¶ Period Pain Action Guide
If pelvic pain exhibits a cyclic pattern, the most effective therapeutic strategy is identification of whether the pain is primary (associated with common cramps) or secondary (caused by an underlying gynecological condition), followed by optimized timing of proven interventions and multimodal layering of non-pharmacological clinical adjuncts to reduce the overall pain burden.
¶ Key Clinical Directives
- Optimize NSAID timing conditionally: For individuals with predictable cycles and no contraindications, starting non-steroidal anti-inflammatory drugs (NSAIDs) 1–2 days before expected bleeding (following label instructions or clinician advice) may optimize efficacy. Otherwise, initiation should occur at the first sign of spotting or cramping.[1][2]
- Apply continuous low-level heat: Continuous low-level topical heat (~40°C or 104°F) has been clinically demonstrated to be as effective as certain oral analgesics for primary dysmenorrhea.[3]
- Rule out secondary causes: If pelvic pain exhibits delayed onset (years after menarche), occurs entirely outside of menses, or is accompanied by severe dyspareunia (painful intercourse), further clinical evaluation is indicated to rule out secondary causes such as endometriosis or fibroids.[4]
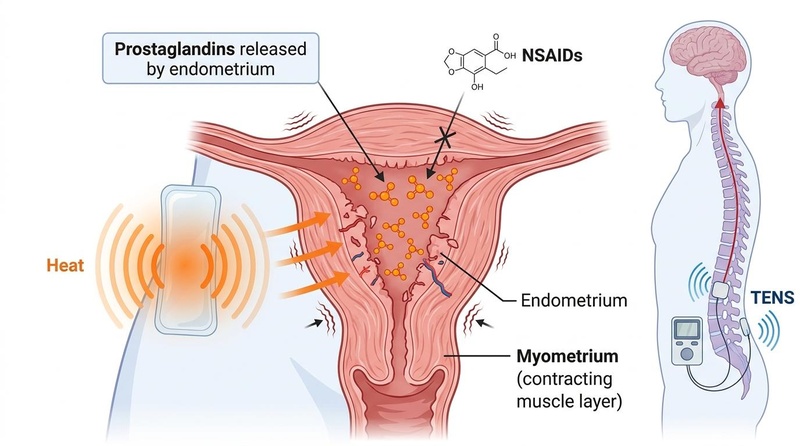
Figure 1: The physiological pathway of primary dysmenorrhea and the targeted mechanisms of common interventions.
¶ Physiological Mechanisms
Primary dysmenorrhea is cramping pain associated with menstruation in the absence of pelvic pathology. It is driven by the release of prostaglandins (primarily prostaglandin F2α and PGE2) from the shedding uterine endometrium. These compounds stimulate vigorous myometrial contractions, causing elevated intrauterine pressure that compresses uterine blood vessels, resulting in transient uterine ischemia and the sensitization of pelvic nociceptors. Secondary dysmenorrhea is distinct, stemming from structural or inflammatory pelvic pathologies such as endometriosis, adenomyosis, or pelvic inflammatory disease (PID).[1:1][4:1]
¶ Clinical Sorting Matrix
| Clinical Presentation | Likely Diagnostic Category | Initial Management / Next Steps |
|---|---|---|
| Cramping in the lower abdomen starting just before or with bleeding; lasts 48–72 hours. | Primary Dysmenorrhea | Optimize NSAID timing (conditional on cycle regularity and contraindications), or consider heat/TENS.[1:2][3:1] |
| Pain that starts years after menarche; occurs outside of menses; non-midline pain. | Secondary Dysmenorrhea | Clinical history evaluation to rule out secondary etiology.[4:2] |
| Pain during intercourse (dyspareunia) or with bowel movements. | Possible Endometriosis | Further medical evaluation (clinical history or empirical therapy; imaging/laparoscopy if indicated).[4:3] |
| Sudden, severe pelvic pain with fever, chills, or unusual discharge. | Possible Infection (PID) | Immediate diagnostic workup for acute pelvic infection.[4:4] |
¶ Interventions Ranked by Evidence
| Intervention | Evidence Level | Clinical Directives | Notes |
|---|---|---|---|
| NSAIDs (e.g., Ibuprofen, Naproxen) | High | Start 1–2 days before expected bleeding if cycles are predictable and no contraindications exist; otherwise, begin at first sign. | First-line medication; inhibits cyclooxygenase (COX) and prostaglandin synthesis. Follow label dosing or clinician guidance.[1:3][2:1] |
| Hormonal Contraceptives | High | Evaluate use of oral contraceptives, progestin-only pills, or levonorgestrel-releasing IUDs. | Inhibits ovulation and suppresses endometrial proliferation, reducing prostaglandin synthesis.[4:5][5] |
| Heat Therapy | Moderate-High | Apply continuous low-level topical heat (~40°C) for several hours. | Enhances local uterine blood flow and promotes myometrial relaxation; synergistic with NSAID therapy.[3:2] |
