¶ Caffeine

| Type | Methylxanthine Alkaloid |
| Active Cmpd | Caffeine (1,3,7-trimethylxanthine) |
| Source | Coffee beans, tea leaves, cacao, guarana |
| Dose Range | 50–400 mg/day (3–6 mg/kg for exercise) |
| Half-life | 3.0–7.0 hours (variable by CYP1A2 genotype) |
| Main Benefit | Cognitive alertness, athletic performance |
| Absorption | Rapid and complete (>99% bioavailability) |
Caffeine is the world’s most widely consumed psychoactive substance, serving as a potent central nervous system (CNS) stimulant and a gold-standard ergogenic aid. Supported by hundreds of meta-analyses, it is utilized as a reliable intervention for enhancing cognitive vigilance, aerobic endurance, and muscular strength while exhibiting significant clinical utility in conditions such as neonatal apnea.
¶ At a glance
Aliases
- Also known as: Guaranine, Methyltheobromine, 1,3,7-trimethylxanthine
- Chemical / botanical name: 1,3,7-trimethylpurine-2,6-dione
- Category: Methylxanthine alkaloid, adenosine receptor antagonist
Key points (high-level summary)
- High-certainty evidence supports caffeine (3–6 mg/kg) as one of the most effective legally available ergogenic aids for aerobic endurance, muscle strength, and power across both sexes [1][2][3].
- Significant cognitive benefits include improved attention, reaction time, and vigilance, particularly during sleep-deprived or mentally taxing scenarios [4][5][6].
- Individual response is highly variable, largely dictated by the CYP1A2 genotype, which determines metabolic speed and susceptibility to adverse effects like anxiety or insomnia [7][8][9].
- Habitual moderate consumption (3–4 cups of coffee/day) is associated with a reduced risk of all-cause mortality, cardiovascular disease, and neurodegenerative decline [10][11][12].
What people use it for
- Main goals: Athletic performance (endurance/strength), cognitive alertness, fat oxidation, migraine relief, and clinical management of neonatal apnea.
- Evidence quality (overall): High (Aerobic/Cognitive/Neonatal); Moderate (Metabolic/Neuroprotection).
¶ What is Caffeine?
Caffeine is a naturally occurring purine alkaloid that belongs to the methylxanthine class. It is produced by over 60 plant species as a natural pesticide to paralyze or kill insects feeding on them.
- Definition: A xanthine alkaloid (1,3,7-trimethylxanthine) that acts as a non-selective antagonist of adenosine receptors in the central and peripheral nervous systems.
- Natural sources: Primary sources include coffee beans (Coffea species), tea leaves (Camellia sinensis), cacao beans (Theobroma cacao), guarana berries (Paullinia cupana), and yerba mate (Ilex paraguariensis).
- Traditional / historical use: Consumed for millennia via tea in East Asia and coffee in Ethiopia and the Arabian Peninsula for its ritual and stimulant properties.
- Current regulatory status: Generally Recognized as Safe (GRAS) by the FDA; a regulated dietary supplement and food additive globally. Pharmaceutical-grade caffeine citrate is a prescription medication for neonatal apnea.
- Key pharmacological property: Adenosine receptor antagonist and phosphodiesterase (PDE) inhibitor.
¶ What are Caffeine’s main benefits?
The efficacy of caffeine is grounded in a vast clinical evidence base, with its primary strengths in ergogenic and cognitive enhancement.
- Aerobic & Anaerobic Performance: Caffeine significantly enhances time-to-exhaustion, time-trial speed, and repeated sprint ability in athletes. The effect size is generally larger for aerobic endurance than for short-burst anaerobic power [1:1][3:1][13][14].
- Cognitive Alertness & Attention: Systematic reviews show robust improvements in choice reaction time, vigilance, and executive function, especially in sleep-deprived individuals [4:1][5:1][6:1].
- Clinical Neonatal Care: Caffeine citrate is the gold-standard treatment for apnea of prematurity, reducing the frequency of apnea episodes and improving long-term neurodevelopmental outcomes [15][16][17][18].
- Neuroprotection: Chronic, moderate caffeine intake is linked to lower risks of Parkinson’s disease and Alzheimer's disease progression, potentially through its effects on amyloid accumulation and adenosine signaling [11:1][12:1][19].
