¶ Statins
| Indication | Hypercholesterolemia, ASCVD Prevention |
| Access | Prescription (Rx) |
| Dosing schedule | Daily (Oral) |
| Safety Profile | Well characterized; varies by drug and dose |
| Key Marker | LDL-C, ApoB, ALT, CK |
3-Hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors, commonly known as statins, are the cornerstone of lipid-lowering pharmacological therapy. They are primarily utilized to reduce low-density lipoprotein cholesterol (LDL-C) and apolipoprotein B (ApoB) to prevent atherosclerotic cardiovascular disease (ASCVD) events, supported by high-certainty clinical trial evidence.
PREGNANCY AND BREASTFEEDING
The FDA removed the class-wide pregnancy contraindication in 2021. Most pregnant patients should still stop statins, but continued treatment may be considered with a specialist for a small group at very high cardiovascular risk. An unintended early-pregnancy exposure is unlikely to harm the fetus. People who need to continue a statin should not breastfeed.[1]
¶ At a glance
¶ Aliases
- Also known as: HMG-CoA reductase inhibitors, cholesterol-lowering drugs
- Chemical/Class name: 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors
- Category: Pharmacological lipid-lowering therapeutics
¶ Key points
- Established Efficacy: Statins produce a dose-dependent reduction in circulating LDL-C (30% to over 50%) and provide a consistent 21% relative reduction in major vascular events per 1 mmol/L (~38.7 mg/dL) decrease in LDL-C.[2][3]
- Baseline-Risk Dependence: While relative risk reduction is uniform across patient groups, the absolute clinical benefit is directly proportional to baseline cardiovascular risk, offering substantial event prevention in secondary prevention and high-risk primary prevention cohorts.[4][3:1]
- Muscle Symptom Reality: Muscle symptoms are frequently reported, but large blinded trials find only a small excess with statins versus placebo. In SAMSON—a 60-person crossover trial of people who had previously stopped statins because of symptoms—the symptom burden triggered by taking a tablet was similar with atorvastatin and placebo; this finding should not be generalized to mean that 90% of every patient's symptoms are psychological.[5][6][7]
- Metabolic and Liver Safety: Statins are associated with a dose-dependent, modest increase in new-onset diabetes risk, primarily concentrated in individuals with pre-existing metabolic syndrome, while severe drug-induced liver injury is exceptionally rare.[8][9]
¶ What people use it for
- Main goals: Atherosclerotic cardiovascular disease (ASCVD) prevention, LDL-C and ApoB reduction, plaque stabilization.
- Evidence quality (overall): High (supported by multiple large-scale individual participant data meta-analyses and double-blind randomized clinical trials).
¶ What is it?
¶ Definition
Statins are a class of synthetic and naturally derived small-molecule therapeutics that competitively inhibit HMG-CoA reductase, the rate-limiting enzyme in the hepatic cholesterol biosynthesis pathway.[10]
¶ Chemistry and Formulations
The statin class is pharmacologically segmented based on physicochemical properties into lipophilic and hydrophilic compounds:
- Lipophilic Statins (e.g., Atorvastatin, Simvastatin, Lovastatin): These compounds passively diffuse through cell membranes and distribute widely into extrahepatic tissues, undergoing extensive Cytochrome P450 (particularly CYP3A4) metabolism.[11]
- Hydrophilic Statins (e.g., Rosuvastatin, Pravastatin): These compounds utilize active membrane transporters (such as Organic Anion Transporting Polypeptide 1B1, SLCO1B1) to target hepatocytes selectively, displaying minimal extrahepatic penetration and minimal CYP3A4 metabolism.[12][11:1]
¶ Current Regulatory Status
Statins are prescription medicines in the United States and many other jurisdictions. Approved indications and product labeling differ by drug and country; clinical guidelines recommend statins for selected primary-prevention patients and for many people with established ASCVD.[2:1][4:1]
¶ Key Pharmacological Property
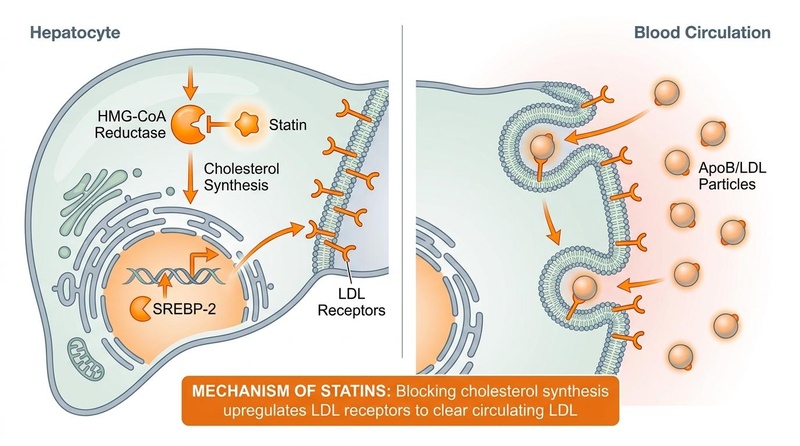
Statins function as hepatic-targeted competitive inhibitors of HMG-CoA reductase, triggering a cellular signaling cascade that upregulates low-density lipoprotein receptors (LDLR) to accelerate the clearance of atherogenic ApoB-containing lipoproteins from the bloodstream.[10:1]
¶ Main benefits
The primary clinical utility of statin therapy is the prevention of major adverse cardiovascular events (MACE), including myocardial infarction, ischemic stroke, and coronary revascularization.
