¶ Morning Light Optimization: Deep Dive
¶ TL;DR
- The Verdict: Morning light is the most potent exogenous synchronizer (zeitgeber) of the human circadian system. A brief 5-to-30-minute exposure initiates molecular cascades that advance melatonin onset, enhance daytime cortisol, and improve sleep efficiency within 3 to 7 days.
- Target Audience: Critical for individuals with delayed sleep phase, seasonal affective disorder, morning grogginess, shift workers, and aging populations experiencing circadian drift.
- Efficacy & Timeline: Expect a 30-to-90-minute phase advance in sleep onset and a 20-40% reduction in sleep latency within 1 week of consistent daily entrainment.
- Primary Safety Concern: Retinal phototoxicity from direct sun-gazing and a high risk of triggering manic or hypomanic switches in patients with pre-existing bipolar spectrum disorders.
- Next Step: Seek outdoor light within 30 minutes of waking (5–10 minutes on sunny days, 20–30 minutes on overcast days) or utilize a 10,000 lux broad-spectrum light box.
¶ Quick Answer
Optimal morning light exposure requires capturing 10,000 lux of broad-spectrum light (or a minimum of 250 melanopic Equivalent Daylight Illuminance [EDI] lux at the eye) for 10 to 30 minutes within 30 to 60 minutes of waking. This stimulus activates melanopsin-expressing intrinsically photosensitive retinal ganglion cells (ipRGCs). These cells transmit electrical signals via the retinohypothalamic tract (RHT) to the suprachiasmatic nucleus (SCN), resetting the master pacemaker. This non-invasive intervention effectively halts melatonin synthesis, elevates morning cortisol, shortens sleep-onset latency, and advances the subsequent night's sleep-wake cycle.
¶ What It Is
Morning light optimization is a strategic behavioral and environmental intervention that leverages natural sunlight or high-intensity artificial light to align endogenous biological rhythms with the 24-hour geophysical cycle. Sunlight acts as the primary "zeitgeber" (external cue) that entrains the internal human master clock, which otherwise runs on an intrinsic period slightly exceeding 24 hours.
¶ The Mechanism: Retinohypothalamic Tract (RHT) to SCN Signaling
Circadian photic entrainment is mediated by a specialized, non-image-forming visual pathway. Unlike classic rod and cone photoreceptors that support spatial vision, this pathway begins with intrinsically photosensitive retinal ganglion cells (ipRGCs) situated in the inner plexiform layer of the retina [1]. These cells directly express the photopigment melanopsin (OPN4), which displays a peak spectral sensitivity in the blue range at approximately 480 nm [2][3].
[ Sunlight / Bright Light (~480 nm) ]
│
▼
[ ipRGCs (Melanopsin/OPN4) ]
│
(Retinohypothalamic Tract / RHT)
│
▼
[ Suprachiasmatic Nucleus / SCN ] ──(Inhibits)──► [ Pineal Gland ] ──► (Melatonin Suppression)
│
(Clock Genes)
│
▼
[ PER1/2 & CRY1/2 Up-regulation ] ──► [ Phase Advance (Shift Sleep Earlier) ]
When photons hit ipRGCs, they trigger a G-protein-coupled signaling cascade that depolarizes the cell membrane, generating action potentials that travel along the retinohypothalamic tract (RHT) [1:1]. The RHT projects directly to the suprachiasmatic nucleus (SCN) of the anterior hypothalamus.
- Photic stimulation of the SCN triggers the release of excitatory neurotransmitters glutamate and pituitary adenylate cyclase-activating polypeptide (PACAP).
- This influx stimulates intracellular calcium and cyclic adenosine monophosphate (cAMP) pathways, activating cAMP-response element-binding protein (CREB).
- Phosphorylated CREB drives the immediate transcription of core clock genes, specifically Period 1 (Per1) and Period 2 (Per2), shifting the transcription-translation feedback loop (TTFL) [4].
- Concurrently, the SCN suppresses the pineal gland's production of melatonin via polysynaptic sympathetic pathways, while driving a robust, localized spike in cortisol (the cortisol awakening response) and elevating core body temperature to facilitate alertness [1:2].