| Exercise (Yoga, Aerobic) | Moderate | Encourage regular physical activity (e.g., 3x/week for 45-60 min). | Stimulates systemic beta-endorphin release and improves pelvic hemodynamics.[6][7][8] |
| TENS | Moderate | Administer high-frequency (50–120 Hz) stimulation. | Modulates pain perception via the gate control theory and increases endogenous opioids.[9][10][11] |
| Supplements (Zinc, Apiaceae herbs, Vit D/E) | Low-Moderate | Maintain a 3-to-6-month therapeutic trial; clinical evidence is supportive but inconsistent. | Zinc inhibits COX-2 and prostaglandin activity; Apiaceae herbs (e.g., fennel) promote spasmolysis; Vitamin D resolves deficiencies.[12][13][14] |
¶ Clinical Integration Protocol
- Characterize cycle pattern: Track the exact onset and duration of pain relative to menstrual bleeding to differentiate primary from secondary patterns.
- Review medication contraindications: Verify whether NSAIDs are appropriate based on individual health history (e.g., absence of gastric or renal issues) and compile therapeutic options.
- Optimize drug administration timing: If cycles are predictable and no contraindications exist, plan to initiate NSAID therapy 1–2 days before the expected onset of menses in accordance with clinical advice or label instructions; otherwise, plan for initiation at the first sign of spotting or cramping.
- Evaluate non-pharmacological modalities: Implement clinical adjuncts such as continuous low-level topical heat (~40°C), light stretching or yoga, or a high-frequency TENS unit during peak pain hours.
¶ Safety and Diagnostic Considerations
NSAIDs represent a primary pharmacological intervention but are associated with notable contraindications, including active peptic ulcer disease, aspirin-sensitive asthma, and renal impairment. Combining multiple NSAIDs is discouraged due to cumulative toxicity risks without added efficacy. Follow standard label instructions or individual clinician guidance.
¶ Diagnostic Red Flags (Clinical Indicators for Investigation)
Professional guidelines highlight several key clinical indicators that differentiate primary dysmenorrhea from acute gynecological emergencies or underlying secondary pathology:
- Ectopic Pregnancy or Ruptured Cyst or Tube: Someone who could be pregnant and has severe one-sided pain, shoulder-tip pain, or fainting needs urgent assessment for ectopic pregnancy. Severe sharp pain can also indicate a ruptured cyst or tube, especially if accompanied by dangerously low blood pressure or fainting.
- Severe Hemorrhage: Excessively heavy bleeding (such as saturating more than one pad or tampon per hour) accompanied by fainting, severe fatigue, or symptoms of anemia.
- Acute Pelvic Infection or Torsion: High fever, chills, abnormal or purulent cervical discharge, or acute-onset severe localized abdominal pain.
- Secondary Dysmenorrhea Patterns: Pain that is progressive (worsening over time), starts years after the first period, occurs entirely outside of menses, or remains refractory to optimized first-line treatments.
¶ FAQ
¶ Can TENS and heat therapy be utilized simultaneously?
While both modalities provide pain relief, they operate via distinct physiological mechanisms: heat promotes vasodilation and muscle relaxation, whereas TENS modulates neural pain gating. They can be used sequentially; before simultaneous application, verify device-specific safety protocols regarding thermal conduction.
¶ How is endometriosis diagnosed?
Endometriosis often presents with pain that is more severe, progressive, or starts earlier in the cycle than typical primary dysmenorrhea. While specialized imaging (such as transvaginal ultrasound or MRI) and diagnostic laparoscopy can identify or confirm lesions, a clinical diagnosis can often be made empirically based on history and clinical response to therapeutic trials, meaning invasive procedures or imaging are not always required for initial management.[4:6]
¶ Are there non-pharmacological botanical or micronutrient alternatives with clinical evidence?
