¶ Ulcerative Colitis
| Pathology Type | Superficial, Symmetrical, Continuous |
| Anatomical Range | Colon and Rectum Only (Starts Rectally) |
| Core Complications | Toxic Megacolon, Severe Hemorrhage, Dysplasia |
| Clinical Class | Autoimmune Mucosal Inflammatory |
| Oral Small Molecules | Upadacitinib, Ozanimod, Etrasimod |
| Surgical Option | Total Proctocolectomy with IPAA (J-Pouch) |
Ulcerative Colitis is a chronic, relapsing, immune-mediated inflammatory bowel disease restricted to the mucosal and submucosal layers of the colon and rectum. Characterized by continuous, symmetrical inflammation extending proximally from the anal verge, it leads to severe tenesmus, bloody diarrhea, and substantial risks of toxic megacolon and colorectal dysplasia[1][2][3]. Over the past decade, the therapeutic paradigm has transitioned from systemic corticosteroids to targeted mucosal-healing protocols utilizing high-potency oral small-molecule inhibitors (JAK inhibitors, S1P receptor modulators) and biologic agents alongside advanced reconstructive surgical options[4][1:1][2:1].
¶ At a glance
Key points (high-level summary)
- Continuous Mucosal Injury: Inflammation starts in the rectum (proctitis) and spreads continuously through the colon without "skip lesions," strictly sparing the small intestine[1:2][2:2].
- Mucosal Healing Target: Clinical management is driven by the Mayo Endoscopic Score, targeting complete mucosal restoration (score of 0 or 1) to prevent long-term neoplastic progression[2:3][5].
- Small-Molecule Revolution: Highly effective oral small molecules (Upadacitinib, Ozanimod, Etrasimod) offer rapid induction of remission, outperforming traditional biologics in speed of action[6][2:4].
- Surgical Cure Pathway: Complete removal of the colon (colectomy) offers a curative pathway, with reconstruction via an Ileal Pouch-Anal Anastomosis (IPAA) to preserve fecal continence[1:3].
What people use it for
- Aims: Induction and maintenance of steroid-free clinical and endoscopic remission, elimination of bloody diarrhea and urgency, prevention of colorectal cancer, and restorative surgical rehabilitation[1:4][2:5].
- Evidence quality: High-certainty evidence from numerous multi-center Phase 3 randomized controlled trials supports mesalamine, biologics, and novel small molecules[1:5][2:6].
¶ What is Ulcerative Colitis?
Ulcerative Colitis is a continuous inflammatory condition that specifically compromises the mucosal integrity of the large intestine.
¶ Pathology and Histopathology
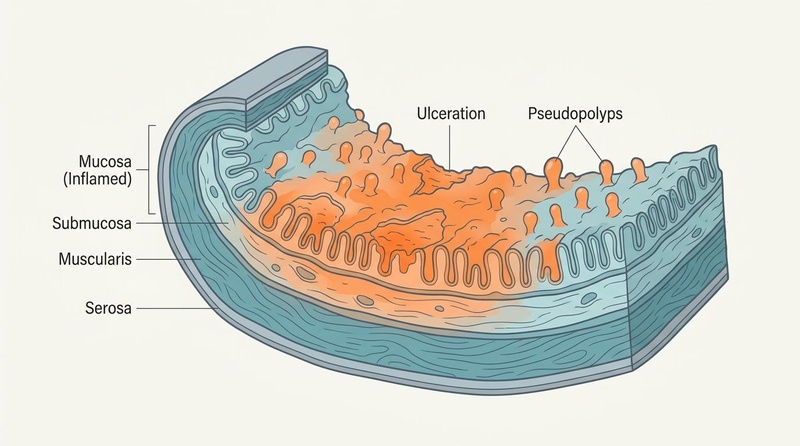
Macroscopically, the inflamed mucosa appears diffuse, erythematous, granular, and friable, bleeding easily upon contact. As shallow ulcerations coalesce, remaining islands of relatively normal or regenerating mucosa project above the surface, forming "pseudopolyps." Unlike Crohn's disease, the muscularis propria is spared except in cases of fulminant colitis or toxic megacolon. Histological hallmarks include mucosal architectural distortion, branched crypts, goblet cell depletion, and neutrophil infiltration of the crypt epithelium, resulting in cryptitis and crypt abscesses.
