¶ Chondroitin Sulfate
| Type | Sulfated Glycosaminoglycan (GAG) |
| Active Cmpd | Chondroitin-4-sulfate, Chondroitin-6-sulfate |
| Source | Bovine, porcine, or marine cartilage |
| Dose Range | 800–1,200 mg/day |
| Half-life | 3–15 hours (formulation dependent) |
| Main Benefit | Osteoarthritis (Symptom & Structure Modification) |
| Absorption | Low (15–24% bioavailability) |
Chondroitin sulfate (CS) is a major structural component of the extracellular matrix in articular cartilage, functioning as a Symptomatic Slow-Acting Drug for Osteoarthritis (SYSADOA) and a potential disease-modifying agent. Clinical evidence distinguishes pharmaceutical-grade formulations from generic nutraceuticals, with highly purified chondroitin showing significant efficacy in reducing joint pain and slowing cartilage degradation.
¶ At a glance
Aliases
- Also known as: Chondroitin 4-sulfate, Chondroitin 6-sulfate, CS, Galactosaminoglycuronoglycan sulfate.
- Category: Sulfated glycosaminoglycan (GAG).
Key points (high-level summary)
- Joint Protection: In patients with knee and hand osteoarthritis, pharmaceutical-grade chondroitin sulfate reduces pain and improves functional mobility similarly to NSAIDs but with a superior safety profile [1][2].
- Disease Modification: Long-term clinical trials demonstrate that 800 mg/day can significantly reduce the progression of joint space narrowing, indicating a structure-preserving effect on cartilage [3][4].
- Formulation Sensitivity: There is a profound efficacy gap between high-purity pharmaceutical preparations and low-purity food-grade supplements, which often fail to replicate clinical benefits [5].
- Anticoagulant Interaction: Chondroitin may enhance the effect of blood thinners like Warfarin, requiring monitoring of the International Normalized Ratio (INR) [6].
What people use it for
- Main goals: Osteoarthritis management, joint pain reduction, cartilage preservation, recovery from joint injury.
- Evidence quality (overall): Moderate to High (for knee/hand OA); Low (for hip/other joints).
¶ What is Chondroitin Sulfate?
Chondroitin sulfate is a complex polysaccharide and a member of the glycosaminoglycan (GAG) family. It consists of alternating chains of N-acetylgalactosamine and glucuronic acid, which are sulfated at specific positions.
- Definition: It is a naturally occurring sulfated GAG found in the connective tissues of all vertebrates, where it provides structural integrity and shock-absorbing properties to the extracellular matrix (ECM).
- Natural sources: Predominantly found in the cartilage of cows (bovine), pigs (porcine), and sharks/skates (marine).
- Traditional / historical use: Utilized since the mid-20th century in Europe as a prescription treatment for degenerative joint diseases.
- Current regulatory status: Classified as a pharmaceutical drug in most European countries (SYSADOA) and as a dietary supplement in the United States and other regions.
- Key pharmacological property: A high-molecular-weight polyelectrolyte that stimulates cartilage synthesis while inhibiting inflammatory and catabolic pathways.
¶ What are Chondroitin Sulfate’s main benefits?
Chondroitin sulfate’s therapeutic potential spans several major health domains, with human evidence increasingly supporting its roles in inflammation and metabolism.
¶ Symptom Relief in Osteoarthritis
The primary clinical benefit of chondroitin sulfate is the reduction of joint pain and the improvement of physical function in patients with knee and hand osteoarthritis. Large-scale trials, such as the CONCEPT trial, have demonstrated that 800 mg of pharmaceutical-grade CS is as effective as the NSAID Celecoxib (200 mg) for pain relief and functional improvement over six months, with significantly better gastrointestinal tolerability [1:1].
¶ Structural Joint Preservation
Unlike standard analgesics, chondroitin sulfate shows evidence of being a Disease-Modifying Osteoarthritis Drug (DMOAD). Data from the 2-year STOPP trial showed that patients taking 800 mg/day experienced significantly less joint space narrowing (cartilage loss) compared to placebo (0.10 mm vs. 0.24 mm loss), suggesting it can slow the underlying progression of the disease [3:1][4:1].
¶ Hand and Finger Osteoarthritis
Chondroitin is one of the few interventions conditionally recommended by the American College of Rheumatology (ACR) for hand osteoarthritis [2:1]. It has been shown to reduce finger joint pain and improve grip strength in patients where other treatments are often ineffective or poorly tolerated.