Herbaceous Apiaceae plants (including fennel, anise, and celery seed) and Traditional Chinese Medicine formulations (such as Siwutang) have demonstrated pain-reduction efficacy in randomized controlled trials. Zinc supplementation initiated 1–4 days before menses has also shown clinical utility in mitigating pain, likely via prostaglandin synthesis inhibition.[13:1][14:1][15]
¶ Related Clinical Resources
If first-line options are insufficient, read our Women's Longevity Guide or explore Perimenopause and Menopause Longevity for hormonal context.
¶ References
French L. Dysmenorrhea. Am Fam Physician. 2005. https://pubmed.ncbi.nlm.nih.gov/15686299/ ↩︎ ↩︎ ↩︎ ↩︎
Zhao M, Zhou F, Qiu C. Long-Term Management and Prevention Strategies for Adolescent Primary Dysmenorrhea: From Precision Diagnosis to Comprehensive Intervention. Int J Womens Health. 2026. https://pubmed.ncbi.nlm.nih.gov/42416113/ ↩︎ ↩︎
Igwea SE, Tabansi-Ochuogu CS, Abaraogu UO. TENS and heat therapy for pain relief and quality of life improvement in individuals with primary dysmenorrhea: A systematic review. Complement Ther Clin Pract. 2016. https://pubmed.ncbi.nlm.nih.gov/27502806/ ↩︎ ↩︎ ↩︎
Burnett M. Guideline No. 345: Primary Dysmenorrhea. J Obstet Gynaecol Can. 2025. https://pubmed.ncbi.nlm.nih.gov/40216328/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Damm T, Lamvu G, Carrillo J. Continuous vs. cyclic combined hormonal contraceptives for treatment of dysmenorrhea: a systematic review. Contracept X. 2019. https://pubmed.ncbi.nlm.nih.gov/32550522/ ↩︎
Zheng Q, Huang G, Cao W. Comparative effectiveness of exercise interventions for primary dysmenorrhea: a systematic review and network meta-analysis. BMC Womens Health. 2024. https://pubmed.ncbi.nlm.nih.gov/39550537/ ↩︎
Alghosi M, Barati M, Sedaghati P. Effects of Lumbopelvic Exercise-based Interventions on Primary Dysmenorrhea: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Midwifery Womens Health. 2026. https://pubmed.ncbi.nlm.nih.gov/41944508/ ↩︎
McGovern CE, Cheung C. Yoga and Quality of Life in Women with Primary Dysmenorrhea: A Systematic Review. J Midwifery Womens Health. 2018. https://pubmed.ncbi.nlm.nih.gov/29902363/ ↩︎
Ahmed MJ, Aldawsari WA, Aleid AM. Transcutaneous electrical nerve stimulation for treatment of primary dysmenorrhea: A systematic review and meta-analysis of randomized controlled trials. Medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/41790650/ ↩︎
Benduch M, Stania M. Is TENS an effective physical monotherapy for primary dysmenorrhea? A systematic review and meta-analysis. Pain Management. 2026. https://pubmed.ncbi.nlm.nih.gov/41383135/ ↩︎
Arik MI, Kiloatar H, Aslan B. The effect of TENS for pain relief in women with primary dysmenorrhea: A systematic review and meta-analysis. Explore (New York). 2022. https://pubmed.ncbi.nlm.nih.gov/32917532/ ↩︎
Hosseini MS, Talayeh M, Haghbin Toutounchi A. Effect of vitamin D and E supplementation on pain relief and premenstrual symptoms in primary dysmenorrhea: a randomized controlled trial. BMC Womens Health. 2025. https://pubmed.ncbi.nlm.nih.gov/41023678/ ↩︎
Hsu TJ, Hsieh RH, Huang CH. Efficacy of Zinc Supplementation in the Management of Primary Dysmenorrhea: A Systematic Review and Meta-Analysis. Nutrients. 2024. https://pubmed.ncbi.nlm.nih.gov/39683510/ ↩︎ ↩︎
Thaliyil Poduval A, Ramalekshmi VL, Vijayan Sarangi N. Efficacy of herbaceous Apiaceae plants in primary dysmenorrhea: A systematic review and meta-analysis of RCTs. Ann Pharm Fr. 2026. https://pubmed.ncbi.nlm.nih.gov/41653970/ ↩︎ ↩︎
Li G, Liu A, Lin M. Chinese herbal formula siwutang for treating primary dysmenorrhea: A systematic review and meta-analysis of randomized controlled trials. Maturitas. 2020. https://pubmed.ncbi.nlm.nih.gov/32631585/ ↩︎