¶ Glucosamine
| Type | Amino sugar |
| Active Cmpd | Glucosamine (Sulfate/HCl) |
| Source | Shellfish shells, fungi |
| Dose Range | 1,500 mg/day |
| Half-life | ~15 hours |
| Main Benefit | Joint health & Osteoarthritis |
| Absorption | High (90% absorbed) |
Glucosamine is a naturally occurring amino sugar and a fundamental building block of joint cartilage. It is widely supplemented to reduce joint pain, delay osteoarthritis progression, and potentially support long-term metabolic and systemic health.
¶ At a glance
Aliases
- Also known as: 2-amino-2-deoxy-D-glucose, chitosamine, glucosamine sulfate, glucosamine hydrochloride
- Chemical / botanical name: (3R,4R,5S,6R)-3-amino-6-(hydroxymethyl)oxane-2,4,5-triol
- Category: Amino sugar derivative
Key points (high-level summary)
- Glucosamine sulfate (specifically prescription crystalline glucosamine sulfate) significantly reduces pain and improves physical function in adults with knee osteoarthritis [1][2][3].
- Glucosamine hydrochloride is widely considered ineffective, failing to outperform placebo in multiple large-scale meta-analyses [3:1][4].
- Emerging meta-analytic evidence suggests habitual glucosamine use is associated with a decreased risk of colorectal and lung cancers [5][6].
- A critical safety concern is a severe interaction with Warfarin, which can dangerously elevate INR and increase bleeding risks [1:1].
What people use it for
- Main goals: Osteoarthritis symptom relief, joint cartilage preservation, reduction of systemic inflammation, and potential cancer prevention.
- Evidence quality (overall): Moderate to High (for knee osteoarthritis using the crystalline sulfate form); Low (for structure-modifying and cancer preventive effects).
¶ What is glucosamine?
Glucosamine is an endogenous amino sugar synthesized from glucose and glutamine, representing a key precursor in the biochemical synthesis of glycosylated proteins and lipids.
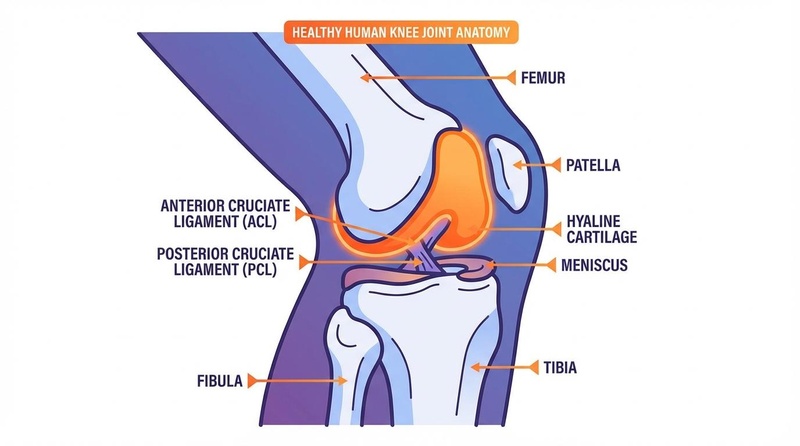
- Definition: It is a prominent component of cartilage matrix glycoproteins and synovial fluid, acting as a structural substrate for glycosaminoglycans (GAGs) such as hyaluronic acid and keratan sulfate.
- Natural sources: While endogenous to human joint tissue, exogenous dietary sources are virtually non-existent in typical foods. Commercial supplements are manufactured via chemical hydrolysis of chitin from shellfish exoskeletons (shrimp, crab, lobster) or via fungal fermentation (Aspergillus niger) for vegan formulations.
- Traditional / historical use: First isolated in 1876, glucosamine gained clinical prominence in the late 20th century as a "symptomatic slow-acting drug in osteoarthritis" (SYSADOA).
- Current regulatory status: Regulated as a prescription drug in Europe and highly regulated clinical contexts, but widely available as an over-the-counter dietary supplement in the United States and other regions.
- Key pharmacological property: Chondroprotective and anti-inflammatory amino sugar.
¶ What are glucosamine’s main benefits?