¶ Visual Card: Neural Signaling Pathway
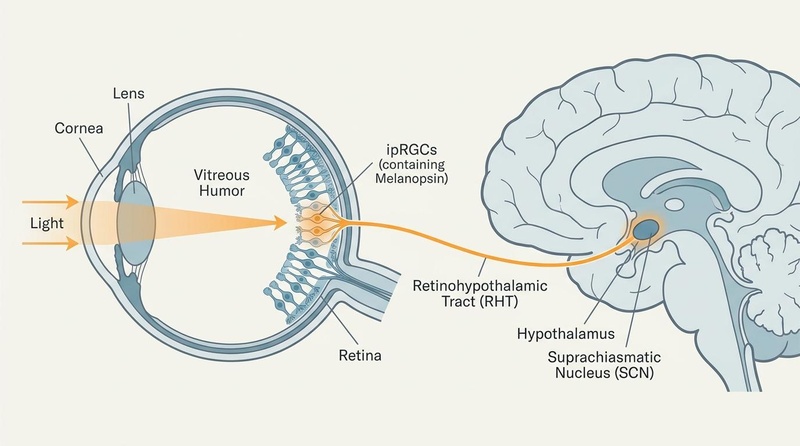
Figure 1: The Retinohypothalamic Tract (RHT) Pathway. Photic signals are captured by melanopsin-expressing ipRGCs in retina, transmitting action potentials directly to the suprachiasmatic nucleus (SCN) to entrain the master circadian clock.
Metadata:
Visual Plan: Diagram of the human eye showing light entering, hitting ipRGCs expressing melanopsin, projecting via RHT to the SCN in the hypothalamus of the brain. Clean, labeled scientific diagram with off-white background, slate lines, muted blue/teal forms, subtle warm orange highlighting the active light path.
Prompt: "Diagram of the human eye showing light entering, hitting intrinsically photosensitive retinal ganglion cells (ipRGCs) expressing melanopsin, projecting via the retinohypothalamic tract (RHT) to the suprachiasmatic nucleus (SCN) in the hypothalamus of the brain."
Seed: Default
Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate lines, muted blue/teal forms, subtle warm orange emphasis, restrained nature motifs).
Dimensions: 800x446px
QA State: Pass
¶ Does It Work? (Evidence Snapshot)
There is high-certainty human clinical evidence that morning light exposure regulates the circadian phase, reduces sleep-onset latency, and improves mood.
¶ Evidence Summary Table (Human Outcomes)
| Outcome | Population | Typical Effect | Certainty (GRADE) | Clinical Study Count & Type | Timeframe |
|---|---|---|---|---|---|
| Circadian Phase Advance (DLMO) | Delayed Sleep-Wake Phase, Insomnia, Healthy Adults | Shifting of Dim-Light Melatonin Onset (DLMO) earlier by 30 to 90 minutes [5] | High | >15 RCTs, systematic reviews [5:1][6][7] | 3 to 7 days |
| Reduction in Sleep-Onset Latency | Chronic Insomnia, Primary Sleep Disturbances | Reduction in latency by 15 to 35 minutes (20–40% decrease) [8][9][10] | High | >10 RCTs [9:1][10:1] | 1 to 2 weeks |
| Increase in Sleep Efficiency | Neurodegenerative Conditions, Healthy Adults, Aging | Sleep efficiency improved by 5% to 12% [11][12] | Moderate | >8 RCTs, systematic reviews [11:1][12:1] | 2 to 4 weeks |
| Melatonin Suppression (Acute) | Healthy Adults, Shift Workers | Melatonin levels suppressed by 50% to 85% within 15 minutes of high-intensity light [13][6:1] | High | >20 laboratory crossover studies [13:1][6:2] | Immediate (<30 min) |
| Reduction in Depressive Symptoms | Seasonal Affective Disorder (SAD), Bipolar Depression | 50% to 65% reduction in depressive symptom scores on SIGH-SAD [14][15] | High | >12 RCTs [14:1][16] | 1 to 3 weeks |
¶ Spectral Comparison: Sunlight vs. Artificial LED
Achieving these clinical benefits is directly dependent on the spectral quality of the light source. Natural morning sunlight provides a rich, continuous distribution of wavelengths, peaking precisely in the blue-green spectrum where melanopsin-expressing ipRGCs are most sensitive [6:3][2:1].
