¶ Microscopic Colitis
| Primary Subtypes | Collagenous Colitis, Lymphocytic Colitis |
| Clinical Presentation | Chronic, Watery, Non-bloody Diarrhea |
| Endoscopy Finding | Normal or Near-Normal Mucosa |
| Primary Drug Triggers | NSAIDs, PPIs, SSRIs, Levodopa |
| First-Line Therapy | Oral Budesonide (9 mg/day) Taper |
| Demographics | Predominantly Females aged >60 |
Microscopic Colitis is a chronic inflammatory bowel disease characterized by persistent, high-volume, watery, non-bloody diarrhea coexisting with a macroscopically normal or near-normal colonic mucosa on colonoscopy. Because mucosal abnormalities are invisible to the naked eye during endoscopy, the diagnosis is established strictly through the histopathological analysis of colonic biopsies, which categorize the disease into two primary subtypes: Collagenous Colitis (CC) and Lymphocytic Colitis (LC)[1]. Often triggered or exacerbated by common pharmaceuticals (such as proton pump inhibitors, non-steroidal anti-inflammatory drugs, and selective serotonin reuptake inhibitors), microscopic colitis exhibits high responsiveness to localized, non-systemic corticosteroid therapy (Budesonide) and bile acid binders, carrying an excellent long-term prognosis without elevating the risk of colorectal dysplasia or malignancy[2][3][1:1].
¶ At a glance
Key points (high-level summary)
- The Endoscopy Paradox: The colon appears completely healthy during standard colonoscopy; random segmental biopsies are mandatory to reveal underlying mucosal inflammation[4][1:2].
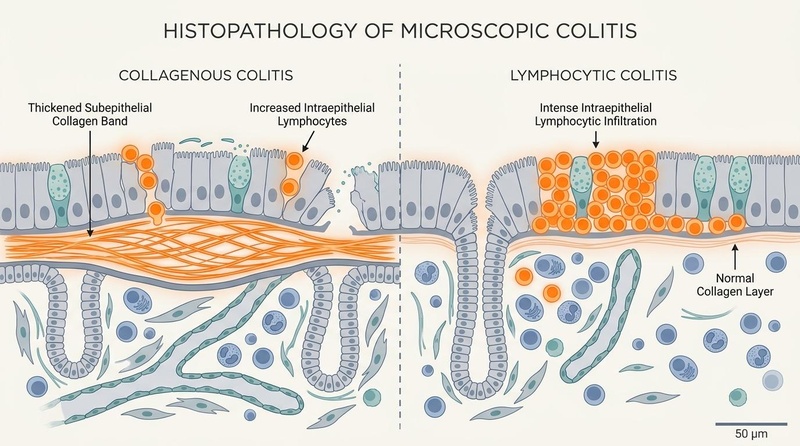
- Clinical Subtypes: Collagenous Colitis is marked by a thickened subepithelial collagen band (>10 µm), whereas Lymphocytic Colitis is defined by intense intraepithelial lymphocytic infiltration (≥20 per 100 enterocytes)[1:3].
- Established Drug Associations: Highly linked to daily medication exposure (especially Lansoprazole, Sertraline, and Ibuprofen); drug discontinuation is a critical first-line diagnostic and therapeutic step[5][6].
- Therapeutic Gold Standard: Oral budesonide (9 mg/day) achieves rapid clinical and histological remission within 2–4 weeks, utilizing an ileocolonic-release mechanism that minimizes systemic side effects[7][2:1][8].
What people use it for
- Primary Goals: Complete cessation of chronic diarrhea, correction of intestinal barrier hyperpermeability, preservation of fluid-electrolyte homeostasis, and long-term, steroid-free clinical and histological remission[3:1][1:4].
- Evidence Quality: High-certainty evidence supports oral budesonide for induction and low-dose maintenance; moderate-certainty evidence supports drug dechallenge protocols, bile acid sequestrant therapy, and anti-TNF biologics for refractory disease[7:1][9][2:2][10].
Budesonide undergoes extensive hepatic first-pass metabolism (~90%) via the CYP3A4 enzyme, making it a safe, localized treatment. However, avoid strong CYP3A4 inhibitors (e.g., ketoconazole, grapefruit juice) which elevate systemic steroid exposure. Routine screening of bone mineral density (DEXA) and intraocular pressure is required during prolonged use.
¶ Clinical Protocol Summary
- Phase 1 (Drug Review): Immediate dechallenge and permanent cessation of all NSAIDs, PPIs, and suspected SSRIs[^16].
- Phase 2 (Induction): Budesonide 9 mg orally once daily in the morning for 6–8 weeks[^20].
- Phase 3 (Taper): Gradual reduction to 6 mg/day for 2 weeks, then 3 mg/day for 2 weeks before discontinuation[^6].
- Phase 4 (Relapse Management): Re-induction followed by the lowest effective maintenance dose (3–6 mg/day) or adjuvant Cholestyramine (4 g/day)[^10][^13].
