¶ Bedroom Darkness: Environmental Sleep-Space Optimization
¶ TL;DR
- The Verdict: Complete bedroom darkness is a primary environmental regulator of human circadian biology, preventing metabolic, autonomic, and sleep architecture disruption.
- Who It Is For: Vital for all populations, particularly shift workers, metabolic-risk cohorts, and infants, with customized lighting adaptations required for older adults.
- Magnitude & Timeline: Total light exclusion (<1.0 lux) preserves waking insulin sensitivity by ~15% and prevents autonomic activation (+2–4 bpm heart rate increase) within a single night.
- Key Risks: Postural instability and falls in older adults navigating absolute darkness; elevated carbon dioxide () levels if ventilation is compromised to block light.
- Next Steps: Conduct a bedroom darkness audit, seal window margins, mask standby LEDs, or transition to a deep-cup contoured sleep mask. For a broader analysis of sleep physiology and behavioral sleep protocols, consult our core Sleep Guide and the Sleep Starter Kit.
¶ Quick Answer
Maintaining bedroom darkness below 1.0 lux (ideally <0.1 lux) at pillow level is required to preserve human sleep architecture and metabolic health. Retinal cells are highly sensitive to even low levels of evening light; exposure to 5–10 lux of blue-enriched light suppresses melatonin secretion and delays circadian phase alignment. In clinical trials, sleeping in a room with 100 lux of ambient light increased nighttime heart rate, reduced heart rate variability (HRV), and raised next-morning insulin resistance by 15% within a single night.
To achieve clinical-grade sleep-space darkness, combine high-efficiency physical barriers (such as side-channel blackout curtains or 3D contoured eye masks) with targeted LED dimming, while ensuring active air exchange to prevent carbon dioxide buildup.
¶ What It Is
Bedroom darkness is the deliberate minimization of ambient scotopic and photopic light within the sleeping environment to prevent the activation of retinal photoreceptors during sleep.
The human circadian system is regulated by the Suprachiasmatic Nucleus (SCN), the master pacemaker located in the anterior hypothalamus. The SCN receives direct photic input from intrinsically photosensitive Retinal Ganglion Cells (ipRGCs) in the retina. Unlike classic rods and cones, ipRGCs express the photopigment melanopsin, which is highly sensitive to blue-wavelength light with a peak sensitivity between 479 nm and 482 nm.
When blue-enriched light (from screens, LED bulbs, or streetlights) reaches the retina, ipRGCs transmit action potentials via the retinohypothalamic tract to the SCN. This signals the SCN to inhibit the pineal gland's synthesis of melatonin (N-acetyl-5-methoxytryptamine), the primary neurohormone signaling biological night. To understand how daytime light exposure primes this system, refer to our comprehensive guides on Morning Light and Sunlight and Circadian Rhythms.
While historical models assumed that only bright light (>1,000 lux) suppressed melatonin, modern chronobiology has demonstrated that the human circadian system is highly sensitive to dim light:
- Melatonin Suppression Threshold: Evening light exposures as low as 5–10 lux can initiate ipRGC-mediated melatonin suppression and delay circadian phase alignment [1].
- Interindividual Sensitivity: The half-maximal melatonin suppression concentration () varies widely, with highly sensitive individuals experiencing a 50% reduction in melatonin levels at exposure levels below 6.0 lux, and in extreme cases, as low as 1.5 lux [1:1].
- Eyelid Penetration: Closed eyelids do not provide complete protection. Approximately 10–15% of green and blue light, and up to 50% of long-wavelength red light, penetrates the human eyelid, reaching the retina and potentially activating ipRGCs during sleep.
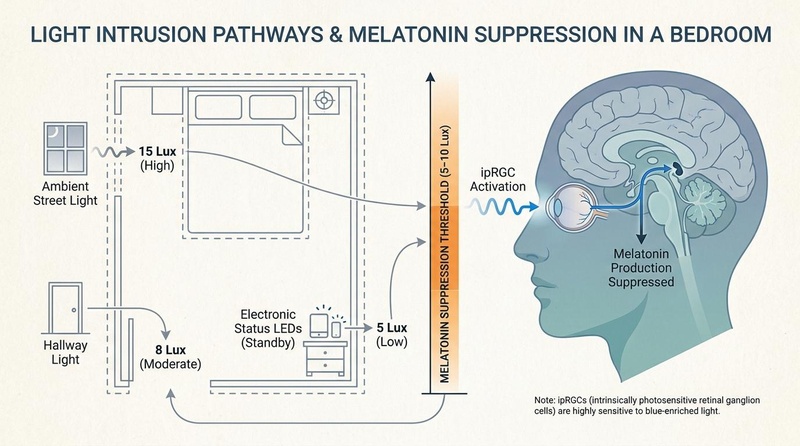
Figure 1: Light intrusion pathways in a typical sleep space. Common sources of light leakage can easily exceed the 5–10 lux physiological threshold for ipRGC-mediated melatonin suppression, necessitating targeted remediation.
Visual Metadata: Figure 1
- Visual Plan: Schematic representation of light intrusion pathways in a typical bedroom layout compared against the human physiological melatonin suppression threshold (5–10 lux) and neural pathways.