¶ Secondary Prevention (Established ASCVD)
In patients with established ASCVD (history of myocardial infarction, acute coronary syndrome, stroke, transient ischemic attack, or peripheral arterial disease), statin therapy provides profound absolute risk reductions.[2:2]
- Efficacy: Intensive lipid lowering using high-intensity statins (e.g., Atorvastatin 80 mg or Rosuvastatin 40 mg) reduces major vascular events by an additional 15% compared to standard-dose regimens.[13]
- Target Thresholds: Clinical guidelines commonly recommend high-intensity statin therapy to lower LDL-C by from baseline. The 2026 ACC/AHA guideline recommends an LDL-C goal below 55 mg/dL (1.4 mmol/L) for secondary-prevention patients at very high risk; less intensive goals may apply to other groups.[2:3]
¶ Primary Prevention and Baseline-Risk Dependence
In primary prevention (individuals with no clinical history of ASCVD), the decision to initiate statin therapy is guided by the patient’s baseline absolute cardiovascular risk and the presence of risk-enhancing factors.[2:4][4:2]
- The 21% Rule: Individual participant data (IPD) meta-analyses from the Cholesterol Treatment Trialists' (CTT) Collaboration demonstrate that every 1 mmol/L (~38.7 mg/dL) reduction in LDL-C consistently reduces the relative risk of major vascular events by approximately 21% (RR 0.79, 95% CI 0.77–0.81).[3:2] This relative benefit remains constant across all risk groups, including those at low baseline risk ( 5-year cardiovascular risk).[3:3]
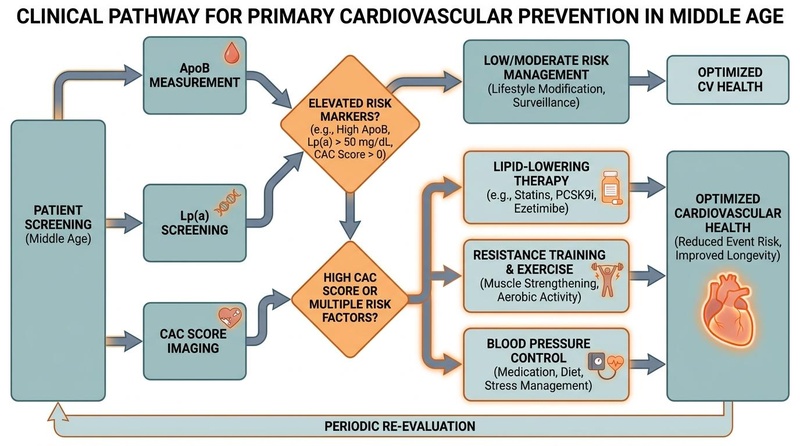
- Absolute vs. Relative Benefit: While the relative risk reduction is constant, the absolute clinical benefit (number of events prevented) depends entirely on the patient's baseline risk. In high-risk cohorts, the absolute risk reduction is substantial, whereas in very low-risk cohorts, the absolute benefit is small, making the risk-benefit balance highly sensitive to individual baseline characteristics.[4:3][3:4] For patients with borderline or intermediate baseline risk, coronary artery calcium (CAC) scoring is frequently utilized to reclassify risk and guide the clinical decision to initiate statin therapy.
¶ Regional Guidelines and Intensity Frameworks
Lipid management guidelines globally utilize standardized risk-stratification models to define statin initiation thresholds:
- ACC/AHA (2026): Uses the PREVENT equations for 10- and 30-year risk assessment in adults aged 30 to 79, followed by personalization with risk-enhancing factors and selective CAC scoring. Statin intensity is categorized by the expected percentage reduction in LDL-C.[2:5]
- USPSTF (2022): Recommends statin initiation for primary prevention in adults aged 40 to 75 years with cardiovascular risk factor (dyslipidemia, diabetes, hypertension, smoking) and an estimated 10-year CVD risk of (Grade B recommendation). For individuals with a 10-year risk of to , a Grade C recommendation suggests selective, individual clinical decision-making.[4:4]
- Canadian Cardiovascular Society (CCS) (2021): Recommends utilizing the Framingham Risk Score (FRS) or Cardiovascular Life Expectancy Model (CLEM), advising statin initiation in high-risk individuals (FRS ) and moderate-risk individuals (FRS to ) with LDL-C mmol/L ( mg/dL) or other risk-enhancing features.[14]
¶ System-Specific Benefits
- Cardiovascular System: Promotes the structural stabilization of vulnerable coronary atherosclerotic plaques, improves endothelial nitric oxide synthase (eNOS) activity, and reduces vascular inflammation (as measured by high-sensitivity C-reactive protein, hs-CRP).[9:1]
- Cerebrovascular System: Lowers the incidence of ischemic stroke and transient ischemic attacks.[3:5]
- Hepatic System: Statins are safe in patients with non-alcoholic fatty liver disease (NAFLD) or non-alcoholic steatohepatitis (NASH), showing improvements in liver transaminases and overall cardiovascular outcomes in this high-risk population.[15]
¶ Evidence summary table (human outcomes)
The clinical evidence for statins is derived from robust double-blind randomized controlled trials (RCTs) and comprehensive individual participant data meta-analyses.
