLST) [3:4][4:6]
Conducted by the National Cancer Institute, the NLST randomized 53,454 asymptomatic current or former heavy smokers (aged 55 to 74 years, ≥30 pack-years, <15 quit years) to undergo three annual rounds of screening with either LDCT or single-view chest radiography [3:5][4:7].
- Lung Cancer Mortality: LDCT screening resulted in a 20.0% relative reduction in lung cancer deaths (247 vs. 309 deaths per 100,000 person-years; ) [4:8].
- All-Cause Mortality: The LDCT group demonstrated a 6.7% reduction in all-cause mortality (), proving that the benefit of early cancer detection was not offset by screening-induced harms [4:9].
¶ 2. The Nederlands-Leuvens Longkanker Screenings Onderzoek (NELSON) [5:7]
The largest European trial randomized 13,195 men and 2,594 women at high risk (aged 50 to 74 years) to undergo volume-based LDCT screening at baseline, year 1, year 3, and year 5.5 versus a control group receiving no screening [5:8].
- Lung Cancer Mortality (Men): At 10 years of follow-up, lung cancer mortality was 24% lower in the screening group (rate ratio 0.76; 95% CI, 0.61 to 0.94; ) [5:9].
- Lung Cancer Mortality (Women): Subgroup analysis in the NELSON trial revealed a pronounced reduction in lung cancer mortality among women, suggesting that women may derive a more significant benefit from early CT detection than men [5:10].
¶ 3. The UK Lung Cancer Screening (UKLS) Trial [2:3]
The UKLS pilot trial randomized 4,055 participants aged 50 to 75 to a single baseline LDCT scan or usual care, using the Liverpool Lung Project (LLPv2) risk model (threshold ≥4.5% over 5 years) for selection [2:4].
- Mortality Outcomes: Single LDCT screening was associated with a reduction in lung cancer death at a median follow-up of 7.3 years, though this did not reach statistical significance due to the trial's pilot sample size [2:5].
- Pooled Meta-Analysis: An international random-effects meta-analysis of nine randomized screening trials (including UKLS, NLST, and NELSON) yielded a pooled relative risk for lung cancer mortality of 0.84 (95% CI, 0.76 to 0.92), providing unequivocal, high-certainty evidence for the efficacy of structured screening programs [2:6].
¶ The Concept of "Stage Shift"
The physiological mechanism driving mortality reduction in these trials is the stage shift [2:7][6:13]. Lung cancer diagnosed symptomatically in clinical practice typically presents as locally advanced or metastatic disease (Stage III or IV) in over 75% of cases, resulting in a 5-year survival rate of less than 5% [3:6][6:14].
In contrast, structured LDCT screening detects the vast majority of lung cancers during the early, localized stages (Stage I or II) [2:8][6:15]:
- The UKLS trial demonstrated that even a single round of LDCT screening can achieve a reduction in lung cancer mortality of a similar magnitude to longitudinal screening trials, with an international meta-analysis confirming a significant pooled mortality reduction [2:9].
- In the clinical cohort analyzed by Rode et al. (2025), 74% of screen-detected non-small cell lung cancers (NSCLC) were Stage I or II [10:6].
- Upon detection, the probability of lung cancer mortality prevention is estimated to be highly favorable, especially for Stage IA tumors [5:11], with micro-simulation modeling estimating mortality prevention at 83% for Stage IA disease [37].
¶ Harms & Clinical Uncertainties
While the mortality benefits of lung cancer screening are profound, they must be balanced against well-documented clinical harms [6:16][13:2].
¶ 1. Cumulative Radiation Exposure
Annual screening with LDCT exposes patients to low levels of ionizing radiation [7:2]. A typical LDCT scan delivers a median effective radiation dose of approximately 1.15 mSv [7:3] to 1.5 mSv [16:1], whereas standard-dose chest CT imaging delivers approximately 5.0 mSv [16:2]. Although this single scan dose is low and carries a negligible lifetime risk of carcinogenesis, cumulative exposure over 10 to 30 years of annual screening can theoretically induce solid chest malignancies (such as breast, thyroid, or lung cancer) in a small fraction of screened individuals [8:1][9:1]. Based on phantom dosimetry studies, the cumulative radiogenic risk of cancer from repeated annual scans is estimated to increase the lifetime intrinsic risk of cancer by 0.13% in males and 0.30% in females [8:2]. Consequently, screening must be strictly limited to cohorts whose absolute risk of lung cancer death is high enough to ensure a substantial net benefit [1:9].