¶ Visual Card: Spectral Distribution Comparison
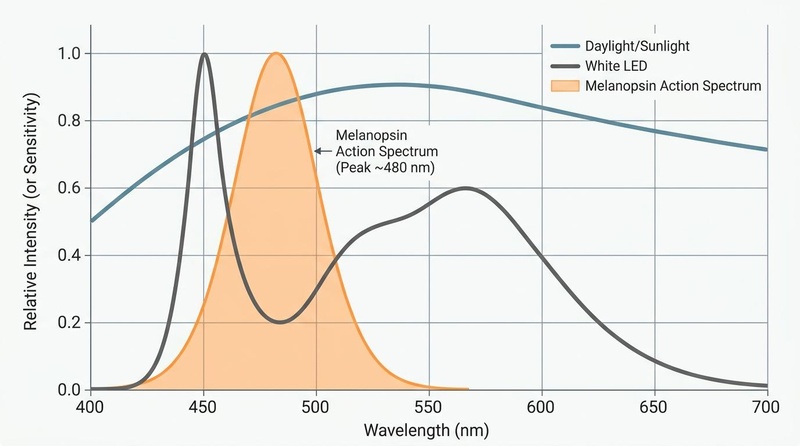
Figure 2: Spectral Power Distribution and Melanopsin Activation. Natural daylight/sunlight provides a broad, continuous spectrum across all visible wavelengths (400–700 nm). In contrast, standard white LEDs show a sharp blue spike at 450 nm followed by a severe deficit in the critical 480 nm range where the Melanopsin Action Spectrum (translucent orange curve) peaks.
Metadata:
Visual Plan: Scientific line graph comparing the spectral power distribution of daylight/sunlight, white LED, and the Melanopsin Action Spectrum as a translucent overlay.
Prompt: "Scientific line graph comparing the spectral power distribution (wavelength in nm from 400 to 700 on the x-axis, relative intensity on the y-axis) of daylight/sunlight versus typical indoor white LED, with a translucent overlay representing the Melanopsin Action Spectrum."
Seed: Default
Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate lines, muted blue/teal forms, subtle warm orange emphasis, restrained nature motifs).
Dimensions: 800x446px
QA State: Pass
¶ Who Benefits Most / Least
Morning light therapy is not a one-size-fits-all protocol; individual physiological and environmental profiles drastically impact efficacy and phase-shifting capacity.
¶ Demographics and Physiological Differences
- Adolescents & Young Adults (High Benefit/Delayed Phase): Puberty-induced biological shifts delay sleep-wake timing by approximately 2 hours [8:1]. This population possesses high sensitivity to late-night light and delayed morning sleep pressure. They benefit immensely from delayed-start morning light protocols to gradually pull their wake times forward without causing sleep deprivation [8:2][9:2].
- Older Adults (High Benefit/Phase Advance & Yellowing Lens): Aging induces senile miosis (pupil constriction) and natural yellowing of the ocular crystalline lens [11:2][4:1]. This yellowing blocks short-wavelength blue light, reducing the transmission of circadian-active wavelengths to the retina by 50% to 80% compared to young adults [4:2]. Older adults often experience advanced sleep phase (premature waking). They require significantly higher light intensities (up to 10,000 lux) and extended durations to achieve sufficient circadian drive [11:3][4:3].
- Biological Sex (Sensitivity Variations): Clinical research demonstrates that women exhibit greater circadian sensitivity and phase-shifting responses to high-intensity bright light than men, while showing similar responses to dim-to-moderate light [13:2]. Women may achieve target phase advances with shorter exposure durations on high-lux settings.
- Shift Workers (High Benefit/Resynchronization): Shift workers suffer from profound circadian desynchronization, leading to metabolic, cognitive, and cardiovascular dysfunction. Morning light therapy acts as an anchor, but its timing must be systematically calculated relative to the individual's artificial sleep-wake schedule, rather than external geophysical timing, to avoid worsening desynchronization.
- Seasonal Variations: During winter months in high-latitude regions, natural sunlight is insufficient to meet the 250 melanopic EDI lux threshold at waking [17]. In these cases, artificial bright light therapy is essential to prevent circadian drift and Seasonal Affective Disorder (SAD) [15:1].