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Vascular Events (Secondary Prevention) | High | High | 26 RCTs | Standard high-intensity regimens reduce vascular events by an additional 15% relative to moderate regimens.[13:1] | |
| Vascular Events (Primary Prevention) | High | High | 27 RCTs | Consistent 21% relative risk reduction per 1 mmol/L LDL-C reduction; absolute benefit is baseline-risk dependent.[4:5][3:6] | |
| LDL-C Clearance | High | High | >50 RCTs | High-intensity statins lower LDL-C by ; moderate-intensity by 30% to 49%.[2:6] | |
| New-Onset Diabetes | High | High | 23 RCTs | Hazard ratio of 1.10 for moderate-intensity and 1.36 for high-intensity; risk concentrated in prediabetes.[8:1] | |
| Muscle Pain / Myalgia | High | High | 19 RCTs | Absolute excess of 11 reports per 1,000 person-years in year 1 in the CTT analysis; most symptom reports in blinded trials were not caused by the statin.[5:1][6:1][7:1] | |
| Hepatic Transaminase Elevation | High | High | >25 RCTs | ALT/AST elevations ULN occur in of patients; typically transient, self-limiting, and reversible.[9:2][15:1] | |
| Cognition / Dementia | Moderate | Moderate | RCTs & cohorts | Randomized evidence has not shown a convincing adverse cognitive effect. Whether statins prevent dementia remains uncertain; observational associations cannot establish causation.[16][17] |
- Effect: Direction and relative magnitude of effect: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Impact direction indicated as: (p) positive health outcome, (n) negative health outcome, (x) neutral/unclear outcome.
- Consistency: Low (conflicting results), Moderate (mixed evidence leaning one way), High (strong agreement across trials).
- Trials: Number of randomized controlled trials informing this outcome.
¶ Mechanisms
The molecular pharmacology of statins extends from biochemical enzyme inhibition to systemic cellular adaptation and receptor-mediated clearance.
+-------------------------------------------------------------+
| Statin Molecule |
+-------------------------------------------------------------+
|
| (Competitively Inhibits)
v
+-------------------------------------------------------------+
| Hepatic HMG-CoA Reductase |
+-------------------------------------------------------------+
|
| (Blocks Mevalonate Pathway)
v
+-------------------------------------------------------------+
| Intracellular Cholesterol Synthesis |
+-------------------------------------------------------------+
|
| (Triggers Nuclear Translocation)
v
+-------------------------------------------------------------+
| SREBP-2 Activation & DNA Binding |
+-------------------------------------------------------------+
|
| (Upregulates Transcription)
v
+-------------------------------------------------------------+
| LDL Receptors (LDLR) on Hepatocyte Membrane |
+-------------------------------------------------------------+
|
| (Accelerates Endocytosis)
v
+-------------------------------------------------------------+
| Clearance of Circulating ApoB / LDL Particles |
+-------------------------------------------------------------+
¶ 1. Competitive Inhibition of HMG-CoA Reductase
Statins possess a chemical moiety that structurally mimics the natural substrate HMG-CoA.[10:2] They competitively bind to the active site of HMG-CoA reductase, the catalytic enzyme that converts HMG-CoA to mevalonate in hepatocytes.[10:3] This competitive blockade halts the rate-limiting step of endogenous cholesterol synthesis.
