¶ Diarrhea
| Condition Class | Functional / Organic Bowel Disorder |
| Primary Types | Osmotic, Secretory, Inflammatory, Fatty (Steatorrhea) |
| Diagnostic Standard | AGA Laboratory Evaluation Guidelines [^1] |
| Key Bio-Markers | Fecal Calprotectin, Fecal Elastase, C4 / SeHCAT [^1][^3] |
| First-Line Therapy | WHO Oral Rehydration, Loperamide, Soluble Fiber [^1][^4] |
| Prevalence | 3–5% of the global adult population (chronic) |
Chronic diarrhea—defined as the passage of three or more loose or watery stools (Bristol Stool Form Scale Type 6 or 7) per day lasting for more than four weeks—is a frequent and challenging gastrointestinal presentation. It represents a fundamental failure of intestinal fluid homeostasis, where the complex balance of fluid absorption and secretion is disrupted by osmotic gradients, active secretory pathways, mucosal inflammation, or hypermotility.
Optimizing chronic diarrhea outcomes requires moving beyond symptomatic suppression to execute systematic, etiology-specific clinical triage.
¶ TL;DR
- Fluid Balance is Highly Precise: The human gut processes approximately 9 liters of fluid daily; a decrease of just 1% in colonic fluid absorption is sufficient to induce watery diarrhea.
- Osmotic vs. Secretory Differentiation: Osmotic diarrhea resolves with fasting () and exhibits a high fecal osmotic gap (). Secretory diarrhea persists during fasting and has a low gap () [1][2].
- Bile Acid Diarrhea is Highly Underdiagnosed: Up to 30% of patients diagnosed with IBS-D or functional diarrhea actually suffer from Bile Acid Malabsorption (BAM). This responds exceptionally well to bile acid sequestrants like colesevelam or cholestyramine [3][4].
- Avoid Empirical Antibiotic Use: Empirical antibiotic therapy for undifferentiated chronic diarrhea is strongly discouraged. It destroys the native commensal microbiota, worsens underlying gut dysbiosis, and elevates the risk of Clostridioides difficile [5].
- Screen for Microscopic Colitis: In postmenopausal females presenting with sudden-onset, voluminous watery diarrhea, prioritize colonoscopy with random mucosal biopsies to rule out lymphocytic or collagenous colitis [6][7].
¶ Quick Answer
The clinical evaluation of chronic diarrhea requires distinguishing between osmotic, secretory, inflammatory, and fatty/malabsorptive etiologies. Under the American Gastroenterological Association (AGA) clinical guidelines, initial screening must utilize high-yield fecal biomarkers (fecal calprotectin, fecal elastase, and fecal osmotic gap) alongside serological testing (celiac tTG-IgA) to rule out organic disease [1:1][8]. While osmotic diarrhea (e.g., lactose malabsorption) is managed via dietary elimination, secretory diarrhea requires identifying the driving mechanism (e.g., microscopic colitis, bile acid malabsorption, or neuroendocrine tumors).
Notably, Bile Acid Diarrhea (BAD) is a major, highly treatable cause of chronic secretory-like diarrhea [3:1]. It is diagnosed via C4 (7-alpha-hydroxy-4-cholesten-3-one) or fecal bile acid assays and treated with bile acid sequestrants, which bind irritating dihydroxy bile acids in the colonic lumen [4:1].
¶ What It Is
Chronic diarrhea is classified under the Rome IV criteria as Functional Diarrhea when patients present with loose or watery stools (BSFS Type 6 or 7) in the absence of abdominal pain or bloating as predominant symptoms for at least three months. However, chronic diarrhea is frequently organic, requiring the clinical exclusion of celiac disease, inflammatory bowel disease (IBD), microscopic colitis, and malabsorptive disorders (via fecal elastase) [9].
¶ Pathophysiological Mechanisms
The fluid dynamics of the gut are governed by four distinct pathophysiological patterns:
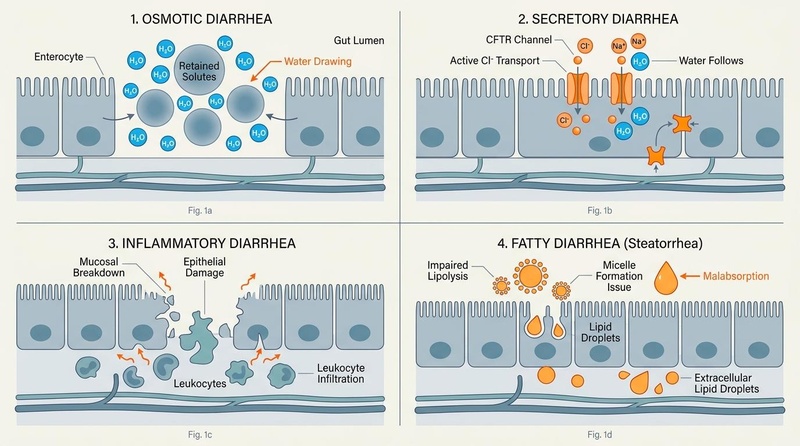
- Osmotic Diarrhea: Driven by the presence of unabsorbed, water-soluble, low-molecular-weight solutes in the intestinal lumen [2:1]. These solutes create an osmotic gradient that draws water out of the extracellular fluid and bloodstream across the mucosal barrier into the lumen. Common causes include magnesium ingestion, lactose intolerance, and sugar alcohol consumption (sorbitol, mannitol, xylitol) [2:2][10].