Bottom Line: Microscopic Colitis is a highly treatable, underdiagnosed cause of chronic secretory diarrhea. Successful management relies on systematic medication dechallenge, targeted colonic mucosal biopsies, and localized budesonide induction.
¶ What is Microscopic Colitis?
Microscopic Colitis is a highly specific clinicopathological entity that represents a major, yet frequently overlooked, cause of chronic diarrhea. It compromises mucosal epithelial water transport and active electrolyte absorption without causing macroscopic ulceration or tissue destruction.
¶ Epidemiology and Age Predominance
Once considered a rare condition, the documented incidence of microscopic colitis has risen significantly over the past three decades. The global incidence currently ranges from 5 to 10 cases per 100,000 person-years, with a prevalence approaching 100 cases per 100,000 individuals—figures comparable to classical inflammatory bowel disease[1:5].
The disease displays a striking age and sex distribution:
- Older Adults (Geriatric Cohorts): The peak age of onset is between 60 and 70 years. Up to 75% of all microscopic colitis cases are diagnosed in patients over the age of 60[7:2]. In this population, the disease can rapidly lead to severe dehydration, prerenal acute kidney injury, and electrolyte depletion.
- Older Women: There is a powerful female predominance. The female-to-male ratio is approximately 4:1 to 9:1 for Collagenous Colitis, and 2:1 to 4:1 for Lymphocytic Colitis[1:6]. Emerging cohort analyses indicate that the clinical course of microscopic colitis is heavily modulated by endocrine factors, with post-menopausal estrogen deficiency playing a primary role in the loss of epithelial tight junction integrity[11].
- Middle-Aged and Young Adults: While less common, microscopic colitis affects young adults and is frequently misdiagnosed as irritable bowel syndrome (IBS-D) or functional diarrhea. In younger patient cohorts, there is a strong association with concurrent autoimmune conditions, particularly celiac disease, type 1 diabetes mellitus, and autoimmune thyroiditis[3:2].
- Pediatric Populations: Pediatric-onset microscopic colitis is exceptionally rare, almost always presenting in children with severe concurrent celiac enteropathy or autoimmune enteropathy[12].
¶ The Normal Colonoscopy Paradox
The defining paradox of microscopic colitis is the coexistence of severe, high-volume secretory diarrhea with a completely normal-appearing colon during standard colonoscopy.
During standard colonoscopy, the mucosal lining of the colon appears healthy, pink, and vascularly intact. In some cases, subtle, non-specific abnormalities may be noted, such as mild mucosal edema, minimal erythema, or fine, superficial longitudinal mucosal tears (known as "cat scratch colon"). However, these findings are completely insufficient to explain the severity of the patient's symptoms[1:7].
This "normal colonoscopy" paradox frequently results in long diagnostic delays. Patients are often mislabeled as having diarrhea-predominant irritable bowel syndrome (IBS-D) for years before random mucosal biopsies are performed to confirm the diagnosis[3:3][1:8].
¶ Subtypes and Histopathological Framework
Microscopic colitis is categorized into two distinct histopathological patterns. While they present with identical clinical symptoms, they exhibit clear differences under microscopic examination:

¶ 1. Collagenous Colitis (CC)
Collagenous Colitis is characterized by the deposition of a thick, continuous subepithelial collagen band directly beneath the surface epithelial basement membrane[1:9].
- Diagnostic Threshold: While a healthy colonic mucosa features a subepithelial collagen layer of less than 3 µm, CC is diagnosed when the collagen band thickness exceeds 10 µm (typically ranging from 15 to 30 µm)[1:10].
- Key Histological Features: The collagen band is easily highlighted using Masson's trichrome stain. The overlying surface epithelium often shows degenerative changes, including cell flattening, mucin depletion, and detachment from the thickened basement membrane (known as epithelial sloughing)[1:11]. There is also a prominent inflammatory infiltration in the lamina propria, consisting mainly of plasma cells and lymphocytes.
¶ 2. Lymphocytic Colitis (LC)
Lymphocytic Colitis is defined by a marked, diffuse increase in the density of intraepithelial lymphocytes (IELs) within the colonic surface epithelium, without a thickened subepithelial collagen band[1:12].
- Diagnostic Threshold: LC is diagnosed when there are ≥20 intraepithelial lymphocytes per 100 epithelial cells (compared to fewer than 5 in healthy mucosa)[1:13].
- Key Histological Features: The subepithelial collagen band remains normal (
 µm). The IELs are predominantly cytotoxic CD8+ T lymphocytes, which can be clearly visualized using CD3 immunohistochemical staining. The lamina propria exhibits a rich inflammatory infiltrate similar to CC, with minimal crypt distortion or architectural damage.
µm). The IELs are predominantly cytotoxic CD8+ T lymphocytes, which can be clearly visualized using CD3 immunohistochemical staining. The lamina propria exhibits a rich inflammatory infiltrate similar to CC, with minimal crypt distortion or architectural damage.
¶ 3. Incomplete Microscopic Colitis (iMC)
In clinical practice, up to 10% of patients present with typical clinical symptoms of microscopic colitis but have borderline histopathological features that do not fully meet the strict diagnostic thresholds for CC or LC[13].