¶ Systemic Inflammation and Cancer Risk
Emerging epidemiological evidence and meta-analyses suggest that long-term use of chondroitin (often with glucosamine) is associated with reduced markers of systemic inflammation (such as C-reactive protein) and a lower risk of certain cancers, particularly colorectal cancer [7][8].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Knee OA Pain (Pharm-grade) | High | High | 10+ RCTs | [800–1200 mg/day; effective as NSAIDs over 6+ months][1:2][9] | |
| Joint Space Preservation | Moderate | Moderate | 4 RCTs | [800 mg/day for 2 years reduces narrowing by ~0.14 mm][3:2][4:2][10] | |
| Hand OA Pain & Function | Moderate | Moderate | 3 RCTs | [800 mg/day; recommended by ACR for hand OA][2:2][11] | |
| Hip OA Pain | Low | Very Low | 2 RCTs | [Inconsistent results; generally not recommended for hip][6:1][2:3] | |
| Knee OA Pain (Food-grade) | High | Moderate | 5+ RCTs | [Low-purity supplements often fail to beat placebo][12][5:1] | |
| Systemic CRP Levels | Moderate | Low | Meta-analysis | [Long-term use associated with lower systemic inflammation][7:1][13] | |
| Colorectal Cancer Risk | Moderate | Low | Systematic Review | [Epidemiological association with 20–50% risk reduction][8:1] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome.
- REQUIRED: Citations in the "Notes" column are linked to specific clinical guidelines, meta-analyses, and pivotal trials.
¶ How does Chondroitin Sulfate work?
Chondroitin sulfate exerts its effects through complex biochemical interactions within the joint environment, targeting multiple cellular pathways simultaneously.
¶ Core Mechanisms
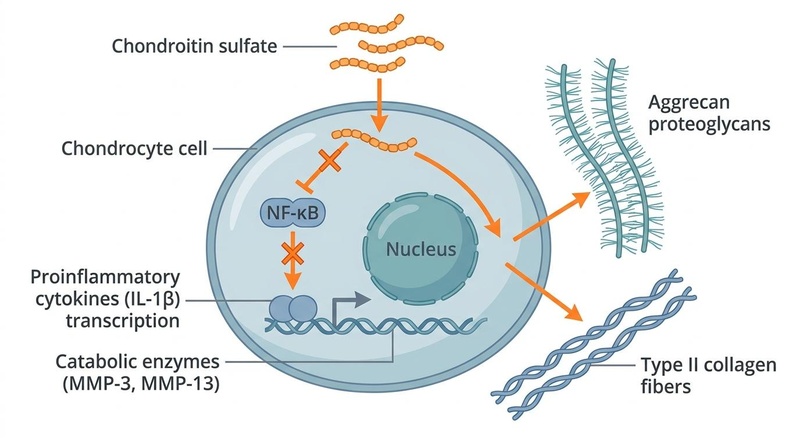
- NF-κB Inhibition & Anti-Inflammatory Action: Chondroitin inhibits the Nuclear Factor-kappa B (NF-κB) pathway, a master regulator of inflammation. This prevents the translocation of NF-κB into the nucleus of chondrocytes and synovial cells, thereby downregulating the expression of pro-inflammatory cytokines like IL-1β and TNF-α [14][15].
- Suppression of Catabolic Enzymes: It suppresses the synthesis and activity of matrix-degrading enzymes, including Matrix Metalloproteinases (MMP-3, MMP-13) and aggrecanases (ADAMTS-4, ADAMTS-5). This directly reduces the rate of cartilage matrix breakdown [14:1][16].
- Anabolic Matrix Stimulation: Chondroitin stimulates chondrocytes to increase the synthesis of Type II collagen and endogenous proteoglycans (aggrecan). This helps rebuild the extracellular matrix and restores cartilage elasticity [15:1][17].
- Subchondral Bone and Synovial Support: It modulates subchondral bone remodeling by reducing osteoblast-mediated bone resorption and increases the production of high-molecular-weight hyaluronic acid by synovial cells, improving joint lubrication [18][17:1].
¶ Pharmacokinetics
Chondroitin sulfate is a high-molecular-weight macromolecule, which presents challenges for oral absorption.
- Absorption: Bioavailability in humans ranges from 15% to 24%. Most of the orally administered CS is absorbed as smaller oligo- and polysaccharides or as the constituent disaccharides after being broken down by colonic microflora [19].
