¶ Glycemic Control
¶ TL;DR
- Verdict: Optimizing glycemic control is a cornerstone of metabolic health and healthspan extension, achieved via a synergistic combination of personalized dietary modification, targeted physical exercise interventions, and real-time biofeedback.
- Target Audience: Ideal for individuals looking to optimize energy, mitigate systemic inflammation, and prevent metabolic decline; not suitable for individuals with active eating disorders or pregnant women without specialized clinical supervision.
- Efficacy & Timeline: Expect a 10% to 15% increase in CGM-derived Time-in-Range (TIR) within 2 to 4 weeks, and a 0.5% to 1.2% absolute reduction in HbA1c over 12 weeks.
- Key Risk: Reactive hypoglycemia or over-restriction of nutrient-dense carbohydrates leading to muscle glycogen depletion and endocrine disruption.
- Next Action: Set a baseline HbA1c and fasting glucose level, then initiate a 14-day continuous glucose monitor (CGM) trial combined with structured post-meal walking.
¶ Quick Answer
Glycemic control refers to the maintenance of blood glucose levels within a narrow physiological range (typically 70 to 140 mg/dL or 3.9 to 7.8 mmol/L postprandially) to minimize glycemic variability and avoid chronic hyper- or hypoglycemia. In clinical settings, optimal control translates to an HbA1c of <5.4% and a continuous glucose monitor (CGM) Time-in-Range (70-140 mg/dL) of >90%. Achieving these metrics reduces systemic advanced glycation end-product (AGE) accumulation and maintains microvascular integrity. This is best accomplished by combining low-glycemic or Mediterranean-style dietary patterns with post-prandial muscular contraction (e.g., 10–15 minute walks) to facilitate non-insulin-mediated glucose clearance.
¶ What It Is
Glycemic control represents the tight homeostatic regulation of blood glucose concentrations by the endocrine system. Under normal physiological conditions, the pancreas secretes insulin (from beta cells) to lower blood glucose, and glucagon (from alpha cells) to raise it. However, chronic overnutrition, physical inactivity, and sleep deprivation disrupt this delicate feedback loop, leading to insulin resistance—a pathological state where peripheral tissues (primarily skeletal muscle and adipose tissue) exhibit a blunted response to insulin signals.
¶ What Counts and What Doesn’t
- What Counts: Minimizing postprandial glucose excursions (spikes), reducing glycemic variability (the amplitude of glucose swings), and maintaining low-normal fasting blood glucose (80–90 mg/dL) and HbA1c (<5.4%).
- What Doesn't: Merely suppressing glucose peaks by starving the body of essential nutrients, or relying entirely on glucose-lowering pharmacological agents (e.g., sulfonylureas) that increase glycemic variability and drive hypoglycemic episodes.
 trace comparison. An unstable profile (left) displays high glycemic variability and extreme spikes/crashes, whereas an optimized profile (right) maintains stable glucose levels within the target 70–140 mg/dL range (>90% Time-in-Range).")
¶ Mechanism in 60 Seconds: Cellular Glucose Transport
Skeletal muscle is the primary sink for postprandial glucose clearance, accounting for up to 80% of insulin-stimulated glucose disposal. This process is mediated by Glucose Transporter Type 4 (GLUT4), a specialized transport protein that resides in intracellular vesicles.
Glucose uptake occurs via two major, non-overlapping cellular pathways:
- The Insulin-Dependent Pathway: Insulin binding to the insulin receptor on the cell membrane triggers the phosphorylation of Insulin Receptor Substrate 1 (IRS-1). This activates Phosphoinositide 3-kinase (PI3K) and downstream Akt (protein kinase B), signaling the GLUT4 storage vesicles (GSVs) to dock and fuse with the plasma membrane, allowing glucose entry.