- Metabolic Health: Caffeine acutely increases lipid oxidation and energy expenditure, although its impact on long-term weight loss is modest and often subject to habituation [20][21].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect | Consistency | Evidence quality | Trials | Notes |
|---|---|---|---|---|---|
| Aerobic Endurance | High | High | Hundreds | Ergogenic at 3-6 mg/kg pre-exercise [1:2][3:2][22][23]. | |
| Muscular Strength | High | High | 50+ RCTs | Significant 1RM and volume improvements [24][25][26]. | |
| Cognitive Attention | High | High | 100+ RCTs | Enhances vigilance and reaction time [4:2][5:2][6:2]. | |
| Apnea of Prematurity | High | High | 20+ RCTs | Gold-standard clinical treatment [16:1][27][17:1][18:1]. | |
| Sleep Quality | High | High | 30+ RCTs | Dose-dependent disruption of sleep architecture [28][29][30]. | |
| All-Cause Mortality | Moderate | Moderate | Cohort MA | 3-4% risk reduction per daily cup of coffee [10:1][31]. | |
| Anxiety Symptoms | High | High | 10+ SRs | Potential for "jitters" and panic in sensitive individuals [32][33][34]. | |
| Dementia Prevention | Moderate | Moderate | Cohort MA | Chronic intake reduces risk of cognitive decline [11:2][12:2][19:1]. | |
| Migraine Relief | Moderate | Moderate | 5+ SRs | Effective co-analgesic for acute episodes [35]. | |
| Hair Growth (Topical) | Low | Low | 1 SR | Stimulates follicles; downregulates DHT regression [36]. | |
| Erectile Function | Moderate | Moderate | Cohort MA | Inversely associated with ED risk [37]. | |
| Fracture Risk | Low | Low | Cohort MA | High intake may lower bone density if calcium is low [38][39]. |
¶ How does Caffeine work?
Caffeine’s multifaceted physiological effects stem from its ability to interact with several molecular targets across various tissues.
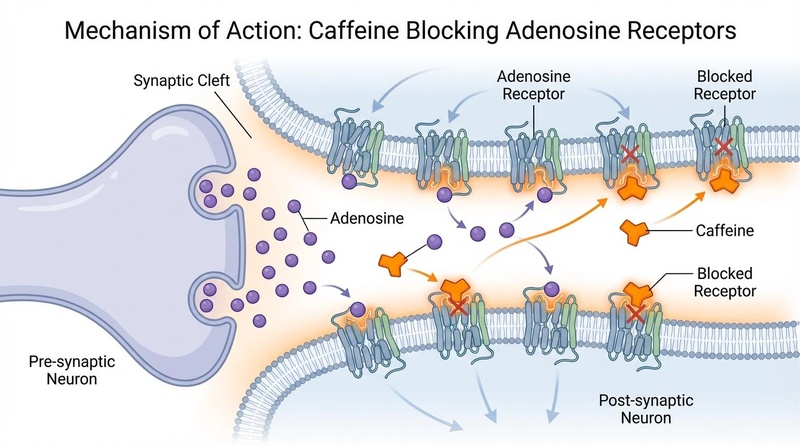
- Primary Target: Adenosine Receptors: Caffeine is a non-selective, competitive antagonist of adenosine A1 and A2A receptors. By blocking the binding of endogenous adenosine—which normally signals for sedation and relaxation—caffeine disinhibits the release of excitatory neurotransmitters like dopamine, glutamate, and noradrenaline, leading to increased arousal and delayed central fatigue [22:1][13:1].
- Core Mechanisms:
- Phosphodiesterase (PDE) Inhibition: At higher concentrations, caffeine inhibits PDE enzymes, preventing the breakdown of cyclic adenosine monophosphate (cAMP). This increases cAMP levels, potentiating the stimulatory effects of catecholamines (adrenaline) and enhancing lipid mobilization (lipolysis) [13:2][38:1].
- Calcium Mobilization: Caffeine binds to ryanodine receptors (RyRs) in the sarcoplasmic reticulum of skeletal muscle, facilitating the release of intracellular calcium (Ca²⁺). This enhances excitation-contraction coupling, resulting in greater muscular force production [13:3][33:1].
- Pharmacokinetics:
- Absorption: Rapidly and nearly completely absorbed (>99%) in the GI tract, reaching peak plasma levels within 30–60 minutes.