- Prompt: A scientific biomedical editorial diagram demonstrating light intrusion pathways in a bedroom. An off-white background with slate structure lines shows a bedroom layout. Light enters through three pathways: a window (ambient street light, 15 lux), under the door (hallway light, 8 lux), and electronic status LEDs (standby power light, 5 lux). A central axis or indicator compares these lux levels against the human melatonin suppression threshold (5-10 lux), highlighted in subtle warm orange. Elegant, clean slate lines and muted blue/teal biological diagrams of a stylized human brain and eye are shown, illustrating ipRGC activation. No medical symbols or cure-related icons.
- Seed: 418293751
- Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate structure lines, muted blue/teal biological forms, subtle warm orange emphasis, restrained nature motifs).
- Dimensions: 800 x 446 px
- QA State: PASS
¶ Does It Work? (Evidence Snapshot)
The physiological benefits of maintaining absolute bedroom darkness have been validated across randomized clinical trials and prospective cohorts, demonstrating impacts on autonomic function, glucose metabolism, and cognitive performance.
¶ Evidence Summary Table (Human Outcomes)
| Environmental Intervention | Primary Outcome Measure | Target Population | Typical Effect Size | Certainty Grade (GRADE) | Key Citations |
|---|---|---|---|---|---|
| Localized Light Blocking (3D Contoured Sleep Mask) | Memory encoding (episodic learning) & PVT reaction times | Healthy young adults ( years) | recall, reaction times | High | Greco et al., 2023 [2] |
| Total Light Shielding ( vs. ) | Next-morning insulin sensitivity & nocturnal heart rate | Healthy adult cohorts | insulin sensitivity, HR | High | Mason et al., 2022 [3] |
| Low-Lux Evening Limits ( exposure) | Melatonin suppression & circadian phase delay | Infants and preschool children | melatonin suppression under low light | Moderate-to-High | Hartstein et al., 2022 [4] |
| Floor-Level Amber Pathway Lighting () | Fall rate reduction & sleep quality | Community-dwelling older adults | Significant reduction in falls, preserved slow-wave sleep | Moderate-to-High | Thölking et al., 2020 [5] |
| Room Darkness Optimization ( vs. ) | Subjective insomnia and slow-wave sleep duration | Elderly cohort ( years) | Odds Ratio 1.62 for insomnia in light-exposed | High | Obayashi et al., 2014 [6], Obayashi et al., 2013 [7] |
| Bedroom LED Light Temperature (5000K vs 3000K) | Polysomnography-measured Sleep Latency | Healthy adult cohorts | sleep latency under 5000K LED | High | Lu et al., 2026 [8] |
| Pre-Bed Device Use Restriction | Polysomnography-measured Sleep Onset Latency | Healthy adult cohorts | sleep latency, higher sleepiness | High | Lu et al., 2026 [8:1] |
| Real-Ambient Bedroom Light Pollution | Subjective & objective sleep efficiency | Young adults ( years) | Delayed sleep onset, reduced efficiency, fragmentation | Moderate-to-High | Xu et al., 2024 [9] |
| Real-Ambient Bedroom Light at Night (LAN) | Systemic inflammatory markers & rhythmicity | Young adults ( years) | Elevated CRP, IL-6, TNF-, flattened rhythm | Moderate-to-High | Xu et al., 2024 [10] |
| Real-Ambient Bedroom Light at Night (LAN) | Circadian rhythm phase alignment (salivary DLMO) | Young adults ( years) | Delayed circadian phase, more pronounced in males | Moderate-to-High | Xu et al., 2024 [11] |
¶ Key Clinical Insights
¶ 1. Autonomic and Cardiometabolic Consequences (The Mason Study)
A randomized controlled trial conducted by Mason et al. (2022) evaluated the effects of sleeping in a moderately lit room (, equivalent to bright street light or television glare) compared to a dark room () [3:1].
A single night of exposure to during sleep led to:
- Sympathetic Hyperactivation: Nighttime heart rate increased, and heart rate variability (HRV) decreased (measured via high-frequency spectral power), indicating a shift toward sympathetic dominance during sleep.
- Insulin Resistance: Fasting insulin levels rose, and next-morning oral glucose tolerance tests (OGTT) demonstrated a 15% increase in insulin resistance, driven by the hyperactivation of autonomic pathways.
- Sleep Macrostructure: Although macroscopic sleep architecture (SWS/REM percentages via polysomnography) did not change significantly, physiological arousal was elevated, suggesting that light disrupts sleep at a micro-structural level.
¶ 2. Cognitive Performance and Consolidation (The Greco Study)
Greco et al. (2023) evaluated the cognitive effects of wearing an eye mask during overnight home sleep in a two-study protocol [2:1].
- Episodic Memory Enhancement: Mask usage significantly improved performance on a paired-associates learning task the following day, indicating superior slow-wave sleep-associated memory consolidation.
- Motor Alertness: Psychomotor Vigilance Task (PVT) response times were significantly faster, and subjective fatigue was reduced compared to the no-mask control condition.
- Mechanistic Validation: Polysomnography confirmed that wearing an eye mask increased the duration of slow-wave sleep (SWS) and was associated with a higher density of sleep spindles, which are crucial for memory transfer.