- The Exercise/Contraction-Dependent Pathway: Muscle contractions deplete cellular energy, increasing the AMP-to-ATP ratio. This activates Adenosine Monophosphate-Activated Protein Kinase (AMPK). AMPK bypasses the insulin receptor entirely, directly triggering GLUT4 translocation. This is why physical activity is highly effective at clearing blood glucose even in severely insulin-resistant individuals.
Once inside the cell, glucose is immediately phosphorylated by hexokinase into glucose-6-phosphate, preventing it from escaping back into the bloodstream.
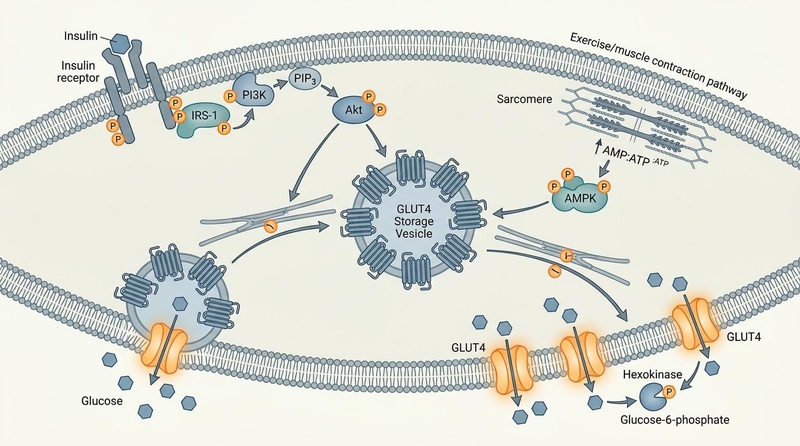
Figure 1: Cellular Mechanisms of Glycemic Control. The dual signaling pathways regulating GLUT4 translocation: the insulin-dependent IRS-1/PI3K/Akt pathway (left) and the exercise/contraction-dependent AMPK pathway (right) converge to drive GLUT4 vesicle docking and facilitate glucose entry.
¶ Does It Work? (Evidence Snapshot)
The clinical utility of dietary and lifestyle interventions for glycemic control is supported by a large volume of Tier 1 evidence, including multi-center randomized controlled trials (RCTs) and systematic reviews.
¶ Human Clinical Outcomes (Evidence Summary Table)
| Target Outcome | Intervention | Population | Typical Effect Size | Certainty Grade (GRADE) | Study Count & Best Design |
|---|---|---|---|---|---|
| HbA1c Reduction | Combined Diet and Exercise | Type 2 Diabetes / Prediabetes | -0.5% to -1.2% absolute reduction over 12–24 weeks [1][2] | High | >30 RCTs, Systematic Meta-Analysis [1:1] |
| Glycemic Variability & Time-in-Range | High-Intensity Interval Training (HIIT) | Adults with Type 2 Diabetes | +10% to +15% TIR; significantly reduced nocturnal glucose [3] | High | Systematic Review & Meta-Analysis of RCTs [3:1] |
| Postprandial Excursions | Frequent Sit-to-Stand Breaks | Sedentary Adults with Dyslipidemia | -15% to -25% reduction in postprandial glucose peaks [4] | High | Randomized Crossover Trial [4:1] |
| HbA1c & Lipids | Carbohydrate Counting & Diet Adherence | Type 1 Diabetes (Brazil cohort) | Lower HbA1c, lower LDL, lower TG, higher rate of achieving HbA1c goals [5] | Moderate (due to observational self-reports) | Multi-center Cohort Survey (3,180 subjects) [5:1] |
| HbA1c & Weight Loss | Low-Carbohydrate Diets (<130g/day) | Type 2 Diabetes | -0.4% to -1.0% HbA1c reduction; substantial fat mass loss [6][7] | Moderate (due to long-term compliance drop-off) | Systematic Review of RCTs (>12 weeks) [6:1] |
| Fasting Blood Glucose & HbA1c | Garlic Supplementation (Adjunct) | Adults with Impaired Glucose | -10 to -22 mg/dL Fasting Glucose; -0.2% to -0.5% HbA1c [8] | Moderate | GRADE-Assessed Dose-Response Meta-Analysis [8:1] |
| Advanced Glycation End-Products (AGEs) | High Mediterranean Diet Adherence | Type 2 Diabetes / Healthy Adults | Significant reduction in systemic AGE accumulation and improved lipid/glycemic markers [9][10] | High | Systematic Reviews & Cross-Sectional Studies [9:1][11] |
| Time-in-Range (TIR) & Hypoglycemia | Continuous Glucose Monitor (CGM) | Glycogen Storage Disease / Healthy | High clinical utility; reduces hypoglycemia risk by providing real-time trend alarms [12] | High | Systematic Review of Utility & Accuracy [12:1] |
¶ Who Benefits Most / Least
¶ Who Benefits Most
- Individuals with Prediabetes or Early Type 2 Diabetes: These subjects possess substantial residual pancreatic beta-cell function, meaning targeted dietary shifts and exercise can frequently restore insulin sensitivity and halt progression [1:2][13].