¶ Osteoarthritis and Joint Pain
In knee and hip osteoarthritis, glucosamine sulfate works by supplying the rate-limiting substrates for cartilage matrix synthesis and down-regulating local inflammatory pathways [1:2][2:1][7]. Multiple high-quality systematic reviews demonstrate that crystalline glucosamine sulfate significantly reduces joint pain (standardized mean difference [SMD] values around -1.11 in positive trials) and improves functional mobility, matching the long-term efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) like celecoxib while avoiding their cardiovascular and gastrointestinal adverse profiles [8][9]. However, glucosamine hydrochloride (HCl) consistently fails to provide clinically meaningful symptom relief [3:2][4:1].
¶ Temporomandibular Joint (TMJ) Osteoarthritis
Oral glucosamine has emerged as an effective therapy for TMJ osteoarthritis [10][11]. Systematic and umbrella reviews of clinical trials show that oral glucosamine (typically 1,200–1,500 mg/day) significantly reduces TMJ pain, decreases joint sounds, and improves physical jaw function, specifically increasing maximum mouth opening [10:1][11:1]. It exhibits comparable efficacy to standard NSAIDs for TMJ symptoms, with a superior safety profile [10:2].
¶ Colorectal and Lung Cancer Prevention
Large-scale prospective epidemiological trials and systematic meta-analyses have highlighted a protective association between habitual glucosamine use and cancer risk [5:1][6:1]. A comprehensive meta-analysis of thirteen clinical and cohort studies found that glucosamine and/or chondroitin intake was associated with a 9% reduction in the risk of colorectal cancer (OR 0.91, 95% CI 0.87–0.94) and a 16% reduction in the risk of lung cancer (OR 0.84, 95% CI 0.79–0.89) [5:2]. These protective associations are hypothesized to stem from systemic anti-inflammatory actions and inhibition of oncogenic signaling pathways [6:2].
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| Knee OA: Pain (Sulfate Form) | High | High | >100 RCTs | 1,500 mg/day of crystalline glucosamine sulfate reduces pain and stiffness [1:3][2:2][12] | |
| Knee OA: Pain (HCl Form) | High | Moderate | Multiple RCTs | Glucosamine hydrochloride fails to show clinical benefit over placebo [3:3][4:2][13] | |
| TMJ OA: Pain & Function | Moderate | Moderate | 8 RCTs | 1,200–1,500 mg/day significantly decreases jaw pain and increases maximum mouth opening [10:3][11:2] | |
| Colorectal Cancer Risk | Moderate | Low | Cohort studies | Habitual use associated with reduced colorectal cancer risk (OR 0.91) [5:3][6:3] | |
| Lung Cancer Risk | Moderate | Low | Cohort studies | Associated with reduced lung cancer risk (OR 0.84) in meta-analysis [5:4] | |
| Joint Space Narrowing | Low | Low | Meta-analysis | Long-term use of pharmaceutical-grade sulfate may delay joint space narrowing [14][15][7:1] | |
| Combination with Exercise | Moderate | Moderate | 6 RCTs | Adding glucosamine to exercise programs does not yield additional pain or functional benefits [16] |
- *Effect: Number of arrows (1-3) indicates magnitude. Direction: ↑ (increase), ↓ (decrease), = (no effect), ? (unclear). Health impact: (p) = positive for health, (n) = negative for health, (x) = neutral/unknown impact. Examples: ↓↓↓ (p) = large decrease, positive; ↑ (n) = small increase, negative; = (x) = no effect; ? = unclear.
- **Consistency: Low (results conflict), Moderate (mixed but leaning one way), High (most trials agree)
- ***Trials: Number of RCTs or total trials informing this outcome (shows evidence depth at a glance)
¶ How does glucosamine work?