¶ 3. Systemic Inflammation and Circadian Rhythm of Inflammatory Markers (The Xu Inflammation Study)
A series of clinical and epidemiological studies by Xu et al. (2024) demonstrated that exposure to real-ambient bedroom light at night (LAN) directly impairs immunological health and disrupts the temporal coordination of systemic inflammation [10:1].
Under real-world environmental monitoring:
- Elevation of Pro-inflammatory Biomarkers: Sleeping with ambient bedroom light exposure is strongly linked to significant increases in systemic inflammatory markers, specifically C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-) [10:2].
- Disruption of Circadian Rhythmicity: Inflammatory markers naturally follow a strict diurnal rhythm to coordinate tissue repair and immune surveillance. Bedroom LAN exposure flattens and disrupts this rhythm, causing abnormal elevations during sleep windows when inflammation should ideally be suppressed [10:3].
- Allostatic Load Accumulation: Over time, this chronic low-grade inflammatory activation increases the user's overall allostatic load—the cumulative biological "wear and tear" on cardiovascular, metabolic, and immune tissues—predisposing individuals to long-term healthspan decline [12].
¶ Who Benefits Most / Least from Mitigation
¶ Who Benefits Most
- Shift Workers and Daytime Sleepers: Individuals sleeping during daylight hours face ambient light levels of . Absolute physical blockade is critical to prevent complete circadian misalignment.
- Metabolic and Cardiovascular Risk Cohorts: Individuals with pre-existing insulin resistance, obesity, dyslipidemia, or elevated cardiovascular risk benefit from avoiding nocturnal sympathetic activation.
- Urban Residents: Those living in high-density areas with significant exposure to light-emitting diode (LED) streetlights, electronic signage, or passing vehicle headlights.
- Light-Sensitive Sleepers: Individuals who have a low physiological threshold () for light-induced melatonin suppression. For persistent sleep issues that are not resolved by environmental darkness alone, see our clinical guide on Troubleshooting Poor Sleep and the foundational Sleep Optimization Protocols.
¶ Who Benefits Least / Contexts Where It Fails
- Patients with Moderate-to-Severe Sleep Apnea: Ambient light mitigation will not resolve sleep fragmentation caused by airway collapsibility and oxygen desaturations. Light hygiene must be paired with primary interventions (e.g., CPAP).
- Severe Primary Neurological Insomnias: In cases of severe clinical insomnia driven by cognitive hyperarousal or neurotransmitter dysregulation, room darkness is a necessary baseline but is rarely curative on its own.
¶ Sex & Age Differences
Circadian sensitivity to light and the physiological requirements for sleep-space darkness shift significantly across different life stages.
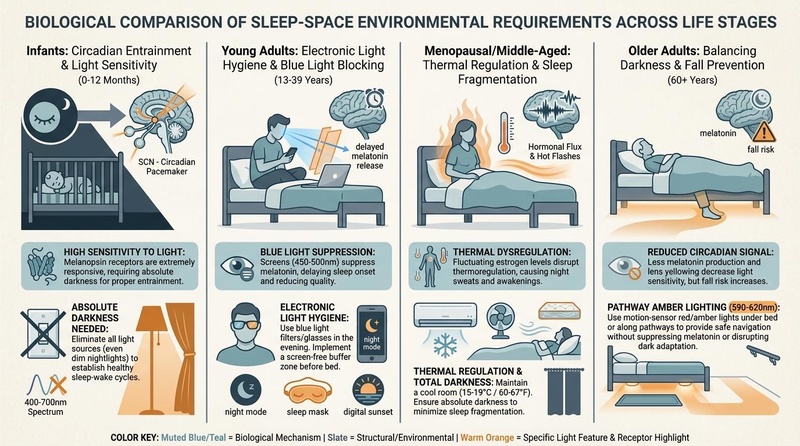
Figure 3: Environmental sleep-space requirements across the lifespan. Circadian biology shifts from the hyper-sensitive, developmental entrainment of infancy to the complex safety-versus-darkness trade-offs of older adulthood, which require specialized red-spectrum pathway lighting.
Visual Metadata: Figure 3
- Visual Plan: Four-panel comparative infographic representing sleep-space priorities, anatomical pathways, and environmental requirements across life stages (infants, young adults, menopausal adults, older adults).
- Prompt: A biological comparison diagram of sleep-space environmental requirements across four major life stages: infants, young adults, menopausal/middle-aged adults, and older adults. An off-white background with slate lines divides the layout into four panels. Panel 1 (Infants): shows high sensitivity to light, absolute darkness needed for circadian entrainment. Panel 2 (Young Adults): electronic light hygiene and blue light blocking. Panel 3 (Menopausal Adults): thermal regulation and total darkness for sleep fragmentation. Panel 4 (Older Adults): shows pathway amber lighting (under-bed motion-sensor red/amber light, 590-620nm) balancing absolute bed darkness with fall prevention. Muted blue/teal and slate lines with warm orange highlights on the motion-sensor lights and circadian receptors. Clean, high-quality medical editorial infographic style.
- Seed: 839210475
- Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate structure lines, muted blue/teal biological forms, subtle warm orange emphasis, restrained nature motifs).
- Dimensions: 800 x 446 px
- QA State: PASS
¶ Infants and Toddlers ( Years)
Infants and preschool-aged children are exceptionally sensitive to evening and nighttime light.