- Sedentary Desk Workers: Individuals who sit for >8 hours per day experience profound improvements in postprandial metabolic efficiency by simply introducing brief muscular contractions (such as sit-to-stand breaks) [4:2][14].
- Athletes and Active Biohackers: CGMs allow active individuals to optimize peri-workout carbohydrate timing, preventing intra-workout hypoglycemia and accelerating muscle glycogen replenishment [15].
- Patients with Type 1 Diabetes: Structured dietary tracking and carbohydrate counting are primary predictors of meeting glycemic targets and avoiding cardiovascular complications [5:2][16].
¶ Who Benefits Least
- Late-Stage Type 2 Diabetics with Beta-Cell Exhaustion: If pancreatic insulin secretory capacity is irreversibly depleted, lifestyle modifications alone are insufficient, and exogenous insulin or intensive pharmacotherapy is required.
- Chronic High-Stress Cohorts: Under constant hypercortisolemia, gluconeogenesis remains highly active regardless of dietary restriction, leading to elevated fasting glucose levels that do not fully respond to standard dietary protocols [17].
- Individuals with Active Eating Disorders: Tracking every gram of carbohydrate or constantly monitoring CGM graphs can worsen orthorexic behaviors and anxiety.
¶ How to Try It (Actionable Protocols)
Implementing glycemic control strategies requires a multi-layered approach that integrates dietary changes, movement, and digital tracking.
¶ 1. The "Postprandial Contraction" Starter Protocol
This protocol leverages the insulin-independent GLUT4 pathway to immediately clear post-meal glucose spikes [4:3].
- Action: Within 10 to 15 minutes of finishing a main meal, perform 10 to 15 minutes of light-to-moderate physical activity.
- Preferred Activities: Brisk walking, continuous bodyweight squats, or utilizing a standing desk with frequent sit-to-stand intervals (at least 2–3 minutes of standing every 30 minutes) [4:4][14:1].
- Expected Outcome: A 15% to 25% reduction in the post-meal glucose peak, with a faster return to baseline (within 2 hours).
¶ 2. The Mediterranean-Based Nutritional Protocol
Adherence to a Mediterranean diet improves peripheral insulin sensitivity and protects pancreatic beta-cells from lipotoxic damage [11:1][10:1].
- Core Composition:
- Fats: High intake of monounsaturated fatty acids (MUFAs), primarily from extra virgin olive oil (2–4 tablespoons daily).
- Proteins: Prioritize wild-caught seafood, lean poultry, and plant-based proteins (legumes, nuts).
- Carbohydrates: Strictly whole grains, vegetables, and low-glycemic fruits (berries). Eliminate all ultra-processed foods (UPFs) which are linked to gut microbiome dysbiosis and elevated glycemic variability [18].