¶ 2. Upregulation of hepatic LDL Receptors (LDLR)
The reduction in hepatocyte cholesterol content activates a homeostatic cellular sensing mechanism:[10:4]
- SREBP-2 Activation: Depleted intracellular cholesterol levels trigger the proteolytic cleavage and activation of Sterol Regulatory Element-Binding Protein 2 (SREBP-2) in the endoplasmic reticulum.[10:5]
- Nuclear Translocation: Activated SREBP-2 translocates to the nucleus and binds to sterol regulatory elements (SRE) on the DNA, upregulating the transcription of the gene encoding the LDL receptor.[10:6]
- Membrane Insertion & Clearance: Newly synthesized LDL receptors are transported to the hepatocyte cell membrane.[10:7] These receptors bind circulating ApoB-containing lipoproteins (LDL and VLDL remnants) with high affinity, internalizing them via receptor-mediated endocytosis and degrading them in lysosomes, which results in a marked decrease in circulating blood lipids.[10:8]
¶ 3. Pleiotropic Effects (Non-Lipid Mechanisms)
In addition to lowering lipids, statins exert valuable clinical effects by blocking other downstream intermediates of the mevalonate pathway, notably isoprenoids (geranylgeranyl pyrophosphate and farnesyl pyrophosphate):[9:3]
- Endothelial Function: Isoprenoid depletion prevents the isoprenylation of Rho/Ras family GTPases, upregulating endothelial nitric oxide synthase (eNOS) and improving vascular reactivity.[9:4]
- Plaque Stabilization: Statins inhibit macrophage proliferation within atheromatous plaques, reducing the secretion of matrix metalloproteinases (MMPs) that degrade the protective fibrous cap of plaques, thereby reducing plaque rupture risk.[9:5]
- Anti-Inflammatory Action: Decreased isoprenylation attenuates pro-inflammatory signaling pathways (NF-κB), leading to a reduction in systemic inflammatory biomarkers such as hs-CRP.[9:6]
¶ 4. Pharmacokinetic Profiles: Lipophilic vs. Hydrophilic
The metabolic and transport pathways of individual statins dictate their systemic exposure, potential for drug interactions, and tissue distribution:
- Lipophilic Statins (Atorvastatin, Simvastatin, Lovastatin):
- Absorption: Passively absorbed across hepatic membranes. They exhibit higher extrahepatic tissue penetration (skeletal muscle, adipose tissue) due to their lipophilicity.[11:2]
- Metabolism: Heavily dependent on the Cytochrome P450 3A4 (CYP3A4) enzyme system.[11:3] Concomitant use of strong CYP3A4 inhibitors dramatically increases systemic concentrations, elevating muscle toxicity risks.[11:4]
- Hydrophilic Statins (Rosuvastatin, Pravastatin):
- Absorption: Require active uptake transporters, primarily OATP1B1 (encoded by the SLCO1B1 gene), to enter hepatocytes.[12:1] Their hydrophilic nature restricts passive diffusion into extrahepatic tissues such as skeletal muscle.[12:2][11:5]
- Metabolism: Rosuvastatin undergoes minimal CYP metabolism (primarily CYP2C9), and pravastatin is metabolized via non-enzymatic degradation, making them highly resistant to CYP3A4 drug-drug interactions.[11:6]
¶ Dosage & Protocols
Statin prescribing is standardized around potency-driven clinical intensity classes to achieve target LDL-C percentage reductions.
¶ Statin Intensity Classification Table
The ACC/AHA framework categorizes statins into three intensity levels based on their expected LDL-C lowering capacity:[2:7]
| Statin Intensity | Expected LDL-C Reduction | Eligible Statin Regimens & Daily Doses |
|---|---|---|
| High Intensity | Atorvastatin 40–80 mg Rosuvastatin 20–40 mg |
|
| Moderate Intensity | to | Atorvastatin 10–20 mg Rosuvastatin 5–10 mg Simvastatin 20–40 mg Pravastatin 40–80 mg Lovastatin 40 mg Fluvastatin XL 80 mg |
| Low Intensity | Simvastatin 10 mg Pravastatin 10–20 mg Lovastatin 20 mg Fluvastatin 20–40 mg |
¶ Initiation and Monitoring Protocols
- Baseline Evaluation: Before treatment, clinicians generally obtain a lipid panel and baseline ALT. Fasting is not required for every lipid panel, and baseline CK is usually reserved for people with muscle symptoms, a history of muscle disease, or other myopathy risk factors.[2:8][9:7][18]
- Follow-up Testing: Lipid levels are typically re-evaluated 4 to 12 weeks after initiation or a dose adjustment to assess adherence and response.[2:9] Subsequent monitoring intervals are individualized according to risk, treatment changes, and whether results would alter management.[2:10]
- Hepatocellular and Myocellular Assessment: Routine, periodic monitoring of ALT, AST, or CK during ongoing, asymptomatic statin therapy is not clinically recommended.[9:8][18:1] Transaminases and CK should be assessed only if clinical symptoms of hepatotoxicity (e.g., jaundice, abdominal pain) or myopathy (e.g., unexplained muscle pain or weakness) manifest.[9:9][18:2]
¶ Special Populations
¶ Older Adults
Clinical trial data confirm that older adults derive substantial cardiovascular benefits from statin therapy, especially in secondary prevention.[19][20]
- Efficacy: IPD meta-analyses of patients aged years demonstrate a 26% relative reduction in major vascular events per 1 mmol/L LDL-C reduction with statin or non-statin lipid-lowering therapies.[20:1]
- Clinical Considerations: In primary prevention for individuals aged , the absolute benefit is weighed against remaining life expectancy, comorbidities, and polypharmacy, often warranting starting at moderate-intensity doses.[19:1]
¶ Chronic Kidney Disease (CKD)
Many patients with CKD have substantially elevated cardiovascular risk, but the magnitude varies with age, kidney function, albuminuria, diabetes, and existing vascular disease.[21]
- Non-Dialysis CKD (Stages 3–5): KDIGO guidelines recommend initiating a statin or a statin/ezetimibe combination (e.g., Simvastatin 20 mg plus Ezetimibe 10 mg, as validated in the SHARP trial) in all adults aged years with non-dialysis-dependent Stage 3–5 CKD (eGFR mL/min/1.73m²), regardless of baseline LDL-C.[21:1][22]
- Maintenance Dialysis: Initiating statin therapy is not recommended in patients who are already on maintenance hemodialysis or peritoneal dialysis, as large RCTs have shown no significant reduction in cardiovascular events in this specific end-stage cohort.[21:2][22:1]
¶ Pregnancy and Lactation
- First-Trimester Exposure: A 2026 Japanese consultation-based cohort found no statistically significant increase in major congenital malformations after early-pregnancy exposure, consistent with the FDA's conclusion that unintended early exposure is unlikely to harm the fetus. Observational data cannot exclude every risk.[23][1:1]
- Regulatory Status: The FDA removed the class-wide pregnancy contraindication in 2021 because an absolute ban was not appropriate for the small group of patients at very high cardiovascular risk. It still advises discontinuing statins in most pregnancies and making an individualized decision for patients with conditions such as homozygous familial hypercholesterolemia or established cardiovascular disease.[1:2]
- Breastfeeding: Patients who require ongoing statin therapy should not breastfeed; those who can pause treatment may resume it after breastfeeding ends in consultation with their clinician.[1:3]
¶ Safety and side effects
Statin safety is well characterized from large randomized trials and decades of clinical use. Most adverse effects are mild or uncommon, while a small number require prompt clinical assessment.