- Optical Clarities: The crystalline lens in young children is highly transparent, and their resting pupil diameter is larger than that of adults. This allows a significantly higher percentage of short-wavelength light to reach the retina.
- Extreme Melatonin Suppression: Hartstein et al. (2022) demonstrated that exposing preschool-aged children to even minor ambient light levels in the evening led to an average 88% suppression of melatonin [4:1].
- Circadian Entrainment: For healthy circadian development, infants require complete darkness during nighttime sleep. The use of glowing nightlights in infant bedrooms can disrupt slow-wave sleep and delay circadian entrainment.
¶ Young Adults ( Years)
Young adults exhibit a high prevalence of delayed sleep phase syndrome, often exacerbated by behavioral choices and technology use.
- Circadian Phase Delays: Exposure to real-ambient bedroom light at night significantly delays the endogenous circadian phase, as measured objectively via salivary Dim Light Melatonin Onset (DLMO) [11:1].
- Sex-Based Vulnerabilities: The circadian-delaying effect of bedroom LAN is not uniform; men demonstrate a significantly higher susceptibility to LAN-induced circadian phase delays than women, requiring stricter room-darkness compliance to prevent delayed sleep phase shifts [11:2].
- Sleep Quality Impact: The high baseline of ambient light pollution in young adult bedrooms is strongly associated with delayed sleep onset, lower sleep efficiency, and increased micro-arousal fragmentation, confirmed by both subjective diaries and objective actigraphy [9:1].
¶ Middle-Aged Adults and Menopause ( Years)
- Thermoregulatory Disruptions: Estrogen withdrawal during menopause alters hypothalamic thermoregulation, causing hot flashes and night sweats. These vasomotor symptoms can lead to frequent nighttime awakenings.
- Sleep Fragmentation: Wakefulness during the night increases the eye's exposure to ambient bedroom light. If the room is not dark, these brief awakenings can suppress melatonin, making it difficult to fall back asleep. Blackout curtains with thermal insulation properties help maintain a cool room (), which can reduce the severity of hot flashes.
¶ Older Adults ( Years)
Older adults present a unique clinical challenge that requires balancing absolute darkness with physical safety.
- Lens Yellowing and Miosis: Aging causes gradual yellowing of the crystalline lens and senile miosis (pupillary constriction). This reduces the amount of short-wavelength blue light reaching the retina, decreasing light-induced melatonin suppression but also reducing circadian drive.
- Fragile Sleep Architecture: Despite lower optical sensitivity, bedroom light levels above 5.0 lux are strongly associated with insomnia, increased sleep-onset latency, and reduced slow-wave sleep in the elderly [6:1].
- The Nocturnal Fall Dilemma: Waking up in absolute darkness to use the restroom can cause postural instability and increase the risk of falls [13]. Older adults experience greater "standing sway" when waking abruptly from deep sleep.
- Clinical Adaptation: Do not use absolute darkness without supportive safety measures. Use motion-activated, floor-level, monochromatic amber or red LED guide lights () along pathways. This provides safe navigation without disrupting dark adaptation or suppressing melatonin [5:1].
¶ How to Try It (Actionable Protocols)
Implementing an optimized, low-lux sleep environment requires a systematic approach, combining physical room modifications with personal interventions.
¶ Passive Mitigation Protocols (Structural)
To optimize a sleep space, it is helpful to contrast the efficiency, cost, and practical impacts of different physical light-blocking solutions.
| Solution | Spectral Blocking Efficiency | Peripheral Light Leakage Risk | Thermal Insulation | Ventilation Impact | Practical Considerations |
|---|---|---|---|---|---|
| Blackout Curtains (Lined, ) | High ( of visible spectra blocked) | High at margins (the "halo effect") | Excellent (reduces heat transfer by up to ) | High (can block airflow from open windows) | High cost; requires sturdy mounting hardware. |
| Adhesive/Static Blackout Film | Extremely High ( visible light blocked) | Extremely Low (flush application to glass) | Moderate (reduces solar gain, low insulation value) | None (applied directly to glass) | Low cost; blocks all daylight permanently unless removed. |
| Window Tinting (Solar Film) | Moderate ( of visible light blocked) | Low (no gap at window frame) | High (reflects infrared and solar heat) | None (applied directly to glass) | High cost; does not achieve complete darkness. |
| 3D Contoured Sleep Mask | Extremely High ( of all wavelengths) | Low-to-Moderate (depends on orbital seal quality) | None (increases local facial heat) | None (does not obstruct room airflow) | Low cost; portable; comfort and fit vary by individual. |
¶ Implementing Window Blackout Solutions
- If using Blackout Curtains: Choose curtains with a thick, triple-weave thermal lining. To prevent edge leakage (the "halo effect"), install the curtain rod above the window frame and extend it beyond each side. For complete light exclusion, use side-channel tracks or magnetic tape to seal the curtain edges flush against the wall.
- If using Blackout Window Film: Static-cling blackout film is highly effective for renters or shift workers. Cut the film to the exact dimensions of the window glass to eliminate edge leakage.