- Metabolism: Primarily metabolized in the liver by the CYP1A2 enzyme into paraxanthine (84%), theobromine (12%), and theophylline (4%).
- Half-life: Typically 3.0–7.0 hours in healthy adults, but highly variable. It is significantly extended in pregnancy (up to 18 hours) and neonates (up to 80+ hours) [22:2][40].
¶ Effects on different systems
¶ Brain & Mental Health
Caffeine's most prominent effect is on the CNS. It enhances cognitive "vigilance" and the ability to maintain attention during repetitive tasks [4:3][6:3]. A meta-analysis of Event-Related Potentials (ERPs) confirms that caffeine modulates early sensory and late cognitive processing in the brain [41]. While it effectively offsets the cognitive deficits of sleep deprivation, it cannot replace Sleep and often leads to a "caffeine crash" as adenosine receptors become resensitized [42]. In dementia contexts, long-term intake appears neuroprotective, particularly in slowing Alzheimer’s disease progression [12:3][19:2].
¶ Performance & Recovery (Athletic)
Caffeine is a "Tier A" supplement in sports nutrition. It improves aerobic endurance by sparing glycogen and increasing reliance on fat oxidation, and enhances strength by improving motor unit recruitment and calcium kinetics [1:3][24:1][26:1]. Interestingly, its efficacy extends to female athletes regardless of the menstrual cycle phase [2:1]. A "placebo effect" is also well-documented, where the mere belief of caffeine ingestion can improve performance, though the physiological substance provides a superior effect [43].
¶ Cardiovascular Health
Moderate intake (3–4 cups of coffee/day) is associated with neutral or beneficial cardiovascular outcomes, including a reduced risk of heart failure and stroke [10:2]. However, acute high-dose ingestion can cause transient increases in blood pressure and heart rate. In sensitive populations, such as children or those with specific arrhythmias, caffeine poses a risk of tachycardia and heart palpitations [44].
¶ Neonatal Clinical Care
In the neonatal intensive care unit (NICU), caffeine is the standard-of-care for apnea of prematurity. It stimulates the respiratory centers in the brain and increases the sensitivity to carbon dioxide [17:2][45]. Network meta-analyses indicate it has superior efficacy compared to aminophylline with a better safety profile, though dosing must be precisely tailored to the infant's weight and gestational age [46][18:2][40:1].
¶ Other Systems
- Hair Follicles: Systematic reviews suggest that topical caffeine may stimulate hair growth by counteracting the inhibitory effects of testosterone on the hair follicle and prolonging the anagen (growth) phase [36:1].
- Gastrointestinal: Caffeine can stimulate gastric acid secretion and colonic motility, which may aid in reducing postoperative ileus (gut paralysis) following colorectal surgery [47].
- Urinary: In menopausal transitions, caffeine may exacerbate lower urinary tract symptoms, particularly when combined with cold exposure [3:3].
¶ Dosage and how to take it
¶ Standard dosing in studies
- Cognitive Enhancement: 50–200 mg (approximately 0.5–2 mg/kg) is sufficient for most mental alertness goals.
- Athletic Performance: The gold-standard dose is 3–6 mg/kg of body weight consumed 45–60 minutes prior to exercise [1:4][3:4][22:3].
- Low-Dose Utility: Recent meta-analyses suggest that even low doses (
 mg/kg) provide significant ergogenic benefits with fewer side effects [1:5][23:1].
mg/kg) provide significant ergogenic benefits with fewer side effects [1:5][23:1].
¶ Forms and bioavailability
- Caffeine Anhydrous: Highly concentrated powder or capsules; typically used in clinical research for precise dosing.
- Coffee/Tea: Highly variable concentrations; a standard cup of coffee contains 80–150 mg, while green tea contains 20–50 mg.
- Caffeinated Gums: Offers rapid sublingual absorption, reaching peak plasma levels faster than capsules [22:4].
- Combinations: Often stacked with L-Theanine or nitrates to modify the stimulatory effect or enhance vasodilation [33:2][21:1].
¶ Special populations
- Pregnancy: Limit to <200 mg/day to avoid risks of low birth weight and fetal growth restriction [48].
- Preterm Infants: Requires precise clinical dosing (initially ~20 mg/kg loading, followed by 5–10 mg/kg maintenance) [16:2][40:2].