¶ Muscle Symptoms and the Nocebo Effect (SAMS)
Statin-associated muscle symptoms (SAMS)—predominantly presenting as symmetrical, proximal myalgia or muscle weakness—are the most common reason for statin discontinuation in real-world cohorts.[18:3]
- The RCT vs. Cohort Discrepancy: While observational cohort studies report SAMS rates of 10% to 15%, large-scale double-blind randomized placebo-controlled trials reveal a very different reality.[5:2][24]
- CTT 2022 Individual Participant Data: In a meta-analysis of 19 double-blind trials (123,940 participants) over a median of 4.8 years, of patients randomized to statins reported muscle pain or weakness, compared to randomized to placebo (RR 1.03, 95% CI 1.01–1.06).[5:3] This indicates that only about 1 in 15 reported cases of muscle symptoms are biologically caused by the drug itself, representing an absolute excess of only 11 episodes per 1,000 patient-years.[5:4]
- The SAMSON and StatinWISE Trials: In SAMSON, 60 people who had previously stopped statins because of symptoms cycled through atorvastatin, placebo, and no-tablet months. The trial's nocebo ratio was 0.90 because symptom scores increased similarly during statin and placebo months compared with no-tablet months.[6:2] StatinWISE likewise found no overall difference in muscle symptom scores between statin and placebo periods.[7:2] These trials show why blinded rechallenge can be informative; they do not prove that any individual symptom is unreal or that 90% of symptoms in the general population are caused by expectation.
¶ Rhabdomyolysis
Rhabdomyolysis—defined as severe muscle injury with CK elevation the upper limit of normal (ULN) accompanied by renal impairment, dark urine, or myoglobinuria—is an exceptionally rare complication.[10:9]
- Incidence: The true incidence of statin-induced rhabdomyolysis is approximately 1.6 cases per 100,000 patient-years.[10:10]
- Predisposing Risk Factors: Clinically significant risk factors include advanced age ( years), female sex, untreated hypothyroidism, compromised renal function (CKD), and the concurrent use of high-dose statins alongside potent CYP3A4-inhibiting drugs.[10:11][18:4]
¶ New-Onset Diabetes Risk
Statin therapy is associated with a dose-dependent, modest increase in the incidence of new-onset diabetes mellitus.[8:2]
- Relative Hazards: CTT individual participant data meta-analyses demonstrate that low-to-moderate intensity statins increase the hazard of new-onset diabetes by 10% (HR 1.10, 95% CI 1.04–1.16), whereas high-intensity statin regimens increase the hazard by 36% (HR 1.36, 95% CI 1.14–1.62).[8:3]
- Risk Concentration: This metabolic risk is highly concentrated in patients who already have pre-existing risk factors for diabetes, such as prediabetes (HbA1c ), obesity, severe insulin resistance, or metabolic syndrome.[8:4] For these individuals, statins slightly accelerate the transition to a formal diabetes diagnosis.[8:5]
- Net Cardiovascular Benefit: The absolute cardiovascular events prevented by statin therapy (e.g., myocardial infarctions and strokes) significantly outweigh the glycemic risks of a modest increase in HbA1c, even within diabetic or prediabetic cohorts.[8:6]
¶ Hepatocellular Safety and Liver Monitoring
- Transaminase Elevations: Asymptomatic, transient elevations of alanine aminotransferase (ALT) or aspartate aminotransferase (AST) ULN occur in fewer than 1% of patients starting statins.[9:10] These elevations are typically self-limiting and resolve spontaneously or with a minor dose reduction.[9:11][15:2]
- Drug-Induced Liver Injury (DILI): True, clinically significant drug-induced liver injury is exceptionally rare, occurring at a rate of approximately 1 in 100,000 patients.[9:12]
- Monitoring Shift: Because transaminase elevations are transient and serious hepatotoxicity is extremely rare, routine periodic monitoring of liver enzymes during ongoing therapy is no longer recommended.[9:13] ALT/AST should only be checked at baseline, and then subsequently if clinical symptoms of liver dysfunction emerge.[9:14]
¶ Cognitive and Dementia Claims
Postmarketing reports raised concern about memory problems, but randomized trials and systematic reviews have not shown a convincing adverse effect on objective cognition.[17:1]
- Dementia prevention: The Cochrane review evaluated statins started in cognitively healthy people in later life and found insufficient evidence that they prevent dementia or cognitive decline.[16:1]
- Observational evidence: Some cohort studies report lower dementia incidence among statin users, but such observational associations are vulnerable to healthy-user bias and other confounding, and should not be presented as proof that statins prevent dementia.[16:2][17:2]