- Adjuncts: Incorporate carob-derived products (rich in d-chiro-inositol) to improve insulin action [19], and consider 800–1200 mg of standardized garlic extract daily to reduce fasting blood glucose [8:2].
- Carbohydrate Sequencing: Always consume fiber, protein, and fats before complex carbohydrates. This delays gastric emptying and dampens the rate of glucose absorption in the small intestine.
¶ 3. The High-Intensity Interval Training (HIIT) Glycemic Protocol
For those seeking to maximize insulin sensitivity and elevate GLUT4 transcription over the medium term, structured HIIT outperforms steady-state cardio for CGM-derived metrics [3:2][17:1].
- Frequency: 2 to 3 sessions per week, separated by at least 48 hours.
- Interval Structure:
- Warm-up: 5 minutes of light rowing or cycling.
- Active Phase: 4 to 6 rounds of 1-minute high-intensity work (85–95% of peak heart rate) followed by 1 minute of active recovery (light cycling/walking).
- Cool-down: 5 minutes of passive stretching.
- Timing: Perform sessions in the late afternoon to specifically mitigate evening and nocturnal glycemic excursions [3:3].
¶ Alternatives
If high-intensity exercise is contraindicated due to cardiovascular risk, structured Yoga has been shown in network meta-analyses to yield comparable HbA1c reductions to HIIT, primarily through cortisol reduction and parasympathetic nervous system activation [17:2].
¶ Safety, Interactions, Red Flags
¶ Who Should Avoid
- Pregnant Women without Medical Oversight: Tight restriction of carbohydrates can lead to gestational ketosis, which requires strict monitoring by an obstetrician [1:3].
- Type 1 Diabetics without Insulin Titration Protocols: Implementing drastic low-carbohydrate diets without adjusting basal and bolus insulin doses carries a severe risk of hypoglycemia or euglycemic diabetic ketoacidosis (DKA) [5:3][16:1].
¶ Common Side Effects & Mitigations
-
The "Low-Carb Flu" (Keto-Induction Phase): Rapidly reducing carbohydrates causes renal sodium excretion, leading to headaches, lethargy, and mild hypotension.
-
Reactive Hypoglycemia: A rapid spike in high-glycemic carbohydrates followed by an over-secretion of insulin, crashing blood glucose below 70 mg/dL.
- Mitigation: Avoid naked carbohydrates; always pair starch or sugar with healthy fats, fiber, or protein.

¶ Drug and Supplement Interactions
- Exogenous Insulin & Sulfonylureas: Combining intensive dietary restriction or post-meal exercise with these medications dramatically increases the risk of severe hypoglycemia. Continuous glucose monitoring is essential for safe dose titration.
- Metformin: Metformin alters gut microbiota metabolism and increases GLP-1 secretion. Combining it with a high-fiber Mediterranean diet produces highly synergistic glycemic benefits, though it may transiently increase mild gastrointestinal distress [2:1].
- SGLT2 Inhibitors (e.g., Empagliflozin): These drugs lower glucose via renal excretion. Combining SGLT2 inhibitors with a strict ketogenic diet increases the risk of euglycemic DKA.
- Herbal Glycemic Agents: Supplements like Berberine, Garlic [8:3], and certain polyphenols act via AMPK activation or SGLT inhibition [21]. Exercise caution when stacking these with prescribed antidiabetic pharmaceuticals.
¶ Discontinuation Criteria (Red Flags)
Cease unsupervised lifestyle shifts and consult a clinician if you encounter:
- Recurrent Hypoglycemia: Confirmed blood glucose readings <55 mg/dL accompanied by diaphoresis, palpitations, or confusion.
- Persistent Ketoacidosis Signs: Elevated blood ketones (>3.0 mmol/L) accompanied by nausea, vomiting, rapid deep breathing, or a sweet-smelling breath.
- Severe Orthostatic Hypotension: Dizziness upon standing that does not resolve with electrolyte replenishment.