- Diagnostic Parameters: Features include a subepithelial collagen band between 5 and 10 µm, or an IEL count of 10 to 19 lymphocytes per 100 epithelial cells, accompanied by typical lamina propria inflammation[13:1].
- Clinical Significance: Large multi-center retrospective analyses have shown that incomplete microscopic colitis (iMC) is clinically identical to classic CC and LC in terms of severity, drug associations, and response to budesonide[13:2][14]. Emerging consensus guidelines suggest expanding the definition of microscopic colitis to include iMC, ensuring these patients are not denied first-line medical therapy[13:3].
¶ Pathophysiological Mechanisms
The development of microscopic colitis involves a complex interaction between genetic susceptibility, environmental drug triggers, epithelial barrier failure, and a dysregulated immune response:
[ HLA-DQ2/DQ8 Genotype / Estrogen Deficiency ]
│
▼
[ Epithelial Barrier Tight Junction Collapse ]
(Triggered by NSAIDs, PPIs, or Luminal Toxins)
│
▼
[ Hyperosmolar Fluid Leakage ]
│
▼
[ Antigen Translocation & Presentation ]
│
┌────────────────────────┴────────────────────────┐
▼ ▼
[ Intraepithelial CD8+ T Cells ] [ Lamina Propria Activation ]
(Release Granzyme B & Perforin) (IL-1β, TNF-α, IFN-γ release)
│ │
▼ ▼
[ Epithelial Cell Apoptosis ] [ Myofibroblast Activation ]
│ │
│ ▼
│ [ Subepithelial Collagen Band ]
│ (Deposition of Type I & III)
│ │
└────────────────────────┬────────────────────────┘
▼
[ Severe Secretory Watery Diarrhea ]
¶ 1. Genetic Susceptibility and HLA Associations
Microscopic colitis is strongly linked to the HLA-DQ2 and HLA-DQ8 haplotypes, sharing a genetic risk profile with celiac disease[1:14]. This genetic basis suggests that microscopic colitis is driven by abnormal antigen presentation to CD4+ T helper cells, triggering a downstream chronic inflammatory cascade in response to otherwise harmless luminal antigens.
¶ 2. Epithelial Barrier Dysfunction
The primary event in microscopic colitis is the breakdown of the intestinal permeability barrier. Daily exposure to medication triggers (such as NSAIDs or PPIs) or luminal toxins alters the intracellular pH and disrupts mitochondrial oxidative phosphorylation in colonocytes.
This disruption causes the collapse of apical tight junction proteins, including claudin-1, claudin-4, and occludin[1:15]. The resulting paracellular hyperpermeability allows luminal bacteria, dietary proteins, and bile acids to penetrate deep into the lamina propria, initiating a robust immune response.
¶ 3. T-Cell-Mediated Cytotoxicity and Epithelial Damage
The colonic epithelium becomes heavily infiltrated by cytotoxic CD8+ T lymphocytes expressing the CD103 integrin (). These CD103+ T cells bind directly to E-cadherin on the basolateral surface of epithelial cells.
Upon activation, they release cytotoxic molecules (such as perforin and granzyme B), which trigger apoptosis and cell flattening in the enterocytes[1:16]. This cytotoxic damage directly impairs the metabolic and absorptive capacity of the colonic lining.
¶ 4. Downregulation of Bicarbonate/Chloride Exchangers
The localized release of pro-inflammatory cytokines—particularly TNF-, IL-1, and IFN-—profoundly alters mucosal transport proteins:
- DRA Transporter Downregulation: There is a dramatic downregulation of the DRA (Downregulated in Adenoma / SLC26A3) exchanger[1:17].
- NHE3 Transporter Downregulation: Concurrently, the NHE3 (Sodium-Hydrogen Exchanger 3 / SLC9A3) transporter is suppressed.
- The loss of these active transporters prevents the colonic mucosa from absorbing luminal sodium and chloride. Instead, it shifts the mucosa into an active secretory state, causing high-volume, watery, sodium-rich diarrhea.
¶ 5. Myofibroblast Activation and Fibrogenesis (in CC)
In Collagenous Colitis, localized chronic inflammation and the production of transforming growth factor-beta 1 (TGF-) activate subepithelial myofibroblasts. These activated cells synthesize and deposit collagen types I and III directly beneath the epithelial basement membrane[1:18].
The resulting subepithelial collagen band acts as a physical barrier, further blocking water and sodium absorption and exacerbating secretory diarrhea.