¶ Statin Intolerance, Rechallenge, and Alternative Therapeutics
Statin intolerance is clinically defined as the inability to tolerate a statin dose necessary to meet risk-reduction goals due to unacceptable side effects.[18:5]
- True Prevalence: While cohort studies report much higher rates, a global meta-analysis of 176 studies (4.14 million patients) revealed the overall prevalence of statin intolerance is 9.1%, dropping to just 4.9% when evaluated in double-blind RCTs, confirming that true biological intolerance is uncommon.[24:1]
- EAS Rechallenge Protocol: In patients presenting with muscle symptoms, clinical protocols suggest a structured approach:[18:6]
- Temporarily hold the statin for a washout period of 2 to 4 weeks to allow symptoms to resolve.[18:7]
- Rechallenge the patient with a low dose of a different statin (such as Rosuvastatin 5 mg daily or Pravastatin, which are hydrophilic and avoid the CYP3A4 pathway).[18:8]
- Consider alternate-day dosing (e.g., Rosuvastatin 5 mg to 10 mg three times weekly), which is often well tolerated and highly effective.[18:9]
- Non-Statin Alternatives: For patients with confirmed, complete statin intolerance who cannot achieve target LDL-C levels, several non-statin lipid-lowering therapies are clinically validated:[2:11]
- Ezetimibe: Inhibits NPC1L1-mediated cholesterol absorption in the small intestine, providing an additional 15% to 20% LDL-C reduction.[22:2]
- PCSK9 Inhibitors (e.g., Alirocumab, Evolocumab): Monoclonal antibodies that prevent the degradation of LDL receptors, delivering powerful LDL-C reductions of 50% to 60%.[2:12]
- Bempedoic Acid: Inhibits ATP-citrate lyase upstream of HMG-CoA reductase, functioning as a prodrug activated selectively in liver tissue to avoid muscle tissue exposure and muscle-related side effects.[2:13]
¶ Shared Decision-Making and Clinical Stopping Rules
Statin therapy should be guided by a shared decision-making process that weighs baseline ASCVD risk, patient preferences, potential side effects, and the absolute magnitude of benefit.[2:14][4:6]
- Clinical Stopping Rules:
- Unexplained CK Elevation ULN: This requires prompt clinical assessment and usually immediate statin discontinuation because of the risk of severe muscle injury.[18:10]
- Persistent ALT/AST ULN: The statin should be held or the dose reduced, and liver enzymes re-evaluated in 2 to 4 weeks.[9:15][18:11]
- Intolerable Muscle Symptoms (Asymptomatic or CK ULN): Hold statin for a 2-to-4 week washout, followed by a low-dose rechallenge or transition to non-statin alternatives.[18:12]
¶ Drug and supplement interactions
Drug interactions with statins primarily involve pathways that alter systemic drug exposure, significantly increasing the risk of concentration-dependent myotoxicity.
¶ CYP3A4 Pathway Interactions
Atorvastatin, simvastatin, and lovastatin are major substrates of the Cytochrome P450 3A4 enzyme system.[11:7]
- Strong CYP3A4 Inhibitors: Co-administration of strong CYP3A4 inhibitors dramatically increases circulating statin concentrations, increasing the risk of SAMS and rhabdomyolysis.[11:8] Major interacting classes include:
- Macrolide Antibiotics: Clarithromycin, erythromycin.[11:9]
- Azole Antifungals: Itraconazole, ketoconazole.[11:10]
- Calcium Channel Blockers: Diltiazem, verapamil, amiodarone (dose limitations are required, particularly with Simvastatin).[11:11]
- Immunosuppressants: Cyclosporine.[11:12]
- Grapefruit Juice: Inhibits intestinal CYP3A4; high daily consumption ( quart) should be avoided in patients taking lipophilic statins.[11:13]
- Alternatives when CYP3A4 interactions matter: Clinicians may consider a statin that is less dependent on CYP3A4, such as rosuvastatin or pravastatin. The choice remains interaction-specific because these drugs can still be affected by transporters and other pathways.[11:14]
¶ Transporter-Mediated Interactions (SLCO1B1)
The OATP1B1 uptake transporter (encoded by SLCO1B1) is responsible for transporting hydrophilic statins, particularly rosuvastatin and pravastatin, into hepatocytes.[12:3][11:15]
- Genetic Polymorphisms: The SLCO1B1 c.521T>C genetic variant (specifically the *5 allele) reduces the functional activity of OATP1B1, resulting in decreased hepatic uptake and significantly higher circulating systemic concentrations of statins.[12:4] This genetic variation is strongly associated with an increased risk of myopathy.[12:5]
- Drug Interactions: Inhibitors of OATP1B1 (such as cyclosporine or gemfibrozil) block hepatic uptake, dramatically raising blood concentrations of almost all statins, and should generally be avoided.[11:16]
¶ FAQ
¶ 1. How long does it take for statins to work?