¶ Epidemiology and Age of Onset
Ulcerative colitis has a peak incidence between 15 and 30 years of age, with a secondary smaller peak occurring in males between 50 and 70. Pediatric-onset ulcerative colitis often manifests as an acute severe pan-colitis, carrying higher rates of primary steroid resistance and an accelerated progression to colectomy. In contrast, elderly-onset UC is typically more distal (proctitis or left-sided) but is associated with a greater baseline risk of cardiovascular comorbidities and severe drug-drug interactions with systemic therapies[7][8][6:1].
¶ Sex-Based Differences
Unlike Crohn's disease, adult ulcerative colitis is slightly more prevalent in males than in females, with a ratio of approximately 1.2:1. Men, particularly those diagnosed after the age of 50, are more likely to present with extensive pancolitis (E3) and carry a significantly higher lifetime risk of developing primary sclerosing cholangitis (PSC) and subsequent colorectal neoplasia[9]. Conversely, women with ulcerative colitis experience unique disease dynamics during pregnancy, where an active disease flare at the time of conception increases the risk of preterm birth, low birth weight, and spontaneous abortion, emphasizing the need for robust pre-conception endoscopic control[10].
¶ Clinical Classification and Staging
Clinical staging of ulcerative colitis incorporates both anatomical extent (E) and clinical severity, which dictate the aggressiveness of the therapeutic approach:
¶ Anatomical Extent (Montreal Classification)
- E1 (Ulcerative Proctitis): Confined strictly to the rectum (proximal extent distal to the rectosigmoid junction).
- E2 (Left-sided Colitis / Distal UC): Inflammation extends proximal to the rectosigmoid junction but is limited to the portion distal to the splenic flexure.
- E3 (Pancolitis / Extensive UC): Inflammation extends proximal to the splenic flexure, involving the entire colon.
¶ Endoscopic Staging (Mayo Endoscopic Subscore)
Endoscopic healing is the primary treatment target, graded from 0 to 3:
- Score 0 (Normal or Inactive Disease): Pale mucosa with normal, clear vascular patterns.
- Score 1 (Mild Disease): Erythema, decreased vascular pattern, and mild friability.
- Score 2 (Moderate Disease): Marked erythema, absent vascular pattern, friability, and erosions.
- Score 3 (Severe Disease): Spontaneous bleeding and prominent, deep ulceration.
¶ Diagnostic and Monitoring Framework
Robust monitoring protocols are required to track subclinical mucosal disease and prevent disease progression:
- Full Colonoscopy with Biopsies: The gold standard diagnostic procedure. Essential to confirm continuous rectal involvement, map colonic extent, and obtain histological biopsies to rule out Crohn's disease (lack of transmural lesions or granulomas) and cytomegalovirus (CMV) superinfection.
- Fecal Calprotectin (FC): Highly correlated with endoscopic and histological activity. Achieving a target of <100 µg/g represents complete mucosal healing, while levels >250 µg/g indicate active mucosal inflammation and dictate therapeutic optimization even in asymptomatic patients.
- C-Reactive Protein (CRP): Elevated CRP (>5 mg/L) indicates systemic inflammation but has lower sensitivity in UC compared to Crohn's; patients with isolated proctitis (E1) or moderate left-sided colitis (E2) often exhibit normal serum CRP despite active mucosal ulceration.
- Intestinal Ultrasound (IUS): Offers rapid, non-invasive assessment of colonic wall thickness. A bowel wall thickness >3.0 mm in the sigmoid or descending colon indicates moderate-to-severe disease activity[11].