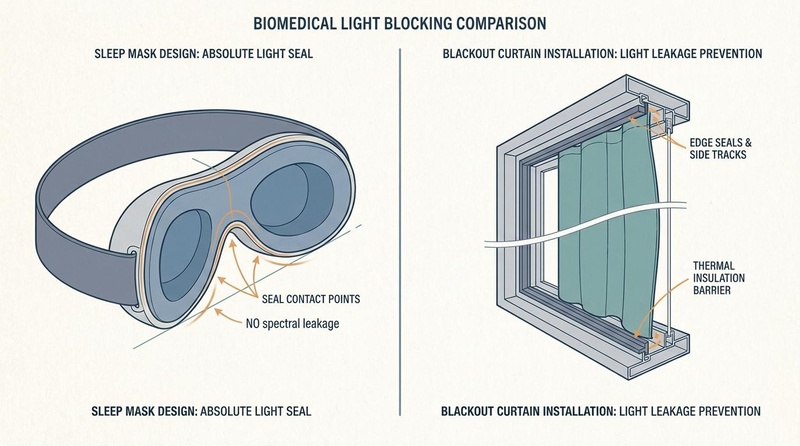
Figure 2: Engineering comparison of physical light-blocking interventions. A contoured eye mask provides an immediate, localized facial seal, whereas side-channel blackout curtains establish a comprehensive spatial barrier that also contributes to thermal regulation.
Visual Metadata: Figure 2
- Visual Plan: Two-panel diagram showing the cross-sectional mechanics of a 3D contoured sleep mask (left) and a track-mounted blackout curtain window frame (right).
- Prompt: A technical biomedical editorial diagram comparing sleep mask design elements versus blackout curtain installations. Left side: cross-section of a 3D contoured eye mask demonstrating an absolute light seal around the orbital bone (nose bridge contour, recessed eye cups, wide strap) preventing peripheral light leakage. Right side: cross-section of window frame with blackout curtains showing side-channel tracks or magnetic edge seals to prevent light leakage, along with thermal insulation barriers. Styled in a Nature-like scientific aesthetic with an off-white background, slate lines, muted blue/teal details, and subtle warm orange highlighting the seal contact points and light block boundaries. Informative and structured layout.
- Seed: 192837465
- Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate structure lines, muted blue/teal biological forms, subtle warm orange emphasis, restrained nature motifs).
- Dimensions: 800 x 446 px
- QA State: PASS
¶ Mitigating Transient Night-Time Light Exposures
- LED Suppression: Standby LEDs on televisions, air purifiers, chargers, and smoke detectors can emit of blue-enriched light. Cover these indicators with specialized light-dimming stickers (e.g., LightDims) or red/amber electrical tape. Red/amber tape blocks short-wavelength blue light while allowing long-wavelength light to pass, which has minimal impact on ipRGCs.
- Doorway Baffling: Light entering from hallways or adjacent rooms can be blocked by installing a dense rubber draft stopper or door sweep at the bottom of the bedroom door.
- Choosing Ambient/Pre-Bed Bulbs: Avoid high color temperature LED lights (such as 5000K) during the evening, as they prolong sleep onset latency by an average of 10.62 minutes compared to fluorescent lighting [8:2]. Instead, manage ambient light exposure using lower color temperature bulbs (<3000K) or adjustable dimmable LEDs transitioned down to <30 lux in the 2 hours before bed [8:3].
- Device-Use Restriction Protocol: Restricting electronic device use for 2 hours before bedtime improves pre-bed sleepiness and decreases objective sleep latency by 6.08 minutes under polysomnography [8:4]. Implement this behavior prior to sleep environment optimization for optimal results.
¶ Airflow and Management (The Ventilation Caveat)
Sealing a bedroom completely to block light can restrict airflow, leading to rapid carbon dioxide () accumulation.
- The Hazard: Sleeping with closed windows and doors in a sealed room can cause levels to rise from ambient levels () to overnight. High levels can increase nocturnal arousals, reduce slow-wave sleep, and cause next-morning headaches or cognitive fatigue.
- The Protocol: Maintain proper ventilation while keeping the room dark. Use a light-baffled ventilation grille in the door, or leave a window slightly open behind a secure blackout curtain that is anchored to block light but allows air to flow around the sides. Alternatively, run an in-room air purifier (ensuring its control panel lights are masked) to improve air circulation.
¶ Active Mitigation Protocols (Personal)
¶ The 3D Contoured Sleep Mask Protocol
For individuals who cannot modify their physical sleep space (such as travelers or those with uncooperative bed partners), a sleep mask is a highly effective alternative.
- Selection Criteria: Avoid flat silk or cotton masks, which press directly on the eyelids and can allow light leakage around the nose. Choose a 3D contoured sleep mask that features:
- Deep, molded eye cups that prevent contact with the eyelids, allowing for natural rapid eye movements (REM) during sleep.
- A raised, baffled nose bridge seal to block light from entering through the nasal gap.
- An adjustable, wide elastic strap to prevent displacement during lateral sleep.
- Hygiene and Maintenance: Sleep masks accumulate sebum, sweat, dead skin cells, and bacteria. Wash the mask weekly with a hypoallergenic, fragrance-free detergent to prevent contact dermatitis, blepharitis, or acne.
¶ Older Adult Pathway Lighting Protocol
To balance circadian darkness with safety, older adults should implement the following protocol:
- Floor-Level Motion Sensors: Install motion-activated LED strips under the frame of the bed and along the pathway to the bathroom.