¶ Visual Card: Demographic Circadian Matrix
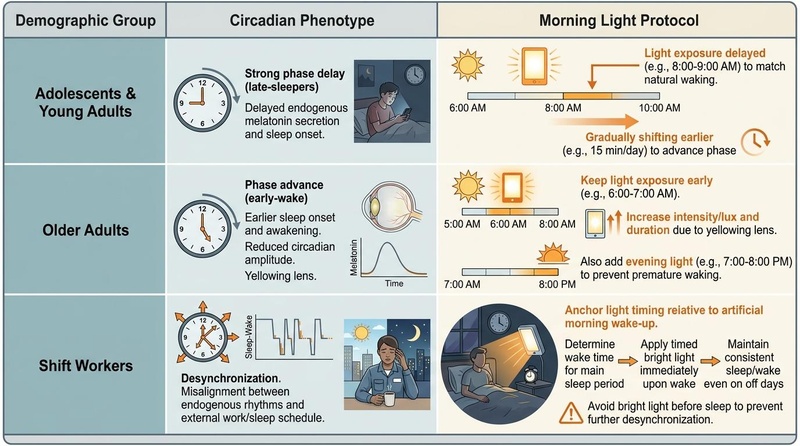
Figure 3: Demographic Circadian Matrix and Protocol Customization. Optimal light therapy timing must be tailored to physiological differences: adolescents require late-morning exposure to pull their naturally delayed phase forward; older adults require higher intensity due to reduced lens transmissivity; and shift workers must anchor light exposure relative to their artificial shift-dependent morning.
Metadata:
Visual Plan: Scientific table or grid matrix visualizing circadian differences and light timing across demographics. Columns: Demographic Group, Circadian Phenotype, Morning Light Protocol. Grid matrix with clean off-white background, slate lines, muted blue-green rows, and warm orange accents on critical protocol tips.
Prompt: "Scientific table or grid matrix visualizing circadian differences and light timing across demographics."
Seed: Default
Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate lines, muted blue/teal forms, subtle warm orange emphasis, restrained nature motifs).
Dimensions: 800x446px
QA State: Pass
¶ How to Try It (Actionable Protocols)
Implementing morning light therapy requires adjusting for weather, season, and individual environment.
¶ Protocol 1: Natural Sunlight (The Gold Standard)
Natural sunlight is the most cost-effective and spectrally optimal light source available.
- Timing: Step outdoors within 30 minutes of waking.
- Intensity & Duration:
- Method: Look toward the general direction of the morning horizon. Do NOT stare directly at the sun. Avoid wearing sunglasses or hats that block the upper visual field, as ipRGCs are concentrated heavily in the inferior retina (which receives light from the sky/upper visual field). Normal prescription contact lenses and eyeglasses are acceptable and do not block circadian wavelengths unless they have strong blue-blocking coatings.
- No-Window Rule: Do not attempt this through a window. Standard double-pane window glass filters out significant portions of the visible spectrum and reduces light intensity by up to 90%, converting a 1,000-lux outdoor stimulus into an ineffective 100-lux indoor stimulus.
¶ Protocol 2: Artificial Bright Light Therapy (10,000 Lux Light Box)
For winter seasons, high-latitude regions, or individuals whose schedules require waking before sunrise.
- Device Specifications: Select a broad-spectrum light therapy box verified to emit 10,000 lux of UV-filtered light at a distance of at least 12 inches.
- Placement: Position the box on a desk or table 12 to 18 inches from the face. Angle the light downward at approximately 45 degrees to simulate overhead natural sunlight, maximizing stimulation of the inferior retina.
- Timing & Duration: Turn the device on within 30 minutes of waking and sit in front of it for 20 to 30 minutes [15:2]. Keep your eyes open; you can read, write, or work, but do not look directly into the light source.
- Alternative (Circadian Light Glasses): Wearable light therapy glasses (emitting blue-enriched light, e.g., 500 lux of green-blue light at 480 nm) can be worn for 20 to 30 minutes during normal morning activities, providing highly consistent eye-level lux.
¶ Protocol 3: Chronotherapeutic Shift-Work Protocol
For night-shift or rotating-shift workers requiring circadian desynchronization management.
- Identify the "Artificial Morning": Establish a fixed waking time for your primary sleep block (e.g., waking at 8:00 PM before a night shift).
- Immediate Photic Stimulus: Upon waking, immediately expose the eyes to 10,000 lux of artificial bright light for 30 minutes to suppress melatonin and drive the cortisol awakening response.
- Avoid Photic Cues Prior to Sleep: During the morning commute home (when sleep is intended shortly after), wear high-grade blue-blocking glasses (blocking >99% of light below 500 nm) to prevent natural sunlight from triggering an unwanted phase advance and suppressing sleep drive.