¶ Evidence summary table (human outcomes)
| Target Outcome / Goal | Intervention | Effect Size | Consistency | Evidence Quality | Secondary Studies | Clinical Notes |
|---|---|---|---|---|---|---|
| Induction of Remission in Mild-to-Moderate UC | Mesalamine (5-ASA) Oral + Rectal Combined | High | High | Cochrane Systematic Reviews[1:6] | Combination oral + rectal therapy is superior to oral or rectal monotherapy alone. | |
| Rapid Induction in Moderate-to-Severe UC | Oral Upadacitinib (JAK Inhibitor) | High | High | Phase 3 RCTs[2:7] | Induces clinical response within 1–2 weeks, outperforming traditional anti-TNFs. | |
| Maintenance of Remission in Moderate-to-Severe UC | Vedolizumab (Anti-integrin) | High | High | Longitudinal Cohorts[11:1] | Highly gut-selective mechanism with an exceptionally favorable long-term safety profile. | |
| Mucosal & Histological Healing | Ozanimod / Etrasimod (S1P Modulators) | High | High | Phase 3 Trials[6:2][2:8] | Prevents lymphocyte egress from lymph nodes; highly effective for left-sided and pancolitis. | |
| Treatment of Refractory Pouchitis | VSL#3 / De Simone Formulation Probiotics | Moderate | Moderate | Systematic Reviews[12] | Prevents flare-ups of chronic pouchitis following surgical ileal pouch-anal anastomosis. | |
| Surgical Resolution of Refractory UC | Restorative Total Proctocolectomy (IPAA) | High | High | ECCO Guidelines[1:7] | Curative surgical procedure; removes all disease-bearing colonic mucosa while preserving continence. |
¶ Pathophysiological Mechanisms
The pathogenesis of Ulcerative Colitis is driven by an atypical Th2-like immune response combined with a profound collapse of the protective mucosal barrier:
[ Dysbiosis / Reduced Butyrate Producers ]
│
▼
[ Defective Mucosal Barrier ]
- Depleted goblet cells (Muc2)
- Downregulated tight junctions
│
▼
[ Luminal Antigen Leakage ]
│
▼
[ Dendritic Cell Activation ]
│
▼
[ Atypical Th2 Cell Induction ]
│
┌─────────────────────┴─────────────────────┐
▼ ▼
[ IL-5 Secretion ] [ IL-13 Secretion ]
│ │
▼ ▼
[ Neutrophil Recruitment ] [ Epithelial Cell Apoptosis ]
- Cryptitis - Tight junction breakdown
- Crypt Abscesses - Coalescing ulcers
│ │
└─────────────────────┬─────────────────────┘
▼
[ Continuous Colonic Damage ]
- Atypical Th2 Cytokine Cascade: In ulcerative colitis, mucosal CD4+ T cells secrete high levels of IL-5 and IL-13, mimicking an atypical Th2 response. IL-5 drives the recruitment and activation of eosinophils and neutrophils, leading to cryptitis. IL-13 binds directly to epithelial cells, inducing pore-forming claudin-2 expression, which downregulates tight junctions and triggers enterocyte apoptosis, causing epithelial desquamation and shallow ulcerations.
- Mucus Layer and Goblet Cell Exhaustion: The protective inner mucus layer (primarily composed of Muc2 glycoprotein synthesized by goblet cells) is profoundly depleted. This allows direct physical contact between commensal bacteria and the epithelial cell surface, activating Toll-like receptor signaling and perpetuating mucosal inflammation.
- Autoantibody Production: Approximately 60–80% of UC patients produce perinuclear anti-neutrophil cytoplasmic antibodies (pANCA). These autoantibodies target human histone H1 or related nuclear proteins, cross-reacting with commensal bacterial antigens and amplifying local neutrophil degranulation.
- S1P-Mediated Lymphocyte Infiltration: Sphingosine-1-phosphate (S1P) gradients drive the egress of activated T and B lymphocytes from secondary lymphoid organs into the systemic circulation. Once in the colonic vasculature, these cells bind to mucosal addressin cell adhesion molecule-1 (MAdCAM-1) via α4β7 integrin, resulting in massive, continuous inflammatory infiltration of the lamina propria.
¶ Therapeutic Protocols and Decision Paths
Treatment is systematically structured based on disease extent and clinical severity.
¶ Mild-to-Moderate Colitis Protocol
- Proctitis (E1): Initiate rectal Mesalamine (1 g suppository daily at bedtime). Rectal mesalamine delivers high local concentrations, achieving superior clinical and histological healing compared to oral 5-ASA.
- Left-sided or Pancolitis (E2/E3): Initiate combined oral Mesalamine (4.8 g/day) plus rectal Mesalamine (4 g/day enema) for 8 weeks. Combined therapy significantly shortens time to clinical remission compared to oral therapy alone[1:8].
- Refractory Mild UC: Add oral multi-matrix (MMX) Budesonide (9 mg/day for 8 weeks). Budesonide MMX utilizes a specialized delivery system that releases the corticosteroid continuously throughout the colon, achieving high local anti-inflammatory effects with minimal systemic bioavailability.
¶ Moderate-to-Severe Colitis Protocol
- First-Line Small Molecules: Initiate oral Upadacitinib (45 mg once daily induction for 8 weeks, followed by 15–30 mg once daily maintenance)[2:9]. Upadacitinib is a highly selective JAK1 inhibitor that blocks the signaling of multiple key cytokines (IL-2, IL-6, IL-15, IFN-gamma), providing rapid symptom control (cessation of bleeding within 72 hours).