¶ Tracking & What “Good” Looks Like
Effective glycemic management relies on a combination of laboratory biomarkers, continuous interstitial glucose monitoring, and subjective physiological feedback.
¶ Key Biomarkers for Glycemic Assessment
| Biomarker | Optimal Target | Frequency | Clinical Significance |
|---|---|---|---|
| HbA1c (Glycated Hemoglobin) | <5.4% | Every 3 months | Reflects the 3-month weighted average of blood glucose levels based on red blood cell glycation. |
| Fasting Blood Glucose | 80 to 90 mg/dL (4.4 to 5.0 mmol/L) | Monthly (or daily via fingerprick) | Indicates basal hepatic glucose output during fasting states. |
| Time-in-Range (TIR) | >90% of readings between 70–140 mg/dL | Continuous (via CGM) | The gold standard for assessing glycemic variability; strongly correlated with lower macrovascular risk [15:1]. |
| Standard Deviation (SD) / Coefficient of Variation (CV) | CV < 36% (SD < 20 mg/dL) | Continuous (via CGM) | Represents the mathematical amplitude of glucose swings; lower numbers mean higher vascular safety. |
| Fasting Insulin | < 5.0 μIU/mL | Every 6 months | Early marker of insulin resistance; can be elevated long before fasting glucose rises. |
¶ Subjective Metrics
- No "Afternoon Slump": Consistent, stable cognitive energy 1 to 3 hours after lunch, indicating a lack of reactive hypoglycemia.
- Reduced Sugar Cravings: Stable appetite levels, driven by flat insulin profiles.
- Improved Sleep Architecture: Absence of nocturnal awakenings caused by reactive hypoglycemia-induced adrenaline surges [22].
¶ Timeline to Benefit
- Interstitial Glucose Profiles (CGM): Visual improvements in glycemic variability and postprandial curves are observable within 24 to 48 hours of starting post-meal walks and carbohydrate sequencing [4:5].
- HbA1c Reductions: Require 10 to 12 weeks of consistent intervention to show significant statistical shifts due to the ~120-day lifespan of red blood cells.
¶ Common Mistakes & Myths
- Myth: "A food is healthy as long as it doesn't spike my blood glucose."
- Reality: Pure fats and oils do not spike blood glucose, yet consuming them in massive excess can induce ectopic lipid accumulation in skeletal muscle and liver tissue, ultimately worsening long-term insulin resistance.
- Myth: "Fasting glucose is the only metric that matters."
- Reality: Fasting glucose is often the last marker to break. An individual can maintain a normal fasting glucose of 90 mg/dL for years while requiring massive, pathological levels of fasting insulin (hyperinsulinemia) to keep it there.
- Mistake: Over-restricting fiber-rich carbohydrates.
- Mistake: Ignoring sleep deprivation.
- Reality: Even a single night of partial sleep deprivation (4 hours) induces acute insulin resistance comparable to several weeks of a high-fat, high-sucrose diet, completely undermining dietary diligence [22:1].
¶ Decision Tree (Text-Based)
[Start: Assess Glycemic Baseline]
│
▼
Is your HbA1c < 5.4% and Fasting Glucose < 95 mg/dL?
├─► YES: Maintain metabolic health.
│ Focus on: 10-min post-meal walks & fiber-first food sequencing.
│
└─► NO (or Unknown):
│
▼
Do you have diagnosed Type 1 Diabetes or pregnant?
├─► YES: DO NOT make rapid dietary shifts alone.
│ Action: Use continuous glucose monitoring (CGM) under strict specialist guidance.
│
└─► NO:
│
▼
Are you highly sedentary (<5,000 steps/day)?
├─► YES: Implement the "Postprandial Contraction" Protocol.
│ Action: Stand or walk for 10-15 mins immediately after every meal.
│
└─► NO:
│
▼
Implement Mediterranean/Low-Carb Diet & HIIT.