¶ 2. High False-Positive Rates & Diagnostic Cascades
On initial diameter-based LDCT baseline screens under the original trial criteria, up to 26.6% of scans will identify a pulmonary nodule classified as a positive screening result requiring further evaluation [22:1]. However, approximately 95% to 96% of these positive scans represent false positives (benign lesions) [4:10][5:12].
The detection of these benign "incidentalomas" triggers diagnostic cascades, which may include [10:7][22:2][5:13]:
- Serial follow-up CT scans, increasing cumulative radiation dose and financial costs [7:4].
- Specialized imaging, such as Fluorodeoxyglucose (FDG) Positron Emission Tomography (PET-CT) scans [11:7].
- Invasive procedures, including percutaneous transthoracic needle biopsies, bronchoscopies, or video-assisted thoracoscopic surgery (VATS) [10:8][23:2].
In real-world cohorts, approximately 4.3% of all screened patients undergo an invasive intervention due to screening findings [10:9]. Surgical resections for lesions that ultimately prove to be benign occur in approximately 4.5% of surgical cases [10:10].
While major complications from invasive testing are low (<1% in experienced centers), they include pneumothorax (requiring chest tube insertion), pulmonary hemorrhage, and post-procedural infection.
¶ 3. Overdiagnosis
Overdiagnosis refers to the detection of screen-identified lung cancers that would not have progressed to cause clinical symptoms or death during the patient's lifetime [3:7][6:17]. These are typically highly indolent, slow-growing adenocarcinomas (such as lepidic-predominant adenocarcinomas). Micro-simulation models and trials indicate that a proportion of screen-detected lung cancers represent overdiagnosis [6:18]. Overdiagnosis leads to unnecessary treatments (surgical resection, radiation, or chemotherapy) and lifelong oncological surveillance, exposing patients to treatment-related morbidity without extending lifespan.
¶ 4. Incidental Extrapulmonary Findings
Because LDCT scans capture the entire thoracic cavity, they frequently reveal incidental extrapulmonary findings of clinical significance [6:19]. Common incidental findings include:
- Coronary Artery Calcification (CAC): Moderate-to-severe coronary calcification is a strong predictor of future cardiovascular events [6:20]. Reporting of CAC on non-gated screening scans provides an important avenue for cardiovascular risk reclassification and preventive therapy [6:21]. In rural mobile screening programs, a significant correlation has been demonstrated between higher Lung-RADS scores and elevated coronary artery calcium (CAC) burden, highlighting the clinical utility of simultaneous lung and cardiovascular risk evaluation [38].
- Emphysema: Allows for the early detection and management of Chronic Obstructive Pulmonary Disease (COPD) [6:22].
- Extrapulmonary Masses: Including suspicious thyroid nodules, mediastinal masses, or aortic aneurysms [6:23].
These findings can provide clinical value, but they also contribute to diagnostic anxiety, out-of-pocket costs, and further downstream diagnostic testing [6:24].
¶ Shared Decision Making & Stopping Considerations
Prior to initiating lung cancer screening, clinicians are encouraged to conduct a formal Shared Decision-Making (SDM) consultation [11:8][1:10].
¶ Key Components of the SDM Consultation
- Establish Eligibility: Confirm the patient's age, calculate exact pack-years, and verify that they have not been smoke-free for more than 15 years [1:11].
- Discuss Net Benefit: Communicate the significant mortality reduction (~20–24% relative reduction) and discuss the concept of the Number Needed to Screen (NNS) qualitatively as a measure of screening efficiency [4:11][5:14].
- Review Potential Harms: Clearly communicate the high probability of finding benign nodules, the risk of false-positive alarms, the cumulative radiation dose, and the potential need for invasive diagnostic procedures [4:12][6:25].
- Ascertain Patient Preferences: Assess the patient's tolerance for diagnostic uncertainty, anxiety regarding potential invasive interventions, and willingness to undergo curative lung surgery if cancer is detected [1:12][11:9].
- Incorporate Smoking Cessation: Provide structured, evidence-based smoking cessation counseling, as quitting smoking delivers an immediate and synergistic reduction in all-cause and cardiovascular mortality [6:26].