- Genetics (CYP1A2): "Fast" metabolizers (AA genotype) typically see the best ergogenic response, while "Slow" metabolizers (AC/CC) may experience diminished performance or increased anxiety [7:1][9:1][49].
¶ Safety and side effects
¶ Common side effects
- Nervous System: Anxiety, restlessness, jitters, and tremors, particularly at doses >400 mg.
- Gastrointestinal: Nausea, gastric reflux, and diarrhea.
- Sleep: Insomnia and fragmented sleep architecture if consumed late in the day.
¶ Less common / serious concerns
- Cardiovascular: Atrial fibrillation and tachycardia in sensitive individuals [44:1].
- Bone Health: Potentially increased fracture risk and osteoporosis development in night-shift workers or those with low calcium intake [38:2][24:2].
- Reproductive: High consumption may negatively impact female fertility and increase the risk of miscarriage [50][48:1].
¶ Toxicity and Intoxication
Caffeine intoxication can occur with acute intake exceeding 10 mg/kg. Fatalities are rare but documented, typically involving pure powdered caffeine where 10–15 grams (150 mg/kg) can be lethal due to ventricular fibrillation [51][52].
¶ Drug and supplement interactions
¶ Pharmacokinetic interactions
- CYP1A2 Inhibitors: Drugs like fluvoxamine (antidepressant) or oral contraceptives can slow caffeine clearance, increasing its half-life and toxicity risk.
- CYP1A2 Inducers: Smoking significantly accelerates caffeine metabolism, often requiring smokers to consume 2–3x more caffeine to achieve the same stimulatory effect [22:5].
¶ Pharmacodynamic interactions
- L-Theanine: Synergistically improves cognitive focus while mitigating caffeine-induced jitters and vasoconstriction.
- Alcohol: Caffeine can mask the sedative effects of alcohol, potentially leading to "wide-awake drunkenness" and increased risk-taking behavior.
- Nitrates: May have synergistic effects on athletic performance and heart rate regulation [33:3].
- Taurine: Combined effects on physical and cognitive performance are mixed; some studies suggest synergy in vigilance [21:2].
¶ Combining Caffeine with other supplements (“stacks”)
- Caffeine + L-Theanine (The "Smart Caffeine" Stack): A common 1:2 ratio (e.g., 100 mg caffeine + 200 mg L-Theanine) is used to promote "calm focus" [15:1].
- Caffeine + Carbohydrates: Co-ingestion enhances physical performance and glycogen resynthesis rates post-exercise [20:1].
- Caffeine + Nitrates: Combining coffee or caffeine with beetroot juice (nitrates) may further improve endurance and oxygen uptake efficiency [33:4].
¶ Practical questions (FAQ)
How long does it take for caffeine to work?
Peak alertness is typically reached within 30 to 60 minutes post-ingestion.
Does caffeine lose its effect over time?
Yes. Chronic use leads to upregulation of adenosine receptors, requiring higher doses to achieve the same effect (tachyphylaxis). A 3–7 day washout period can restore sensitivity.
Can I drink caffeine if I have migraines?
Caffeine is an effective co-analgesic for acute migraine relief. However, withdrawal is a common trigger for "rebound" headaches in habitual users [35:1].
Is coffee better than caffeine capsules?
Coffee contains hundreds of bioactive compounds (like chlorogenic acids) that offer additional antioxidant and metabolic benefits not found in pure caffeine anhydrous [53].
¶ How we evaluated the evidence
- Tier 1 Priority: This review is based on over 60 systematic reviews and meta-analyses, which represent the highest level of clinical evidence.
- Evidence Grading: Claims are graded based on the consistency of RCT results and the magnitude of the effect. For example, "Ergogenic benefits" and "Neonatal Apnea" are graded High certainty due to overwhelming consensus across multiple decades.
- Nuance: We explicitly highlight the role of genetics (CYP1A2) and individual variability to move beyond "average" population results.