¶ Chondroprotection and Structural Substrate
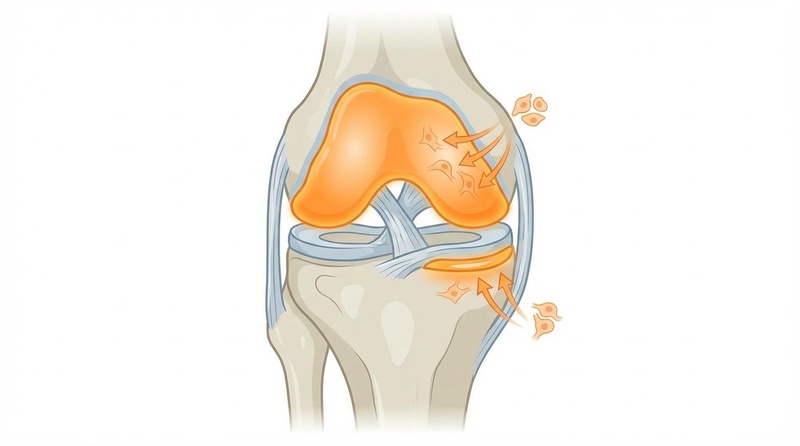
Glucosamine is a fundamental rate-limiting precursor in the biosynthesis of glycosaminoglycans (GAGs) and proteoglycans, which form the structural backbone of articular cartilage and synovial fluid [13:1]. Exogenous glucosamine is rapidly taken up by chondrocytes via glucose transporters (GLUT1, GLUT2, GLUT4) and phosphorylated into glucosamine-6-phosphate, stimulating the synthesis of aggrecan and collagen type II [17][13:2]. Preclinical systematic reviews confirm that chronic administration down-regulates matrix metalloproteinases (MMPs) and aggrecanases, arresting cartilage matrix degradation [17:1].
¶ Anti-Inflammatory Pathways (NF-κB Inhibition)
At the cellular level, glucosamine exerts profound anti-inflammatory properties by inhibiting the Nuclear Factor-kappa B (NF-κB) signaling pathway [6:4][13:3]. It prevents the intracellular cascade of Interleukin-1 beta (IL-1β), suppressing the transcription of pro-inflammatory cytokines (such as IL-6, IL-8, and TNF-α) as well as cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS) [6:5]. This molecular action is highly synergistic with other joint-health agents [12:1].
¶ Autophagy and Longevity Mechanics
Glucosamine acts as a cellular caloric restriction mimetic, inducing autophagy through the inhibition of the mTOR (mammalian target of rapamycin) pathway [1:4]. This preserves cellular homeostasis, clears damaged proteins and organelles within senescent chondrocytes, and promotes cell survival under metabolic stress [1:5].
¶ Pharmacokinetics
- Absorption: Oral absorption is highly efficient (~90%), but extensive first-pass hepatic metabolism and gut microflora degradation reduce absolute oral bioavailability to approximately 26% [4:3].
- Distribution: Free glucosamine actively concentrates in articular cartilage and synovial fluid, where it remains detectable above baseline levels for up to 48 hours [13:4].
- Half-life: The elimination half-life from human plasma is estimated to be approximately 15 hours [1:6].
¶ Effects on different systems
¶ Metabolic Health
Early animal models utilizing massive intravenous doses of glucosamine suggested potential impairment of insulin sensitivity. However, high-quality human systematic reviews and clinical trials have conclusively demonstrated that standard oral doses (1,500 mg/day) do not adversely affect fasting blood glucose, insulin resistance, or HbA1c levels in healthy individuals, pre-diabetic patients, or those with well-controlled type 2 diabetes [1:7].
¶ Oncology
Systemic anti-inflammatory effects, particularly the inhibition of NF-κB and downstream PGE2 signaling, are believed to explain the chemopreventive associations observed in colorectal and lung tissues [6:6]. In colorectal tissues, glucosamine inhibits inflammatory cascades within precursor adenomas and serrated polyps, reducing their progression to invasive colorectal cancer [6:7].
¶ Musculoskeletal & Connective Tissue
Glucosamine concentrates heavily in connective tissues, where it enhances chondrocyte metabolic activity and stimulates synovial fluid viscoelasticity by promoting high-molecular-weight hyaluronic acid production [17:2][13:5]. While exercise remains the most powerful intervention for improving knee physical function, glucosamine provides biochemical support to joint tissues [16:1].
¶ Dosage and how to take it
¶ Standard Dosing in Studies
- Daily Dose: 1,500 mg per day.
- Dosing Schedule: Can be taken as a single 1,500 mg dose once daily (achieving higher peak plasma concentrations) or split into three 500 mg doses [1:8].
- Duration: Clinical trials typically range from 4 weeks to 3 years [1:9][15:1]. Symptomatic benefits require a minimum of 4 to 12 weeks of continuous compliance to become apparent [1:10][4:4].