- Secretory Diarrhea: Driven by active, stimulated mucosal secretion of anions—principally chloride ions () via cystic fibrosis transmembrane conductance regulator (CFTR) channels—which secondarily draws sodium () and water into the lumen. Unlike osmotic diarrhea, secretory diarrhea is voluminous, persists during fasting, and is associated with a low fecal osmotic gap () [1:2][8:1].
- Inflammatory / Exudative Diarrhea: Driven by structural damage to the mucosal lining (due to IBD, microscopic colitis, or invasive infections), resulting in the leakage of mucus, blood, and inflammatory proteins into the lumen, combined with impaired absorption of fluids and electrolytes [1:3][7:1].
- Fatty Diarrhea (Steatorrhea): Characterized by impaired lipolysis or defective micelle formation in the intestinal lumen [9:1]. This leads to unabsorbed fat content in the feces, which presents as pale, voluminous, foul-smelling, and greasy stools that float and are difficult to flush. Common drivers include Exocrine Pancreatic Insufficiency (EPI) and extensive small bowel mucosal damage (e.g., celiac disease) [9:2][11].
¶ Does It Work? (Evidence Snapshot)
The efficacy of various therapeutic interventions for chronic diarrhea is well-established across clinical guidelines and randomized trials.
¶ Primary Interventions for Chronic Diarrhea
| Intervention | Intended Etiology | Outcome Measure | Expected Clinical Effect Size | Evidence Quality (GRADE) | Supported Study Count |
|---|---|---|---|---|---|
| Loperamide | Functional Diarrhea / IBS-D | Reduction in stool frequency | Significant increase in transit time, reduction in daily stool volume [1:4][8:2] | High | >15 RCTs |
| Cholestyramine / Colesevelam | Bile Acid Diarrhea (BAD) | Stool consistency & frequency | 70–80% response rate (rapid normalization of bowel habits) [3:2][4:2] | High | >10 RCTs, Systematic Reviews |
| Budesonide (Oral, M/R) | Microscopic Colitis | Clinical and histological remission | Up to 80% clinical remission rate, massive mucosal recovery [12][7:2] | High | Multiple Phase-III RCTs |
| Low-FODMAP Diet | IBS-D / Functional Diarrhea | Global symptom scores | 50–60% reduction in stool loose-form frequency [13][10:1] | Moderate | >20 RCTs |
| Pancreatic Enzyme (PERT) | Exocrine Pancreatic Insufficiency (EPI) | Fat absorption / Steatorrhea | Marked reduction in fecal fat output and stool frequency [11:1] | High | Multiple RCTs |
| Berberine | Secretory / Functional Diarrhea | Inhibition of mucosal secretion | Direct blockage of CFTR and CaCC channels, reducing fluid output [14] | Moderate | >10 RCTs |
| Rifaximin | IBS-D / SIBO-induced Diarrhea | Stool consistency & abdominal pain | 40–45% sustained clinical relief post-treatment [15][16] | Moderate | 3 Phase-III RCTs |
| Saccharomyces boulardii | Dysbiosis / Secretory Diarrhea | Enterotoxin degradation | Prevention of mucosal fluid loss, accelerated tight junction repair [2:3] | Moderate | >15 RCTs |
¶ Who Benefits Most / Least
¶ Sex, Age, and Subgroup Variations
- Postmenopausal Females: Postmenopausal females exhibit a 5-fold higher incidence of microscopic colitis (collagenous and lymphocytic colitis) compared to the general population [6:1][7:3]. It presents as sudden-onset, painless, voluminous watery diarrhea and is frequently misdiagnosed as functional diarrhea or IBS-D. These patients benefit rapidly and profoundly from low-dose oral budesonide induction therapy [6:2][7:4].