Action: Cut UPFs, add monounsaturated fats, and do HIIT 2-3x/week.
Track: Perform a 14-day CGM self-experiment to identify triggers.
¶ FAQs
¶ Can healthy, non-diabetic individuals benefit from wearing a CGM?
Yes. Healthy individuals frequently experience asymptomatic glycemic excursions into the diabetic range (>140 mg/dL) following specific food triggers. Wearing a CGM for a brief 14-day period provides valuable real-time biofeedback, allowing individuals to identify personal "hyper-spikers" and adjust their dietary architecture accordingly [15:2]. For a comprehensive guide on designing a structured testing protocol around glycemic biofeedback and other biomarker-specific dietary trials, see our N-of-1 Nutrition Testing monograph.
¶ Why does sleep deprivation raise blood glucose levels?
Sleep deprivation elevates systemic cortisol and sympathetic nervous system activity. Cortisol stimulates hepatic gluconeogenesis (glucose production by the liver) and inhibits insulin-stimulated GLUT4 translocation in skeletal muscle, leading to elevated fasting and postprandial glucose levels [22:2].
¶ Is a ketogenic diet superior to a Mediterranean diet for glycemic control?
In the short-to-medium term (3 to 6 months), a ketogenic diet typically induces a faster and deeper reduction in HbA1c and glycemic variability [7:2]. However, over 12 months, systematic reviews show that the difference in HbA1c between low-carb and high-quality Mediterranean diets narrows, largely due to long-term compliance challenges with ketogenic protocols [6:2][20:2]. Additionally, the Mediterranean diet provides superior long-term cardiovascular safety and gut microbiome support [11:2][10:2][16:3].
¶ How does garlic supplementation improve fasting glucose?
Garlic contains bioactive sulfur compounds, such as allicin, which have been shown in meta-analyses to enhance insulin secretion from pancreatic beta-cells, improve insulin sensitivity, and exert antioxidant effects that reduce pancreatic inflammation [8:4].
¶ Glossary
- HbA1c: Glycated hemoglobin; a biomarker reflecting the average blood glucose concentration over the preceding 8 to 12 weeks.
- Time-in-Range (TIR): The percentage of time an individual's glucose level remains within a target range (typically 70–140 mg/dL for optimal health).
- Glycemic Variability: The degree of fluctuation in blood glucose levels, including the amplitude and frequency of spikes and drops throughout the day.
- GLUT4: Glucose Transporter Type 4; the primary insulin-regulated glucose transporter found in skeletal muscle and adipose tissue.
- AMPK: Adenosine Monophosphate-Activated Protein Kinase; an energy-sensing cellular enzyme that, when activated by exercise, triggers glucose uptake independently of insulin.
- Advanced Glycation End-Products (AGEs): Harmful compounds formed when proteins or fats combine with sugar in the bloodstream, contributing to cellular aging and vascular stiffness.
¶ Methods (Transparency)
This deep dive was compiled using a systematic literature review of databases including PubMed, Cochrane Library, and Google Scholar up to July 2026.
¶ Inclusion and Exclusion Rules
- Inclusion: Randomized controlled trials, systematic reviews, meta-analyses, and large cohort studies assessing dietary, lifestyle, or supplement interventions on HbA1c, fasting glucose, or CGM-derived metrics in humans.
- Exclusion: Animal or in vitro mechanistic models unless directly clarifying a human pathway; studies evaluating pharmacological interventions as a primary therapy (with the exception of metformin-lifestyle interaction tracking).
¶ Evidence Grading Rubric
- High Certainty: Requires multiple well-designed RCTs or prospective meta-analyses demonstrating consistent glycemic outcomes with low risk of bias.
- Moderate Certainty: Attributed to interventions with 1–2 high-quality RCTs, large observational cohorts with self-reported data, or those exhibiting higher variability in human compliance (e.g., long-term low-carbohydrate diets).