¶ Stopping Criteria: When to Discontinue Screening
Annual lung cancer screening is not a lifelong intervention. Screening should be discontinued if the patient meets any of the following criteria:
- Age Limits: The patient reaches the upper age limit of the guideline (80 years based on the USPSTF criteria) [1:13].
- Tobacco-Free Interval: The patient has successfully remained smoke-free for 15 years [1:14].
- Limiting Comorbidities: The patient develops a progressive, life-limiting health problem (such as advanced congestive health failure, end-stage renal disease, or severe dementia) that would substantially limit life expectancy or make them physically unable or unwilling to undergo curative thoracic surgery [1:15].
¶ Clinical Red Flags
lung-cancer-screening is strictly a preventive tool for asymptomatic individuals [1:16]. It is not a diagnostic test for symptomatic patients.
¶ Symptoms Requiring Immediate Diagnostic Workup
The presence of any of the following symptoms constitutes a clinical red flag, indicating the need for an immediate, comprehensive diagnostic chest CT with contrast and appropriate specialist referral, rather than a screening LDCT [1:17][12:10]:
- Hemoptysis: Coughing up blood or blood-streaked sputum [12:11].
- Unexplained Weight Loss: Unintentional or unexplained weight loss, or loss of appetite [12:12].
- New or Changing Chronic Cough: A persistent cough that does not go away or worsens over time [12:13].
- Persistent Chest Pain: New, unexplained, or persistent chest pain, discomfort, or localized thoracic pain [12:14].
- Progressive Dyspnea or Wheezing: New-onset difficulty breathing, shortness of breath, or localized wheezing [12:15].
- Hoarseness or Dysphagia: Unexplained voice changes (hoarseness) or difficulty swallowing [12:16].
Utilizing a low-dose screening CT in a symptomatic patient is clinically inappropriate, as national guidelines strictly define screening eligibility for asymptomatic individuals, while symptomatic patients require standard diagnostic evaluation [1:18][12:17].
¶ Evidence Summary
The following table summarizes the clinical evidence and estimated health outcomes associated with low-dose computed tomography (LDCT) lung cancer screening.
¶ Evidence summary table (human outcomes)
| Goal / Target Outcome | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Lung Cancer-Specific Mortality | High | High | 9 RCTs | Demonstrates a 20% to 24% relative reduction in lung cancer deaths in high-risk cohorts over 10 years [4:13][5:15][2:10]. | |
| All-Cause Mortality Reduction | Moderate | High | 1 Large RCT | Shows a 6.7% reduction in all-cause mortality in the NLST [4:14]; the NELSON trial did not demonstrate a statistically significant reduction in all-cause mortality [5:16]. | |
| Stage Shift (Early Detection) | High | High | Multiple RCTs | Significantly increases the detection of early-stage (Stage I and II) cancers, enabling curative surgical resection [10:11][2:11]. | |
| False-Positive Nodule Rate | High | High | Multiple RCTs | Up to 26.6% of patients have positive baseline scans under original criteria; ~95% of these nodules are benign granulomas or scars [22:3][5:17]. | |
| Diagnostic Nodule Referrals (Volumetric) | High | High | 1 Large RCT | Volumetric CT (NELSON protocol) resulted in 9.2% indeterminate follow-up scan rates and a low 2.1% direct specialist referral rate, compared to a 26.6% false-positive rate under original criteria in the diameter-based NLST [5:18]. | |
| Invasive Procedures for Benign Disease | Moderate | Moderate | Cohort Studies | Approximately 4.3% of screened patients undergo invasive testing; 4.5% of surgical resections are for benign nodules [10:12]. | |
| Overdiagnosis of Indolent Cancer | Moderate | Moderate | Modeling | A proportion of screen-detected cancers represent indolent tumors that would not cause clinical symptoms or death during the patient's lifetime [3:8][6:27]. | |
| Risk-Based Selection Efficacy | High | High | Cohort Studies | PLCOm2012 risk-based screening improves eligibility sensitivity and significantly reduces racial/sex disparities [36:1][35:5][33:3]. |
- *Effect: Compact renderer encoding (preferred when using custom tags):
<effect e="[dir][mag][impact]"></effect>wheredir=u|d|e|q,mag=0|1|2|3,impact=p|n|x. Examples:↓↓ (p)-><effect e="d2p"></effect>,= (x)-><effect e="e0x"></effect>,?-><effect e="q0x"></effect>. - **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
¶ Clinician-Discussion Checklist & Actionable Next Steps
¶ Lung-RADS v1.1 / v2022 Management Protocol
The following table outlines the standardized Lung-RADS categories, malignancy risk levels, and clinical recommended pathways for screening-detected nodules based on official ACR Lung-RADS standards [17:6][24:2]. Unlike breast imaging classification (BI-RADS), which utilizes a Category 4C, the standardized Lung-RADS framework attributes only 4A, 4B, and 4X as suspicious or highly suspicious subcategories [17:7][24:3].