- Alternative Biologic Pathways:
- Vedolizumab: Initiate at 300 mg IV at weeks 0, 2, and 6, then every 8 weeks. Target trough levels are >15 µg/mL. Ideal for patients seeking a gut-selective mechanism with minimal systemic infectious risk[11:2].
- Infliximab: 5–10 mg/kg IV infusion, combined with oral Azathioprine (2 mg/kg/day) to prevent anti-drug antibody formation[4:1].
¶ Surgical Restoration (Total Proctocolectomy with IPAA)
- Indications: Medically refractory moderate-to-severe UC, acute severe colitis failing rescue therapy (cyclosporine or infliximab), or detection of high-grade colonic dysplasia/adenocarcinoma.
- Procedure: A multi-stage total proctocolectomy is performed. The entire colon and rectal mucosa are resected, and a J-pouch is constructed from the terminal ileum and anastomosed to the anus (IPAA). This removes 100% of the disease-bearing mucosa, offering a clinical cure while preserving natural fecal continence[1:9].
¶ Safety, Toxicology, and Clinical Monitoring
Vigilant monitoring is mandatory to manage systemic risks associated with immunomodulation:
¶ Serious Adverse Events & Warnings
- Toxic Megacolon: A life-threatening complication characterized by rapid colonic dilation (>6 cm on abdominal plain radiograph) combined with systemic toxicity (fever, tachycardia, leukocytosis). Systemic corticosteroids and urgent surgical consultation are required; antimotility agents (loperamide) are strictly contraindicated during active colitis due to megacolon risk.
- JAK Inhibitor Safety (MACE & VTE): Upadacitinib carries black-box warnings for deep vein thrombosis (DVT), pulmonary embolism (PE), major adverse cardiovascular events (MACE), and herpes zoster reactivation. Avoid Upadacitinib in patients with active thromboembolic risk factors, previous myocardial infarction, or age >65[2:10].
- Pouchitis: Up to 50% of patients develop pouchitis (inflammation of the ileal pouch) within 5 years of IPAA surgery, presenting with increased stool frequency, urgency, and pelvic pressure. First-line therapy is oral Ciprofloxacin (500 mg twice daily) or Metronidazole (250 mg three times daily) for 14 days[1:10].
¶ Clinical Monitoring Pathway
┌────────────────────────────────────────────────────────┐
│ UPADACITIBIN / BIOLOGIC START │
│ - Screening: QuantiFERON Gold, VZV, HBV, Lipid Profile│
│ - Record baseline Fecal Calprotectin & CBC │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ WEEK 4 BIOCHEMICAL CHECK │
│ - Measure CBC (monitor for lymphopenia/anemia) │
│ - Evaluate LFTs & fasting lipid panel │
│ - Check hs-CRP (confirm systemic downward trend) │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ MONTH 3 SURVEILLANCE │
│ - Repeat Fecal Calprotectin (FC target <100 µg/g) │
│ - Evaluate clinical response (stool frequency <3/day) │
│ - Confirm complete resolution of rectal bleeding │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ MONTH 12 ENDOSCOPY │
│ - Perform surveillance Sigmoidoscopy │
│ - Confirm Mayo Endoscopic Score of 0 or 1 │
│ - Screen for dysplasia in long-standing pancolitis │
└────────────────────────────────────────────────────────┘
¶ Practical FAQ
What is the "backwash ileitis" in ulcerative colitis?
Backwash ileitis is a term used to describe superficial, mild inflammation of the terminal ileum that occurs in approximately 10–20% of patients with extensive pancolitis (E3). It is not a sign of Crohn's disease, but rather a benign consequence of an incompetent ileocecal valve allowing highly alkaline, inflammatory colonic contents to reflux back into the distal ileum.
How does the risk of colorectal cancer change over time in UC?
The risk of colorectal cancer in patients with extensive ulcerative colitis increases progressively with disease duration. The risk is estimated at approximately 2% after 10 years, 8% after 20 years, and up to 18% after 30 years of active pancolitis. This mandate highlights the necessity of initiating annual surveillance colonoscopies with chromoendoscopy and targeted biopsies after 8 years of disease duration.
Can probiotics be used to maintain remission in active UC?
Yes, but only in mild-to-moderate disease. High-potency, multi-strain probiotic formulations (such as the De Simone Formulation or VSL#3) have been shown in randomized controlled trials to be as effective as low-dose oral mesalamine for maintaining clinical remission in mild-to-moderate UC and are highly effective for preventing recurrent flare-ups of chronic pouchitis[12:1]. They are not effective for induction in moderate-to-severe disease.