¶ Diagnostic Pathways and Pitfalls
Because the colon appears normal on colonoscopy, making the diagnosis of microscopic colitis depends on following a precise, systematic diagnostic pathway:
Chronic Watery Diarrhea Presentation
│
▼
Standard Colonoscopy Scheduled
│
┌────────────────────┴────────────────────┐
▼ ▼
Macroscopic Lesions Seen Mucosa Appears Normal
│ │
▼ ▼
Biopsy Directed to Lesion (segmental-biopsies)
(Rule out Crohn's/UC/Cancer) Perform Segmental Biopsies
(Right, Transverse, Left Colon)
│
┌────────────────────┴────────────────────┐
▼ ▼
CC or LC Confirmed Borderline Findings
│ (iMC / Borderline)
▼ │
Initiate Budesonide 9 mg/day ▼
Evaluate Clinical History
& Treat Symtomatically
¶ 1. The Segmental Biopsy Protocol
The most significant diagnostic pitfall in microscopic colitis is the failure to obtain a sufficient number of biopsies from multiple segments of the colon.
- Patchy Distribution: Histopathological changes in microscopic colitis are notoriously patchy and segmental. The subepithelial collagen thickening and intraepithelial lymphocytic infiltration are often more pronounced in the right (ascending and transverse) colon compared to the left (descending and sigmoid) colon[4:1][1:19].
- The Rectosigmoid Pitfall: Obtaining biopsies from the rectum or sigmoid colon alone will miss up to 20% of cases of microscopic colitis[4:2][1:20]. Therefore, random colonic biopsies must be obtained from at least three distinct anatomical segments: the ascending colon, transverse colon, and descending/sigmoid colon[4:3]. Clinicians should obtain at least two tissue specimens per segment.
¶ 2. Laboratory Testing and Differential Diagnosis
To confirm the diagnosis, clinicians must systematically rule out other causes of chronic watery diarrhea:
- Celiac Disease Screening: Given the strong genetic association (HLA-DQ2/DQ8), all patients diagnosed with microscopic colitis should undergo screening for celiac disease using serum IgA anti-tissue transglutaminase (anti-tTG) antibodies[1:21].
- Stool Testing: Rule out active infections, including Clostridioides difficile, Giardia lamblia, and other enteric pathogens, particularly in patients with a history of recent antibiotic use or travel.
- Fecal Calprotectin: While fecal calprotectin is a reliable biomarker for mucosal inflammation in Crohn's disease and ulcerative colitis, it is often only mildly elevated or normal in microscopic colitis. A normal fecal calprotectin level does not rule out microscopic colitis[1:22].
¶ Pharmaceutical Triggers
A key clinical feature of microscopic colitis is its strong, causal association with several widely prescribed medications. In drug-induced cases, the medication acts as an antigen or disrupts epithelial barrier function, triggering mucosal inflammation.
| Medication Class | Primary Examples | Proposed Pathophysiological Mechanism | Clinical Dechallenge Expectations |
|---|---|---|---|
| Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) | Ibuprofen, Diclofenac, Naproxen, Meloxicam | NSAIDs inhibit cyclooxygenase (COX-1 and COX-2) enzymes, depleting cytoprotective prostaglandins. This increases mucosal permeability, allowing luminal antigens to enter[5:1]. | High response. Discontinuation leads to complete clinical resolution in up to 30% of patients within 2–4 weeks[5:2]. |
| Proton Pump Inhibitors (PPIs) | Lansoprazole, Omeprazole, Esomeprazole, Pantoprazole | PPIs alter luminal pH, inhibit colonic -ATPase pumps, and disrupt colonocyte mitochondrial function, breaking down epithelial tight junctions[5:3][6:1]. | Lansoprazole has the strongest clinical association. Complete resolution often occurs within 2 weeks of stopping the drug[6:2]. |
| Selective Serotonin Reuptake Inhibitors (SSRIs) | Sertraline, Fluoxetine, Escitalopram, Citalopram | Serotonin transporters (SERT) are highly expressed in the intestinal mucosa. SSRIs alter mucosal serotonin levels, promoting mast cell degranulation and leukocyte recruitment[5:4]. | Sertraline is highly linked to flares in older women. Tapering and stopping the drug typically yields symptom resolution[5:5]. |
| Angiotensin II Receptor Blockers (ARBs) | Olmesartan, Valsartan | Olmesartan can trigger a severe, sprue-like enteropathy with mucosal atrophy and lymphocytic infiltration that mimics celiac disease and lymphocytic colitis[5:6]. | Stopping the drug results in complete mucosal healing and resolution of secretory diarrhea within 4–8 weeks[5:7]. |
| Levodopa/Carbidopa | Sinemet, Duopa | Oral levodopa formulations are associated with drug-induced microscopic colitis. The mechanism is thought to involve local dopaminergic toxicity to colonocytes[15]. | Excellent response. Transitioning patients to subcutaneous delivery systems (e.g., subcutaneous foslevodopa) leads to complete resolution[15:1]. |
| Immune Checkpoint Inhibitors | Pembrolizumab, Nivolumab, Ipilimumab | Blockade of PD-1, PD-L1, or CTLA-4 pathways triggers immune-mediated colitis, which can present histologically as microscopic colitis[5:8]. | Often refractory to drug stopping alone. Typically requires systemic corticosteroids or biologic therapy (Infliximab)[5:9]. |
¶ Overlap with Bile Acid Malabsorption (BAM)
A major clinical challenge in managing microscopic colitis is its significant pathophysiological overlap with Bile Acid Malabsorption (BAM).