- Older Adults: Older adults are highly susceptible to catastrophic complications of diarrhea, including severe dehydration, acute kidney injury (AKI), and profound electrolyte derangements (hypokalemia, hypomagnesemia). They show lower tolerance to high-dose antimotility agents (which can induce fecal impaction or urinary retention due to anticholinergic overlap) and require immediate hydration-first protocols. Older adults also have a higher prevalence of subclinical Exocrine Pancreatic Insufficiency (EPI) and drug-induced diarrhea [15:1][11:2].
- Patients with Ileal Resection / Cholecystectomy: Up to 30–50% of patients who undergo gallbladder removal (cholecystectomy) or terminal ileal resection experience persistent Bile Acid Diarrhea due to unregulated hepatic bile acid secretion or loss of apical sodium-dependent bile acid transporters (ASBT) [3:3][4:3]. They are highly responsive to bile acid sequestrants [4:4].
- Young Adults: Frequently present with functional diarrhea or IBS-D related to dietary carbohydrate malabsorption, high caffeine intake, or autonomic stress responses. They benefit significantly from dietary restriction (Low-FODMAP) [13:1][10:2], soluble fiber bulking, and stress mitigation, while rarely requiring aggressive pharmacological interventions [15:2].
¶ Detailed Clinical Etiologies & Differential Diagnosis
To accurately treat chronic diarrhea, the clinician must differentiate between organic and functional drivers.
¶ 1. Bile Acid Malabsorption (BAM) / Bile Acid Diarrhea (BAD)
Bile acid diarrhea is a major cause of chronic watery diarrhea, accounting for up to 30% of cases classified as diarrhea-predominant irritable bowel syndrome (IBS-D) or functional diarrhea [3:4]. Normally, of bile acids are reabsorbed in the terminal ileum via the Apical Sodium-Dependent Bile Acid Transporter (ASBT) and recycled back to the liver [4:5][17].
When reabsorption is impaired, excess bile acids spill into the colon. In the colonic lumen, dihydroxy bile acids (chenodeoxycholic acid and deoxycholic acid) stimulate cAMP-dependent CFTR chloride channels, inducing active fluid secretion and accelerating colonic motility [4:6].
BAM is classified into three distinct clinical types [4:7][16:1]:
- Type 1: Secondary to ileal resection, terminal ileitis (e.g., Crohn's disease), or bypass [16:2].
- Type 2: Idiopathic or primary bile acid diarrhea, characterized by normal ileal anatomy but decreased production of the negative feedback hormone Fibroblast Growth Factor 19 (FGF19) by enterocytes, leading to uncontrolled hepatic bile acid synthesis [18][17:1].
- Type 3: Associated with other gastrointestinal conditions, including post-cholecystectomy, SIBO (where bacterial deconjugation prevents reabsorption), celiac disease, or chronic pancreatitis [3:5][4:8].
 in the terminal ileum and the binding action of polymeric bile acid sequestrants in the colon.")
¶ 2. Microscopic Colitis
Microscopic colitis is a chronic inflammatory bowel disease characterized by chronic, watery, non-bloody diarrhea [6:3]. The endoscopic appearance of the colon is completely normal; diagnosis can only be made via histological examination of random mucosal biopsies taken during colonoscopy [7:5]. It is subclassified into:
- Collagenous Colitis: Distinguished by a thick subepithelial collagen band () beneath the surface epithelium [6:4].
- Lymphocytic Colitis: Distinguished by an increased number of intraepithelial lymphocytes ( lymphocytes per 100 epithelial cells) with no collagen deposition [6:5].
The disease is highly associated with autoimmune disorders and is triggered or exacerbated by medications, including Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), Proton Pump Inhibitors (PPIs), selective serotonin reuptake inhibitors (SSRIs), and checkpoint inhibitors [6:6][7:6].
¶ 3. Celiac Disease
Celiac disease is a systemic, immune-mediated enteropathy triggered by dietary gluten in genetically susceptible individuals (HLA-DQ2/DQ8 positive) [18:1]. The immune response triggers intraepithelial lymphocytosis, crypt hyperplasia, and progressive villous atrophy in the duodenum, causing a combined secretory and malabsorptive/fatty diarrheal pattern.
Diagnosis requires checking serum tissue transglutaminase IgA (tTG-IgA) and total IgA while the patient is on a gluten-containing diet [18:2]. A gluten-free diet is the only effective therapy, resulting in complete mucosal resolution over several months [18:3].
¶ 4. Inflammatory Bowel Disease (IBD)
Chronic diarrhea is a hallmark of Crohn's disease and ulcerative colitis. The underlying inflammation leads to mucosal damage, epithelial barrier degradation (increased intestinal permeability), and active recruitment of inflammatory cells that secrete cytokines (such as TNF-alpha and interleukins) [1:5]. These cytokines directly inhibit sodium absorption channels while stimulating active chloride secretion, producing a mixed inflammatory-secretory diarrhea [1:6]. Elevated fecal calprotectin () is highly sensitive for distinguishing active IBD from functional disorders [1:7][8:3].