- Low Certainty: Applied to mechanistic hypotheses, small pilot studies, or those with highly conflicting clinical results.
¶ References
¶ Update Log
- July 2026: Fully updated with the latest clinical data from multi-center trials on continuous glucose monitoring (CGM) metrics, low-carbohydrate and Mediterranean diet impacts, and exercise synergy outcomes.
Huang X, Huang G, Jiang M. Effectiveness of diet-combined exercise interventions for glycemic control in patients with type 2 diabetes: a meta-analysis of randomized controlled trials. The Journal of Sports Medicine and Physical Fitness. 2026. https://pubmed.ncbi.nlm.nih.gov/41664973/ ↩︎ ↩︎ ↩︎ ↩︎
Verde L, Annunziata G, Camajani E. Personalized Medical Nutrition Therapy and Physical Exercise: The Future of Diabesity Care. Current Obesity Reports. 2026. https://pubmed.ncbi.nlm.nih.gov/41813871/ ↩︎ ↩︎
Li J, Yuan J, Zhang Y. High-intensity interval training and continuous glucose monitoring-derived glycemic outcomes in adults with type 2 diabetes: a systematic review and meta-analysis. Frontiers in Endocrinology. 2026. https://pubmed.ncbi.nlm.nih.gov/42388860/ ↩︎ ↩︎ ↩︎ ↩︎
Vanherle JLP, Franssen WMA, Nieste I. Sit-To-Stand Breaks to Optimize Cardiometabolic Health Effects Following Exercise in Sedentary Adults With Dyslipidaemia: A Randomized Crossover Trial. Scandinavian Journal of Medicine & Science in Sports. 2026. https://pubmed.ncbi.nlm.nih.gov/42400437/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Davison KA, Negrato CA, Cobas R, et al. Relationship between adherence to diet, glycemic control and cardiovascular risk factors in patients with type 1 diabetes: a nationwide survey in Brazil. Nutrition Journal. 2014. https://pubmed.ncbi.nlm.nih.gov/35459205/ ↩︎ ↩︎ ↩︎ ↩︎
Castañeda-González LM, Bacardí Gascón M, Jiménez Cruz A. Effects of low carbohydrate diets on weight and glycemic control among type 2 diabetes individuals: a systemic review of RCT greater than 12 weeks. Nutricion Hospitalaria. 2011. https://pubmed.ncbi.nlm.nih.gov/22411372/ ↩︎ ↩︎ ↩︎
An Y, Norris N, Li D. Ketogenic Diet in Obesity and Diabetes: A Narrative Review. Nutrients. 2026. https://pubmed.ncbi.nlm.nih.gov/42356391/ ↩︎ ↩︎ ↩︎
Alsanie SA, Alblaji M, Almutairi SM. Effects of garlic supplementation on glycemic indices in adults: a GRADE-assessed systematic review and dose-response meta-analysis of randomized controlled trials. Diabetes Research and Clinical Practice. 2026. https://pubmed.ncbi.nlm.nih.gov/42398591/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Patsiliva M, Theodorakopoulou A, Stergioti A. Association Between Advanced Glycation End-Products and Adherence to the Mediterranean Diet in Individuals with Type 2 Diabetes Mellitus: A Cross-Sectional Study. Nutrients. 2026. https://pubmed.ncbi.nlm.nih.gov/42356273/ ↩︎ ↩︎
Vavitis A, Anastasiou IA, Kounatidis D. Adherence to the Mediterranean Diet Is a Strong Predictor of Glycemic and Lipidemic Control in Adults with Type 2 Diabetes: An Observational Study. Nutrients. 2026. https://pubmed.ncbi.nlm.nih.gov/41599898/ ↩︎ ↩︎ ↩︎