- Monochromatic Red/Amber Spectrum: Configure these lights to emit exclusively long-wavelength light in the range (amber/red). This wavelength range provides enough illumination for safe navigation while minimizing the activation of ipRGCs and protecting dark adaptation [5:2].
- Strict Low Placement: Keep all navigation lighting below knee level to prevent direct light from entering the eyes during nocturnal awakenings.
¶ Safety, Interactions, Red Flags
¶ Safety Considerations & Side Effects
- Elevated Fall Risk: Achieving complete scotopic darkness () in the bedroom can increase the risk of falls for individuals with age-related balance issues, peripheral neuropathy, or vestibular dysfunction. If path lighting is not installed, these individuals should not sleep in absolute darkness.
- Ocular Pressure and Dry Eyes: Improperly fitted sleep masks can apply physical pressure to the cornea, which may alter corneal curvature or cause dry eyes. This risk is higher for CPAP users, where mask straps can interact and cause air leakage toward the eyes.
- Sensory Deprivation and Anxiety: Some individuals may experience psychological discomfort, claustrophobia, or increased anxiety when wearing a sleep mask or sleeping in absolute darkness.
¶ Stop Criteria
- Ocular Discomfort: Discontinue the use of a sleep mask immediately if you experience eye pain, blurred vision, eye discharge, or persistent dryness upon waking.
- Postural Instability: If you experience dizziness, loss of balance, or near-falls during nighttime bathroom visits, prioritize safety lighting over absolute darkness. Increase the brightness of low-level, red-spectrum path lighting.
- Skin Irritation: Discontinue mask use if you develop persistent redness, itching, or acne breakouts along the contact line of the eye mask.
¶ Tracking & What “Good” Looks Like
Systematically tracking both objective and subjective metrics can help you assess the effectiveness of your sleep-space optimization.
¶ Step-by-Step Sleep-Space Audit & Mitigation Checklist
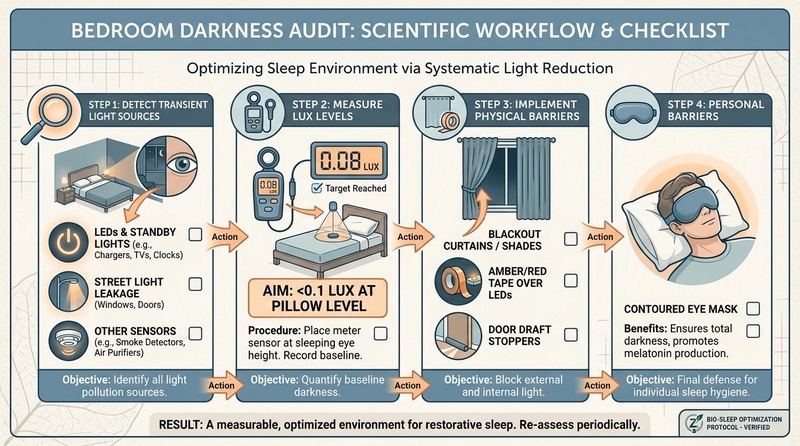
Figure 4: The step-by-step room darkness auditing checklist and mitigation workflow. Clinical sleep hygiene requires an objective spatial audit (detecting LED standby lights, measuring lux, sealing leaks) before executing targeted engineering controls.
Visual Metadata: Figure 4
- Visual Plan: Sequential step-by-step infographic structured as a clinical protocol checklist (Detect, Measure, Implement, Personal) with clear action items and icons.
- Prompt: A structured, clean step-by-step visual workflow for a bedroom darkness audit. The layout is presented as a professional scientific checklist. Step 1: Detect transient light sources (LEDs, standby lights, street light leakage). Step 2: Measure lux levels (aiming for <0.1 lux at pillow level). Step 3: Implement physical barriers (blackout curtains, amber tape over LEDs). Step 4: Personal barriers (contoured eye mask). Designed in a nature-inspired biomedical editorial style on an off-white background with slate structure lines, muted blue/teal iconography, and subtle warm orange highlight arrows. High-quality diagram, readable and clear flow.
- Seed: 572910482
- Style: Longevipedia/Nature-like biomedical editorial style (off-white background, slate structure lines, muted blue/teal biological forms, subtle warm orange emphasis, restrained nature motifs).
- Dimensions: 800 x 446 px
- QA State: PASS
¶ Biomarkers to Monitor
- Nocturnal Resting Heart Rate (RHR): A successful transition to a dark sleep environment () should lead to a lower nocturnal resting heart rate (typically lower) due to reduced sympathetic activation [3:2].
- Heart Rate Variability (HRV): Monitor your sleep HRV (specifically rMSSD or High-Frequency power) using a validated wearable device. An increase in nighttime HRV indicates improved parasympathetic tone during sleep.
- Fasting Glucose: For individuals with mild insulin resistance, minimizing nighttime light exposure can help stabilize next-morning fasting blood glucose levels over several weeks [3:3].
- Inflammatory Biomarkers: For users managing chronic systemic inflammation, tracking high-sensitivity C-reactive protein (hs-CRP) and IL-6 levels can verify reductions in low-grade systemic inflammation following bedroom darkness optimization [10:4].