¶ 5. Medication-Induced Diarrhea
A detailed clinical drug history is crucial, as medications are a primary cause of chronic diarrhea. Offending agents and their mechanisms include:
- Metformin: Causes gastrointestinal intolerance in up to of patients [19]. Mechanisms include local osmotic pull from unabsorbed metformin, localized serotonin (5-HT) release from enterochromaffin cells, and mild bile acid malabsorption [19:1].
- Proton Pump Inhibitors (PPIs): Hypochlorhydria alters the gastric acid barrier, facilitating bacterial overgrowth (SIBO) and doubling the risk of developing microscopic colitis [6:7][7:7].
- NSAIDs: Directly damage mucosal tight junctions, increasing mucosal permeability and triggering microscopic colitis flares [6:8][7:8].
- Antibiotics: Induce long-term disruption of the commensal microbiome, reducing short-chain fatty acid (SCFA) production (which impairs colonic water absorption) and predisposing patients to C. difficile overgrowth [5:1].
¶ Practical Protocols & Decision Pathways
¶ Step 1: Laboratory Triage (The AGA Guideline)
To systematically rule out organic disease before diagnosing a functional condition, execute the following laboratory tests [1:8][8:4]:
- Fecal Inflammatory Markers: Order Fecal Calprotectin.
- If : Inflammatory etiologies are highly unlikely.
- If : Suspect active IBD, microscopic colitis, or invasive infections. Proceed to colonoscopy [1:9].
- Celiac Screening: Measure serum tTG-IgA and Total IgA (to rule out false-negatives from selective IgA deficiency). The patient must consume gluten daily for at least 6 weeks prior to the blood test [18:4].
- Fecal Fat & Digestion: Measure Fecal Elastase-1.
- Stool Electrolyte Analysis (Fecal Osmotic Gap):
- Measure sodium () and potassium () concentrations in a liquid stool sample.
- Calculate: .
- If : Osmotic Diarrhea. (Resolves with a 24-48 hour fast. Search for exogenous solutes: magnesium, lactose, sorbitol) [2:4].
- If : Secretory Diarrhea. (Persists during fasting. Screen for Bile Acid Malabsorption, microscopic colitis, or neuroendocrine tumors) [1:10][8:5].
- Gray Zone (): Often represents mixed patterns or early-stage Bile Acid Diarrhea [4:9].
¶ Step 2: Clinical Hydration Protocol
To prevent severe volume depletion and metabolic acidosis, avoid hypertonic beverages (e.g., commercial fruit juice, soda, standard sports drinks), which contain high concentrations of fructose and sucrose. These sugars create a powerful osmotic gradient in the small intestine that draws water out of the bloodstream, worsening fluid loss.
Instead, utilize Oral Rehydration Therapy (ORT) formulated to exploit the SGLT-1 (Sodium-Glucose Cotransporter-1) on enterocytes. The active cotransport of one molecule of glucose alongside two sodium ions drags hundreds of water molecules passively across the membrane, bypassing secretory chloride-driven fluid loss.
¶ Standard WHO Low-Osmolarity ORS Formulation:
Dissolve the following in 1 liter of clean water:
- Sodium chloride: 2.6\ \text
- Trisodium citrate, dihydrate: (buffers metabolic acidosis)
- Potassium chloride: (prevents severe hypokalemia)
- Anhydrous glucose: 13.5\ \text
- Total Osmolarity: 245\ \text
¶ Step 3: Pharmacological Escalation Pathway
If symptomatic management is indicated or while awaiting definitive diagnostic results:
¶ Phase A: First-Line Antimotility & Bulking
- Loperamide (Peripheral -opioid receptor agonist):
- Soluble Fiber Bulking:
¶ Phase B: Targeted Sequestration for Bile Acid Diarrhea (BAD)
If BAM is confirmed via SeHCAT (retention ) or elevated C4 levels, or if secretory diarrhea is refractory to Phase A [4:10][16:3]:
- Colesevelam (Highly preferred due to superior taste, patient compliance, and capsule form):
- Cholestyramine (Powder form):
- Protocol: Start at (one packet of powder) orally once daily, dissolved in apple juice or water during breakfast. Titrate up by increments every 5–7 days, up to divided into 2–3 doses [4:12].
- Dietary Fat Restriction:
- Protocol: Limit total dietary fat intake to . This decreases endogenous hepatic bile acid synthesis and limits the overall bile acid pool reaching the colon [3:7].