| Lung-RADS Category | Concept & Nodule Description | Malignancy Risk Level | Recommended Clinical Approach |
|---|---|---|---|
| Category 1 (Negative) | No pulmonary nodules detected on baseline chest scan [17:8][24:4]. | Very Low | Annual Screening: Continue standard annual screening with low-dose CT in 12 months [17:9][24:5]. |
| Category 2 (Benign Appearance) | Small nodules with highly benign features or very low likelihood of growth [17:10][24:6]. | Very Low | Annual Screening: Continue standard annual screening with low-dose CT in 12 months [17:11][24:7]. |
| Category 3 (Probably Benign) | Intermediate-sized or stable nodules requiring short-term surveillance [17:12][24:8]. | Low | Surveillance: Short-term follow-up LDCT to assess interval growth or volume-doubling time [17:13][24:9]. |
| Category 4A / 4B (Suspicious) | Larger, growing, or suspicious solid/subsolid nodules [17:14][24:10]. | Intermediate to High | Diagnostic Workup: More frequent follow-up LDCT, advanced diagnostic imaging, or specialty referral [17:15][24:11]. |
| Category 4X (Highly Suspicious) | Nodules exhibiting highly suspicious clinical or imaging features (e.g., rapid growth or aggressive appearance) [17:16][24:12]. | High | Immediate Evaluation: Direct referral for diagnostic interventions, tissue biopsy, or thoracic surgery [17:17][24:13]. |
| Category S (Incidental findings) | Significant findings outside of lung nodules (e.g., cardiovascular calcifications or severe emphysema) [11:10]. | N/A | Clinical Referral: Direct communication to primary care or relevant specialist for appropriate evaluation [11:11]. |
¶ Action Plan for Clinicians and Patients
To implement a clinically effective lung cancer screening protocol, follow these sequential steps:
- Assess Individual Eligibility: Calculate the patient's tobacco exposure in pack-years. If the patient is aged 50–80 with ≥20 pack-years, calculate their 6-year absolute risk using the PLCOm2012 risk calculator to refine risk, particularly if they are female or of African American descent [36:2][35:6][33:4].
- Conduct Shared Decision-Making: Schedule a dedicated consultation to discuss the benefits, risks (radiation, false-positives, biopsy complications), and the patient's preferences regarding potential surgical intervention [11:12][1:19].
- Initiate Smoking Cessation Counseling: For current smokers, integrate structured behavioral therapy and pharmacotherapy (e.g., varenicline, nicotine replacement) [13:3][12:18].
- Order the Scan at an Accredited Facility: Ensure the LDCT is scheduled at an ACR-accredited lung cancer screening center that utilizes standardized low-dose imaging parameters and structured Lung-RADS reporting [11:13].
- Review the Results and Execute Follow-Up: Review the formal Lung-RADS category. For Category 1 or 2, schedule the next annual scan. For Category 3 or higher, execute the recommended diagnostic follow-up pathway without delay [11:14][17:18].
¶ FAQ
¶ What is a "pack-year" and how do I calculate it?
A pack-year is a clinical unit of measurement used to quantify a person's lifetime tobacco exposure. It is calculated by multiplying the number of packs of cigarettes smoked per day by the number of years the person has smoked. For example, smoking 1 pack per day for 20 years equals 20 pack-year; smoking 2 packs per day for 10 years also equals 20 pack-years; smoking half a pack per day for 40 years also equals 20 pack-years.
¶ At what age should lung cancer screening be discontinued?
Lung cancer screening should be discontinued once a person reaches the upper age limit of 80 years, has not smoked for 15 years, or develops a limiting health problem that substantially reduces life expectancy or the willingness/ability to undergo curative lung surgery [^4].
¶ How does volumetric-based screening differ from standard diameter-based screening?