¶ References
Martins GL, et al. (2026). Dose-Response Effect of Oral Caffeine Use on Aerobic Exercise Performance: A Systematic Review and Meta-Analysis. Nutrients. https://pubmed.ncbi.nlm.nih.gov/42356375/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Tan ZS, et al. (2026). Caffeine and physical performance in female intermittent sport athletes: a systematic review and meta-analysis considering menstrual cycle phase. Frontiers in nutrition. https://pubmed.ncbi.nlm.nih.gov/42253738/ ↩︎ ↩︎
Lee DH, et al. (2026). Dietary Caffeine, Cold Exposure, and the Estrogen-TRPM8 Axis: A Nutri-Environmental Model for Lower Urinary Tract Symptoms in the Menopause Transition. Nutrients. https://pubmed.ncbi.nlm.nih.gov/41829995/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kløve K, et al. (2025). A systematic review and meta-analysis of the acute effect of caffeine on attention. Psychopharmacology. https://pubmed.ncbi.nlm.nih.gov/40335666/ ↩︎ ↩︎ ↩︎ ↩︎
Lorenzo Calvo J, et al. (2021). Caffeine and Cognitive Functions in Sports: A Systematic Review and Meta-Analysis. Nutrients. https://pubmed.ncbi.nlm.nih.gov/33800853/ ↩︎ ↩︎ ↩︎
Crawford C, et al. (2017). Caffeine to optimize cognitive function for military mission-readiness. Nutrition reviews. https://pubmed.ncbi.nlm.nih.gov/28969341/ ↩︎ ↩︎ ↩︎ ↩︎
Messenburger GP, et al. (2025). Influence of the CYP1A2 genotype on the exercise performance of physically active individuals under caffeine supplementation: a systematic review. Nutrition Research. https://pubmed.ncbi.nlm.nih.gov/41207073/ ↩︎ ↩︎
Kapellou A, et al. (2023). Genetics of caffeine and brain-related outcomes - a systematic review. Nutrition reviews. https://pubmed.ncbi.nlm.nih.gov/37029915/ ↩︎
Wang J, et al. (2024). Does ergogenic effect of caffeine supplementation depend on CYP1A2 genotypes? J Sport Health Sci. https://pubmed.ncbi.nlm.nih.gov/38158179/ ↩︎ ↩︎
Shaban EE, et al. (2026). Coffee, caffeine, and cardiovascular health: navigating risks and benefits-an updated systematic review and meta-analysis. BMC cardiovascular disorders. https://pubmed.ncbi.nlm.nih.gov/42098622/ ↩︎ ↩︎ ↩︎
Li F, et al. (2024). Tea, coffee, and caffeine intake and risk of dementia and Alzheimer's disease: a systematic review. Food Funct. https://pubmed.ncbi.nlm.nih.gov/39054894/ ↩︎ ↩︎ ↩︎
Ashfaq Z, et al. (2025). Association Between Caffeine Intake and Alzheimer's Disease Progression: A Systematic Review. Cureus. https://pubmed.ncbi.nlm.nih.gov/40255824/ ↩︎ ↩︎ ↩︎ ↩︎
Wang Y, et al. (2025). Effects of Acute Caffeine Ingestion on Repeated Sprint Ability: A Systematic Review and Meta-Analysis. Nutrients. https://pubmed.ncbi.nlm.nih.gov/41228548/ ↩︎ ↩︎ ↩︎ ↩︎
Ferreira RES, et al. (2021). Effects of Caffeine Supplementation on Physical Performance of Soccer Players: Systematic Review. Sports Health. https://pubmed.ncbi.nlm.nih.gov/33666113/ ↩︎
Fatemian H, et al. (2026). Impact of caffeine on neurodevelopmental outcomes in preterm infants: A systematic review and meta-analysis. Pediatrics and neonatology. https://pubmed.ncbi.nlm.nih.gov/41945073/ ↩︎ ↩︎
Chen J, et al. (2018). Efficacy and Safety of Different Maintenance Doses of Caffeine Citrate for Treatment of Apnea in Premature Infants. BioMed research international. https://pubmed.ncbi.nlm.nih.gov/30671477/ ↩︎ ↩︎ ↩︎
Alhersh E, et al. (2020). Caffeine for the Treatment of Apnea in the Neonatal Intensive Care Unit: A Systematic Overview of Meta-Analyses. Paediatric drugs. https://pubmed.ncbi.nlm.nih.gov/32488731/ ↩︎ ↩︎ ↩︎