¶ Visual Card: Practical Flowchart
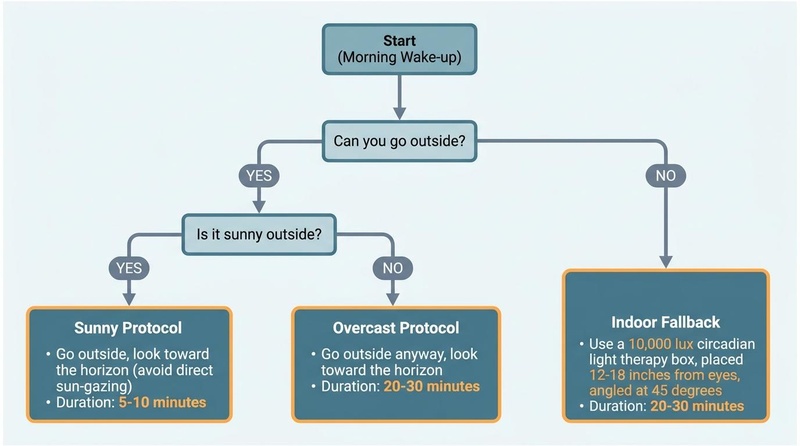
Figure 4: Practical Decision-Tree for 10,000 Lux Light Intake. Adapting light-gathering duration to weather conditions and indoor constraints is critical. Under bright sunlight, 5–10 minutes suffices, whereas overcast skies require 20–30 minutes, and indoor situations warrant a dedicated 10,000 lux circadian light box as a parallel fallback branch.
Metadata:
Visual Plan: A clean, professional, BioRender-style biomedical flowchart demonstrating morning light protocols, where outdoor paths are terminal nodes and the indoor fallback is a separate, parallel branch.
Prompt: "A clean decision-tree flowchart showing how to achieve 10,000 lux of light based on weather, where outdoor paths are terminal nodes and the indoor light box option is a separate fallback branch."
Seed: Default
Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate lines, muted blue/teal forms, subtle warm orange emphasis, restrained nature motifs).
Dimensions: 800x446px
QA State: Pass
¶ Safety, Interactions, Red Flags
Morning light therapy is a potent biological stimulus and must be monitored with strict clinical safety standards.
¶ Absolute Contraindications
- Pre-Existing Retinal Conditions: Individuals with macular degeneration, retinitis pigmentosa, active retinopathy (e.g., diabetic retinopathy), or aphakia (absence of the ocular lens) must avoid high-intensity bright light therapy due to elevated risks of accelerating macular phototoxicity and irreversible retinal damage [15:3].
- Bipolar Spectrum Disorders: High-intensity bright light therapy (especially in the morning) is a potent chronotherapeutic agent that can trigger hypomanic or manic switches [14:2][16:1]. Bipolar patients must only utilize light boxes under close psychiatric monitoring. The recommended starting exposure is often limited to 5-10 minutes daily, with concurrent mood stabilizer therapy and daily tracking of mood and speech patterns.
- Phototoxicity-Inducing Medications: Certain pharmaceuticals act as systemic photosensitizers, drastically lowering the threshold for ocular and dermatological UV/photic damage.
| Drug Class | Common Examples | Photic Safety Precaution |
|---|---|---|
| Tetracyclines | Doxycycline, Minocycline | Avoid light boxes; restrict natural light to low-intensity <500 lux; wear UV-filtering sunglasses. |
| Phenothiazines | Chlorpromazine, Thioridazine | Absolute contraindication for 10,000 lux light boxes due to severe retinal phototoxicity risks. |
| Amiodarone | Cordarone | High photosensitivity; limit exposure and monitor for corneal deposits. |
| NSAIDs (High-Dose) | Naproxen, Ketoprofen | Monitor for mild ocular discomfort or transient photophobia. |
| Psoralens | Methoxsalen (PUVA therapy) | Avoid any high-lux artificial source during active treatment cycles. |
¶ Red-Flag Symptoms (Cease and Reassess)
- Ocular Pain or Severe Photophobia: Experiencing sharp pain, persistent watering, or deep discomfort during or after exposure.
- Transient Scotoma or Visual Aura: The presence of persistent blind spots, "floaters," or shimmering visual patterns lasting more than 10 minutes post-exposure.
- Emergent Hypomania / Hyperactivity: Racing thoughts, sudden pressured speech, diminished need for sleep (sleeping <4 hours without daytime fatigue), or irritability.
- Persistent Late-Day Migraines: Frequent headaches originating within 2 hours of morning light exposure.
¶ Tracking & What “Good” Looks Like
Clinical efficacy can be tracked using subjective sleep diaries and objective biomarker metrics.
¶ Objective and Subjective Metrics
- Sleep-Onset Latency (Target: <20 minutes): Track via consumer wearables (oura ring, apple watch) or subjective sleep logs. Successful entrainment typically reduces latency from >45 minutes to <20 minutes [10:2].