Diameter-based assessment measures the average of the largest perpendicular diameters of a nodule on a single two-dimensional CT slice [^18]. Volumetric-based screening utilizes advanced computerized software to calculate the true three-dimensional volume (mm³) of the nodule and analyze its exact rate of growth over time (volume-doubling time) [^23]. Volumetric screening is highly superior at filtering out benign nodules. For instance, in the NELSON trial, 9.2% of screened participants underwent at least one additional CT scan for initially indeterminate nodules, while only 2.1% had suspicious findings requiring direct referral to a specialist [^21], compared to the 26.6% baseline false-positive screening rate under the original diameter-based NLST criteria [^20].
¶ Does a negative lung screening scan mean I am entirely free of lung cancer risk?
No. A negative scan (Lung-RADS 1) indicates that no suspicious pulmonary nodules were detected at the time of the scan [^16]. However, it does not guarantee that cancer will not develop in the future, nor does it rule out highly rapid-growing tumors that can arise between annual scans (interval cancers) [^23]. High-risk individuals must continue annual screening as long as they meet eligibility criteria [^4].
¶ What should be done if the scan reveals severe coronary artery calcification?
A screening chest scan captures the heart and coronary arteries, frequently revealing [coronary artery calcification (CAC)](coronary-artery-calcium-scoring.md) as an incidental finding (reported as Lung-RADS "S") [^16]. Severe coronary calcification is a strong predictor of future cardiovascular events [^23]. If detected, the finding should be discussed with a physician to determine if cardiovascular preventive measures, such as lipid-lowering therapy (statins) or blood pressure control, are warranted [^23].
¶ References
US Preventive Services Task Force, Krist AH, Davidson KW, et al. Screening for Lung Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(10):961-970. https://pubmed.ncbi.nlm.nih.gov/33687470/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Field JK, Vulkan D, Davies MPA, et al. Lung cancer mortality reduction by LDCT screening: UKLS randomised trial results and international meta-analysis. The Lancet regional health. Europe. 2021;10:100179. https://pubmed.ncbi.nlm.nih.gov/34806061/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
National Lung Screening Trial Research Team. The National Lung Screening Trial: overview and study design. Radiology. 2011;258(1):243-253. https://pubmed.ncbi.nlm.nih.gov/21045183/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
National Lung Screening Trial Research Team, Aberle DR, Adams AM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. The New England journal of medicine. 2011;365(5):395-409. https://pubmed.ncbi.nlm.nih.gov/21714641/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. The New England journal of medicine. 2020;382(6):503-513. https://pubmed.ncbi.nlm.nih.gov/31995683/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Oudkerk M, Liu S, Heuvelmans MA, et al. Lung cancer LDCT screening and mortality reduction - evidence, pitfalls and future perspectives. Nature reviews. Clinical oncology. 2021;18(3):135-151. https://pubmed.ncbi.nlm.nih.gov/33046839/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Iball GR, Beeching CE, Gabe R. An evaluation of CT radiation doses within the Yorkshire Lung Screening Trial. The British journal of radiology. 2024;97(1154):347-353. https://pubmed.ncbi.nlm.nih.gov/38308037/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Perisinakis K, Seimenis I, Tzedakis A, et al. Radiation burden and associated cancer risk for a typical population to be screened for lung cancer with low-dose CT: A phantom study. European radiology. 2018;28(10):4370-4378. https://pubmed.ncbi.nlm.nih.gov/29651767/ ↩︎ ↩︎ ↩︎