¶ Prevalence and Coexistence
Up to 30% to 44% of patients with active microscopic colitis have concurrent Bile Acid Malabsorption[16][17]. In these patients, excess bile acids enter the colon and stimulate apical secretion through the cystic fibrosis transmembrane conductance regulator (CFTR) channel. This exacerbates secretory diarrhea, making it highly resistant to standard therapies.
¶ Cholecystectomy as a Risk Factor
A history of cholecystectomy is a major, independent risk factor for developing microscopic colitis[18]. Without a gallbladder to store bile, there is a continuous flow of bile acids into the small intestine, overwhelming the absorptive capacity of the terminal ileum.
This continuous exposure to high levels of luminal bile acids damages the colonic mucosa, disrupts tight junctions, and triggers the inflammatory cascade that leads to microscopic colitis[18:1].
¶ Diagnostic and Therapeutic Approaches
- Bile Acid Testing: The gold standard for diagnosing BAM is the HCAT (Selenium Homotaurocholic Acid Test) scan (retention <10% indicates malabsorption)[17:1]. Where HCAT is unavailable, clinicians can measure serum 7-hydroxy-4-cholesten-3-one (C4) levels or fecal bile acid excretion over 48 hours[9:1][17:2].
- Bile Acid Sequestrants: For patients who do not respond to budesonide, or who have proven concurrent BAM, initiate a bile acid binder such as Cholestyramine (4 g orally 1 to 3 times daily) or Colesevelam (625 mg, 2 to 4 tablets daily)[9:2][19]. These agents bind luminal bile acids, preventing them from stimulating colonic fluid secretion and providing rapid symptomatic relief[9:3].
¶ Therapeutic Protocols
The management of microscopic colitis focuses on removing environmental triggers, inducing clinical and histological remission, and preventing long-term relapse.
CONCURRENT SUSPECTED DRUG EXPOSURE
│
▼
Step 1: Medication Dechallenge
- Stop NSAIDs (substitute Acetaminophen)
- Stop PPIs (substitute H2-Blockers)
- Evaluate and taper suspected SSRIs
│
┌────────────────────────┴────────────────────────┐
▼ ▼
Mild Symptoms (<3 stools/day) Moderate to Severe Symptoms
│ │
▼ ▼
(symptom-control) (budesonide-induction)
Loperamide (2-4 mg/day) as needed Budesonide 9 mg/day (6-8 weeks)
│ │
│ ▼
│ (budesonide-taper)
│ Taper Budesonide:
│ - 6 mg/day for 2 weeks
│ - 3 mg/day for 2 weeks
│ - Stop
│ │
└────────────────────────┬────────────────────────┘
│
▼
┌──────────────────────────────┐
▼ ▼
Sustained Remission Symptomatic Relapse
│ │
▼ ▼
Annual Monitoring; [relapse-management]
No repeat biopsy - Re-induce with Budesonide 9 mg/day
needed - Establish Maintenance (3-6 mg/day)
- Add Cholestyramine (4 g/day)
¶ Step 1: Medication Review and Dechallenge
Review the patient's complete medication list. Systematically stop all suspected triggers (NSAIDs, PPIs, and SSRIs) for at least 2 to 4 weeks. For patients requiring acid suppression, substitute H2-receptor antagonists (such as Famotidine)[5:10].
¶ Step 2: Budesonide Induction Therapy
For patients with moderate-to-severe symptoms (typically defined as ≥3 loose stools per day), initiate first-line pharmacological induction:
- Budesonide (Entocort EC / Ortikos): 9 mg orally once daily in the morning for a continuous course of 6 to 8 weeks[1:23].
- Pharmacokinetics: Budesonide uses an ethylcellulose-coated granule formulation. This delays release until the drug reaches the terminal ileum and the ascending colon, ensuring maximum local concentration at the primary site of inflammation[7:3]. Because it undergoes extensive hepatic first-pass metabolism (~90%) via the CYP3A4 enzyme, it delivers potent local anti-inflammatory effects with minimal systemic steroid toxicity[7:4].
¶ Step 3: Budesonide Tapering Protocol
To prevent a sudden flare-up of symptoms upon stopping treatment, initiate a gradual tapering protocol over 4 weeks:
- Weeks 1–2 of Taper: Budesonide 6 mg orally once daily in the morning[7:5].
- Weeks 3–4 of Taper: Budesonide 3 mg orally once daily in the morning, then discontinue[7:6].
¶ Step 4: Management of Relapse and Maintenance Therapy
Symptomatic relapse is a common challenge in the long-term management of microscopic colitis.
- Relapse Statistics: Approximately 30% to 40% of patients experience a relapse within 6 months of completing their initial budesonide taper[2:3]. Relapse is more common in patients over 65, those with severe initial symptoms, and those with a history of long-term NSAID use[17:3][2:4].
- Budesonide Maintenance: For patients who relapse, re-induce with budesonide 9 mg/day until symptoms resolve, then establish a long-term maintenance dose. The goal is to find the lowest effective dose to maintain remission—typically 3 mg to 6 mg orally once daily[2:5][8:1].