- Source Differences: Bovine and porcine CS (14–26 kDa) typically have lower molecular weights and better absorption profiles than marine CS (50–70 kDa), which reaches peak blood levels much slower (8.7 hours vs. 2–5 hours) [19:1][5:2].
- Half-life: The elimination half-life ranges from 3 to 15 hours depending on the specific formulation and purity level [19:2].
¶ Effects on different systems
¶ Joint, Bone & Connective Tissue
Chondroitin's primary domain is the musculoskeletal system. It is recognized as a SYSADOA for its ability to provide long-term analgesic effects that persist even after treatment cessation (the "carry-over" effect).
- Knee Osteoarthritis: Meta-analyses show a small but clinically significant effect on pain (SMD ~0.2) when pharmaceutical-grade CS is used. It is strongly recommended by ESCEO as a first-line background therapy for knee OA [9:1][20].
- Bone Health: In older populations, pharmacological-grade CS has been observed to have antiresorptive effects, potentially supporting bone density alongside cartilage preservation [18:1].
¶ Digestive & Metabolic Health
While not its primary indication, chondroitin sulfate interacts significantly with the gut microbiome and systemic metabolic markers.
- Microbiome Interaction: Chondroitin is metabolized by colonic bacteria (e.g., Bacteroides thetaiotaomicron), which can influence the gut-joint axis and systemic inflammatory tone [19:3].
- Cancer Prevention: Large systematic reviews have found that regular use of chondroitin/glucosamine is associated with a significantly reduced risk of colorectal cancer, possibly due to the reduction of chronic intestinal inflammation [8:2].
¶ Cardiovascular and Neurological Health
Preliminary research suggests potential benefits beyond joint health, though human evidence is less robust.
- Vascular Integrity: Genetic studies link polymorphisms in chondroitin-related proteoglycan genes (CSPG2) to susceptibility for intracranial aneurysms, suggesting a role in maintaining vascular wall integrity [21].
- Brain Health: Chondroitin sulfate proteoglycans (CSPGs) are critical in the brain's extracellular matrix. Research into receptors like CSPG4 is exploring their role in glioblastoma cell invasion and potential targeted therapies [22].
¶ Dosage and how to take it
Standard dosing in studies
- Typical Daily Dose: 800 mg to 1,200 mg.
- Common Schedules: Can be taken as a single 800 mg dose or divided into 400 mg or 600 mg doses twice daily. Both methods show similar efficacy in trials [9:2][13:1].
- Duration: Benefits for pain usually appear within 2 to 4 weeks. Structural benefits (cartilage preservation) require continuous use for at least 2 years [3:3][4:3].
Forms and bioavailability
- Pharmaceutical Grade: Look for highly purified formulations (>95% purity) standardized for molecular weight. Trials showing efficacy (e.g., CONCEPT, STOPP) exclusively used pharmaceutical-grade CS [1:3][5:3].
- Nutraceutical/Food Grade: Often contains significantly less active ingredient than labeled and higher levels of impurities. These are generally less effective in clinical trials [5:4].
- Salt Forms: Most commonly available as Chondroitin Sulfate Sodium.
Special populations
- Renal Impairment: Limited data; caution is advised in severe renal disease due to sodium content in some formulations.
- Pregnancy/Breastfeeding: Generally avoided due to lack of safety data in these populations.
¶ Safety and side effects
Safety Traffic Light: GREEN
Chondroitin sulfate has an exceptionally high safety profile, comparable to placebo in large-scale clinical trials and major safety reviews [6:2][1:4].
Common side effects
- Mild gastrointestinal symptoms: nausea, bloating, diarrhea, or constipation (frequency <5%).
- Occasional reports of epigastric pain or heartburn.
Less common / serious concerns
- Bleeding Risk: Rare reports of increased bleeding tendency, specifically when used in combination with anticoagulants.
- Hypersensitivity: Allergic reactions (rash, itching) are rare but possible, particularly in those with sensitivities to the source material.
Who should be especially cautious or avoid it
- Shellfish Allergy: Individuals with severe shellfish allergies should choose bovine or porcine sources rather than marine-derived CS.
- Anticoagulant Users: Requires monitoring of clotting factors (INR) due to potential potentiation of drug effects.
¶ Drug and supplement interactions
Pharmacokinetic interactions
- CYP450 Enzymes: Chondroitin does not appear to significantly induce or inhibit major cytochrome P450 enzymes (e.g., CYP3A4), suggesting a low risk of metabolic drug-drug interactions.