¶ Forms and Bioavailability
- Crystalline Glucosamine Sulfate (pCGS): This specific patented formulation, stabilized with sodium chloride, represents the prescription standard in Europe. It provides highly consistent oral bioavailability, stable plasma concentrations, and established clinical efficacy [4:5][13:6].
- Glucosamine Hydrochloride (HCl): While cheaper and highly common in over-the-counter supplements, it lacks the necessary sulfate moiety, exhibits poor joint tissue concentration, and has consistently failed to show therapeutic efficacy over placebo [3:4][4:6].
- Fungal-Derived Glucosamine: Chemically identical to shellfish-derived forms, fungal-derived (usually Aspergillus niger or fermented corn) glucosamine is the preferred option for vegetarians, vegans, or individuals with severe shellfish allergies.
¶ Special Populations
- Older Adults: Highly well-tolerated with no unique dosage adjustments required; represents the most heavily studied population.
- Renal/Hepatic Impairment: Glucosamine is extensively metabolized and excreted primarily as carbon dioxide via expired air, with minimal renal clearance. However, high-quality data in severe renal or hepatic failure is lacking.
- Pregnancy & Lactation: Clinical safety data is absent; use is not recommended due to insufficient human evidence.
¶ Safety and side effects
Glucosamine exhibits an outstanding safety profile. Large systematic reviews demonstrate that the incidence of adverse events with oral glucosamine is virtually indistinguishable from placebo [1:11][2:3][12:2].
¶ Common Side Effects
When adverse reactions occur, they are generally mild, transient, and gastrointestinal:
- Mild nausea or dyspepsia
- Abdominal pain or bloating
- Diarrhea or constipation
¶ Less Common / Serious Concerns
- Shellfish Allergy: Because most commercial glucosamine is derived from the outer skeletons of shellfish, individuals with severe anaphylactic shellfish allergies must exercise extreme caution. Though the allergen protein is typically removed during processing, choosing vegan/fungal-derived glucosamine is highly recommended to eliminate risk.
¶ Who Should Be Cautious
- Individuals taking oral anticoagulants (see Interactions).
- Individuals with severe, uncompensated diabetes (who should closely monitor blood glucose when initiating therapy).
¶ Drug and supplement interactions
¶ Critical Pharmacokinetic Interactions
- Warfarin (Coumadin): Severe and clinically documented interaction. Oral glucosamine co-administration significantly potentiates the anticoagulant effect of Warfarin, leading to rapid, dangerous elevations in the International Normalized Ratio (INR) (sometimes exceeding 10.0) and severe bleeding events [1:12]. The exact molecular mechanism remains poorly understood, but may involve competitive binding or inhibition of hepatic metabolism. Glucosamine must be strictly avoided by patients on Warfarin, or require exceptionally rigorous INR monitoring during initiation and discontinuation [1:13].
¶ Pharmacodynamic Interactions
- Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): Excellent synergistic relationship. Evidence from scoping and systematic reviews indicates that co-administering glucosamine sulfate with NSAIDs (such as ibuprofen or celecoxib) produces superior, synergistic pain relief in knee osteoarthritis [18][19]. This combination may allow for a significant reduction in the required daily dose of NSAIDs, thereby lowering the risk of NSAID-induced gastrointestinal ulcers and cardiovascular complications [18:1][19:1].
¶ Combining glucosamine with other supplements (“stacks”)
¶ Glucosamine + Chondroitin Sulfate
This is the most common joint-health combination. Chondroitin sulfate is a larger glycosaminoglycan that provides osmotic resistance and water retention in joint cartilage, acting through complementary anti-inflammatory and cartilage-preserving pathways. Network meta-analyses confirm that the combination of pharmaceutical-grade glucosamine sulfate and chondroitin sulfate provides significant structural protection and substantial pain relief in moderate-to-severe knee osteoarthritis [2:4][9:1][12:3].
¶ Glucosamine + Omega-3 Fatty Acids
Combining glucosamine with long-chain omega-3 fatty acids (EPA/DHA) provides highly complementary anti-inflammatory effects [8:1]. While glucosamine works locally via chondrocyte matrix synthesis and NF-κB inhibition, omega-3 fatty acids systematically suppress pro-inflammatory eicosanoids and cytokines (PGE2, IL-1β), resulting in robust pain relief and joint functional improvements [8:2].