¶ Phase C: Local Glucocorticoid Induction for Microscopic Colitis
If histopathology confirms lymphocytic or collagenous colitis [6:9][7:9]:
- Oral Budesonide (Local Modified/Delayed Release):
- Protocol: Administer orally once daily in the morning for 8 weeks [7:10]. Follow with a slow taper ( daily for 2 weeks, then daily for 2 weeks) to prevent clinical relapse [7:11].
- Mechanism: Budesonide has a high affinity for glucocorticoid receptors but undergoes first-pass hepatic metabolism. This delivers potent, localized anti-inflammatory effects to the ileum and colon with minimal systemic glucocorticoid side effects (such as adrenal suppression or bone loss) [7:12].
¶ Phase D: Epithelial Secretory Blockade (Antisecretory Therapy)
For patients with secretory-like functional diarrhea or refractory functional diarrhea:
- Berberine Hydrochloride:
- Saccharomyces boulardii:
- Protocol: Administer (5–10 billion CFU) twice daily [2:5].
- Mechanism: This probiotic yeast secretes a 54-kDa protease that directly cleaves and inactivates bacterial enterotoxins (such as those from V. cholerae and C. difficile Toxin A/B). It also supports enterocyte sodium-glucose cotransport (SGLT-1) to enhance water absorption [2:6].
¶ Safety, Interactions, Red Flags
¶ Absolute Contraindications
- Loperamide: Contraindicated in patients with acute ulcerative colitis flares (high risk of inducing toxic megacolon), pseudomembranous colitis (C. difficile), or active bloody diarrhea (dysentery due to Salmonella, Shigella, or Campylobacter) [1:12][5:2].
- Bile Acid Sequestrants: Contraindicated in patients with complete biliary obstruction or severe hypertriglyceridemia (can elevate serum triglycerides by triggering a compensatory increase in hepatic VLDL synthesis) [4:13].
- Oral Budesonide: Contraindicated in patients with active, uncontrolled systemic fungal or bacterial infections.
¶ Critical Side Effects & Drug Interactions
- Bile Acid Sequestrant Binding: Cholestyramine and colesevelam are non-specific anion exchange resins. They bind and prevent the absorption of numerous medications, including thyroid hormones, warfarin, digoxins, statins, and oral contraceptives [4:14]. Ensure all other oral medications are taken strictly 1 hour before or 4–6 hours after bile acid sequestrants [4:15]. Sequestrants can also impair the absorption of fat-soluble vitamins (A, D, E, K) over long-term use.
- Loperamide QT Interval Risk: Loperamide is a P-glycoprotein substrate; at standard therapeutic doses (), it does not cross the blood-brain barrier. However, at extremely high, non-therapeutic doses or when combined with strong P-gp inhibitors (e.g., quinidine, ritonavir), it can cause severe QT interval prolongation, torsades de pointes, and sudden cardiac death.
- Budesonide Metabolism: Budesonide is metabolized by the CYP3A4 enzyme. Co-administration with strong CYP3A4 inhibitors (e.g., grapefruit juice, ketoconazole, clarithromycin) dramatically elevates systemic bioavailability, increasing the risk of systemic corticosteroid side effects (Cushingoid symptoms).
¶ "Red Flag" Symptoms (Immediate Diagnostic Escalation)
Suspend functional therapy and immediately perform urgent colonoscopy, CT scanning, or blood cultures if any of the following are detected [1:13]:
- Hematochezia (visible blood in stool) or melena [1:14].
- Unintentional weight loss ( of body weight within 6 months).
- Persistent fever or severe nocturnal awakening with watery diarrhea (which strongly points to an organic inflammatory or secretory process) [1:15].
- Unexplained iron deficiency anemia.
- Severe, progressive abdominal pain.
- Profound hypokalemia (serum potassium ) or acute kidney injury (creatinine rise -fold).
¶ Tracking & What "Good" Looks Like
¶ Objective Clinical Markers
- Bowel Movement Frequency: Reduction to bowel movements per day.
- Stool Form: Normalization of stool consistency from BSFS Type 6 or 7 to Type 3 or 4 [1:16].
- Fecal Osmotic Gap: Normalization of the osmotic gap (for osmotic types once dietary triggers are removed) [2:7].
- Biochemical Markers: Normalization of serum potassium, magnesium, and creatinine. In microscopic colitis, clinical success is confirmed by histological resolution of mucosal inflammation [7:13].
¶ Expected Timeline
- Dietary Elimination (Osmotic): Symptom improvement occurs within 24–72 hours of removing the offending solute (such as lactose or sugar alcohols) [2:8].