McCunney RJ, Li J. Radiation risks in lung cancer screening programs: a comparison with nuclear industry workers and atomic bomb survivors. Chest. 2014;145(3):618-624. https://pubmed.ncbi.nlm.nih.gov/24590022/ ↩︎ ↩︎
Rode MM, Sykes AG, Allen MS. Risk-Based Lung Cancer Screening in Clinical Practice. Journal of thoracic oncology : official publication of the International Association for the Study of Lung Cancer. 2025;20(9):1230-1238. https://pubmed.ncbi.nlm.nih.gov/40379047/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Expert Panel on Thoracic Imaging, Sandler KL, Henry TS, et al. ACR Appropriateness Criteria® Lung Cancer Screening: 2022 Update. Journal of the American College of Radiology : JACR. 2023;20(5S):S112-S121. https://pubmed.ncbi.nlm.nih.gov/37236754/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wolf AMD, Oeffinger KC, Shih TY, et al. Screening for lung cancer: 2023 guideline update from the American Cancer Society. CA: A Cancer Journal for Clinicians. 2024;74(1):50-81. https://pubmed.ncbi.nlm.nih.gov/37909877/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Veronesi G, Baldwin DR, Henschke CI. Recommendations for Implementing Lung Cancer Screening with Low-Dose Computed Tomography in Europe. Cancers. 2020;12(7):1672. https://pubmed.ncbi.nlm.nih.gov/32599792/ ↩︎ ↩︎ ↩︎ ↩︎
Hu QJ, Liu YW, Chen C, et al. Prospective Study of Low- and Standard-dose Chest CT for Pulmonary Nodule Detection: A Comparison of Image Quality, Size Measurements and Radiation Exposure. Current medical science. 2021;41(5):981-987. https://pubmed.ncbi.nlm.nih.gov/34652628/ ↩︎ ↩︎ ↩︎
Milanese G, Ledda RE, Sabia F, et al. Ultra-low dose computed tomography protocols using spectral shaping for lung cancer screening: Comparison with low-dose for volumetric LungRADS classification. European journal of radiology. 2023;161:110752. https://pubmed.ncbi.nlm.nih.gov/36878153/ ↩︎
Sakane H, Ishida M, Shi L. Biological Effects of Low-Dose Chest CT on Chromosomal DNA. Radiology. 2020;295(2):439-445. https://pubmed.ncbi.nlm.nih.gov/32154776/ ↩︎ ↩︎ ↩︎
Christensen J, Prosper AE, Wu CC, et al. ACR Lung-RADS v2022: Assessment Categories and Management Recommendations. Journal of the American College of Radiology : JACR. 2024;21(3):351-366. https://pubmed.ncbi.nlm.nih.gov/37820837/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chang YC, Chen PT, Hsieh MS, et al. Discrimination of invasive lung adenocarcinoma from Lung-RADS category 2 nonsolid nodules through visual assessment: a retrospective study. European radiology. 2024;34(5):3112-3120. https://pubmed.ncbi.nlm.nih.gov/37914975/ ↩︎
Meng Q, Liu T, Peng H, et al. Construction and validation of a risk stratification model based on Lung-RADS® v2022 and CT features for predicting the invasive pure ground-glass pulmonary nodules in China. Insights into imaging. 2025;16(1):42. https://pubmed.ncbi.nlm.nih.gov/40121609/ ↩︎
Mendoza DP, Petranovic M, Som A, et al. Lung-RADS Category 3 and 4 Nodules on Lung Cancer Screening in Clinical Practice. AJR. American journal of roentgenology. 2022;219(1):153-162. https://pubmed.ncbi.nlm.nih.gov/35080453/ ↩︎
van Riel SJ, Jacobs C, Scholten ET, et al. Observer variability for Lung-RADS categorisation of lung cancer screening CTs: impact on patient management. European radiology. 2019;29(2):485-493. https://pubmed.ncbi.nlm.nih.gov/30066248/ ↩︎
Pinsky PF, Gierada DS, Black W. Performance of Lung-RADS in the National Lung Screening Trial: a retrospective assessment. Annals of internal medicine. 2015;162(7):485-491. https://pubmed.ncbi.nlm.nih.gov/25664444/ ↩︎ ↩︎ ↩︎ ↩︎
Horeweg N, Scholten ET, de Jong PA, et al. Detection of lung cancer through low-dose CT screening (NELSON): a prespecified analysis of screening test performance and interval cancers. The Lancet. Oncology. 2014;15(11):1212-1221. https://pubmed.ncbi.nlm.nih.gov/25282284/ ↩︎ ↩︎ ↩︎