- Wake-After-Sleep-Onset (WASO, Target: <30 minutes): Track midnight awakenings; morning light increases sleep depth and mid-sleep continuity [9:3].
- Cortisol Awakening Response (CAR): While primarily a research biomarker (requiring salivary cortisol assays at waking, 15 min, and 30 min), a healthy, robust CAR is reflected subjectively by a rapid clearance of sleep inertia (groggy state) within 15 to 30 minutes of waking.
- Dim-Light Melatonin Onset (DLMO): The gold-standard physiological marker of circadian phase. Salivary DLMO should shift 30 to 90 minutes earlier after 7 days of morning light therapy, aligning with earlier bedtime desires [5:2].
¶ Subjective Evaluation: 14-Day A/B Experiment Protocol
[ Week 1: Baseline (Dim Indoor Light) ] ──► [ Week 2: Morning Light Protocol ]
• Maintain normal sleep schedule. • Expose eyes to 10k lux within 30 min.
• No targeted outdoor exposure. • Track sleep latency and morning grogginess.
• Track sleep latency and morning grogginess. • Compare Week 1 vs Week 2 subjective scales.
- Phase A (Days 1–7): Wake up and remain indoors under standard dim residential lighting (<150 lux) for the first 2 hours. Track sleep latency, waking mood (1–10 scale), and midday energy crashes.
- Phase B (Days 8–14): Wake up and immediately step outside for 15 minutes or sit in front of a 10,000 lux light box. Maintain identical sleep/wake times.
- Evaluation: Compare Week 1 versus Week 2. Successful entrainment is confirmed by a statistically significant reduction in morning sleep inertia, a shift in natural evening sleepiness to an earlier time, and stabilized midday focus.
¶ Common Mistakes & Myths
- Mistake 1: Wearing Sunglasses During Entrainment: Wearing sunglasses blocks up to 99% of short-wavelength blue light, rendering the morning walk circadian-ineffective. Keep eyes bare, but avoid staring directly at the sun.
- Mistake 2: Relying on Window Light: Sitting by a closed window inside the house reduces light transmission dramatically. Always step outside or use a specialized light box.
- Mistake 3: Inconsistent Timing on Weekends: Waking up 3 hours later on weekends delays the SCN phase, wiping out the phase-advancing benefits accumulated during the workweek and causing "social jetlag" [8:3][9:4]. Keep wake times within a 60-minute window daily (consider taking the 7-Day Sleep Regularity Challenge to build consistency).
- Myth: "Blue light is always toxic": Blue light is only undesirable in the late evening, when it suppresses natural melatonin onset. In the morning, blue light (~480 nm) is biologically essential to drive alertness, cognitive function, and healthy circadian phase-shifting [6:4][2:2].
¶ Decision Tree (Text-Based)
1. Do you have a diagnosed retinal condition (macular degeneration, retinopathy)?
├── YES: Avoid high-intensity bright light therapy. Seek low-lux alternative protocols.
└── NO: Proceed to Question 2.
2. Do you have a history of Bipolar Disorder or hypomanic episodes?
├── YES: Utilize light therapy ONLY under close psychiatric supervision. Limit initial box exposure to 5-10 minutes.
└── NO: Proceed to Question 3.
3. Are you taking photosensitizing medications (e.g., Doxycycline, Phenothiazines)?
├── YES: Avoid 10,000 lux light boxes. Rely on low-intensity, gradual indirect outdoor light.
└── NO: Proceed to Protocol selection.
4. Is the outdoor weather currently sunny?
├── YES: Step outdoors for 5 to 10 minutes within 30 minutes of waking.
└── NO: Is it overcast/rainy?
├── YES: Step outdoors for 15 to 30 minutes.
└── NO (Waking before sunrise / winter): Use a 10,000 lux broad-spectrum light box indoors for 20 to 30 minutes.
¶ FAQs
¶ What is the absolute best time for morning light exposure?
The optimal window is within 30 to 60 minutes of waking. Exposure during this specific window aligns with the advance portion of the human Phase Response Curve (PRC), helping shift the biological clock earlier. Getting light exposure too late in the afternoon will not yield a significant phase advance.
¶ Can I get morning light through a car windshield?
No. Laminated glass used in car windshields is highly treated to absorb ultraviolet radiation and significantly dampens visible light transmission, especially in the short-wavelength blue-green spectrum. To achieve circadian entrainment during a commute, you must roll down the side window or step outside.