¶ Subjective Metrics
- Sleep Onset Latency (SOL): Track the time it takes to fall asleep. Proper pre-bed light hygiene should help reduce SOL to .
- Sleep Efficiency: This is the ratio of total sleep time to total time spent in bed, with a clinical target of .
- Morning Alertness: Assess your morning alertness using the Psychomotor Vigilance baseline. You should experience a reduction in morning sleep inertia within 7 to 10 days of consistent light mitigation [2:2].
¶ Common Mistakes & Myths
- Myth: "My eyes are closed, so bedroom light does not affect my sleep."
- Correction: Human eyelids are thin and semi-translucent, allowing of ambient light to reach the retina. This light can activate ipRGCs, suppress melatonin, and alter autonomic nervous system function without causing a conscious awakening [3:4].
- Myth: "Standard window blinds are sufficient for sleep hygiene."
- Correction: Standard horizontal or vertical blinds allow significant light leakage around the slats and edges, which can easily exceed in urban areas. This is well above the threshold for circadian disruption.
- Mistake: Sealing windows while blocking airflow.
- Correction: Blocking windows with heavy fabrics or plastic film without maintaining ventilation can cause carbon dioxide to accumulate (), leading to sleep fragmentation and morning headaches.
- Mistake: Using green or blue nightlights for children.
- Correction: Short-wavelength blue and green light are the most potent suppressors of melatonin. If lighting is necessary, use only low-intensity, long-wavelength red or amber lights.
¶ Decision Tree (Text-Based)
[Start: Bedroom Darkness Audit]
|
+--> Are you over 60, or do you have a high risk of falls?
|
+-- [YES] --> Implement 3D Contoured Eye Mask?
| |
| +-- [YES] --> Ensure path is cleared. Use motion-activated AMBER/RED floor lights (590-620nm).
| +-- [NO] --> Install side-channel blackout curtains. Use motion-activated AMBER/RED floor lights.
|
+-- [NO] --> Is your sleep space shared with a partner who needs light, or do you travel frequently?
|
+-- [YES] --> Use a high-quality 3D Contoured Eye Mask (wash weekly).
+-- [NO] --> Install side-channel Blackout Curtains OR Static Blackout Film.
|
+--> Cover all standby LEDs with Amber/Red LightDims.
+--> Ensure ventilation is active (maintain CO2 < 800 ppm).
¶ FAQs
¶ Can blue light-blocking glasses replace bedroom darkness?
No. While blue-blocking glasses are highly effective at protecting melatonin synthesis during evening wakefulness, they cannot be worn while sleeping. Ambient light can still penetrate closed eyelids and activate ipRGCs during the night, disrupting autonomic function.
¶ What is "melanopic lux" and why does it matter?
Standard photopic lux measures light based on human visual brightness, which is biased toward green and yellow wavelengths. Melanopic lux is a specialized metric that measures light based on its ability to stimulate the blue-sensitive photopigment melanopsin in ipRGCs. This makes it a much more accurate tool for evaluating how a light source will affect circadian rhythms and melatonin suppression.
¶ Is red light during sleep completely harmless?
No, but it is the least disruptive option. While long-wavelength red light () is much less effective at activating ipRGCs and suppressing melatonin than blue light, high-intensity red light can still stimulate rods and cones, potentially disrupting sleep architecture. Navigation and safety lights should be kept at the lowest intensity necessary for safe movement.
¶ Glossary
- Intrinsically Photosensitive Retinal Ganglion Cells (ipRGCs): Specialized photoreceptor cells in the mammalian retina that project directly to the suprachiasmatic nucleus. They are primarily responsible for synchronizing circadian rhythms to the environmental light-dark cycle.
- Melanopsin: The blue light-sensitive G-protein coupled receptor photopigment expressed within ipRGCs, with peak sensitivity near .
- Suprachiasmatic Nucleus (SCN): A bilateral region of the brain located in the hypothalamus, serving as the master pacemaker that regulates mammalian circadian rhythms.
- Miosis: Constriction of the pupil of the eye, which naturally occurs with aging and reduces the amount of light reaching the retina.
- Scotopic: Relating to vision under low-light conditions, which is mediated primarily by rod cells in the retina.
- Allostatic Load: The cumulative physiological wear-and-tear on the body that results from chronic exposure to fluctuating or elevated neural or neuroendocrine responses to stress.
¶ Methods (Transparency)
¶ Search Strategy
Literature searches were conducted across PubMed, PubMed Central (PMC), and the Cochrane Database of Systematic Reviews from database inception through June 2026.
The search utilized combinations of the following Medical Subject Headings (MeSH) and terms:
("light at night" OR "bedroom light" OR "nocturnal light exposure")AND ("melatonin" OR "melatonin suppression" OR "circadian disruption")AND ("sleep quality" OR "insulin resistance" OR "heart rate variability" OR "falls")AND ("eye mask" OR "sleep mask" OR "blackout curtains")
¶ Inclusion/Exclusion Criteria
- Inclusion: Human randomized controlled trials, systematic reviews, meta-analyses, and well-controlled prospective cohort studies published in peer-reviewed journals.