Majić Milotić D, Bulum T, Peroš K. Mediterranean Dietary Pattern in Type 2 Diabetes Management: Pathways and Clinical Evidence. Biomedicines. 2026. https://pubmed.ncbi.nlm.nih.gov/42351778/ ↩︎ ↩︎ ↩︎
Mohsenipour R, Abbasi F, Ghaderian MS. Continuous Glucose Monitoring in Glycogen Storage Diseases: A Systematic Review of Clinical Utility, Accuracy and Patient Outcomes. Endocrinology, Diabetes & Metabolism. 2026. https://pubmed.ncbi.nlm.nih.gov/42394382/ ↩︎ ↩︎
Lalama E, Csanalosi M, Kabisch S. Effect of a Personalized Mobile App on Glucose Control in Adults With Prediabetes and Type 2 Diabetes: Exploratory Pilot Randomized Controlled Trial. JMIR Human Factors. 2026. https://pubmed.ncbi.nlm.nih.gov/42342244/ ↩︎
Park C, Dietrich M, Larsen B. Feasibility and Preliminary Efficacy of a "Sit Less" Program Leveraging Fitbit Tracking and Tailored Text Messages in Cardiometabolic Disease: Findings from Two Parallel Randomized Controlled Trials. JMIR mHealth and uHealth. 2026. https://pubmed.ncbi.nlm.nih.gov/42350337/ ↩︎ ↩︎
Zakaria L. Leveraging Wearable Technology to Support Behavior Change in Personalized Nutrition and Lifestyle Medicine. American Journal of Lifestyle Medicine. 2026. https://pubmed.ncbi.nlm.nih.gov/42395931/ ↩︎ ↩︎ ↩︎
Abuqwider J, Pasolli E, Scidà G. Gut microbiome profiles and associated functional pathways are linked to Mediterranean diet adherence and blood glucose control in adults with type 1 diabetes mellitus. Nutrition, Metabolism, and Cardiovascular Diseases : NMCD. 2026. https://pubmed.ncbi.nlm.nih.gov/41484024/ ↩︎ ↩︎ ↩︎ ↩︎
Thu SYW, Patnaik S, Shih YH. Yoga and High-Intensity Interval Training Show Comparable Effects on HbA1c in Type 2 Diabetes: A Systematic Review and Preliminary Pilot Network Meta-Analysis in Adult Populations. Healthcare (Basel, Switzerland). 2026. https://pubmed.ncbi.nlm.nih.gov/42354561/ ↩︎ ↩︎ ↩︎
Abuqwider J, Pasolli E, Scidà G. Ultra-processed food intake and its associations with atherogenic dyslipidemia, glycemic control, and gut microbiome features in adults with type 1 diabetes from Southern Italy. Diabetes Research and Clinical Practice. 2026. https://pubmed.ncbi.nlm.nih.gov/42341885/ ↩︎
Victoria-Montesinos D, González-Louzao R, Barcina-Pérez P. Effects of carob (Ceratonia siliqua) and carob-derived products on glycaemic control and insulin resistance: A systematic review of clinical trials. Nutrition Research (New York, N.Y.). 2026. https://pubmed.ncbi.nlm.nih.gov/42372710/ ↩︎
Cioffi G, Cuomo G, Carluccio R. Ketogenic diet, cardiometabolic diseases and aging. Journal of Geriatric Cardiology : JGC. 2026. https://pubmed.ncbi.nlm.nih.gov/42395849/ ↩︎ ↩︎ ↩︎
Harbuwono DS, Wardhani Y, Hadinata E. A putative SGLT-relevant mechanistic perspective on quercetin-3-O-glucoside and rutin in diabetic kidney disease. Diabetology & Metabolic Syndrome. 2026. https://pubmed.ncbi.nlm.nih.gov/42399973/ ↩︎
Xu Y, Jin R, Pang J. Sleep patterns, physical activity and glycemic control in newly diagnosed type 2 diabetes patients from a joint perspective: a cross-sectional study. Frontiers in Endocrinology. 2026. https://pubmed.ncbi.nlm.nih.gov/42388868/ ↩︎ ↩︎ ↩︎