Chelala L, Hossain R, Kazerooni EA. Lung-RADS Version 1.1: Challenges and a Look Ahead, From the AJR Special Series on Radiology Reporting and Data Systems. AJR. American journal of roentgenology. 2021;216(6):1413-1422. https://pubmed.ncbi.nlm.nih.gov/33470834/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Arshad S, Arshad A, Fatima M. Use of a single-scan Lung-RADS for pulmonary nodule assessment in resource-limited clinical settings. Current problems in diagnostic radiology. 2026;55(1):102-110. https://pubmed.ncbi.nlm.nih.gov/41667372/ ↩︎
Marshall RC, Tiglao SM, Thiel D. Updated USPSTF screening guidelines may reduce lung cancer deaths. The Journal of family practice. 2021;70(7):350-353. https://pubmed.ncbi.nlm.nih.gov/34818167/ ↩︎ ↩︎
Potter AL, Bajaj SS, Yang CJ. The 2021 USPSTF lung cancer screening guidelines: a new frontier. The Lancet. Respiratory medicine. 2021;9(7):689-691. https://pubmed.ncbi.nlm.nih.gov/33965004/ ↩︎ ↩︎ ↩︎
Wood DE, Kazerooni EA, Aberle D, et al. NCCN Guidelines® Insights: Lung Cancer Screening, Version 1.2022. Journal of the National Comprehensive Cancer Network : JNCCN. 2022;20(7):754-764. https://pubmed.ncbi.nlm.nih.gov/35830884/ ↩︎ ↩︎ ↩︎ ↩︎
Smeltzer MP, Liao W, Goss J, et al. Reducing Smoking Requirements for Lung Screening to Address Health Disparities in a Community Cohort. JAMA network open. 2025;8(6):e251102. https://pubmed.ncbi.nlm.nih.gov/40553471/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Liu Y, Halpern MT, Volk RJ, et al. Characteristics of the Newly Eligible Population under Two Recent Updates of Lung Cancer Screening Recommendations. Cancer prevention research (Philadelphia, Pa.). 2025;18(6):321-330. https://pubmed.ncbi.nlm.nih.gov/40209067/ ↩︎ ↩︎ ↩︎
Hernandez M, Maki KG, Zhao H. Lung Cancer Screening among Adults Older than Medicare's Upper Age Eligibility Criteria. Cancer prevention research (Philadelphia, Pa.). 2025;18(11):655-662. https://pubmed.ncbi.nlm.nih.gov/40625204/ ↩︎ ↩︎ ↩︎
Han SS, Chow E, Ten Haaf K, et al. Disparities of National Lung Cancer Screening Guidelines in the US Population. Journal of the National Cancer Institute. 2020;112(11):1125-1132. https://pubmed.ncbi.nlm.nih.gov/32040195/ ↩︎ ↩︎ ↩︎ ↩︎
Pu CY, Lusk CM, Neslund-Dudas C, et al. Comparison Between the 2021 USPSTF Lung Cancer Screening Criteria and Other Lung Cancer Screening Criteria for Racial Disparity in Eligibility. JAMA oncology. 2022;8(3):374-382. https://pubmed.ncbi.nlm.nih.gov/35024781/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Manful A, Amanna N, Park SL, et al. The Impact of the 2023 American Cancer Society Screening Recommendations on Racial, Ethnic, and Sex Disparities in Lung Cancer Screening Eligibility. Chest. 2026;169(6):1412-1420. https://pubmed.ncbi.nlm.nih.gov/41580073/ ↩︎
Aredo JV, Choi E, Ding VY, et al. Racial and Ethnic Disparities in Lung Cancer Screening by the 2021 USPSTF Guidelines Versus Risk-Based Criteria: The Multiethnic Cohort Study. JNCI cancer spectrum. 2022;6(3):pkac031. https://pubmed.ncbi.nlm.nih.gov/35642317/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Pasquinelli MM, et al. Addressing Sex Disparities in Lung Cancer Screening Eligibility: USPSTF vs PLCOm2012 Criteria. Chest. 2022;161(1):248-256. https://pubmed.ncbi.nlm.nih.gov/34252436/ ↩︎ ↩︎ ↩︎
de Nijs K, Ten Haaf K, Hubert J, et al. Stage- and histology-specific sensitivity for the detection of lung cancer of the NELSON screening protocol-A modeling study. International journal of cancer. 2025;157(11):1812-1820. https://pubmed.ncbi.nlm.nih.gov/40650354/ ↩︎
Berzingi S, Piechowski K, Hendricks E, et al. Integrating cardiovascular risk assessment into mobile low-dose CT lung screenings in rural Appalachia: A comprehensive analysis of the relationship between lung cancer risk, coronary artery calcium burden, and cardiovascular risk reduction strategies. American journal of preventive cardiology. 2024;19:100714. https://pubmed.ncbi.nlm.nih.gov/39252854/ ↩︎