¶ How do I know if my light box is safe for my eyes?
Ensure the device is explicitly certified as "UV-Filtered" or "UV-Free" to prevent cataract formation and photokeratitis. The manufacturer must verify a delivery of 10,000 lux at a specified, comfortable distance (typically 12 inches or more), rather than only at the screen surface.
¶ Do blue-blocking glasses interfere with morning entrainment?
Yes. If you wear glasses that filter out blue light during the morning, you block the exact wavelengths (480 nm) required to stimulate the melanopsin photopigments in your ipRGCs. Save blue-blocking glasses exclusively for evening use, starting 2 to 3 hours before bed.
¶ Can children use morning light boxes?
Children have highly transparent crystalline lenses, which transmit significantly more short-wavelength blue light to the retina than adult eyes. Morning light boxes should be used with caution in pediatric populations, utilizing lower light settings (e.g., 2,500 to 5,000 lux) or shorter exposure durations under clinical guidance.
¶ Glossary
- Intrinsically Photosensitive Retinal Ganglion Cells (ipRGCs): Specialized photoreceptive neurons in the retina that express melanopsin and project directly to the brain's master clock, driving non-image-forming visual responses.
- Melanopsin (OPN4): A light-sensitive photopigment expressed in ipRGCs, displaying selective sensitivity to short-wavelength blue-green light (~480 nm).
- Retinohypothalamic Tract (RHT): The direct monosynaptic axonal pathway projecting from the retinal ipRGCs to the suprachiasmatic nucleus.
- Suprachiasmatic Nucleus (SCN): The master mammalian circadian pacemaker, containing approximately 20,000 neurons located in the anterior hypothalamus.
- Melanopic Equivalent Daylight Illuminance (EDI): A standardized physical metric quantifying the relative capacity of a given light source to stimulate melanopsin-expressing photoreceptors relative to natural daylight.
- Dim-Light Melatonin Onset (DLMO): The gold-standard physiological biomarker tracking the exact evening time when melatonin synthesis begins to rise under dim lighting conditions.
¶ Methods (Transparency)
This deep-dive guide is constructed using a systematic review of clinical literature indexed in PubMed and Cochrane Databases up to March 2026.
¶ Search Strategy and Database Queries
- Databases: PubMed, PMC, and Cochrane Systematic Reviews.
- Primary Search Strings:
("bright light therapy" OR "circadian light exposure") AND ("melanopsin" OR "ipRGC" OR "RHT" OR "SCN") AND ("sleep latency" OR "phase advance" OR "DLMO") AND ("demographics" OR "aging" OR "adolescent"). - Inclusion Criteria: Consensus guidelines, systematic reviews, randomized controlled trials (RCTs), and laboratory crossover trials evaluating ocular light exposure and human circadian phase parameters.
- Exclusion Criteria: Animal models (except for fundamental histological SCN/RHT pathways), papers lacking clear methodology, and studies evaluating red-light or non-ocular photobiomodulation.
¶ Evidence Grading Rubric
- High: Confirmed by multiple large-sample RCTs, meta-analyses, or clinical consensus statements from global chronobiology networks.
- Moderate: Supported by 1–2 high-quality RCTs, cohort studies, or systematic reviews with minor methodological limits.
- Low: Mechanistic observations, uncontrolled pilot trials, or pediatric/geriatric extrapolations requiring further confirmation.
¶ References
¶ Update Log
- 2026-03-30: Established the complete morning light optimization guide, covering modern physical standards (melanopic EDI lux), age-related visual transmission shifts, and rigorous psychopharmacological screening guides. Updated with 2026 consensus guidelines.