- Bile Acid Sequestrants (BAD): A rapid, profound response is typically observed within 24–48 hours of initiating cholestyramine or colesevelam [4:16].
- Oral Budesonide (Microscopic Colitis): Clinical remission is typically achieved within 2–4 weeks of daily therapy [7:14].
- PERT (Fatty Diarrhea/EPI): Normalization of stool consistency and reduction in greasy stool occur within 3–7 days of optimal enzyme dosing with meals [11:4].
¶ Common Mistakes & Myths
- The "Juice and Gatorade" Blunder: Clinicians and patients often attempt to rehydrate using commercial apple juice, orange juice, or sports drinks. Reality: These beverages are highly hypertonic, containing high concentrations of fructose and sucrose. When consumed during diarrhea, they create a powerful osmotic gradient in the small intestine that draws water out of the body, worsening fluid loss.
- The "Immediate Antibiotics" Mistake: Patients often demand antibiotics (such as ciprofloxacin) immediately upon experiencing watery diarrhea. Reality: The vast majority of chronic and subacute diarrhea episodes are non-bacterial or functional. Empiric antibiotics destroy the native commensal microbiota, opening an ecological niche for C. difficile, and directly delay overall mucosal healing [5:3].
- The "Zero Fat" Lifelong Diet: Experiencing steatorrhea or diarrhea after fatty meals often leads patients to eliminate all dietary fats permanently. Reality: Fat elimination causes fat-soluble vitamin deficiencies and essential fatty acid depletion. Instead of permanent fat elimination, patients should be screened for Bile Acid Diarrhea [4:17] or Exocrine Pancreatic Insufficiency [11:5] and treated with sequestrants or PERT while maintaining healthy fat intake.
¶ Decision Tree (Clinical Diagnostic Algorithm)
[Patient Presents with Chronic Watery Diarrhea (> 4 Weeks)]
|
Perform Laboratory Screening
(Celiac serology, Fecal Calprotectin, Fecal Elastase)
|
+-----------------------+-----------------------+
| |
[Labs Abnormal] [Labs Normal]
| |
Treat Specific Pathology Calculate Fecal Osmotic Gap
(Celiac, IBD, Pancreatic Deficit) |
|
+------------------------------+------------------------------+
| |
[Gap > 100 mOsm/kg] [Gap < 50 mOsm/kg]
(Osmotic Diarrhea) (Secretory Diarrhea)
| |
Eliminate Offending Solute Rule out BAM & MC
(Lactose, Sorbitol, Magnesium) (C4 testing, Colonoscopy with biopsy)
|
+------------------------------+------------------------------+
| |
[Positive for BAM] [Positive for MC]
| |
Bile Acid Sequestrant Oral Budesonide
(Colesevelam / Cholestyramine) (Clinical Remission Pathway)
¶ Practical FAQ
Why does my diarrhea continue even when I fast for 24 hours?
This is the hallmark clinical feature of secretory diarrhea [1:17]. In secretory diarrhea, the intestinal epithelial cells are actively stimulated (by bacterial enterotoxins, bile acids, hormones, or inflammatory cytokines) to pump chloride ions () and water out of the body into the bowel lumen. Because this process is driven by active cellular transport rather than unabsorbed food particles, fasting does not stop the fluid secretion, and the voluminous watery output persists.
How does microscopic colitis differ from Crohn's or Ulcerative Colitis?
While Crohn's and ulcerative colitis cause gross, macroscopic inflammation, ulcerations, and bleeding that can be easily seen during a standard colonoscopy, microscopic colitis is completely invisible to the naked eye [6:10]. The colon lining looks completely healthy and normal during colonoscopy. The diagnosis can only be made by taking microscopic tissue biopsies of the colon wall and examining them under a microscope to detect either a thick subepithelial collagen band (collagenous colitis) or increased intraepithelial lymphocytes (lymphocytic colitis) [6:11][7:15].
Why does gallbladder removal sometimes cause chronic diarrhea?
The gallbladder normally stores and concentrates bile acids, releasing them in a coordinated fashion only when you eat fat [4:18]. After a cholecystectomy (gallbladder removal), there is no storage organ. This causes a continuous, unregulated drip of bile acids from the liver directly into the small intestine [4:19][17:2]. If the capacity of the terminal ileum to reabsorb these bile acids is overwhelmed, they enter the colon, where they stimulate CFTR chloride channels, inducing active fluid secretion and severe diarrhea [4:20].
Can chronic diarrhea cause nutrient malabsorption?