- On-Demand Budesonide: Emerging qualitative studies suggest that an "on-demand" approach (where patients self-administer 3–9 mg/day during symptom flares and stop during periods of remission) is a highly effective, patient-preferred strategy that minimizes total drug exposure[20].
¶ Evidence Summary Table (Human Outcomes)
| Target Indication | Intervention | Typical Effect Size | Certainty of Evidence | Primary Study Support | Clinical Notes |
|---|---|---|---|---|---|
| Induction of Remission (CC & LC) | Oral Budesonide (9 mg/day) | High | Multi-center randomized controlled trials[2:6][8:2][1:24] | Achieves complete clinical remission and histopathological healing in >80% of cases within 2–4 weeks. First-line therapy. | |
| Maintenance of Remission | Low-dose Budesonide (3–6 mg/day) | High | Systematic reviews and meta-analyses[2:7][8:3] | Highly effective at preventing flares in budesonide-dependent patients. Long-term use requires monitoring. | |
| Drug-Induced MC Management | Discontinuation of offending drug (PPI, NSAID, SSRI) | Moderate | Retrospective cohort and pharmacovigilance studies[5:11][6:3] | Achieves complete resolution of secretory diarrhea in up to 30% of drug-induced cases without requiring steroids. | |
| Bile Acid Overlap Treatment | Bile Acid Sequestrants (Cholestyramine 4 g/day) | Moderate | Systematic reviews and clinical trials[9:4][19:1] | Indicated for patients with concurrent BAM or those who do not respond to budesonide. Highly effective. | |
| Symptom Control in Mild MC | Loperamide or Bismuth Subsalicylate | Low | Retrospective studies and clinical cohorts[21][1:25] | Provides mild-to-moderate symptomatic control of diarrhea; does not induce histological healing. | |
| Refractory MC Treatment | Anti-TNF Biologics (Infliximab / Adalimumab) | Moderate | Multi-center cohort studies (GETAID)[10:1][1:26] | Indicated for rare cases that are refractory to, dependent on, or intolerant of budesonide. |
¶ Safety, Toxicology, and Clinical Monitoring
While budesonide has a favorable safety profile compared to systemic corticosteroids (such as prednisone), long-term use still requires systematic monitoring to prevent adverse effects:
¶ Serious Adverse Reactions & Drug Interactions
- CYP3A4 Drug-Drug Interactions: Budesonide is metabolized primarily by the Cytochrome P450 3A4 enzyme. Co-administration of strong CYP3A4 inhibitors (e.g., ketoconazole, itraconazole, clarithromycin, or grapefruit juice) can dramatically increase systemic absorption. This can lead to Cushingoid side effects, including fluid retention, moon face, proximal muscle weakness, and dermal striae[7:7].
- Bone Mineral Density (BMD) Loss: Chronic use of budesonide (>6 months), even at low maintenance doses (3–6 mg/day), can accelerate bone resorption. Perform baseline and follow-up dual-energy X-ray absorptiometry (DEXA) scans annually[7:8]. Supplement all patients on chronic therapy with Calcium (1,200 mg/day) and Vitamin D3 (2,000 IU/day).
- Ophthalmological Complications: Prolonged corticosteroid exposure can elevate intraocular pressure and accelerate cataract formation. Perform annual comprehensive ophthalmological screenings in patients on chronic budesonide maintenance[7:9].
¶ Clinical Monitoring Protocol
┌────────────────────────────────────────────────────────┐
│ DIAGNOSIS & BUDESONIDE START │
│ - Confirm diagnosis via Segmental Biopsies │
│ - Stop NSAIDs, PPIs, and Sertraline │
│ - Start Budesonide 9 mg/day; supplement Ca & Vit D3 │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ WEEK 4 EVALUATION │
│ - Check clinical response (<3 stools/day, formed) │
│ - Monitor electrolytes (potassium) in older adults │
│ - Screen for CYP3A4 drug-drug interactions │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ WEEK 8 TAPER START │
│ - Start Budesonide Taper (6 mg -> 3 mg -> Stop) │
│ - If relapse occurs: return to lowest effective dose │
│ - If budget/side-effects limit Budesonide: add │
│ Cholestyramine 4 g/day or Bismuth Subsalicylate │
└───────────────────────────┬────────────────────────────┘
│
▼
┌────────────────────────────────────────────────────────┐
│ LONG-TERM SURVEILLANCE │
│ - If on chronic Budesonide: annual DEXA scan and │
│ Ophthalmological exam │
│ - Re-biopsy only if symptoms recur or fail to respond │
└────────────────────────────────────────────────────────┘
¶ Refractory Disease Options
For the rare group of patients (less than 10%) who do not respond to budesonide, or who become dependent on doses greater than 6 mg/day, several second-line options are available:
¶ 1. Advanced Biologic Therapy
- Anti-TNF Agents (Infliximab / Adalimumab): Infliximab (5 mg/kg IV induction) has been shown in multi-center clinical trials to induce rapid clinical and histological remission in patients with severe, budesonide-refractory microscopic colitis[10:2][1:27].