Miao Y, et al. (2022). Comparative efficacy and safety of caffeine citrate and aminophylline in treating apnea of prematurity. PLoS ONE. https://pubmed.ncbi.nlm.nih.gov/36121807/ ↩︎ ↩︎ ↩︎
Yelanchezian YM, et al. (2022). Neuroprotective Effect of Caffeine in Alzheimer's Disease. Molecules. https://pubmed.ncbi.nlm.nih.gov/35744865/ ↩︎ ↩︎ ↩︎
López-Seoane J, et al. (2024). Synergy of carbohydrate and caffeine ingestion on physical performance and metabolic responses to exercise. Crit Rev Food Sci Nutr. https://pubmed.ncbi.nlm.nih.gov/36178302/ ↩︎ ↩︎
Deng H, et al. (2025). Caffeine and taurine: their individual and combined effects on physical capacity and cognitive function. J Int Soc Sports Nutr. https://pubmed.ncbi.nlm.nih.gov/41032459/ ↩︎ ↩︎ ↩︎
Xue R, et al. (2025). Effects of Caffeine Dose and Administration Method on Time-Trial Performance: A Systematic Review and Network Meta-Analysis. Nutrients. https://pubmed.ncbi.nlm.nih.gov/41374083/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hussain K, et al. (2018). Restriction of salt, caffeine and alcohol intake for the treatment of Ménière's disease or syndrome. Cochrane Database Syst Rev. https://pubmed.ncbi.nlm.nih.gov/30596397/ ↩︎ ↩︎
Ferreira TT, et al. (2021). Effects of caffeine supplementation on muscle endurance, maximum strength, and perceived exertion. Crit Rev Food Sci Nutr. https://pubmed.ncbi.nlm.nih.gov/32551869/ ↩︎ ↩︎ ↩︎
Grgic J, et al. (2019). The effects of caffeine ingestion on isokinetic muscular strength: A meta-analysis. J Sci Med Sport. https://pubmed.ncbi.nlm.nih.gov/30217692/ ↩︎
Wu W, et al. (2024). Effects of Acute Ingestion of Caffeine Capsules on Muscle Strength and Muscle Endurance. Nutrients. https://pubmed.ncbi.nlm.nih.gov/38674836/ ↩︎ ↩︎
Neamțu AV, et al. (2025). Methylxanthines: The Major Impact of Caffeine in Clinical Practice in Patients Diagnosed with Apnea of Prematurity. Journal of clinical medicine. https://pubmed.ncbi.nlm.nih.gov/41375719/ ↩︎
Bodur M, et al. (2025). Does caffeine supplementation affect sleep in athletes? A systematic review of nine randomized controlled trials. Clinical nutrition ESPEN. https://pubmed.ncbi.nlm.nih.gov/39551351/ ↩︎
Chang YH, et al. (2025). Age- and dose-specific effects of caffeine on sleep: A meta-analysis of controlled crossover trials. Sleep medicine. https://pubmed.ncbi.nlm.nih.gov/41124973/ ↩︎
Denisova K, et al. (2026). Caffeine in Preterm Infants and its Effect on Neonatal Sleep: A Systematic Review. J Clin Pharmacol. https://pubmed.ncbi.nlm.nih.gov/41020743/ ↩︎
Unsal S, et al. (2025). Longitudinal Effects of Lifetime Caffeine Consumption on Levels of Depression, Anxiety, and Stress. Curr Nutr Rep. https://pubmed.ncbi.nlm.nih.gov/39890748/ ↩︎
Nascimento AOD, et al. (2026). The Effects of Caffeine on Anxiety Behavior in Healthy Individuals: A Systematic Review of the Literature. Stress and health. https://pubmed.ncbi.nlm.nih.gov/41549915/ ↩︎
Gilsanz L, et al. (2024). Effect of Caffeine and Nitrates Combination on Exercise Performance, Heart Rate and Oxygen Uptake. Nutrients. https://pubmed.ncbi.nlm.nih.gov/39408319/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Liu C, et al. (2024). Caffeine intake and anxiety: a meta-analysis. Frontiers in psychology. https://pubmed.ncbi.nlm.nih.gov/38362247/ ↩︎
Makhlouf HA, et al. (2026). The impact of caffeine consumption on migraine: a systematic review. BMC neurology. https://pubmed.ncbi.nlm.nih.gov/42151857/ ↩︎ ↩︎