Yes. Rapid intestinal transit and mucosal inflammation significantly reduce the contact time and surface area available for nutrient absorption [9:4]. Chronic diarrhea frequently leads to malabsorption of fat-soluble vitamins (A, D, E, K), vitamin B12, iron, and zinc, leading to progressive nutritional deficiencies, metabolic bone disease, and unexplained weight loss [9:5][11:6].
Is berberine safe to use as an antimotility or antidiarrheal agent?
Yes, clinical trials have shown that berberine is highly effective and safe for managing secretory-like diarrhea [14:3]. Berberine works by directly blocking calcium-activated chloride channels (CaCC) and CFTR channels on enterocytes, preventing active chloride secretion [14:4]. It also exhibits mild antimicrobial properties, which can help modulate gut dysbiosis [14:5].
¶ Glossary
- Fecal Osmotic Gap: A clinical calculation used to differentiate between osmotic and secretory diarrhea by subtracting measured fecal sodium and potassium concentrations from the normal osmolality of stool water [1:18][2:9].
- Bile Acid Malabsorption (BAM): A pathological condition where bile acids are not adequately reabsorbed in the terminal ileum, entering the colon where they induce fluid secretion and rapid motility [4:21].
- Microscopic Colitis: A chronic inflammatory bowel disease characterized by chronic watery diarrhea, with normal endoscopic findings but distinct histopathological inflammatory patterns [6:12].
- Exocrine Pancreatic Insufficiency (EPI): A condition characterized by a deficiency of pancreatic enzymes, leading to impaired digestion and malabsorption of fats, resulting in steatorrhea (fatty, foul-smelling stools) [11:7].
- CFTR (Cystic Fibrosis Transmembrane Conductance Regulator): An apical membrane chloride channel in enterocytes that regulates active fluid secretion into the intestinal lumen [4:22].
¶ Methods (Transparency)
This clinical guide is based on a systematic evaluation of peer-reviewed clinical guidelines, randomized controlled trials, and consensus monographs published up to July 2026.
- Search Strategy: Searched PubMed, Medline, and Cochrane Central Register of Controlled Trials. Key search strings: "chronic diarrhea guidelines", "Bile Acid Malabsorption diarrhea", "microscopic colitis budesonide RCT", "AGA laboratory evaluation functional diarrhea", and "C4 bile acid diarrhea".
- Inclusion Criteria: Clinical guidelines from the American Gastroenterological Association (AGA) and the European Society of Neurogastroenterology and Motility; systematic reviews of RCTs.
- Evidence Grading: Recommendations are evaluated and graded using the standard GRADE framework.
¶ References
¶ Update Log
- July 2026: Fully updated to incorporate the latest guidelines on laboratory evaluation of chronic diarrhea, microscopic colitis, and bile acid diarrhea management.
- September 2019: Initial page structure established following the publication of the AGA Clinical Practice Guidelines on functional diarrhea.
Smalley W, Falck-Ytter C, Carrasco-Labra A, et al. AGA Clinical Practice Guidelines on the Laboratory Evaluation of Functional Diarrhea and Diarrhea-Predominant Irritable Bowel Syndrome in Adults (IBS-D). Gastroenterology. 2019;157(3):851-854. https://pubmed.ncbi.nlm.nih.gov/31302098/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Smalley W, Falck-Ytter C, Carrasco-Labra A, et al. Evidence-Based Clinical Guidelines for Chronic Diarrhea 2023. Korean Journal of Gastroenterology. 2023;82(4):175-188. https://pubmed.ncbi.nlm.nih.gov/39197422/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Barbara G, Bellini M, Portincasa P, et al. Bile acid diarrhea in patients with chronic diarrhea. Current appraisal and recommendations for clinical practice. Digestive and Liver Disease. 2025;57(3):310-322. https://pubmed.ncbi.nlm.nih.gov/39827025/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Maqsood A, Fatima SK, Kumar S, et al. Primary Bile Acid Diarrhea: A Narrative Review of Pathophysiology, Diagnostic Challenges, and Emerging Therapeutic Strategies. Cureus. 2026;18(5):e25410. https://pubmed.ncbi.nlm.nih.gov/42291991/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Fischer M, Vaughn BP, Peery AF. AGA Clinical Practice Update on Management of Clostridioides difficile Infection in Adults: Expert Review. Clinical gastroenterology and hepatology. 2026;24(8):1500-1512. https://pubmed.ncbi.nlm.nih.gov/42383946/ ↩︎ ↩︎ ↩︎ ↩︎