Statins achieve their near-maximal LDL-C lowering effect within 2 to 4 weeks of initiating therapy or adjusting the dose.[2:15] Consequently, follow-up lipid panels to assess efficacy are typically scheduled 4 to 12 weeks after starting the medication.[2:16]
¶ 2. Can statins be taken long term?
Yes, statin therapy is designed as a long-term preventive intervention.[2:17] Large cardiovascular outcome trials and long-term cohort studies spanning decades demonstrate that the cardiovascular benefits are sustained over long-term use, without evidence of cumulative toxicity or an increased risk of cancer or non-cardiovascular death.[3:7][13:2]
¶ 3. Can statins be taken alongside supplements like CoQ10?
Coenzyme Q10 (CoQ10) is frequently co-administered with statins because statins inhibit the synthesis of mevalonate, a precursor to both cholesterol and endogenous CoQ10.[10:12][18:13] Although statins lower circulating CoQ10, randomized trials have produced mixed and largely negative results for relieving statin-associated muscle symptoms; routine CoQ10 supplementation is therefore not supported by consistent evidence.[18:14]
¶ 4. Is a statin useful if an individual is otherwise healthy but has elevated LDL-C?
Yes. In primary prevention for individuals with no clinical cardiovascular disease but elevated LDL-C, the utility of a statin depends on their overall estimated absolute risk.[4:7] If LDL-C is severely elevated ( mg/dL), statin therapy is recommended regardless of 10-year risk calculators due to the high lifetime risk of cardiovascular events.[2:18] For milder elevations, decisions are guided by calculating the 10-year ASCVD risk and assessing the presence of other risk factors.[4:8]
¶ 5. Does starting a statin mean a patient must take it forever?
Statin therapy is typically a long-term commitment because discontinuing the medication results in LDL-C levels returning to their pre-treatment baseline within a few weeks, losing the cardiovascular protection.[2:19] However, a statin regimen can be modified, adjusted, or discontinued if a patient's absolute cardiovascular risk profile changes significantly, if they experience complete statin intolerance, or if their clinical goals shift towards palliative care.[18:15]
¶ How we evaluated the evidence
To compile this clinical guide, we prioritized high-certainty primary evidence and authoritative professional consensus guidelines:
- Study Types: Individual participant data (IPD) meta-analyses from the Cholesterol Treatment Trialists' (CTT) Collaboration, double-blind randomized placebo-controlled trials (e.g., SAMSON, StatinWISE, SHARP), and consensus guidelines from major cardiovascular societies (ACC/AHA, USPSTF, CCS, KDIGO, EAS) were strictly prioritized.
- Evidence Grading: We applied the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) framework:
- High Certainty: Multiple large-scale, low-bias RCTs or IPD meta-analyses with consistent, direct results. Applies to statin efficacy in cardiovascular risk reduction, LDL-C lowering, SAMS/nocebo characterization, and new-onset diabetes risk.
- Moderate Certainty: RCTs with minor design limitations or inconsistent results, or very high-quality cohort studies. Applies to certain sub-population primary prevention risk thresholds.
- Low Certainty: Observational studies, cohort analyses with potential confounding, or trials with serious limitations. Applies to specific genetic sub-analyses of transporter-mediated side effects.
- Very Low Certainty: Expert opinion, case reports, or in vitro mechanics without human clinical validation.