¶ Practical questions (FAQ)
How long does it take for glucosamine to work?
Can I take glucosamine if I am allergic to shellfish?
While the allergic proteins are located in the meat of shellfish and glucosamine is extracted from the shells, some risk of contamination remains. Individuals with severe shellfish allergies should avoid animal-derived glucosamine and strictly select fungal-derived or vegan glucosamine supplements [1:15].
Why is there a disagreement about whether glucosamine works?
The medical disagreement stems from the formulation used. European clinical guidelines strongly recommend prescription crystalline glucosamine sulfate because it has high bioavailability and proven efficacy in clinical trials [4:8]. Conversely, American guidelines recommend against it because American over-the-counter supplements predominantly use glucosamine hydrochloride (HCl), which consistently fails to outperform placebo in clinical trials [3:5][4:9].
Does glucosamine cause insulin resistance?
No. High-dose intravenous injections of glucosamine can induce insulin resistance in animal models, but robust human trials show that standard oral doses of 1,500 mg/day have no adverse effects on blood glucose control, insulin sensitivity, or HbA1c in healthy or diabetic adults [1:16].
¶ How we evaluated the evidence
Our scientific evaluation of glucosamine sulfate is built upon a hierarchy of evidence that prioritizes Tier 1 systematic reviews and meta-analyses of human randomized controlled trials (RCTs).
We systematically graded the clinical recommendations according to standard GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) criteria:
- High Certainty: Based on multiple large-scale, placebo-controlled RCTs and systematic network meta-analyses (such as those analyzing crystalline glucosamine sulfate in knee osteoarthritis) with consistent outcomes, low risk of bias, and robust sample sizes.
- Moderate Certainty: Based on moderate-sized RCTs with minor limitations, or mixed results where sub-analyses (e.g., differentiating sulfate vs. hydrochloride formulations) reveal distinct effects.
- Low Certainty: Based on smaller clinical trials, prospective cohort studies (such as cancer prevention or mortality associations), or trials with high risk of bias or conflicting endpoints.
- Very Low Certainty: Based on preclinical animal models, in vitro molecular studies, or isolated clinical case reports.
We plan to dynamically update this monograph as major new double-blind, randomized clinical trials or high-impact clinical guidelines are published.
¶ References
Baden KER, Hoeksema SL, Gibson N, Gadi DN, Craig E, Draime JA, Tubb SM, Chen AMH. The Safety and Efficacy of Glucosamine and/or Chondroitin in Humans: A Systematic Review. Nutrients. 2025;17(13):2093. https://pubmed.ncbi.nlm.nih.gov/40647198/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Rabade A, Viswanatha GL, Nandakumar K. Evaluation of efficacy and safety of glucosamine sulfate, chondroitin sulfate, and their combination regimen in the management of knee osteoarthritis: a systematic review and meta-analysis. Inflammopharmacology. 2024;32(3):1455-1471. https://pubmed.ncbi.nlm.nih.gov/38581640/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Vo NX, Le NNH, Chu TDP. Effectiveness and Safety of Glucosamine in Osteoarthritis: A Systematic Review. Pharmacy (Basel). 2023;11(4):117. https://pubmed.ncbi.nlm.nih.gov/37489348/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Reginster JY, Bruyere O, Neuprez A. Current role of glucosamine in the treatment of osteoarthritis. Rheumatology (Oxford). 2007;46(5):731-735. https://pubmed.ncbi.nlm.nih.gov/17401134/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Liu B, Yang W, Zhang K. Role of Glucosamine and Chondroitin in the Prevention of Cancer: A Meta-Analysis. Nutrition and Cancer. 2023;75(3):803-812. https://pubmed.ncbi.nlm.nih.gov/36715012/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Khan AA, Mannan V, Pervaiz MA. The Role of Glucosamine and Chondroitin Sulfate in the Prevention of Colorectal Cancer: A Systematic Review. Cureus. 2022;14(5):e25401. https://pubmed.ncbi.nlm.nih.gov/35774674/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Zhu X, Sang L, Wu D. Effectiveness and safety of glucosamine and chondroitin for the treatment of osteoarthritis: a meta-analysis of randomized controlled trials. Journal of Orthopaedic Surgery and Research. 2018;13(1):170. https://pubmed.ncbi.nlm.nih.gov/29980200/ ↩︎ ↩︎