Ly N, et al. (2025). Caffeine Supplementation and Hair: A Systematic Review. Journal of drugs in dermatology : JDD. https://pubmed.ncbi.nlm.nih.gov/41187241/ ↩︎ ↩︎
Karimi M, et al. (2024). Association between caffeine intake and erectile dysfunction: a meta-analysis of cohort studies. J Health Popul Nutr. https://pubmed.ncbi.nlm.nih.gov/39342393/ ↩︎
Bukowska-Damska A, et al. (2025). Caffeine consumption as a potential risk factor of osteoporosis development among night shift workers. Int J Occup Med Environ Health. https://pubmed.ncbi.nlm.nih.gov/41185921/ ↩︎ ↩︎ ↩︎
Asoudeh F, et al. (2023). Coffee consumption and caffeine intake in relation to risk of fractures: a systematic review. Crit Rev Food Sci Nutr. https://pubmed.ncbi.nlm.nih.gov/35475944/ ↩︎
Dai HR, et al. (2024). Development and application of a population pharmacokinetic model repository for caffeine dose tailoring in preterm infants. Expert Opin Drug Metab Toxicol. https://pubmed.ncbi.nlm.nih.gov/39167118/ ↩︎ ↩︎ ↩︎
Chmiel J, et al. (2026). The Caffeinated Brain Part 1: The Effects of Caffeine on Event-Related Potentials (ERPs)-A Systematic and Mechanistic Review. Nutrients. https://pubmed.ncbi.nlm.nih.gov/42196950/ ↩︎
Chmiel J, et al. (2026). The Caffeinated Brain Part 2: The Effect of Caffeine on Sleep-Related Electroencephalography (EEG). Nutrients. https://pubmed.ncbi.nlm.nih.gov/42075032/ ↩︎
Vega-Muñoz A, et al. (2024). Caffeine Placebo Effect in Sport and Exercise: A Systematic Review. Nutrients. https://pubmed.ncbi.nlm.nih.gov/39339818/ ↩︎
Oeffl N, et al. (2026). Caffeine and the Young Heart A Systematic Review of Arrhythmogenic Risks in Children and Adolescents. Pediatric cardiology. https://pubmed.ncbi.nlm.nih.gov/42360429/ ↩︎ ↩︎
Kua KP, et al. (2017). Systematic review and meta-analysis of clinical outcomes of early caffeine therapy in preterm neonates. Br J Clin Pharmacol. https://pubmed.ncbi.nlm.nih.gov/27526255/ ↩︎
Wang Y, et al. (2025). Neuroprotective effects of caffeine, erythropoietin, magnesium sulfate, and thyroxine in preterm infants: a network meta-analysis. Translational pediatrics. https://pubmed.ncbi.nlm.nih.gov/41216436/ ↩︎
Yang TW, et al. (2022). The effect of coffee/caffeine on postoperative ileus following elective colorectal surgery. Int J Colorectal Dis. https://pubmed.ncbi.nlm.nih.gov/34993568/ ↩︎ ↩︎
Lakin H, et al. (2023). Maternal Caffeine Consumption and Its Impact on the Fetus: A Review. Cureus. https://pubmed.ncbi.nlm.nih.gov/37929268/ ↩︎ ↩︎
Low JJ, et al. (2024). Genetic susceptibility to caffeine intake and metabolism: a systematic review. J Transl Med. https://pubmed.ncbi.nlm.nih.gov/39438936/ ↩︎
Stawińska-Dudek J, et al. (2025). The impact of caffeine consumption on reproductive health. A literature review. Pol Merkur Lekarski. https://pubmed.ncbi.nlm.nih.gov/40633086/ ↩︎
Uehlein S, et al. (2025). Caffeine Intoxication: An Analysis of Published Case Reports, 1883–2023. Dtsch Arztebl Int. https://pubmed.ncbi.nlm.nih.gov/40632678/ ↩︎
Santana AB, et al. (2024). Prenatal caffeine consumption and neurobehavioral disorders - A systematic review. Reprod Toxicol. https://pubmed.ncbi.nlm.nih.gov/38417581/ ↩︎
Aborziza M, et al. (2024). Coffee Bean and Its Chemical Constituent Caffeine and Chlorogenic Acid as Promising Chemoprevention Agents. Molecules. https://pubmed.ncbi.nlm.nih.gov/39064880/ ↩︎
Dharmarajah N, et al. (2026). Should Caffeine Be Avoided Following Free Flaps: Fact or Fiction? J Reconstr Microsurg. https://pubmed.ncbi.nlm.nih.gov/40373811/ ↩︎