¶ References
US Food and Drug Administration. FDA requests removal of strongest warning against using cholesterol-lowering statins during pregnancy; still advises most pregnant patients should stop taking statins. 2021. https://www.fda.gov/drugs/drug-safety-and-availability/fda-requests-removal-strongest-warning-against-using-cholesterol-lowering-statins-during-pregnancy ↩︎ ↩︎ ↩︎ ↩︎
Blumenthal RS, Morris PB, Gaudino M, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2026;173(17):e1-e120. https://pubmed.ncbi.nlm.nih.gov/41824552/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cholesterol Treatment Trialists' (CTT) Collaborators, Mihaylova B, Emberson J, Baigent C, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380(9841):581-590. https://pubmed.ncbi.nlm.nih.gov/22607822/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
US Preventive Services Task Force, Mangione CM, Barry MJ, et al. Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2022;328(8):746-753. https://pubmed.ncbi.nlm.nih.gov/35997723/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cholesterol Treatment Trialists' Collaboration. Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials. Lancet. 2022;300(10355):832-845. https://pubmed.ncbi.nlm.nih.gov/36049498/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Howard JP, Wood FA, Finegold JA, et al. Side Effect Patterns in a Crossover Trial of Statin, Placebo, and No Treatment. Journal of the American College of Cardiology. 2021;78(12):1210-1222. https://pubmed.ncbi.nlm.nih.gov/34531021/ ↩︎ ↩︎ ↩︎
Herrett E, Williamson E, Brack K, et al. Statin treatment and muscle symptoms: series of randomised, placebo controlled n-of-1 trials. BMJ. 2021;372:n135. https://pubmed.ncbi.nlm.nih.gov/33627334/ ↩︎ ↩︎ ↩︎
Cholesterol Treatment Trialists’ Collaboration. Effects of statin therapy on diagnoses of new-onset diabetes and worsening glycaemia in large-scale randomised blinded statin trials: an individual participant data meta-analysis. The Lancet Diabetes & Endocrinology. 2024;12(5):306-319. https://pubmed.ncbi.nlm.nih.gov/38554713/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Newman CB, Preiss D, Tobert JA, et al. Statin Safety and Associated Adverse Events: A Scientific Statement From the American Heart Association. Arteriosclerosis, Thrombosis, and Vascular Biology. 2019;39(2):e38-e81. https://pubmed.ncbi.nlm.nih.gov/30580575/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Safitri N, Alaina MF, Pitaloka DAE, et al. A Narrative Review of Statin-Induced Rhabdomyolysis: Molecular Mechanism, Risk Factors, and Management. Drug, Healthcare and Patient Safety. 2021;13:211-221. https://pubmed.ncbi.nlm.nih.gov/34795533/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Wiggins BS, Saseen JJ, Page RL 2nd, et al. Recommendations for Management of Clinically Significant Drug-Drug Interactions With Statins and Select Agents Used in Patients With Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2016;134(21):e468-e495. https://pubmed.ncbi.nlm.nih.gov/27754879/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Choi SA, Kim JS, Park YA, et al. Transporter Genes and statin-induced Hepatotoxicity. Cardiovascular Drugs and Therapy. 2025;39(4):553-562. https://pubmed.ncbi.nlm.nih.gov/38809397/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cholesterol Treatment Trialists’ Collaboration, Baigent C, Blackwell L, Emberson J, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681. https://pubmed.ncbi.nlm.nih.gov/21067804/ ↩︎ ↩︎ ↩︎
Pearson GJ, Thanassoulis G, Anderson TJ, et al. 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults. The Canadian Journal of Cardiology. 2021;37(8):1129-1150. https://pubmed.ncbi.nlm.nih.gov/33781847/ ↩︎
Pastori D, Pani A, Di Rocco A, et al. Statin liver safety in non-alcoholic fatty liver disease: A systematic review and metanalysis. British Journal of Clinical Pharmacology. 2022;88(2):441-451. https://pubmed.ncbi.nlm.nih.gov/34133035/ ↩︎ ↩︎ ↩︎
McGuinness B, Craig D, Bullock R, et al. Statins for the prevention of dementia. The Cochrane Database of Systematic Reviews. 2016;1:CD003160. https://pubmed.ncbi.nlm.nih.gov/26727124/ ↩︎ ↩︎ ↩︎
Swiger KJ, Manalac RJ, Blumenthal RS, et al. Statins and cognition: a systematic review and meta-analysis of short- and long-term cognitive effects. Mayo Clinic Proceedings. 2013;88(11):1213-1221. https://pubmed.ncbi.nlm.nih.gov/24095248/ ↩︎ ↩︎ ↩︎
Stroes ES, Thompson PD, Corsini A, et al. Statin-associated muscle symptoms: impact on statin therapy-European Atherosclerosis Society Consensus Panel Statement on Assessment, Aetiology and Management. European Heart Journal. 2015;36(17):1012-1022. https://pubmed.ncbi.nlm.nih.gov/25694464/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Cholesterol Treatment Trialists' Collaboration. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet. 2019;393(10170):407-415. https://pubmed.ncbi.nlm.nih.gov/30712900/ ↩︎ ↩︎
Gencer B, Marston NA, Im K, et al. Efficacy and safety of lowering LDL cholesterol in older patients: a systematic review and meta-analysis of randomised controlled trials. Lancet. 2020;395(10263):1611-1620. https://pubmed.ncbi.nlm.nih.gov/33186535/ ↩︎ ↩︎
Wanner C, Tonelli M, Kidney Disease: Improving Global Outcomes Lipid Guideline Development Work Group Members. KDIGO Clinical Practice Guideline for Lipid Management in CKD: summary of recommendation statements and clinical approach to the patient. Kidney International. 2014;85(6):1303-1309. https://pubmed.ncbi.nlm.nih.gov/24552851/ ↩︎ ↩︎ ↩︎
Baigent C, Landray MJ, Reith C, et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet. 2011;377(9784):2181-2192. https://pubmed.ncbi.nlm.nih.gov/21663949/ ↩︎ ↩︎ ↩︎
Fujioka I, Goto M, Anzai T, et al. Pregnancy and neonatal outcomes following statin exposure in early pregnancy: a nationwide consultation-based cohort study in Japan. BMC Pregnancy and Childbirth. 2026;26(1):198. https://pubmed.ncbi.nlm.nih.gov/41832452/ ↩︎
Bytyçi I, Penson PE, Mikhailidis DP, et al. Prevalence of statin intolerance: a meta-analysis. European Heart Journal. 2022;43(34):3213-3223. https://pubmed.ncbi.nlm.nih.gov/35169843/ ↩︎ ↩︎