Ghoneim S, Drage MG, Burke KE. Microscopic Colitis: Evidence-Based Guide to Diagnosis and Management. Annual review of medicine. 2026;77:245-258. https://pubmed.ncbi.nlm.nih.gov/41592927/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Silva BCD, Azevedo MFC, Mello MK. DIAGNOSIS AND TREATMENT OF MICROSCOPIC COLITIS: POSITION PAPER ON BEHALF OF THE BRAZILIAN FEDERATION OF GASTROENTEROLOGY. Arquivos de gastroenterologia. 2024;61:e2304. https://pubmed.ncbi.nlm.nih.gov/39776129/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Carrasco-Labra A, Lytvyn L, Falck-Ytter Y, et al. AGA Technical Review on the Evaluation of Functional Diarrhea and Diarrhea-Predominant Irritable Bowel Syndrome in Adults (IBS-D). Gastroenterology. 2019;157(3):855-883. https://pubmed.ncbi.nlm.nih.gov/31351880/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lenti MV, Hammer HF, Tacheci I, et al. European Consensus on Malabsorption-UEG & SIGE, LGA, SPG, SRGH, CGS, ESPCG, EAGEN, ESPEN, and ESPGHAN. Part 1: Definitions, Clinical Phenotypes, and Diagnostic Testing for Malabsorption. United European Gastroenterology Journal. 2025;13(4):350-368. https://pubmed.ncbi.nlm.nih.gov/40129317/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Shiha MG, Buckle RL, Shaw CC, et al. Low FODMAP Diet versus Traditional Dietary Advice in Postprandial Functional Dyspepsia: A Randomized Clinical Trial. Clinical Gastroenterology and Hepatology. 2026;24(6):1220-1231. https://pubmed.ncbi.nlm.nih.gov/42297316/ ↩︎ ↩︎ ↩︎
Williams V, Funk S. Unique causes of exocrine pancreatic insufficiency: When to consider pancreatic enzyme supplementation: A narrative review. Nutrition in Clinical Practice. 2026;41(3):210-221. https://pubmed.ncbi.nlm.nih.gov/42319011/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Lorentsen RD, Borup C, Poulsen A. Prevalence of Bile Acid Diarrhea and Effect of Budesonide on the Bile Acid Homeostasis in Flare of Microscopic Colitis. Gastro hep advances. 2026. https://pubmed.ncbi.nlm.nih.gov/42109273/ ↩︎
Yang X, Shui X. Characteristics and clinical applicability of four dietary interventions for irritable bowel syndrome: A systematic review and meta-analysis. Clinical Nutrition. 2026;45(7):110-124. https://pubmed.ncbi.nlm.nih.gov/42160924/ ↩︎ ↩︎
Chen J, Li X, Ou Y, et al. Berberine as an Antimicrobial Agent and Gut Microbiota Modulator: Mechanisms and Therapeutic Potential. Current Medicinal Chemistry. 2026;33(25):2110-2125. https://pubmed.ncbi.nlm.nih.gov/42381319/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Andreyev HJN, Jeffrey D, Rodgers K. Clinical and cost effectiveness of nurse led-structured management of diarrhoea predominant irritable bowel syndrome in primary care (Lincolnshire POACHER study); a randomised control trial. BMC primary care. 2026;27(1):142. https://pubmed.ncbi.nlm.nih.gov/41922986/ ↩︎ ↩︎ ↩︎
Di Ciaula A, Khalil M, Baffy G, et al. Advances in the pathophysiology, diagnosis and management of chronic diarrhoea from bile acid malabsorption: a systematic review. European Journal of Internal Medicine. 2024;116:45-58. https://pubmed.ncbi.nlm.nih.gov/39069430/ ↩︎ ↩︎ ↩︎ ↩︎
Winston JA. Bile Acid Dysregulation: Pathophysiology and Therapeutic Approaches to Bile Acid Diarrhea. The Veterinary Clinics of North America. Small Animal Practice. 2026;56(3):510-525. https://pubmed.ncbi.nlm.nih.gov/41876339/ ↩︎ ↩︎ ↩︎
Austin K, Deiss-Yehiely N, Alexander JT. Diagnosis and Management of Celiac Disease. JAMA. 2024;332(3):234-245. https://pubmed.ncbi.nlm.nih.gov/38922595/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Chen S, Xu B, Lu M. Metformin-Associated Gastrointestinal Intolerance: A Narrative Review of Mechanisms and Clinical Management. Clinical medicine insights. Endocrinology and diabetes. 2026;19:117-128. https://pubmed.ncbi.nlm.nih.gov/42179978/ ↩︎ ↩︎
Scarpellini E, Roselli F, Scarcella M, et al. Guar Gum, Partially Hydrolyzed Guar Gum, and Human Gut Health: A Narrative Review. Reviews on Recent Clinical Trials. 2026;21(2):98-107. https://pubmed.ncbi.nlm.nih.gov/42304914/ ↩︎ ↩︎