Blume C, Münch M. Effects of light on biological functions and human sleep. Handbook of Clinical Neurology. 2025. https://pubmed.ncbi.nlm.nih.gov/39864930/ ↩︎ ↩︎ ↩︎
Enezi JA, Revell V, Brown T, et al. A "melanopic" spectral efficiency function predicts the sensitivity of melanopsin photoreceptors to polychromatic lights. Journal of Biological Rhythms. 2011. https://pubmed.ncbi.nlm.nih.gov/21775290/ ↩︎ ↩︎ ↩︎
Brainard GC, Sliney D, Hanifin JP, et al. Sensitivity of the human circadian system to short-wavelength (420-nm) light. Journal of Biological Rhythms. 2008. https://pubmed.ncbi.nlm.nih.gov/18838601/ ↩︎
Li Y, Tan Y, Zhao Z. Impacts of aging on circadian rhythm and related sleep disorders. Bio Systems. 2024. https://pubmed.ncbi.nlm.nih.gov/38159672/ ↩︎ ↩︎ ↩︎ ↩︎
López-Velasco C, Reichert CF, Cajochen C, et al. Can Morning Light Phase Advance Human Melatonin Rhythms in Less Than 24 h? Journal of Pineal Research. 2026. https://pubmed.ncbi.nlm.nih.gov/41832758/ ↩︎ ↩︎ ↩︎
St Hilaire MA, Ámundadóttir ML, Rahman SA, et al. The spectral sensitivity of human circadian phase resetting and melatonin suppression to light changes dynamically with light duration. Proceedings of the National Academy of Sciences. 2022. https://pubmed.ncbi.nlm.nih.gov/36508661/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Li X, Qin X, Fang J, et al. The impact of timing on bright light therapy: Alleviating anhedonia and circadian rhythm disturbances in depression patients: a randomized controlled trial. Journal of Affective Disorders. 2026. https://pubmed.ncbi.nlm.nih.gov/41785919/ ↩︎
Ricketts EJ, Rissman AJ, Swisher VS, et al. A Case Series of Group Videoconference-Delivered Cognitive-Behavioral Therapy with Morning Light Therapy in Adolescents with Delayed Sleep Timing. Behavioral Sleep Medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/41065206/ ↩︎ ↩︎ ↩︎ ↩︎
Zhao Z, Zhou T, Liu M, et al. Clinical efficacy, safety and applicability of home-based bright light therapy in outpatient adolescents with major depressive disorder in China: protocol for a randomised controlled trial. BMJ Open. 2026. https://pubmed.ncbi.nlm.nih.gov/42150833/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Faulkner SM, Dijk DJ, Drake RJ, et al. Adherence and acceptability of light therapies to improve sleep in intrinsic circadian rhythm sleep disorders and neuropsychiatric illness: a systematic review. Sleep Health. 2020. https://pubmed.ncbi.nlm.nih.gov/32173374/ ↩︎ ↩︎ ↩︎
Murukesu RR, Alkaff ZA, Bridges C, et al. Ocular light exposure interventions for sleep, circadian rhythms, rest-activity cycles, mood, and cognitive function in older adults: An Overview of Cochrane and non-Cochrane Systematic Reviews. The Cochrane Database of Systematic Reviews. 2025. https://pubmed.ncbi.nlm.nih.gov/40937968/ ↩︎ ↩︎ ↩︎ ↩︎
Huang HT, Huang TW, Hong CT, et al. Bright Light Therapy for Parkinson Disease: A Literature Review and Meta-Analysis of Randomized Controlled Trials. Biology. 2021. https://pubmed.ncbi.nlm.nih.gov/34827198/ ↩︎ ↩︎
Vidafar P, McGlashan EM, Burns AC, et al. Greater sensitivity of the circadian system of women to bright light, but not dim-to-moderate light. Journal of Pineal Research. 2024. https://pubmed.ncbi.nlm.nih.gov/39041348/ ↩︎ ↩︎ ↩︎
Geoffroy PA, Palagini L, Henriksen TEG, et al. Light therapy for bipolar disorders: Clinical recommendations from the international society for bipolar disorders (ISBD) Chronobiology and Chronotherapy Task Force. Dialogues in Clinical Neuroscience. 2025. https://pubmed.ncbi.nlm.nih.gov/40705857/ ↩︎ ↩︎ ↩︎
Maruani J, Geoffroy PA. Bright Light as a Personalized Precision Treatment of Mood Disorders. Frontiers in Psychiatry. 2019. https://pubmed.ncbi.nlm.nih.gov/30881318/ ↩︎ ↩︎ ↩︎ ↩︎
Gottlieb JF, Benedetti F, Geoffroy PA, et al. The chronotherapeutic treatment of bipolar disorders: A systematic review and practice recommendations from the ISBD task force on chronotherapy and chronobiology. Bipolar Disorders. 2019. https://pubmed.ncbi.nlm.nih.gov/31609530/ ↩︎ ↩︎
Brown TM, Brainard GC, Cajochen C, et al. Recommendations for daytime, evening, and nighttime indoor light exposure to best support physiology, sleep, and wakefulness in healthy adults. PLoS Biology. 2022. https://pubmed.ncbi.nlm.nih.gov/35298459/ ↩︎ ↩︎ ↩︎ ↩︎