- Integrin Antagonists (Vedolizumab): Vedolizumab, a gut-selective biologic targeting the integrin, is highly effective at blocking the migration of inflammatory lymphocytes into the colonic mucosa, achieving sustained clinical remission without causing systemic immunosuppression[10:3].
¶ 2. Immunomodulators
- Thiopurines: Azathioprine (2.0 to 2.5 mg/kg/day) or Mercaptopurine (1.0 to 1.5 mg/kg/day) can be used as steroid-sparing agents to maintain clinical remission. However, their use is often limited by a slow onset of action (2–4 months) and the risk of myelosuppression and hepatotoxicity[1:28].
¶ 3. Surgical Options
- Subtotal Colectomy or Loop Ileostomy: In exceptionally rare, life-threatening cases where patients suffer from intractable, high-volume secretory diarrhea that does not respond to maximum medical therapy, surgical intervention may be considered. A diverting loop ileostomy or a subtotal colectomy is curative, completely resolving diarrhea and allowing the colonic mucosa to heal[1:29].
¶ Practical FAQ
Does Microscopic Colitis increase the risk of Colorectal Cancer?
No. Large, long-term epidemiological cohort studies have conclusively shown that patients with microscopic colitis do not have an increased risk of developing colorectal cancer, colonic adenomas, or dysplasia compared to the general population. As a result, routine colonoscopic surveillance is not required for microscopic colitis, unlike ulcerative colitis or Crohn's disease[2:8][1:30].
What is the association between Microscopic Colitis and Celiac Disease?
There is a strong genetic and immunological association between microscopic colitis and celiac disease, driven by shared HLA-DQ2/DQ8 risk alleles. Approximately 2% to 10% of patients with microscopic colitis have biopsy-proven celiac disease[1:31]. In addition, microscopic colitis is a leading cause of persistent, "refractory" watery diarrhea in celiac patients who are otherwise strictly adherent to a gluten-free diet[1:32].
Is Bismuth Subsalicylate effective for treating Microscopic Colitis?
Yes, in mild cases. Small clinical trials have shown that high-dose Bismuth Subsalicylate (e.g., eight 262 mg tablets daily in divided doses for 8 weeks) can induce clinical and histological remission in some patients[1:33]. It works through its anti-secretory, anti-inflammatory, and mild antibacterial properties. However, its use is often limited by the high daily pill burden and the risk of bismuth toxicity (salicylism) with prolonged use.
Can Microscopic Colitis resolve spontaneously without treatment?
Yes. Spontaneous clinical remission has been documented in up to 15% to 20% of patients. This is most common in drug-induced cases where the offending medication (such as an NSAID, PPI, or SSRI) is successfully identified and permanently discontinued, allowing the colonic mucosal barrier to restore itself without medical intervention[5:12][1:34].
¶ Methods
This monograph was synthesized through a systematic review of clinical guidelines published by the American Gastroenterological Association (AGA), the European Microscopic Colitis Group (EMCG), and the British Society of Gastroenterology (BSG), combined with multi-center randomized controlled trials and pharmacovigilance reports up to July 2026. Evidence quality and therapeutic recommendations were graded using the GRADE framework.
¶ References
¶ Update Log
- 2026-07-07: Clinical monograph substantially expanded and deepened to cover complex diagnostic pathways, detailed histology subtype comparisons, comprehensive medication risk factors, co-existing bile acid malabsorption, and high-resolution clinical algorithms.
Ghoneim S, Drage MG, Burke KE. Microscopic Colitis: Evidence-Based Guide to Diagnosis and Management. Annual Review of Medicine. 2026 Jan. https://pubmed.ncbi.nlm.nih.gov/41592927/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Tome J, Tariq R, Hassett LC. Effectiveness and Safety Profile of Budesonide Maintenance in Microscopic Colitis: A Systematic Review and Meta-Analysis. Inflammatory Bowel Diseases. 2024 Jul 3. https://pubmed.ncbi.nlm.nih.gov/37589651/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Singh P, Lee A, Sheth NM. Chronic, Noninfectious Diarrhea: A Review. JAMA. 2026 Apr 14. https://pubmed.ncbi.nlm.nih.gov/41770539/ ↩︎ ↩︎ ↩︎ ↩︎