Pharmacodynamic interactions
- Warfarin & Anticoagulants: The most clinically relevant interaction. Chondroitin (especially when paired with glucosamine) can increase the International Normalized Ratio (INR), heightening the risk of bleeding in patients on Warfarin or Coumadin [6:3].
- NSAIDs (Synergy): Chondroitin has an additive effect when combined with NSAIDs like Ibuprofen or Celecoxib, often allowing for a lower dose of the NSAID to achieve the same pain relief, thereby reducing NSAID-related gastrointestinal risks [9:3].
¶ Combining Chondroitin Sulfate with other compounds (“stacks”)
- Glucosamine Sulfate: The most common combination. Mechanistically synergistic; while glucosamine provides the building blocks for GAG synthesis, chondroitin inhibits the enzymes that break them down. Use Glucosamine Sulfate rather than Hydrochloride for better results [23][24].
- MSM (Methylsulfonylmethane): Often added for its sulfur-donating properties, which support the sulfation of chondroitin chains and provide additional anti-inflammatory support.
- Hyaluronic Acid: Combined to support synovial fluid viscosity and joint lubrication, potentially enhancing the "cushioning" effect in the joint [9:4].
- Type II Collagen: Used to provide the structural scaffolding of the cartilage matrix, complementing the proteoglycan-stimulating effects of chondroitin.
¶ Practical questions (FAQ)
How long does it take for chondroitin to work?
Analgesic effects typically take 2 to 4 weeks to become noticeable. Unlike NSAIDs, it is a "slow-acting" drug, but its benefits often persist for several weeks after stopping the supplement.
Is pharmaceutical-grade chondroitin better than store-bought?
Yes. Clinical research shows that many over-the-counter supplements contain only a fraction of the labeled dose and have lower purity, which explains why some trials show no benefit [5:5].
Can I take chondroitin if I have diabetes?
Yes. Early concerns about glucosamine/chondroitin affecting insulin resistance have been largely debunked by human clinical trials showing no significant impact on blood glucose or HbA1c [6:4].
Does chondroitin actually regrow cartilage?
Should I take it with or without food?
Absorption is not significantly impacted by food, but taking it with a meal can help minimize the risk of mild stomach upset.
¶ How we evaluated the evidence
Evidence was graded using the GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) framework, prioritizing systematic reviews and double-blind, randomized controlled trials.
- Priority Sources: Cochrane Systematic Reviews, the CONCEPT and STOPP trials, and guidelines from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the American College of Rheumatology (ACR).
- Certainty Levels: Claims regarding knee OA pain and structural preservation are supported by moderate-to-high certainty evidence. Claims regarding hip OA and cancer prevention are graded as low certainty due to less robust trial data.
¶ References
Reginster JY, et al. Pharmaceutical-grade Chondroitin sulfate is as effective as celecoxib and superior to placebo in symptomatic knee osteoarthritis: the CONCEPT Trial. Ann Rheum Dis. 2017. https://pmc.ncbi.nlm.nih.gov/articles/PMC5561371/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Kolasinski SL, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020. https://pubmed.ncbi.nlm.nih.gov/31908149/ ↩︎ ↩︎ ↩︎ ↩︎
Kahan A, et al. Long-term effects of chondroitins 4 and 6 sulfate on knee osteoarthritis: the STOPP Trial. Arthritis Rheum. 2009. https://pubmed.ncbi.nlm.nih.gov/19180484/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hochberg MC. Structure-modifying effects of chondroitin sulfate in knee osteoarthritis: an updated meta-analysis of randomized placebo-controlled trials. Osteoarthritis Cartilage. 2010. https://pubmed.ncbi.nlm.nih.gov/20399895/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Restaino OF, et al. Pharmaceutical Grade vs. Food Grade Chondroitin Sulfate: The Structural and Biological Differences. Pharmaceutics. 2021. https://pubmed.ncbi.nlm.nih.gov/34065415/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Singh JA, et al. Chondroitin for osteoarthritis. Cochrane Database Syst Rev. 2015. https://pubmed.ncbi.nlm.nih.gov/25629485/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Liu B, et al. Role of Glucosamine and Chondroitin in the Prevention of Cancer: A Meta-Analysis. Nutr Cancer. 2023. https://pubmed.ncbi.nlm.nih.gov/36715012/ ↩︎ ↩︎