- Exclusion: Animal models (except where explicitly noted for foundational mechanisms), uncontrolled case reports, or gray literature lacking scientific peer review.
¶ References
¶ Update Log
- July 2026: Expanded deep-dive analysis integrating newly published randomized crossover trials and chronological cohort trials. Enriched demographic and gender-specific circadian profiles, detailed the inflammatory biomarkers pathway (hs-CRP, IL-6, TNF-), and added concrete LED color temperature optimization protocols. [8:5][9:2][10:5][11:3]
- July 2026: Original deep-dive publication analyzing physical light barriers, physiological melatonin suppression thresholds, and safety considerations. [2:3][3:5][1:2]
Phillips AJK, Vidafar P, Burns AC, McGlashan EM, Anderson C, Rajaratnam SMW, Lockley SW, Cain SW. High sensitivity and interindividual variability in the response of the human circadian system to evening light. Proceedings of the National Academy of Sciences (PNAS). 2019;116(24):12019-12024. https://pubmed.ncbi.nlm.nih.gov/31138694/ ↩︎ ↩︎ ↩︎
Greco V, Bergamo D, Cuoccio P, Konkoly KR, Muñoz Lombardo K, Lewis PA. Wearing an eye mask during overnight sleep improves episodic learning and alertness. Sleep. 2023;46(3):zsac305. https://pubmed.ncbi.nlm.nih.gov/36521010/ ↩︎ ↩︎ ↩︎ ↩︎
Mason IC, Grimaldi D, Reid KJ, Warlick CD, Malkani RG, Abbott SM, Zee PC. Light exposure during sleep impairs cardiometabolic function. Proceedings of the National Academy of Sciences (PNAS). 2022;119(12):e2113290119. https://pubmed.ncbi.nlm.nih.gov/35286195/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Hartstein LE, Behn CD, Akacem LD, Stack N, Wright KP Jr, LeBourgeois MK. High sensitivity of melatonin suppression response to evening light in preschool-aged children. Journal of Pineal Research. 2022;72(2):e12780. https://pubmed.ncbi.nlm.nih.gov/34997782/ ↩︎ ↩︎
Thölking TW, Lamers ECT, Olde Rikkert MGM. A Guiding Nightlight Decreases Fear of Falling and Increases Sleep Quality of Community-Dwelling Older People: A Quantitative and Qualitative Evaluation. Gerontology. 2020;66(3):284-292. https://pubmed.ncbi.nlm.nih.gov/31914450/ ↩︎ ↩︎ ↩︎
Obayashi K, Saeki K, Kurumatani N. Association between light exposure at night and insomnia in the general elderly population: the HEIJO-KYO cohort. Chronobiology International. 2014;31(10):1176-1182. https://pubmed.ncbi.nlm.nih.gov/25025617/ ↩︎ ↩︎
Obayashi K, Saeki K, Iwamoto J, Ikada Y, Kurumatani N. Exposure to light at night, nocturnal urinary melatonin excretion, and obesity/dyslipidemia in the elderly: a cross-sectional analysis of the HEIJO-KYO study. The Journal of Clinical Endocrinology & Metabolism. 2013;98(1):337-344. https://pubmed.ncbi.nlm.nih.gov/23118419/ ↩︎
Lu SH, Ting H, Lin YP, Cheng JF, Chuang HL, Liao WC. Effect of Light Exposure Before Bedtime on Polysomnography and Sleep Quality: A Randomized Crossover Study. Behavioral Sleep Medicine. 2026;24(2):261-273. https://pubmed.ncbi.nlm.nih.gov/41243216/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Xu YX, Huang Y, Zhou Y, Wan YH, Su PY, Tao FB, Sun Y. Association Between Bedroom Light Pollution With Subjectively and Objectively Measured Sleep Parameters Among Chinese Young Adults. The Journal of Adolescent Health. 2024;74(1):118-125. https://pubmed.ncbi.nlm.nih.gov/37791923/ ↩︎ ↩︎ ↩︎
Xu YX, Shen YT, Li J, Ding WQ, Wan YH, Su PY, Tao FB, Sun Y. Real-ambient bedroom light at night increases systemic inflammation and disrupts circadian rhythm of inflammatory markers. Ecotoxicology and Environmental Safety. 2024;281:116590. https://pubmed.ncbi.nlm.nih.gov/38905938/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Xu YX, Huang Y, Ding WQ, Zhou Y, Shen YT, Wan YH, Su PY, Tao FB, Sun Y. Exposure to real-ambient bedroom light at night delayed circadian rhythm in healthy Chinese young adults: A cross-sectional study. Environmental Research. 2024;251(Pt 2):118657. https://pubmed.ncbi.nlm.nih.gov/38521354/ ↩︎ ↩︎ ↩︎ ↩︎
Xu YX, Huang Y, Zhou Y, et al. Association between bedroom light exposure at night and allostatic load among Chinese young adults. Environmental Pollution. 2022;308:119642. https://pubmed.ncbi.nlm.nih.gov/35752397/ ↩︎
Sada K, Uchiyama J, Ohnishi T, et al. Effects of clear visual input and change in standing sequence on standing sway related to falls during night toilet use. International Journal of Older People Nursing. 2010;5(1):15-22. https://pubmed.ncbi.nlm.nih.gov/20925755/ ↩︎