Zhu X, Wu D, Sang L. Comparative effectiveness of glucosamine, chondroitin, acetaminophen or celecoxib for the treatment of knee and/or hip osteoarthritis: a network meta-analysis. Clinical and Experimental Rheumatology. 2018;36(4):595-602. https://pubmed.ncbi.nlm.nih.gov/29465368/ ↩︎ ↩︎ ↩︎
Zeng C, Wei J, Li H. Effectiveness and safety of Glucosamine, chondroitin, the two in combination, or celecoxib in the treatment of osteoarthritis of the knee. Scientific Reports. 2015;5:16827. https://pubmed.ncbi.nlm.nih.gov/26576862/ ↩︎ ↩︎
Derwich M, Górski B, Amm E. Oral Glucosamine in the Treatment of Temporomandibular Joint Osteoarthritis: A Systematic Review. International Journal of Molecular Sciences. 2023;24(5):4925. https://pubmed.ncbi.nlm.nih.gov/36902359/ ↩︎ ↩︎ ↩︎ ↩︎
Sivakumar S, Kumar PP, Prasanna PL. Efficiency of Glucosamine in Treating Temporomandibular Joint Osteoarthritis: A Meta-Analytic Umbrella Review. Current Rheumatology Reviews. 2025;21(1):42-51. https://pubmed.ncbi.nlm.nih.gov/38867545/ ↩︎ ↩︎ ↩︎
Wang Z, Wang R, Yao H. Clinical Efficacy and Safety of Chondroitin Combined with Glucosamine in the Treatment of Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Computational and Mathematical Methods in Medicine. 2022;2022:5285244. https://pubmed.ncbi.nlm.nih.gov/35924114/ ↩︎ ↩︎ ↩︎ ↩︎
Lopes Júnior OV, Inácio AM. Use of glucosamine and chondroitin to treat osteoarthritis: a review of the literature. Revista Brasileira de Ortopedia. 2013;48(4):300-306. https://pubmed.ncbi.nlm.nih.gov/31304125/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Knapik JJ, Pope R, Hoedebecke SS. Effects of Oral Glucosamine Sulfate on Osteoarthritis-Related Pain and Joint-Space Changes: Systematic Review and Meta-Analysis. Journal of Special Operations Medicine. 2018;18(4):139-147. https://pubmed.ncbi.nlm.nih.gov/30566740/ ↩︎
Black C, Clar C, Henderson R. The clinical effectiveness of glucosamine and chondroitin supplements in slowing or arresting progression of osteoarthritis of the knee: a systematic review and economic evaluation. Health Technology Assessment. 2009;13(52):1-228. https://pubmed.ncbi.nlm.nih.gov/19903416/ ↩︎ ↩︎
Čeh T, Šarabon N. Effects of adding glucosamine or glucosamine combined with chondroitin to exercise on pain and physical function in adults with knee osteoarthritis: a systematic review and meta-analysis. European Journal of Translational Myology. 2023;33(4):12013. https://pubmed.ncbi.nlm.nih.gov/37997783/ ↩︎ ↩︎
Fernández-Martín S, González-Cantalapiedra A, Muñoz F. Glucosamine and Chondroitin Sulfate: Is There Any Scientific Evidence for Their Effectiveness as Disease-Modifying Drugs in Knee Osteoarthritis Preclinical Studies?-A Systematic Review from 2000 to 2021. Animals. 2021;11(6):1608. https://pubmed.ncbi.nlm.nih.gov/34072407/ ↩︎ ↩︎ ↩︎
Veronese N, Ecarnot F, Cheleschi S. Possible synergic action of non-steroidal anti-inflammatory drugs and glucosamine sulfate for the treatment of knee osteoarthritis: a scoping review. BMC Musculoskeletal Disorders. 2022;23(1):1082. https://pubmed.ncbi.nlm.nih.gov/36510167/ ↩︎ ↩︎
Kongtharvonskul J, Anothaisintawee T, McEvoy M. Efficacy and safety of glucosamine, diacerein, and NSAIDs in osteoarthritis knee: a systematic review and network meta-analysis. European Journal of Medical Research. 2015;20(1):24. https://pubmed.ncbi.nlm.nih.gov/25889669/ ↩︎ ↩︎