Khan AA, et al. The Role of Glucosamine and Chondroitin Sulfate in the Prevention of Colorectal Cancer: A Systematic Review. Cureus. 2022. https://pubmed.ncbi.nlm.nih.gov/35774674/ ↩︎ ↩︎ ↩︎
Bruyere O, et al. Algorithm for the management of knee osteoarthritis: An updated recommendation from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Ann Rheum Dis. 2019. https://pubmed.ncbi.nlm.nih.gov/31036637/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Knapik JJ, et al. Effects of Oral Chondroitin Sulfate on Osteoarthritis-Related Pain and Joint Structural Changes: Systematic Review and Meta-Analysis. J Special Oper Med. 2019. https://pubmed.ncbi.nlm.nih.gov/30859538/ ↩︎
Black C, et al. The clinical effectiveness of glucosamine and chondroitin supplements in slowing or arresting progression of osteoarthritis of the knee: a systematic review and economic evaluation. Health Technol Assess. 2009. https://pubmed.ncbi.nlm.nih.gov/19903416/ ↩︎
Clegg DO, et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis (GAIT Trial). N Engl J Med. 2006. https://pubmed.ncbi.nlm.nih.gov/16495392/ ↩︎
Rabade A, et al. Evaluation of efficacy and safety of glucosamine sulfate, chondroitin sulfate, and their combination regimen in the management of knee osteoarthritis: a systematic review and meta-analysis. Inflammopharmacology. 2024. https://pubmed.ncbi.nlm.nih.gov/38581640/ ↩︎ ↩︎
Martel-Pelletier J, et al. Effects of chondroitin sulfate in the pathophysiology of the osteoarthritic joint: a narrative review. Osteoarthritis Cartilage. 2010. https://pubmed.ncbi.nlm.nih.gov/20399897/ ↩︎ ↩︎
Bali JP, et al. Biochemical basis of the pharmacologic action of chondroitin sulfates on the osteoarticular system. Seminars Arthritis Rheum. 2001. https://pubmed.ncbi.nlm.nih.gov/11503140/ ↩︎ ↩︎
Fernandez-Martin S, et al. Glucosamine and Chondroitin Sulfate: Is There Any Scientific Evidence for Their Effectiveness as Disease-Modifying Drugs in Knee Osteoarthritis Preclinical Studies? Animals (MDPI). 2021. https://pubmed.ncbi.nlm.nih.gov/34072407/ ↩︎
Zhu X, et al. Effectiveness and safety of glucosamine and chondroitin for the treatment of osteoarthritis: a meta-analysis of randomized controlled trials. J Orthop Surg Res. 2018. https://pubmed.ncbi.nlm.nih.gov/29980200/ ↩︎ ↩︎
Shavlovskaya OA, et al. Antiresorptive activity of pharmacological chondroitin sulfate in the older age group. Ter Arkh. 2020. https://pubmed.ncbi.nlm.nih.gov/33720577/ ↩︎ ↩︎
Volpi N, et al. Oral absorption and bioavailability of ichthyic origin chondroitin sulfate in healthy male volunteers. Osteoarthritis Cartilage. 2003. https://pubmed.ncbi.nlm.nih.gov/12801483/ ↩︎ ↩︎ ↩︎ ↩︎
Baden KER, et al. The Safety and Efficacy of Glucosamine and/or Chondroitin in Humans: A Systematic Review. Nutrients. 2025. https://pubmed.ncbi.nlm.nih.gov/40647198/ ↩︎
Liu H, et al. The Association between Genes Polymorphisms of Heparan Sulfate Proteoglycan 2 (HSPG2) and Chondroitin Sulfate Proteoglycan 2 (CSPG2) and Intracranial Aneurysm Susceptibility: A Meta-Analysis. Iran J Public Health. 2019. https://pubmed.ncbi.nlm.nih.gov/31970092/ ↩︎
Hadri SH, et al. Exploring the potential of multiple receptors overexpressed on glioblastoma cells as biomarkers for the targeted therapy; a review. Therapeutic Delivery. 2026. https://pubmed.ncbi.nlm.nih.gov/42273826/ ↩︎
Wang Z, et al. Clinical Efficacy and Safety of Chondroitin Combined with Glucosamine in the Treatment of Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Comput Math Methods Med. 2022. https://pubmed.ncbi.nlm.nih.gov/35924114/ ↩︎
Meng Z, et al. Efficacy and safety of the combination of glucosamine and chondroitin for knee osteoarthritis: a systematic review and meta-analysis. Arch Orthop Trauma Surg. 2023. https://pubmed.ncbi.nlm.nih.gov/35024906/ ↩︎