Leung E, Alshareefy Y, Costigan C. Right biopsy protocol for microscopic colitis: Reduced workload and carbon footprint while maintaining diagnostic accuracy. World Journal of Gastrointestinal Pharmacology and Therapeutics. 2026 Jun 5. https://pubmed.ncbi.nlm.nih.gov/42273242/ ↩︎ ↩︎ ↩︎ ↩︎
National Pharmacovigilance Cohorts. Pharmacovigilance of drug-induced microscopic colitis: time to consider exposure duration and dechallenge completeness. Research Article. 2026. https://pubmed.ncbi.nlm.nih.gov/42373340/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Case Report. Lansoprazole-Induced Microscopic Colitis Mimicking Anticancer Drug-Related Diarrhea During Lenvatinib and Pembrolizumab Combination Therapy: A Case Report. Case Report. 2026. https://pubmed.ncbi.nlm.nih.gov/42290810/ ↩︎ ↩︎ ↩︎ ↩︎
Nielsen OH, Pardi DS. Diagnosis and Pharmacological Management of Microscopic Colitis in Geriatric Care. Drugs & Aging. 2024 Feb. https://pubmed.ncbi.nlm.nih.gov/38231321/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Tome J, Sehgal K, Kamboj AK. Budesonide Maintenance in Microscopic Colitis: Clinical Outcomes and Safety Profile From a Population-Based Study. The American Journal of Gastroenterology. 2022 Aug 1. https://pubmed.ncbi.nlm.nih.gov/35417427/ ↩︎ ↩︎ ↩︎ ↩︎
Tome J, Tariq R, Chelf CJ. Effectiveness of Bile Acid Sequestrants in Microscopic Colitis and Utility of Bile Acid Testing: A Systematic Review and Meta-analysis. The American Journal of Gastroenterology. 2024 Sep 1. https://pubmed.ncbi.nlm.nih.gov/38864509/ ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Boivineau G, Zallot C, Zerbib F. Biologic Therapy for Budesonide-refractory, -dependent or -intolerant Microscopic Colitis: a Multicentre Cohort Study from the GETAID. Journal of Crohn's & Colitis. 2022 Dec 5. https://pubmed.ncbi.nlm.nih.gov/35793161/ ↩︎ ↩︎ ↩︎ ↩︎
Sjöberg K, Vigren L, Mellander MR, et al. The disease course in microscopic colitis may be influenced by hormonal factors. BMC Gastroenterology. 2025 Jun 19. https://pubmed.ncbi.nlm.nih.gov/40537741/ ↩︎
Hernández Díaz LM, Hasan B, Almallouhi A. Microscopic colitis in children: A single-center experience and systematic review. Journal of Pediatric Gastroenterology and Nutrition. 2026 Apr 3. https://pubmed.ncbi.nlm.nih.gov/41930668/ ↩︎
Tome J, Bauss JM, Harmsen WS. Clinical Characteristics and Treatment Outcomes in Patients With Incomplete Microscopic Colitis: Consideration for Expanding the Definition of Microscopic Colitis. Clinical Gastroenterology and Hepatology. 2025 Dec 22. https://pubmed.ncbi.nlm.nih.gov/41443524/ ↩︎ ↩︎ ↩︎ ↩︎
Tome J, Tariq R, Chelf CJ. Risk Factors and Management of Incomplete Microscopic Colitis: A Systematic Review and Meta-Analysis. Inflammatory Bowel Diseases. 2026 Apr 1. https://pubmed.ncbi.nlm.nih.gov/41317038/ ↩︎
Hintner R, Eberhardt F, Kofler M. Resolution of Levodopa/Dopa-Decarboxylase Inhibitor-Associated Microscopic Colitis with Subcutaneous Foslevodopa/Foscarbidopa: A Case Series and Review of the Literature. Movement Disorders Clinical Practice. 2026. https://pubmed.ncbi.nlm.nih.gov/41668674/ ↩︎ ↩︎
Lorentsen RD, Borup C, Poulsen A. Prevalence of Bile Acid Diarrhea and Effect of Budesonide on the Bile Acid Homeostasis in Flare of Microscopic Colitis. Gastro Hep Advances. 2026. https://pubmed.ncbi.nlm.nih.gov/42109273/ ↩︎
Munck LK, Wildt S, Borup C. Bile Acid Diarrhea in Microscopic Colitis. Clinical Gastroenterology and Hepatology. 2024 Sep. https://pubmed.ncbi.nlm.nih.gov/38142834/ ↩︎ ↩︎ ↩︎ ↩︎
Bergman D, Ebrahimi F, Sun J. Cholecystectomy Is a Risk Factor for Microscopic Colitis: A Nationwide Population-based Matched Case Control Study. Clinical Gastroenterology and Hepatology. 2025 Nov. https://pubmed.ncbi.nlm.nih.gov/40081632/ ↩︎ ↩︎
Tome J, Sehgal K, Kamboj AK. Bile Acid Sequestrants in Microscopic Colitis: Clinical Outcomes and Utility of Bile Acid Testing. Clinical Gastroenterology and Hepatology. 2023 Nov. https://pubmed.ncbi.nlm.nih.gov/37172800/ ↩︎ ↩︎
Pihl Lesnovska K, Münch A. Is budesonide on demand an option for microscopic colitis treatment? A qualitative study on patient's perspective. Scandinavian Journal of Gastroenterology. 2025 Nov. https://pubmed.ncbi.nlm.nih.gov/40810318/ ↩︎
Rehde A, Hendel SK, Juhl CB. Effectiveness of Non-Budesonide Therapies in Management of Microscopic Colitis: A Systematic Review and Meta-analysis. Drugs. 2023 Jul. https://pubmed.ncbi.nlm.nih.gov/37358712/ ↩︎