Why is rectal therapy necessary if I am already taking oral mesalamine?
Oral mesalamine formulations release the active drug in the distal ileum or proximal colon. However, by the time the stool reaches the rectum, the concentration of active 5-ASA is often insufficient. Concomitant rectal mesalamine suppositories or enemas deliver extremely high local drug concentrations directly to the rectal mucosa, accelerating mucosal healing and clinical remission compared to oral mesalamine alone[1:11].
¶ Methods
This clinical monograph was prepared by conducting a comprehensive synthesis of clinical consensus statements (such as the ECCO Guidelines on Therapeutics in Ulcerative Colitis and AGA guidelines), multi-center Phase 3 clinical trial data, and longitudinal cohorts up to July 2026. Evidence quality was assessed using the GRADE framework.
¶ References
¶ Update Log
- 2026-07-07: Clinical monograph created, detailing mucosal-only Ulcerative Colitis pathology, Mayo Endoscopic Subscore staging, oral JAK1 inhibitors, and J-pouch surgical reconstruction.
Adamina M, Kienle P, Chaparro M. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Surgical Treatment. Journal of Crohn's & colitis. 2026. https://pubmed.ncbi.nlm.nih.gov/42381162/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zulfiqar O, Ali T, Mohayy Ud Din G. Oral Small-Molecule Therapies Versus Biologic Agents in Moderate-to-Severe Ulcerative Colitis: A Systematic Review of Pivotal Phase 3 Trials. Cureus. 2026. https://pubmed.ncbi.nlm.nih.gov/42344814/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Diao J, Cao H, Zhou J. Pathological reprogramming of innate immune cells drives resistance to biologics in inflammatory bowel diseases. Autoimmunity reviews. 2026. https://pubmed.ncbi.nlm.nih.gov/42190856/ ↩︎
Gordon M, Sinopoulou V, Akobeng AK. Biologic drugs for induction and maintenance of remission in Crohn's disease: a network meta-analysis. The Cochrane database of systematic reviews. 2026. https://pubmed.ncbi.nlm.nih.gov/42333672/ ↩︎ ↩︎
Denton KH, Slaughter JC, Bennett A. Patient Perspectives of Intestinal Ultrasound in IBD: A Quantitative Evaluation of Satisfaction and Diagnostic Preference. Digestive diseases and sciences. 2026. https://pubmed.ncbi.nlm.nih.gov/42348050/ ↩︎
Alsaeid M, Abu Hawi O, Bessissow T. IBD and Immune-Mediated Inflammatory Diseases: What Is the Optimal Management? Journal of clinical medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/42355576/ ↩︎ ↩︎ ↩︎
Williams J, Gurram B. Advanced therapies in management of pediatric inflammatory bowel disease. Current opinion in pediatrics. 2026. https://pubmed.ncbi.nlm.nih.gov/42361097/ ↩︎
Huo BL, Zhao AL, Liu W. Dual biologics or combination therapy with small molecules in pediatric inflammatory bowel disease: a systematic review and meta-analysis. World journal of pediatrics. 2026. https://pubmed.ncbi.nlm.nih.gov/42387245/ ↩︎
Clayton MW, Dierkhising RA, Gores GJ. Gallbladder neoplasia is associated with a higher incidence of cholangiocarcinoma in patients with primary sclerosing cholangitis. Canadian liver journal. 2026. https://pubmed.ncbi.nlm.nih.gov/42404986/ ↩︎
Gerbier E, Abolhassani N, Dupuis M. Use of medications to treat inflammatory bowel diseases before and during pregnancy in Switzerland between 2012 and 2019: an observational study using the claims-based MAMA cohort. BMC gastroenterology. 2026. https://pubmed.ncbi.nlm.nih.gov/42277663/ ↩︎
Jairath V, Armuzzi A, Agboton C. A decade of clinical data with vedolizumab: the past, present, and future. Therapeutic advances in gastroenterology. 2026. https://pubmed.ncbi.nlm.nih.gov/42205859/ ↩︎ ↩︎ ↩︎
Rosali MI, V Thanga Velu DP, Mokhtar MH. Specificity vs. Synergy Between Single-Strain and Multi-Strain Probiotics for Ulcerative Colitis Treatment: A Review of the Literature. Biomedicines. 2026. https://pubmed.ncbi.nlm.nih.gov/42351814/ ↩︎ ↩︎